
Wearable Multimodal Skin Sensing for the Diabetic Foot


Abstract
:
1. Introduction
2. Experimental Platform
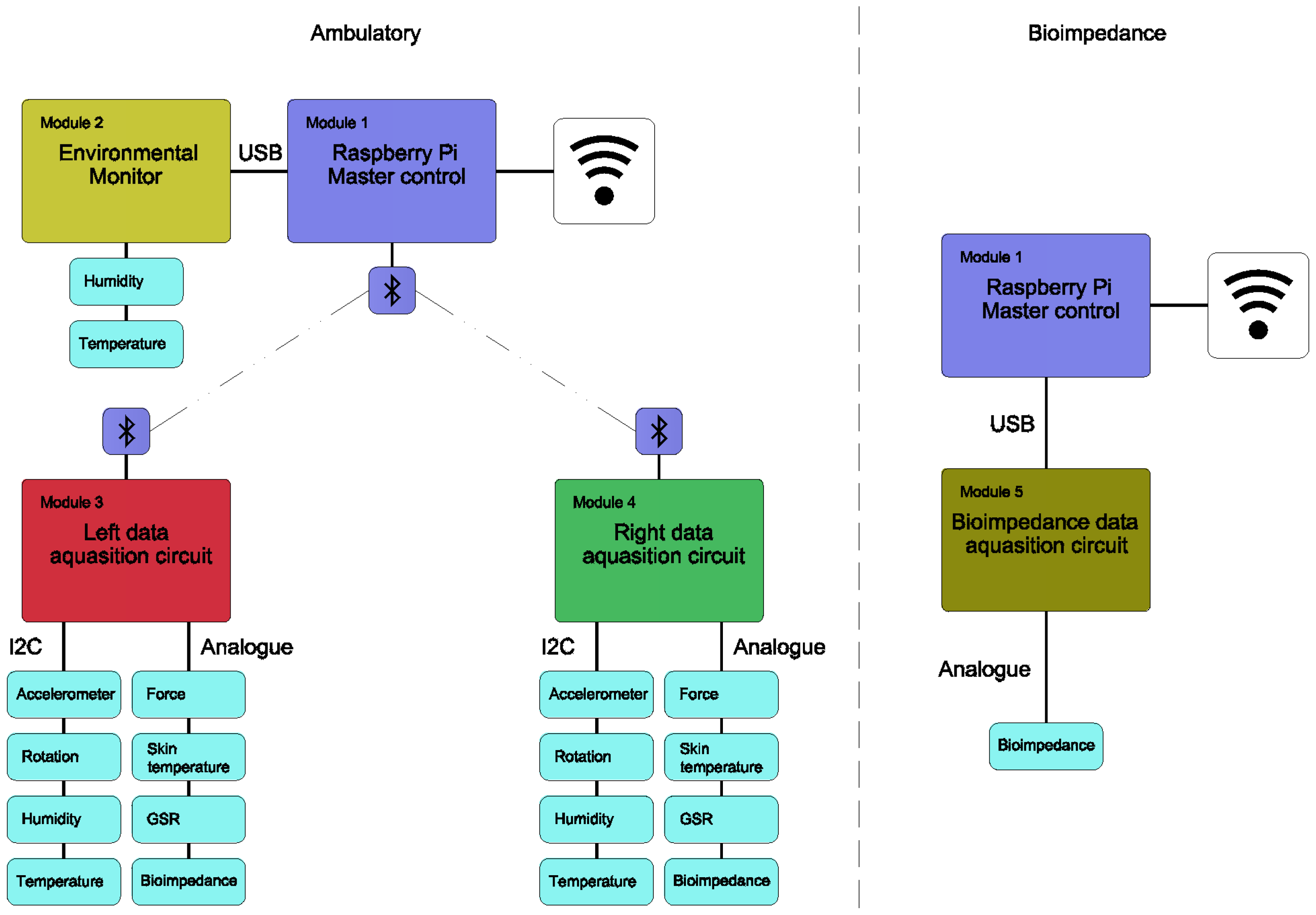
2.1. System Modules
2.2. Enviromental Monitor
2.3. In Shoe Data Acquisition Circuit
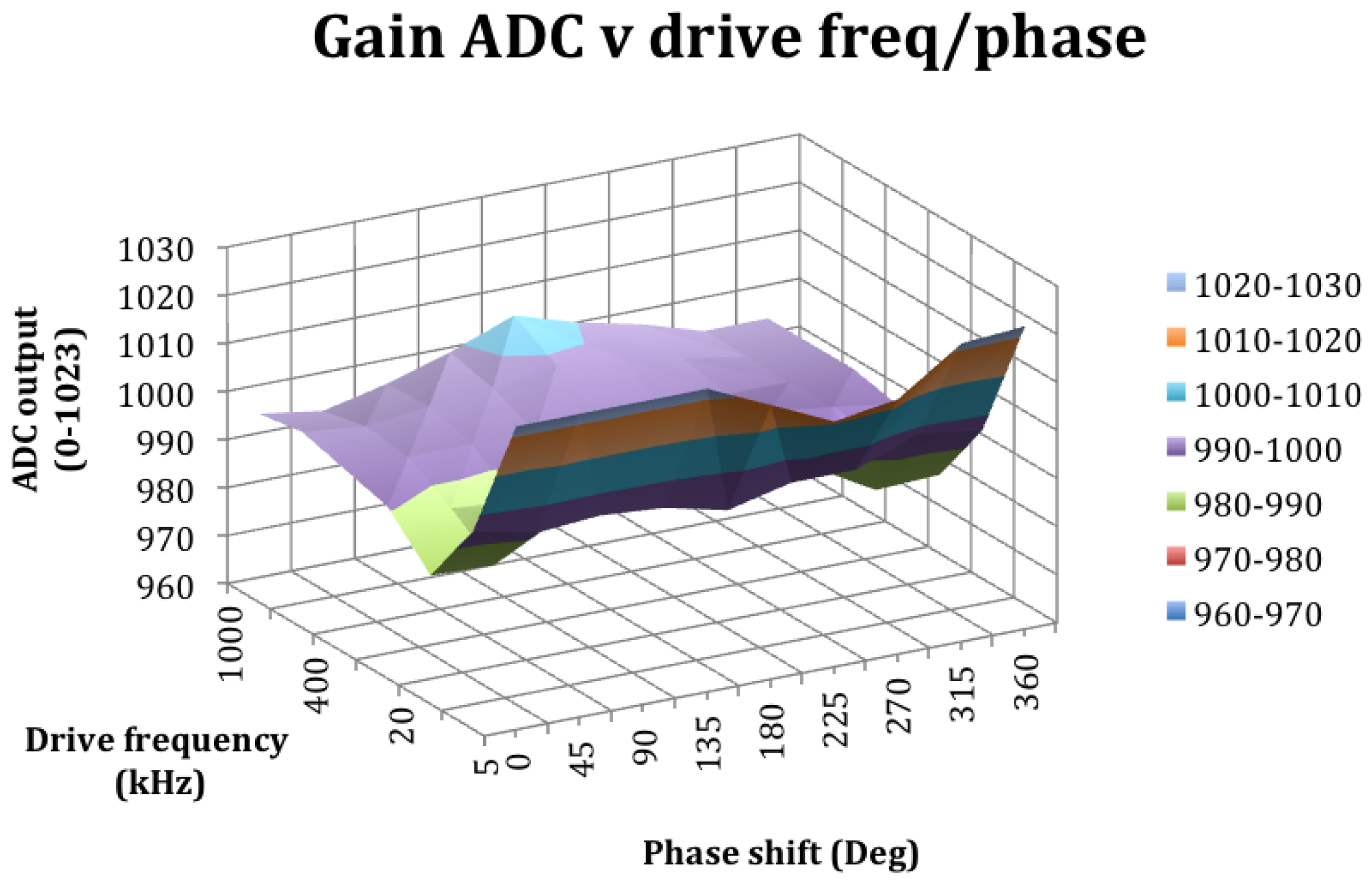
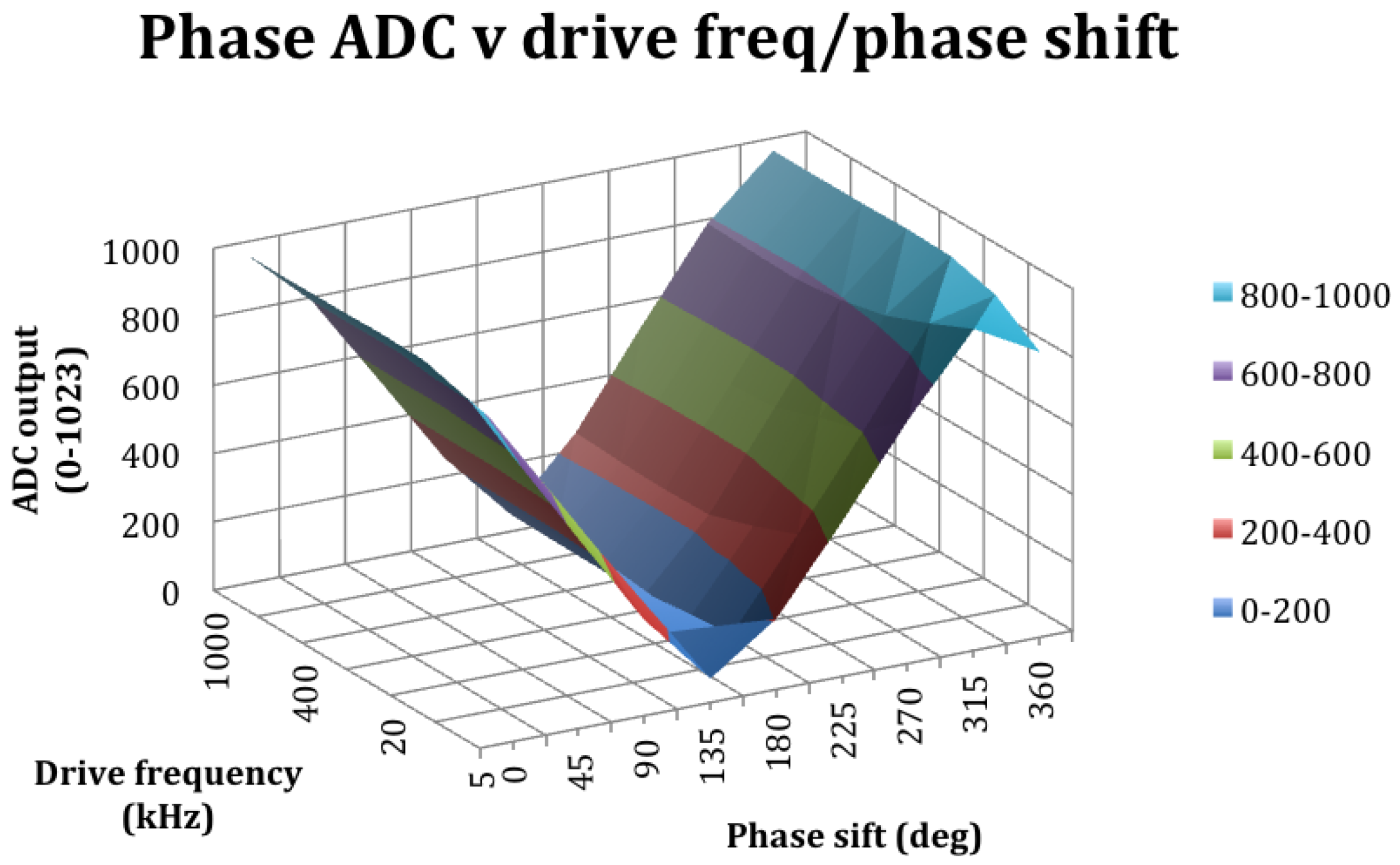
2.4. Bioimpedance Sensor
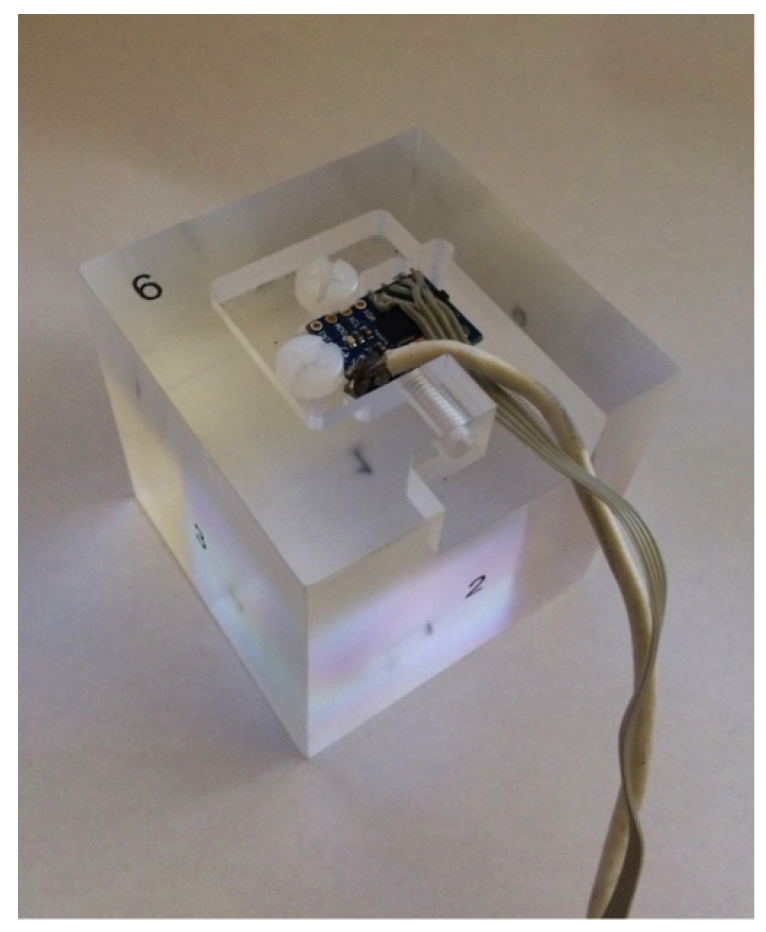
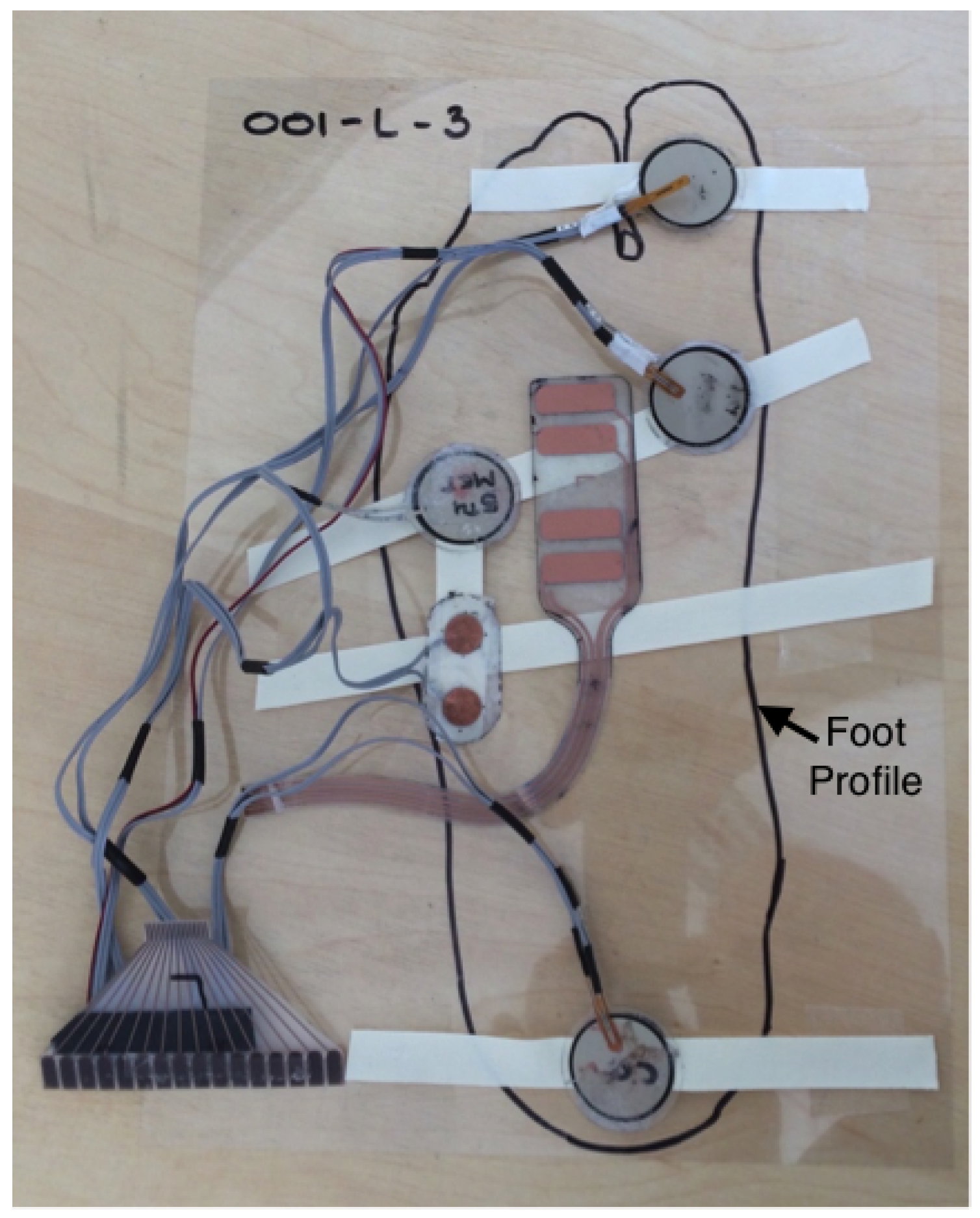
2.5. Foot Mounted Sensor Array
2.6. Calibration and Validation
2.7. Sensor Evaluation
3. Test Protocol
3.1. Laboratory Setup
3.2. Test Subject Demographic
3.3. Test Setup
3.4. In Shoe Testing
3.5. Bioimpedance Testing
4. Results and Discussion
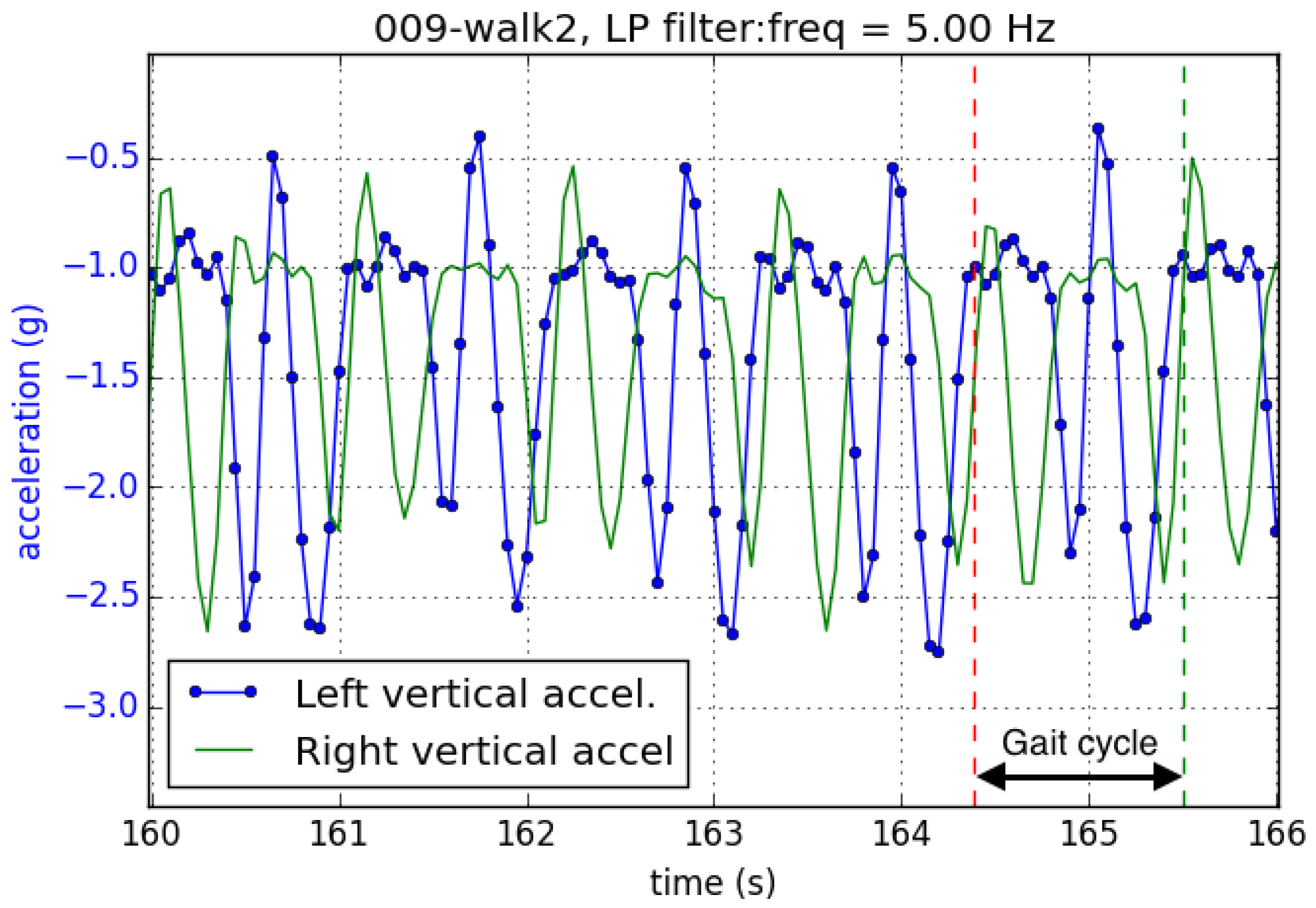
4.1. Vertical Acceleration
4.2. Acceleration and Force
4.3. Humidity and GSR
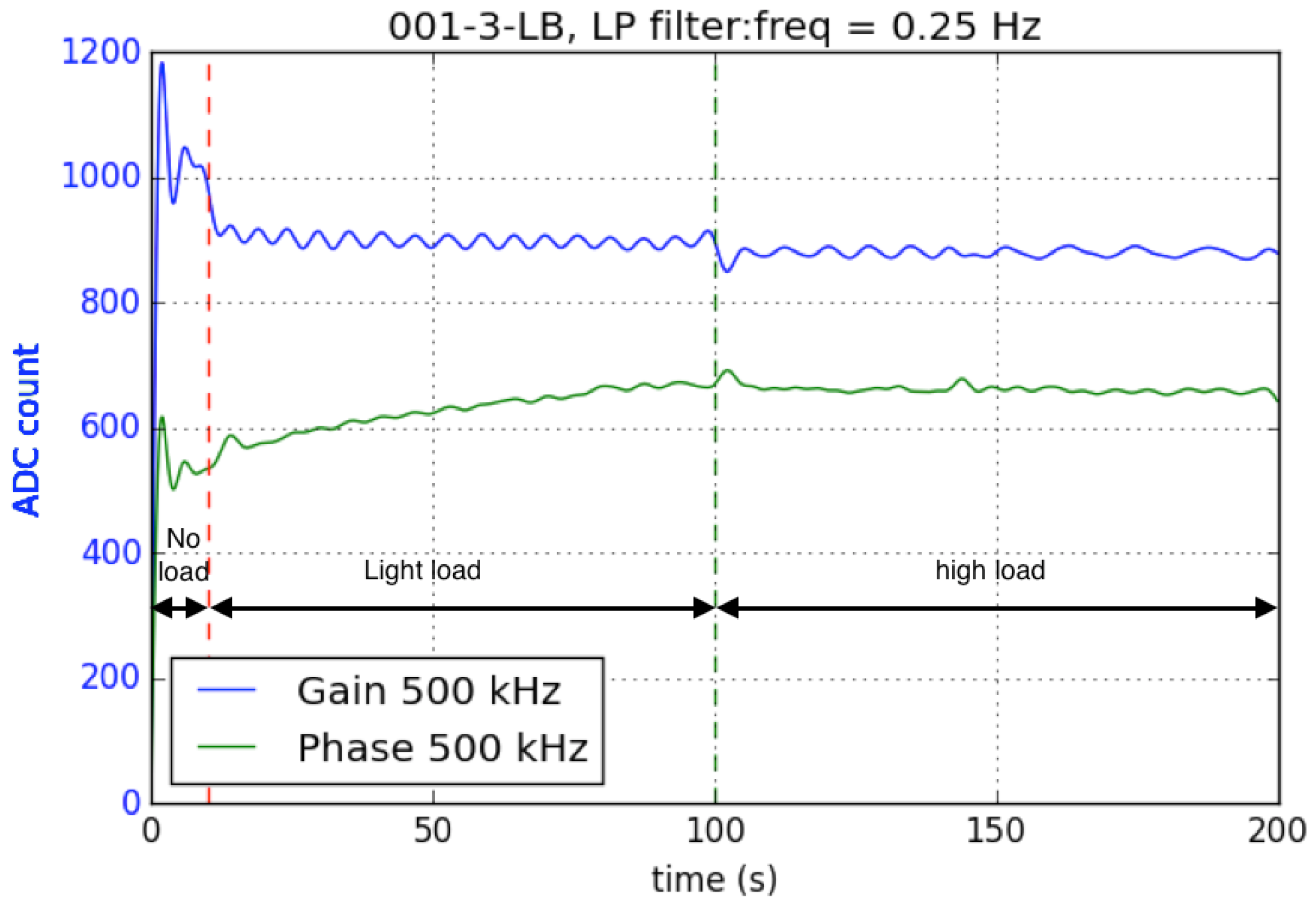
4.4. Bioimpedance
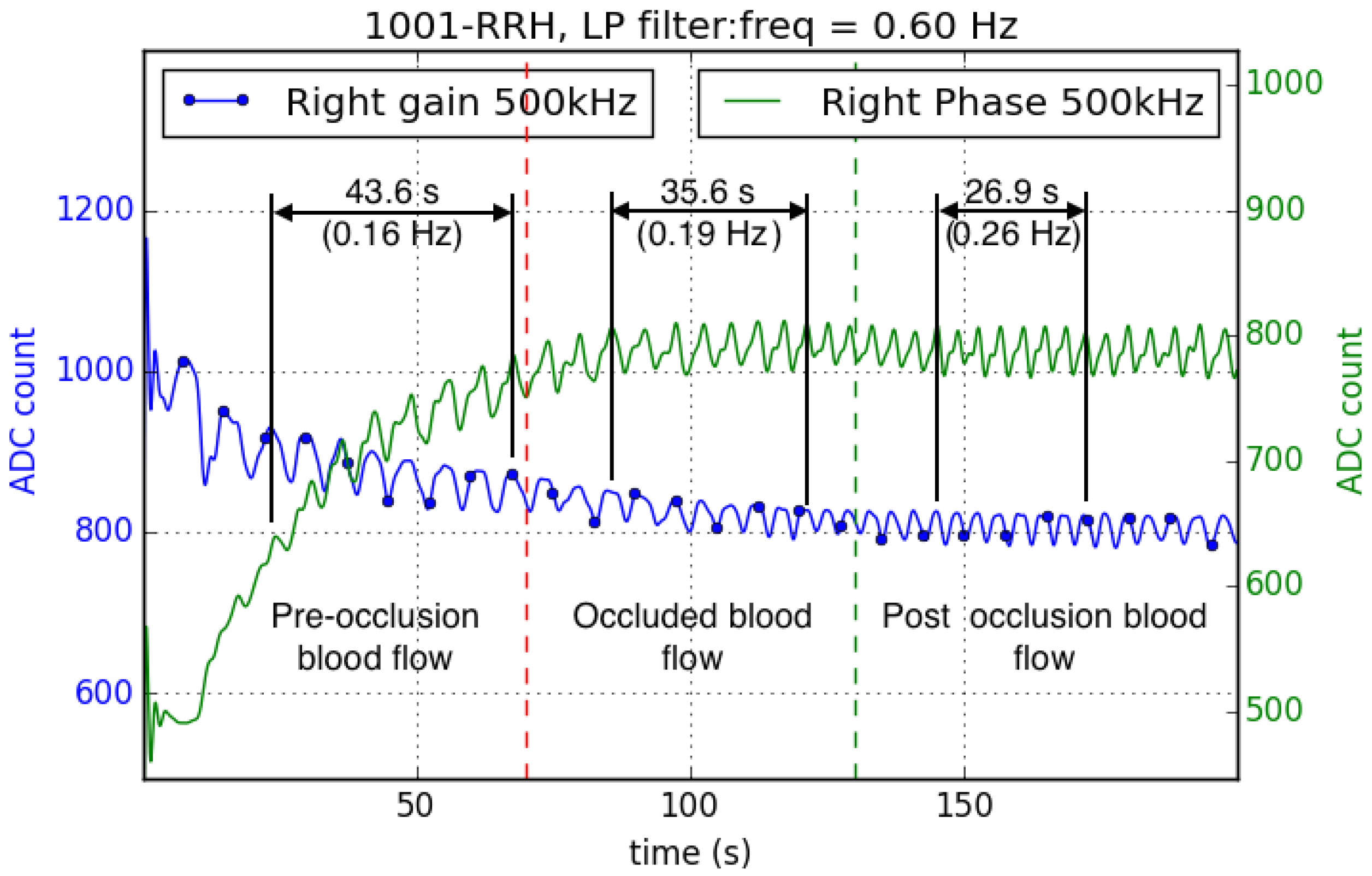
4.5. Occluded Blood Flow
4.6. Limitations of the Current Device for Long Term Use
5. Conclusions
Acknowledgments
Author Contributions
Conflicts of Interest
References
- Raspberry Pi Foundation. Available online: https://www.raspberrypi.org (accessed on 21 May 2016).
- Raspbian OS. Available online: https://www.raspbian.org (accessed on 21 May 2016).
- NICE. Diabetic Foot Problems: Prevention and Management (NG19); NICE: London/Manchester, UK, 2015. [Google Scholar]
- Hex, N.; Bartlett, C.; Wright, D.; Taylor, M.; Varley, D. Estimating the current and future costs of Type 1 and Type 2 diabetes in the UK, including direct health costs and indirect societal and productivity costs. Diabet. Med. 2012, 29, 855–862. [Google Scholar] [CrossRef] [PubMed]
- Lavery, L.A.; Higgins, K.R.; Lanctot, D.R.; Constantinides, G.P.; Zamorano, R.G.; Armstrong, D.G.; Athanasiou, K.A.; Agrawal, C.M. Home monitoring of foot skin temperatures to prevent ulceration. Diabet. Care 2004, 27, 2642–2647. [Google Scholar] [CrossRef]
- Armstrong, D.G.; Lavery, L.A.; Liswood, P.J.; Todd, W.F.; Tredwell, J.A. Infrared dermal thermometry for the high-risk diabetic foot. Phys. Therapy 1997, 77, 169–175. [Google Scholar]
- Edmonds, M. The Neuropathic Foot in Diabetes Part I: Blood Flow. Diabet. Med. 1986, 3, 111–115. [Google Scholar] [CrossRef] [PubMed]
- Flynn, M.; Edmonds, M.; Tooke, J.; Watkins, P. Direct measurement of capillary blood flow in the diabetic neuropathic foot. Diabetologia 1988, 31, 652–656. [Google Scholar] [CrossRef] [PubMed]
- Soames, R. Foot pressure patterns during gait. J. Biomed. Eng. 1985, 7, 120–126. [Google Scholar] [CrossRef]
- Maluf, K.S.; Morley, R.E.; Richter, E.J.; Klaesner, J.W.; Mueller, M.J. Foot pressures during level walking are strongly associated with pressures during other ambulatory activities in subjects with diabetic neuropathy. Arch. Phys. Med. Rehabil. 2004, 85, 253–260. [Google Scholar] [CrossRef] [PubMed]
- Nardone, A.; Grasso, M.; Schieppati, M. Balance control in peripheral neuropathy: are patients equally unstable under static and dynamic conditions? Gait Posture 2006, 23, 364–373. [Google Scholar] [CrossRef] [PubMed]
- D’Addio, G.; Iuppariello, L.; Pagano, G.; Biancardi, A.; Bifulco, P.; Cesarelli, M. New Posturographic Assessment by mean of Novel E-textile and Wireless Socks Device in Normal Subjects. Available online: http://www.gamant.it/download/IEEE%20EMBS%202015%20-%20D’Addio%20-%20Sensoria.pdf (accessed on 21 May 2016).
- Zammit, G.V.; Menz, H.B.; Munteanu, S.E. Research Reliability of the TekScan MatScan® system for the measurement of plantar forces and pressures during barefoot level walking in healthy adults. J. Foot. Ankle Res. 2010, 3. [Google Scholar] [CrossRef] [PubMed]
- Nicolopoulos, C.; Anderson, E.; Solomonidis, S.; Giannoudis, P. Evaluation of the gait analysis FSCAN pressure system: clinical tool or toy? Foot 2000, 10, 124–130. [Google Scholar] [CrossRef]
- Morley, R.E., Jr.; Richter, E.J.; Klaesner, J.W.; Maluf, K.S.; Mueller, A.J. In-shoe multisensory data acquisition system. IEEE Trans. Biomed. Eng. 2001, 48, 815–820. [Google Scholar] [CrossRef] [PubMed]
- Maluf, K.S.; Morley, R.E.; Richter, E.J.; Klaesner, J.W.; Mueller, M.J. Monitoring in-shoe plantar pressures, temperature, and humidity: Reliability and validity of measures from a portable device. Arch. Phys. Med. Rehabil. 2001, 82, 1119–1127. [Google Scholar] [CrossRef] [PubMed]
- Armstrong, D.G.; Holtz-Neiderer, K.; Wendel, C.; Mohler, M.J.; Kimbriel, H.R.; Lavery, L.A. Skin temperature monitoring reduces the risk for diabetic foot ulceration in high-risk patients. Am. J. Med. 2007, 120, 1042–1046. [Google Scholar] [CrossRef] [PubMed]
- Gefen, A. Plantar soft tissue loading under the medial metatarsals in the standing diabetic foot. Med. Eng. Phys. 2003, 25, 491–499. [Google Scholar] [CrossRef]
- Sawacha, Z.; Gabriella, G.; Cristoferi, G.; Guiotto, A.; Avogaro, A.; Cobelli, C. Diabetic gait and posture abnormalities: A biomechanical investigation through three dimensional gait analysis. Clin. Biomech. 2009, 24, 722–728. [Google Scholar] [CrossRef] [PubMed]
- Segev-Bar, M.; Landman, A.; Nir-Shapira, M.; Shuster, G.; Haick, H. Tunable touch sensor and combined sensing platform: Toward nanoparticle-based electronic skin. ACS Appl. Mater. Interfaces 2013, 5, 5531–5541. [Google Scholar] [CrossRef] [PubMed]
- Stefanovska, A.; Bračič, M.; Kvernmo, H.D. Wavelet analysis of oscillations in the peripheral blood circulation measured by laser Doppler technique. IEEE Trans. Biomed. Eng. 1999, 46, 1230–1239. [Google Scholar] [CrossRef] [PubMed]
- Klaesner, J.W.; Hastings, M.K.; Zou, D.; Lewis, C.; Mueller, M.J. Plantar tissue stiffness in patients with diabetes mellitus and peripheral neuropathy. Arch. Phys. Med. Rehabil. 2002, 83, 1796–1801. [Google Scholar] [CrossRef] [PubMed]
- Orlin, M.N.; McPoil, T.G. Plantar pressure assessment. Phys. Therapy 2000, 80, 399–409. [Google Scholar]
- Petrofsky, J.S.; McLellan, K. Galvanic skin resistance—A marker for endothelial damage in diabetes. Diabet. Technol. Therap. 2009, 11, 461–467. [Google Scholar] [CrossRef] [PubMed]
- De Mul, F.F.; Morales, F.; Smit, A.J.; Graaff, R. A model for post-occlusive reactive hyperemia as measured with laser-Doppler perfusion monitoring. IEEE Trans. Biomed. Eng. 2005, 52, 184–190. [Google Scholar] [CrossRef] [PubMed]












{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Sensing Modality | Part Number | Manufacturer | Interface | Range | Units | Calibration or Validation |
|---|---|---|---|---|---|---|
| Accelerometer | MPU6050 | Invensense | I2C | ±16 | g | Validation |
| Rotation | MPU6050 | Invensense | I2C | ±2000 | Validation | |
| Humidity | HYT271 | Hygrochip | I2C | 0–99 | % RH | Validation |
| Temperature | HYT271 | Hygrochip | I2C | –40–125 | Validation | |
| GSR | - | Self built | Analogue | 0–5000 | kΩ | Validation |
| Bioimpedance | AD9850 AD8302 | Analogue Devices | Analogue | 0–1023 | AU | Validation |
| Force | A401-25 | Flexiforce | Analogue | 0–140 | N | Calibration |
| Temperature skin | 104JT-25 | ATC-Semitec | Analogue | 20–40 | Calibration |
| Volunteer | Gender | Age | Height (m) | Weight (kg) | BMI |
|---|---|---|---|---|---|
| 001 | M | 46.00 | 1.78 | 97.00 | 30.61 |
| 009 | M | 29.00 | 1.80 | 75.80 | 23.40 |
| 1001 | F | 27.00 | 1.70 | 55.70 | 19.27 |
| Participants | Age | Height (m) | Weight (kg) | BMI | |
|---|---|---|---|---|---|
| Min | 24.00 | 1.67 | 59.80 | 19.31 | |
| n = 15 | Mean | 33.40 | 1.80 | 80.83 | 24.88 |
| Max | 49.00 | 1.90 | 99.00 | 30.61 |
| Test | Exercise | Description |
|---|---|---|
| 1 | Stand 1 | free standing |
| 2 | Sit 1 | sitting in a rigid office chair |
| 3 | Walk 1 | walk at 2.0 km/h on the treadmill |
| 4 | Walk 2 | walk at 4.5 km/h on the treadmill |
| 5 | Stand 2 | free standing |
| 6 | Walk 3 | walk at a self-selected pace |
| 7 | Walk 4 | walk at a self-selected pace |
| 8 | Stand 3 | free standing |
| 9 | Sit 2 | sitting in a rigid office chair |
© 2016 by the authors; licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC-BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Coates, J.; Chipperfield, A.; Clough, G. Wearable Multimodal Skin Sensing for the Diabetic Foot. Electronics 2016, 5, 45. https://doi.org/10.3390/electronics5030045
Coates J, Chipperfield A, Clough G. Wearable Multimodal Skin Sensing for the Diabetic Foot. Electronics. 2016; 5(3):45. https://doi.org/10.3390/electronics5030045
Chicago/Turabian StyleCoates, James, Andrew Chipperfield, and Geraldine Clough. 2016. "Wearable Multimodal Skin Sensing for the Diabetic Foot" Electronics 5, no. 3: 45. https://doi.org/10.3390/electronics5030045