1. Introduction
Social inequality has gained greater visibility in different socioeconomic contexts due to the impact of COVID-19. There are human settlements characterized by deficiencies in the sanitary area, which have become one of the many scenarios of living in a worrying vulnerable state at present. According to the study conducted by the Economic Commission for Latin America and the Caribbean (CEPAL) [
1], certain parameters have been identified, such as overcrowding, lack of sanitation and lack of access to drinking water, which make indigenous communities vulnerable areas and, at the same time, a focus of concern in the face of the health crisis.
In the Peruvian context, it is recognized that there are efforts by the central government to support these vulnerable areas as intervention plans of the Ministry of Health (MINSA) [
2,
3] facilitate the health intervention of regional governments and MINSA; however, the support is truncated. Under this scenario, the community of Conayca, located in the Peruvian Andes (Huancavelica at 3642 m.a.s.l.), has become a field of study of interest, not only because of its inaccessibility, lack of resources and absence of government, but also because it allows us to reflect on the effects of the pandemic on the life of the predominant inhabitants of this community: inhabitants between 69 and 99 years of age.
Considering the characteristics of the inhabitants such as their most common comorbidities typical of their age (gastrointestinal diseases, and malnutrition), their social isolation (they live alone and in a state of abandonment, generating depression) and their labor activity (mainly agriculture and livestock activity), it is important to understand how their direct contact with nature, such as rural areas, greatly influences their wellbeing.
Accordingly, this exploration is based on the impact of the landscape on the mental and physical health of the inhabitants and how nature-based solutions (NbS) can be implemented in rural environments in a state of extreme vulnerability in order to contribute to a better quality of life for the elderly inhabitants, and to prepare for different types of crises (other pandemics) in the future.
Taking NbS as a starting point allows us to re-evaluate the role of ecosystems in the development of a sustainable life and to respond to societal challenges such as the health crisis. A large number of studies confirm the positive impact the natural environment has on the mental and physical health of the user. The quarantine adopted by various societies is evidence of how the everyday environment alters occupants’ wellbeing. Therefore, a 10-month period of medical data collection in the study area and recognition of the natural elements characteristic of the rural area allowed for a reflection on how to counteract this current state of vulnerability.
2. Policy Framework
2.1. Relationship of the Human Being and the Environment
According to the Mandala of Health model, a sociological model based on the human ecosystem, the human being is a key part of the wider ecological fabric, operating as an entity within planetary boundaries. It is composed of an interplay between the body, mind and spirit because human values, attitudes and habits are linked to human biology, behavioral trades, psychosocial environments and the physical environment. Therefore, the model of the human health ecosystem integrates the natural and built environments with a dynamic model [
4]. Access to public spaces and green areas has been demonstrated to improve mental health and wellbeing. In this sense, landscape design and management solutions that sustain accessibility to parks, gardens, bodies of water, forests and other green spaces promote physical activity and healthier lifestyles [
5].
A vast number of studies have reported adverse effects of the built and social environments on health and health determinants through direct or indirect pathways, highlighting the links between the environment and health [
6]. In times of the COVID-19 crisis, it is important to understand the integral connection between the environment, health, and the economy [
7]. Mental illness is the single cause of long-term medical care, and a major driver of healthcare and other social costs. Thus, when mainstreaming health and wellbeing, people in vulnerable situations such as migrants, indigenous people, children, and elderly people, both in urban and rural areas, must also be considered [
8].
2.2. Impacts of the Natural Environment on Health
Human health is part of a global ecosystem, but it also sustains it. Damage to the ecosystem will therefore affect human health worldwide. Thus, to sustain and re-establish ecosystems across the globe, policies must consider ecology and social science as major informants in the process [
6]. Considering that disease can be prevented by enhancing the design, creation and management of environments in which people live, many initiatives have been led by the World Health Organization to propose the Ottawa Charter for Health Promotion. This charter contributed to putting health promotion on the international agenda, recognizing that decisions in non-health-related sectors often have an impact on health, and stressed the necessity to build intersectoral approaches to create supportive environments [
6].
Climate change’s effects on health, social, economic, environmental, and demographic aspects will generate greater impacts on public health [
6]. Currently, urban cities, through the living environment, transport, buildings, etc., have impacts on physical health (respiratory and cardiovascular pathologies, trauma), mental health (stress, depression, isolation) and health inequalities (social, environmental, and territorial) [
3]. Moreover, public health research suggests that disease tends to take place in those who (a) have fewer meaningful social relationships, (b) are in lower hierarchical positions and (c) are disconnected from their biological and cultural heritages [
6].
Likewise, lifestyles in rural areas are also exposed to diseases related to agricultural practices [
9]. The most common diseases are diarrheal diseases and Japanese encephalitis. Additionally, due to the management of wastewater for irrigation, intestinal nematode diseases are present [
10]. In this sense, the WHO and partner organizations have been developing substantive guidance and providing support for building healthier environments for healthier populations [
7]. As part of the WHO’s six prescriptions for achieving healthier environments, prescription one is focused on the protection and preservation of nature as the source of human health. This is because individuals and communities derive myriad non-material benefits from ecosystems [
11] such as clean air, water, and food. Further, the various cultures, religions and lifestyles in a community must be considered [
9].
2.3. Nature-Based Solutions for Healthy Environments
Ecosystems are the support of life on the planet for the human species and all other forms of life [
11]. Thus, nature-based solutions (NbS), which are solutions inspired and supported by nature, contribute to enhancing wellbeing and quality of life. However, values related to spiritual or cultural aspects tend not to be valued. Moreover, most of the research conducted has been focused on urban areas rather than rural areas or it has rarely focused on the landscape scale encompassing both rural and urban areas. Therefore, there is an opportunity to understand the values and benefits that nature provides, particularly in rural spaces and at the landscape level [
12].
In this sense, NbS play a key role in building sustainable communities to support the development of rural sustainability or the generation of sustainable communities at the landscape level. This is because understanding the ecological and landscape contexts of development can open opportunities for biodiversity [
13]. Evidence shows that the more proximity to and experience of nature, the more shaping the values that individuals hold about sustainability challenges and actions and behaviors they should take and perform. Thus, NbS play a role in (1) generating new types of connections of values for nature and, (2) understanding what consequences are taking place in equity terms [
12].
3. Methodology
The method used was retrospective, namely, a study based on a database of the local medical center. Thus, the methodology involved the collection of two types of data: First, the data based on the medical visits made by the inhabitants of Conayca were collected. During the interviews, COVID protocols were maintained through the use of masks and appropriate distancing. These interviews were significant in that these individuals not only displayed positive aptitude but also consented to the use of their interviews for academic research. This allowed us to know the diseases and ailments suffered by older adults, specifically those who attended the family medicine clinic, located in the only health post that belongs to the health network of the department of Huancavelica. Second, residents’ histories were collected, which allowed us to know their living conditions, their type of housing, their occupation, the number of family members, their customs, their work routines, their knowledge regarding COVID-19, etc.
In this way, both methods contribute to exploratory research, which focuses on analyzing specific aspects that have not yet been analyzed in depth in the Peruvian context. The aim of this study was to find significant patterns in the data to be analyzed so that, based on these results, the vulnerable condition of this type of community forgotten by the government can be clarified and updated. This methodology is the first approach in a vulnerable rural area that invites further research so that it can be directed to a deeper analysis.
3.1. Eligibility Criteria
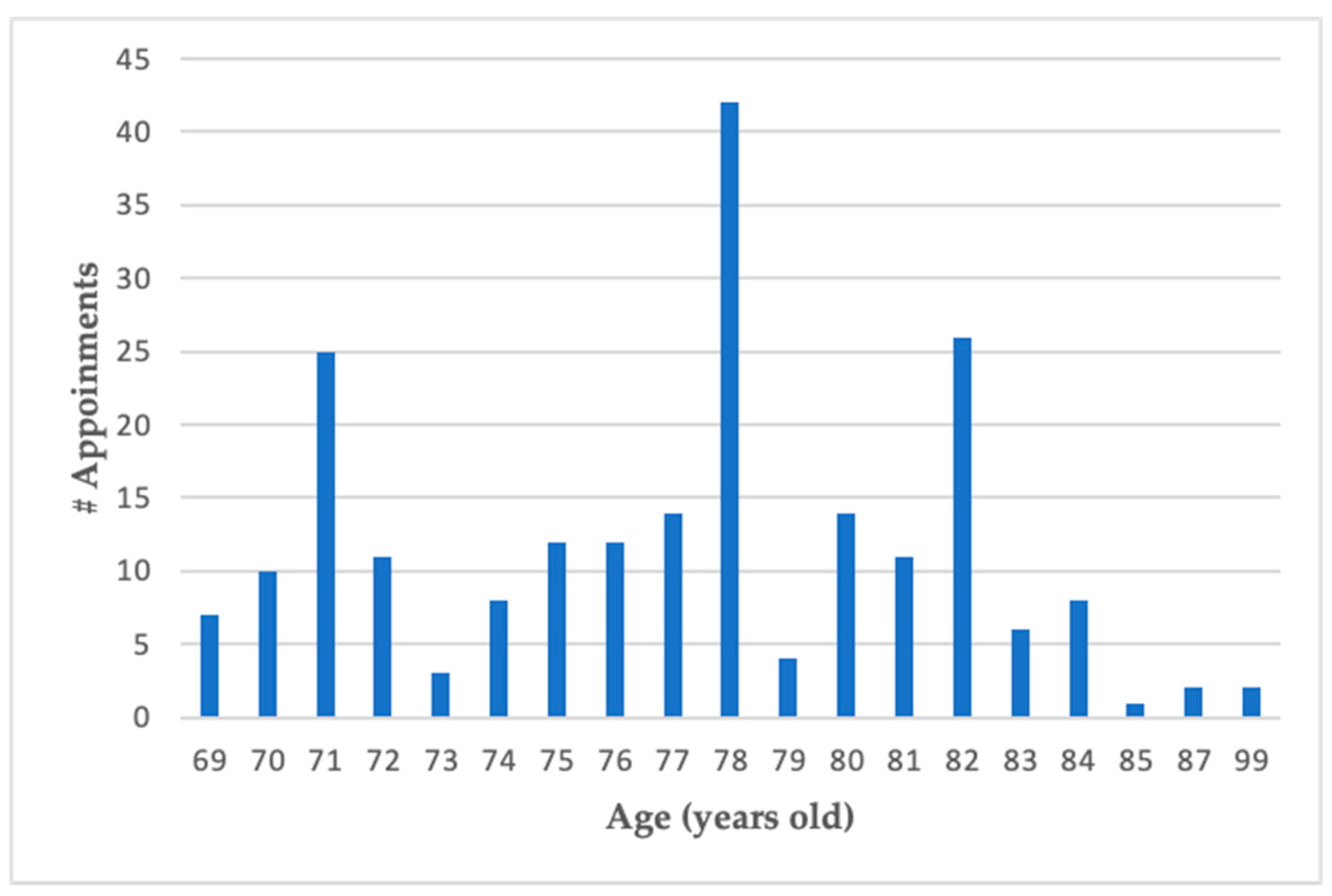
The community of Conayca has 1219 inhabitants with a population density of 29 inhabitants per km2. The low population density is due to the constant waves of migration that occur in these rural areas, as the children and grandchildren of resident families prefer to live in cities with better services in search of a better future. However, older adults prefer to remain in their place of origin even if it means living on their own. Thus, our study focused on diagnosing the wellbeing of elderly Conayca residents living alone in a vulnerable rural community by randomly considering 100 elderly patients due to the difficult access to their homes.
After an approximate general count of the medical visits, it was possible to observe the type of patient according to their age (see
Figure 1), where the range was between 69 and 99 years of age. It is understood that they live in a delicate state of health due to their age.
3.2. Information Source and Search Strategy
The medical data collection was conducted by Dr. Cristina Torres-Mallma during her 10-month period of rural and marginal urban health service (SERUMS), under the role of director of the health post located in the community of Conayca. However, faced with the lack of accessibility and disability of some residents, Dr. Torres-Mallma had to go to the patients’ residences to conduct some interviews. Although some patients were not as interested in talking to the medical staff, the visits to the homes allowed us to gain a better insight into their daily environment since they are located in remote areas with little accessibility. Each interview took approximately 10 min. Additionally, the interview considered personal data, socioeconomic situation, family history and personal health history.
3.3. Assessment
Since there are no assessment parameters for rural communities located in Latin America, the patterns proposed by the World Health Organization [
6] were considered, emphasizing the relationship between the environment and the health status of the inhabitants. Therefore, of the 11 key parameters for healthy cities, communities and towns proposed by Hancock and Duhl [
6], we focused on the second parameter which refers to “an ecosystem that is stable now and sustainable in the long term” to explore and reflect on the current situation of the community of Conayca. Likewise, approaches and techniques for community participation in local health and sustainable development developed [
14] by the WHO were considered.
4. Results
The results arose by considering three aspects. (1) What is the relationship between the community and the environment? (2) What is the impact of the landscape on the mental and physical health of the members of this community? (3) How are nature-based solutions (NBS) applied to rural areas in favor of the preservation of the identity and belonging of a vulnerable community? The elderly population of indigenous communities needs to be understood in terms of sociocultural, environmental, and economic factors to alleviate the condition of their bodily vulnerability through practices of care that guarantee quality of life not only during pandemic situations [
7] but also on a daily basis.
4.1. What Is the Relationship between the Community and the Environment?
For a better understanding, it is relevant to know the inhabitants’ profiles. Thus, after collecting medical data and histories for ten months in the community of Conayca,
Table 1 shows a profile of the inhabitants of Conayca based on information with a holistic and integrated perspective focusing on the relationships between the social, environmental, and economic factors. The population of this community (average age 69–99 years old) shows a general clinical diagnosis of gastrointestinal diseases and mental health issues. Lack of food essentials and abandonment of family members have been the main causes of malnutrition and depression disorders, respectively. Furthermore, the local government ignores the urgent needs of its elderly inhabitants and promotes practices of (un)care that endanger the health of its inhabitants such as the continuity of festivities without practicing protocol measures.
The general health situation of this population is alarming because they are inhabitants who are in a situation of poverty and in total abandonment not only by their families but also by the government. Due to their physical condition and limited accessibility, they tend not to socialize with other members of the community, nor do they manage frequenting health centers to obtain routine health services (see
Figure 2). In terms of accessibility, interprovincial public transportation is scarce, and residents have to walk at least 2 kilometers every day if they need to access another town. Furthermore, the pedestrian walkways have been converted into rustic roads that are laid out for the constant use of the inhabitants without any safety measures. Another factor against them is that there is no comprehensive linguistic inclusion, in the sense that sometimes the information and training that come from the central government are neglected when it comes to communicating in Conayca’s native language, Quechua. The immediate effect is the lack of interest in health campaigns, training, workshops, etc.
However, their wellbeing depends on agricultural and/or livestock activities. It is observed that this community has an average of three animals per household, which become a source of companionship due to the emotional ties between the elderly and their pets, and a source of food, as in the case of livestock. Likewise, their daily life is dedicated to agriculture as a source of diet. Therefore, the relationship of this community with its environment is limited to being individualistic and for survival purposes.
4.2. What Is the Impact of the Landscape on the Mental and Physical Health of the Members of This Community?
Since human health is part of and depends on the global ecosystem [
2], the Conayca community evidences positive impacts on its physical and mental health thanks to the landscape and rural environment. Despite suffering from diseases related to agricultural practices such as gastrointestinal diseases, there are no other cardiovascular, respiratory or endocrinological diseases or other age-related complications. This is because of the physical activity involved in agriculture and the deficient diet, since they only eat a few vegetables such as potatoes but are free of fats, not to mention the dry and cold climate and the absence of air pollution. Furthermore, even if they suffer from depression due to their fewer meaningful social relationships due to family abandonment, the impressive relief of the area characterized by mountains and ravines and the native vegetation of the area (e.g., natural grasses such as ichu, and eucalyptus trees) contribute to the distraction of the mind and mitigation of stress in the elderly (see
Figure 3). As a result, Conayca can be defined as a long-lived community, where the landscape and its natural resources are part of an ecological context that shapes the lifestyle by strengthening connections and values with nature through agriculture and livestock. However, it is understood that this is not enough because other factors (i.e., cultural and religious) also influence the integral development of healthy environments.
4.3. How Are Nature-Based Solutions Applied to Rural Areas in Favor of the Preservation of the Identity and Belonging of a Vulnerable Community?
The community of Conayca shows an idiosyncrasy characterized by a nature-dependent lifestyle in a rugged rural environment with little attention to health, education, and basic infrastructure services. Its economic activity allows the community to value nature only in the sense of harvesting crops and feeding livestock. Although there is respect for Pachamama or Mother Earth, inherited from their ancestors, cultural practices have ceased to be collective due to personal isolation and lack of accessibility to public spaces (main square) and their own homes. It has also been observed that if the local authority decides to celebrate a festivity, it is carried out without complying with sanitary protocols to avoid COVID-19 contagion. This governance exercise evidences the lack of safety and care criteria for the elderly in Conayca. Faced with this problem, it is considered that the survival of older adults represents a way of integrating NbS into human life, even in very vulnerable and precarious areas. In other words, Conayca has the opportunity to reinforce its link with nature and strengthen its identity as a rural community, since all economic, cultural, social and religious activities revolve around it. Therefore, this contributes to ecosystems where the health of the inhabitants and their environment develop in harmony and stability now and in the long term.
While Conayca facilitates physical health as the environment is free of polluted air and disturbing noises, its exposure to natural hazards such as rain and thunderstorms generates exposure to risks. The lifestyle in Conayca also facilitates mental health because the main mode of transportation is pedestrian, and the main economic activity is agriculture, allowing for daily physical activity and access to healthier food. In addition, the presence of the rural wilderness landscape allows for the protection and preservation of the ecosystem and biodiversity. However, loneliness and family abandonment are decisive factors in the community’s mental health. In contrast, health equity represents a challenge because the community’s exposure to health risks is exacerbated by the lack of adequate health infrastructure and resources that respond to its wellbeing, as well as the lack of policies and regulations and local governments that consider this vulnerable population. In short, the health and wellbeing of the Conayca inhabitants are local government challenges that exacerbate the incipient awareness to achieve the Sustainable Development Goals and the 2030 Agenda for Sustainable Development.
5. Discussion and Conclusions
From the experience of living with other members of the Conayca community, more questions have been generated since this case represents one of the many socioenvironmental challenges in the high Andean areas of Peru. Although Peru has a national program on age-friendly environments [
10], little or nothing is known about indigenous communities. The starting question is, how do we speak of an ecosystem if the population is completely abandoned and isolated by various factors? This leads us to propose a vision of how to strengthen the relationship between community and environment for building local health communities.
The Conayca community’s inhabitants represent a vulnerable population because, being elderly, in addition to their health status that is usually more delicate than that of young people, they are not listened to due to governmentality issues (i.e., weak exercise of authority, lack of planning and absence of the voice of the villager). This is why, through this exploratory research, we sought to hear their voices through medical consultations and thus be able to understand their social, cultural and emotional worlds. By raising the voices of these communities, their participation plays an important role in combating social exclusion in Peruvian society. In this way, the results of this research contribute not only to decision making to build appropriate responses, but also to health equity and solidarity in action between indigenous communities, between groups of people of different ages and between genders.
If the government response is slow and resources are limited, there are opportunities to work together with universities and international non-governmental organizations to apply the methods and techniques of the community participation approach in local health and sustainable development. Likewise, the opportunity to have young doctors who choose to carry out the SERUM experience in wild and rural areas for a year is a very significant contribution because their experiences constitute knowledge for public health based on their proximity to the populations and their everyday reality. For this reason, studies need to be carried out in rural areas where vulnerable populations also reside and who are practically socially excluded, as well as on vulnerable populations in urban areas, to achieve equity in health and dignified lives.
The health of rural communities, such as the case of Conayca, depends directly on the local productive ecosystems that are the sources of basic nutrition, but having a survival lifestyle, they suffer from malnutrition and gastrointestinal diseases. Furthermore, the inhabitants paint a depressive picture due to family abandonment and the absence of affective relationships in their community. For this reason, it is necessary to have some parameters for the Latin American or Andean rural context that are simple to understand and practical in order to avoid procedures and delays so that the residents and leaders can easily organize themselves by integrating the elderly. This allows defining the starting points for principles of spaces adapted to the elderly and indigenous communities based on updated systematic inventories.
A culture of change is needed in the health field, as poverty and the high burden of disease in these communities also impair their ability to prepare for the future. Human wellbeing and poverty reduction also depend on the quality of ecosystems. Likewise, contact with nature, being physical and palpable as well as visual, evidence positive impacts, contributing to the hypothesis that the stimulation of contact with the richness and diversity of ecosystems benefits physical and mental health. Furthermore, in a context of a lack of basic infrastructure, integrating health in urban and territorial planning is vital because it will not only help to achieve SDG 3 (health and wellbeing) but will also strengthen the relationships among the 17 SDGs.
This research provides a strong conclusion in light of the different approaches, methods, models and assumptions, and one that is expected to be relatively unaffected by uncertainties. In this context, by addressing key uncertainties regarding changes in ecosystems and human health, social and environmental challenges towards healthier environments in high Andean areas can provide precision regarding the quantification of the magnitude or times of the impacts, costs, benefits, changes in ecosystems, impacts on human wellbeing or results. Since health and wellbeing for all at all ages are key determinants to achieve the Sustainable Development Goals, the lives of the most vulnerable, such as the elderly in indigenous communities, should not go unnoticed but rather be valued for their role as protectors of rural ecosystems. At the same time, they should be respected as the bearers of cultural identity. By improving human health and wellbeing, the Conayca inhabitants will foster resilience and continue to protect the environment.







{kind=link}
{kind=link}
{kind=link}