
Investigating the Feasibility of Virtual Reality (VR) for Teaching Cardiac Morphology

Institute of Cardiovascular Science, University College London, London WC1E 6BT, UK
*
Author to whom correspondence should be addressed.
Electronics 2021, 10(16), 1889; https://doi.org/10.3390/electronics10161889
Submission received: 11 June 2021
/
Revised: 28 July 2021
/
Accepted: 4 August 2021
/
Published: 6 August 2021
(This article belongs to the Special Issue Digital Twin Technology: New Frontiers for Personalized Healthcare)
Abstract
:Congenital heart disease (CHD) is the most common defect at birth. Effective training for clinical professionals is essential in order to provide a high standard of care for patients. Visual aids for teaching complex CHD have remained mostly unchanged in recent years, with traditional methods such as diagrams and specimens still essential for delivering educational content. Diagrams and other 2D visualisations for teaching are in most cases artistic illustrations with no direct relation to true, 3D medical data. Specimens are rare, difficult for students to access and are limited to specific institutions. Digital, patient-specific models could potentially address these problems within educational programmes. Virtual Reality (VR) can facilitate the access to digital models and enhance the educational experience. In this study, we recorded and analysed the sentiment of clinical professionals towards VR when learning about CHD. A VR application (VheaRts) containing a set of patient-specific models was developed in-house. The application was incorporated into a specialised cardiac morphology course to assess the feasibility of integrating such a tool, and to measure levels of acceptance. Attendees were clinical professionals from a diverse range of specialities. VR allowed users to interact with six different patient-derived models immersed within a 3D space. Feedback was recorded for 58 participants. The general response towards the use of VR was overwhelmingly positive, with 88% of attendees rating 4 or 5 for ‘helpfulness of VR in learning CHD’ (5-points Likert scale). Additionally, 70% of participants with no prior VR experience rated 4 or 5 for ‘intuitiveness and ease of use’. Our study indicates that VR has a high level of acceptance amongst clinical trainees when used as an effective aid for learning congenital heart disease. Additionally, we noted three specific use-cases where VR offered novel teaching experiences not possible with conventional methods.
1. Introduction
Congenital heart disease (CHD) encompasses an array of distinct malformations and defects present within the heart at birth. CHD is the most common type of birth defect, with an incidence of almost 1 in 100 live births, representing the leading cause of infant morbidity and mortality [1]. Patients with CHD often present with highly variable and unique abnormalities, which despite advancements in imaging and diagnosis, remain difficult to understand. Therefore, communicating a visual understanding of these anatomical defects is especially challenging for educators in CHD.
Conventional methods of teaching the anatomy of CHD include textbooks, off-the-shelf anatomical heart models, medical images including computed tomography (CT), magnetic resonance imaging (MRI) and echocardiography, and pathological specimens. The latter in particular is considered the ‘gold standard’ resource for learning cardiac morphology [2]. Unfortunately, specimens degrade over time and their availability is limited to a few select institutions, making them inaccessible for many. Fetal specimens are especially rare in educational settings, despite a growing emphasis on earlier pre-natal detection of CHD [3]. As an alternative, 3D printed models derived from 3D images have been used for demonstrating classic CHD lesions and for practising surgical procedures [4,5]. Meanwhile, the burden of CHD continues to increase [1], likely leading to more clinicians requiring specialist training in this discipline. The use of cutting-edge technology may become necessary in the future to support this growth.
Innovations in patient-specific computational tools have enabled the possibility to convert 3D medical images into models. The in silico representation of clinical data has the potential to contribute to the realization of precision medicine with therapies tailored towards each patient. Virtual reality (VR) is a rapidly evolving technology which provides an immersive experience where users can visualise and interact with 3D objects. In the field of CHD, VR can be used to view 3D models when planning complex surgeries [6,7]. The integration of VR in courses for teaching CHD is, however, still in its infancy [8,9,10]. Current commercial solutions typically rely on artistic 3D models, not derived from 3D patient images. In addition, the high cost of individual VR headsets can be prohibitive to large scale educational activities. Due to these barriers, the average curriculum continues to be based primarily on conventional teaching methods [2].
In this study, we present a novel VR application (VheaRts) containing a library of 3D CHD models reconstructed from images. Using VheaRts, we aimed to explored the sentiment towards VR for learning CHD, and to record any scenarios where VR may allow for new and improved teaching possibilities. We hypothesised that VR would be a suitable tool to integrate within CHD training courses, and that user feedback would indicate a strongly positive sentiment towards VR. We predicted that attendees would rate the VR application highly in three qualitative metrics: helpfulness in learning CHD; intuitiveness; and willingness to continue using VR in their respective professional field.
2. Materials and Methods
VheaRts is a novel VR application designed at UCL Institute of Cardiovascular Science—Centre for Clinical Engineering. The software was developed specifically to explore 3D models of patients or pathological specimens. The application was tested in a dedicated section of the UCL ‘hands-on’ Cardiac Morphology Course. This 3-day short course has been running for the past 15 years and teaches CHD morphology to clinicians from a mix of backgrounds with the aide of anatomical specimens, all under expert guidance [11]. In order to assess the feasibility and level of acceptance of VR for teaching, we included specific digital models relevant for the sessions. The application was tested by the participants during the course, and user feedback was collected to record their response towards the usage of VR in education and cardiology.
2.1. Image Acquisition, Anatomical Specimens and 3D Models
Six patient-specific models of hearts were included in this study, one normal and a selection of 5 CHDs (Table 1). There were 2 models derived from patient CT clinical datasets (Siemens Somatom Force, 0.24 mm spatial resolution), whereas 4 were from post-mortem fetal samples (including 3 fetal specimens and 1 post-natal). Out of these four, three were imaged using micro-CT (Nikon Metrology HMX ST 225, spatial resolution of 5–125 m), with the last specimen imaged using a propagation-based, Synchrotron, X-ray phase contrast imaging technology (PB-XPCI, Paul Scherrer Institut, Switzerland).
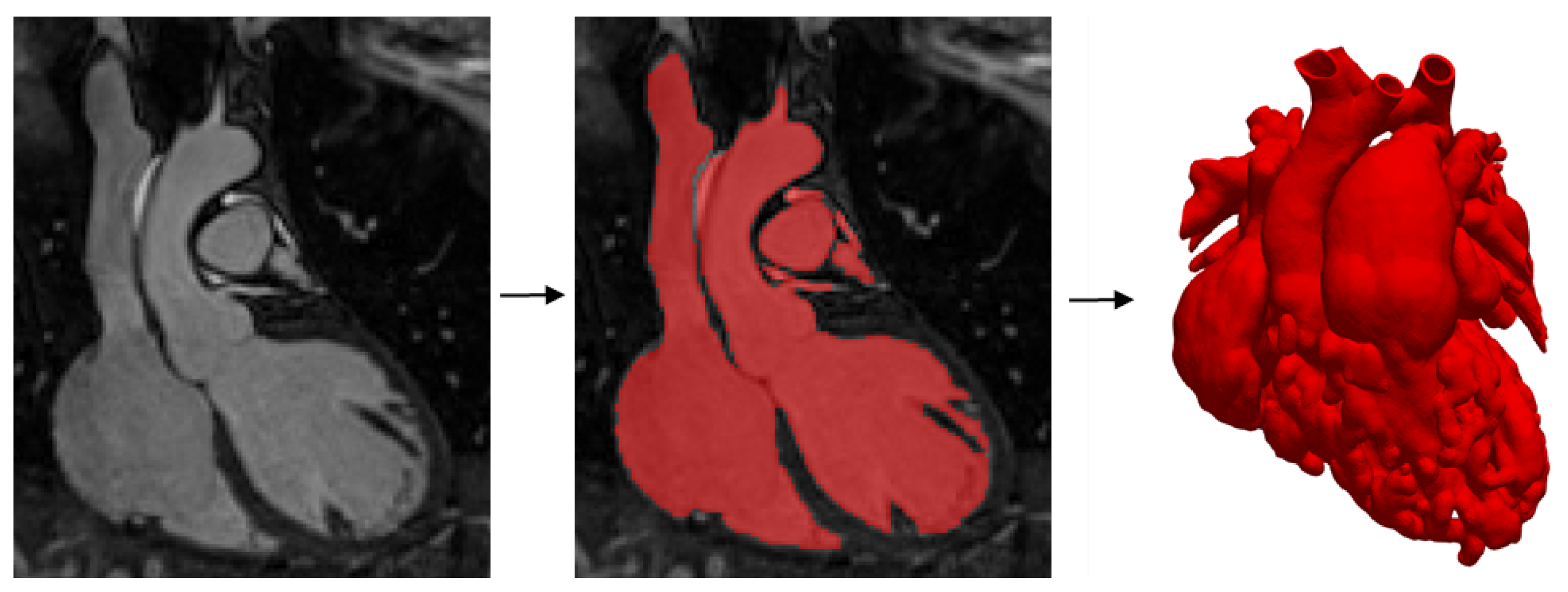
All DICOM images were segmented using commercially available software ScanIP (Simpleware, Synopsis). The main anatomical components (chambers, great arteries, valves) were segmented independently to generate separate masks. For the anatomical samples, the myocardium was reconstructed, while for the clinical images only the blood pool was segmented (Figure 1). Models were exported as surface meshes (.stl) and after further refinement, prepared for VheaRts as Wavefront.obj files.
2.2. Virtual Reality Platform
VheaRts was developed with the game engine Unity (Unity Technologies), for use with the commercial Oculus Rift/Quest headsets (Facebook Technologies). For the duration of this study, the Oculus Rift was connected to an Alienware 17 R5 gaming laptop. A specific module of VheaRts with the 6 cases was prepared. Upon entering the virtual room, the user was presented with two menus to activate digital models and the following tools:
- Handling and rotating the 3D heart models: with the controllers, the user may ‘grip’ models in 3D space and move them freely.
- Slicing the 3D heart models: with a slicing tool, the user can ‘crop’ the mesh freely in real-time. Options to clip with a plane or sphere are available (Figure 2).
- Displaying labels of structures: the main anatomical parts of each case are highlighted and labelled, and each structure can be grabbed and moved independently (Figure 2).
- Ultrasound probe simulator: when moving the probe inside the 3D model, a 2D ultrasound projection is displayed on a screen.
- Measuring and placing markers: the user may place points in 3D space in order to highlight structures and measure distances.
2.3. Feasibility Study
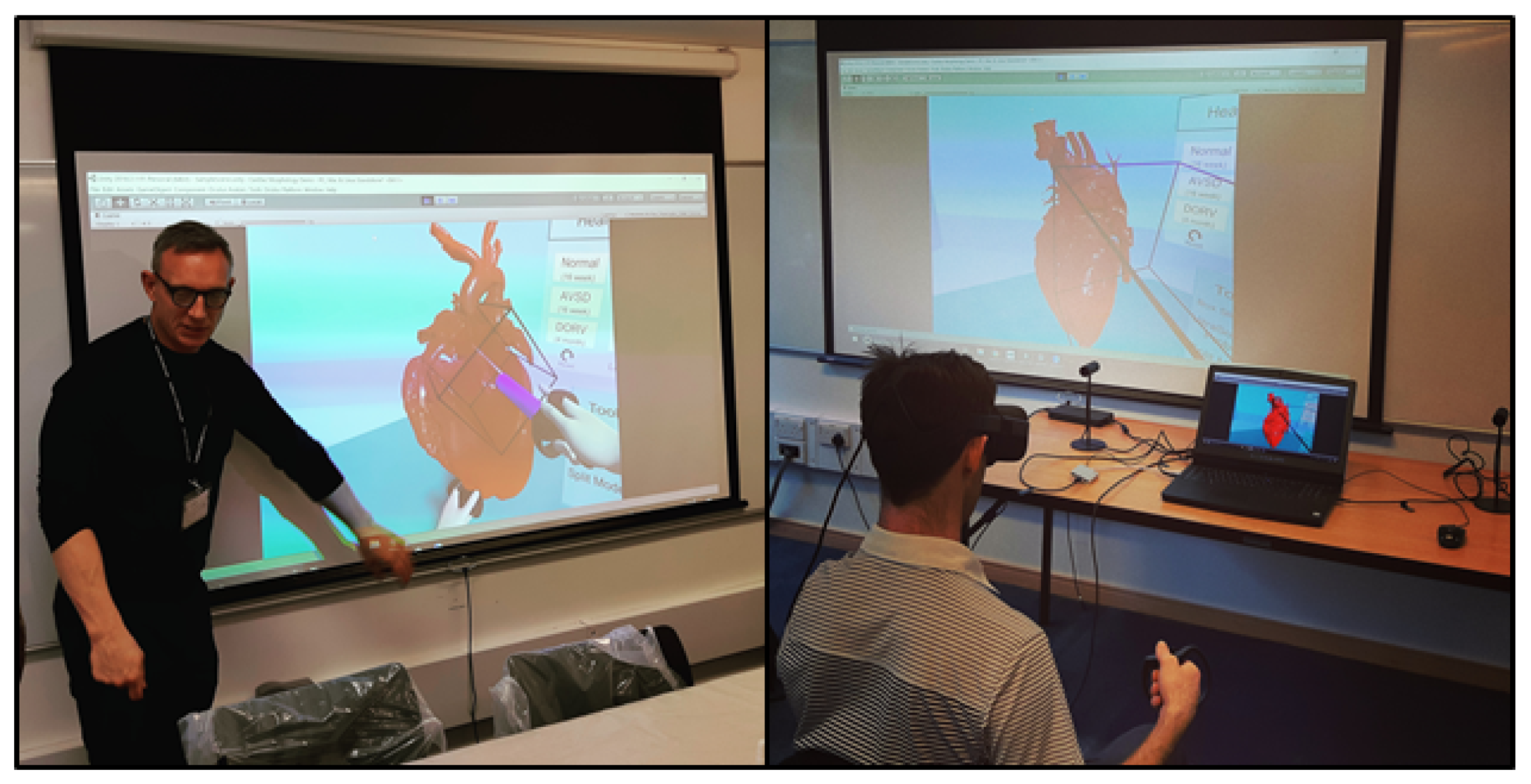
Participants to the courses that ran between October 2018 and January 2020 were invited to test VheaRts over a dedicated 2-h session. After a short adaptation period, users independently explored the contents and tools of the VR demo. The perspective of the participants was streamed live, and guidance was offered by the course’s tutors (Figure 3).
Following the VR demo, users were asked to provide feedback via a short questionnaire, designed specifically to capture the first impressions of the participants. Likert-scale type questionnaires are common for understanding the early feasibility of VR, and have been widely reported in similar studies focused on evaluating participant response to 3D technologies [12,13]. Feedback form structure varies greatly between studies; however, questions related to ‘ease of use’ and perceived ‘gained knowledge’ are frequently included [14,15]. In order to minimise any disruption to the teaching programme, we devised three 5-point Likert scale questions. Respondents were asked about: (i) the ease of interaction with both the content and tools within the virtual environment; (ii) the usefulness of the VR experience in improving the understanding of morphology for the selected CHD cases; and (iii) their willingness to implement/use VR within their respective working environment. With these three questions, we aimed to gain a preliminary understanding of how feasible the continued use of VR would be for teaching CHD. In addition, attendees were required to provide initial information related to their professional background/clinical area of expertise, and asked about any previous VR experience. Finally, an open-ended question concluded the survey to capture any further ideas and suggestions for improvement.
Responses were analysed by calculating overall average scores and exploring correlations with subgroups based on different backgrounds and previous experience. The text from open-ended responses was reviewed to identify keywords and trends. Our hypothesis was that VR would score very highly for all three questions where feedback was recorded. In addition to gathering responses, we aimed to observe specific examples where VR could be more advantageous than traditional methods such as diagrams or specimens.
3. Results
In total, 58 participants tested VheaRts over seven sessions (average = 8.3 participants per session) for ∼10 min each. Once in the virtual room, each user was guided in order to gain familiarity with the environment, models and tools. The users were then left free to explore the application in any order they wished. Users spent most of their allotted time observing anatomical structures and identifying specific defects while using different tools. Each participant examined all 6 heart models. Participants were encouraged to explore the capabilities of each tool at least once. The user perspective was always mirrored on a screen in order to address any content-related questions while the user was within VR. There were no records of bugs or unexpected software failures.
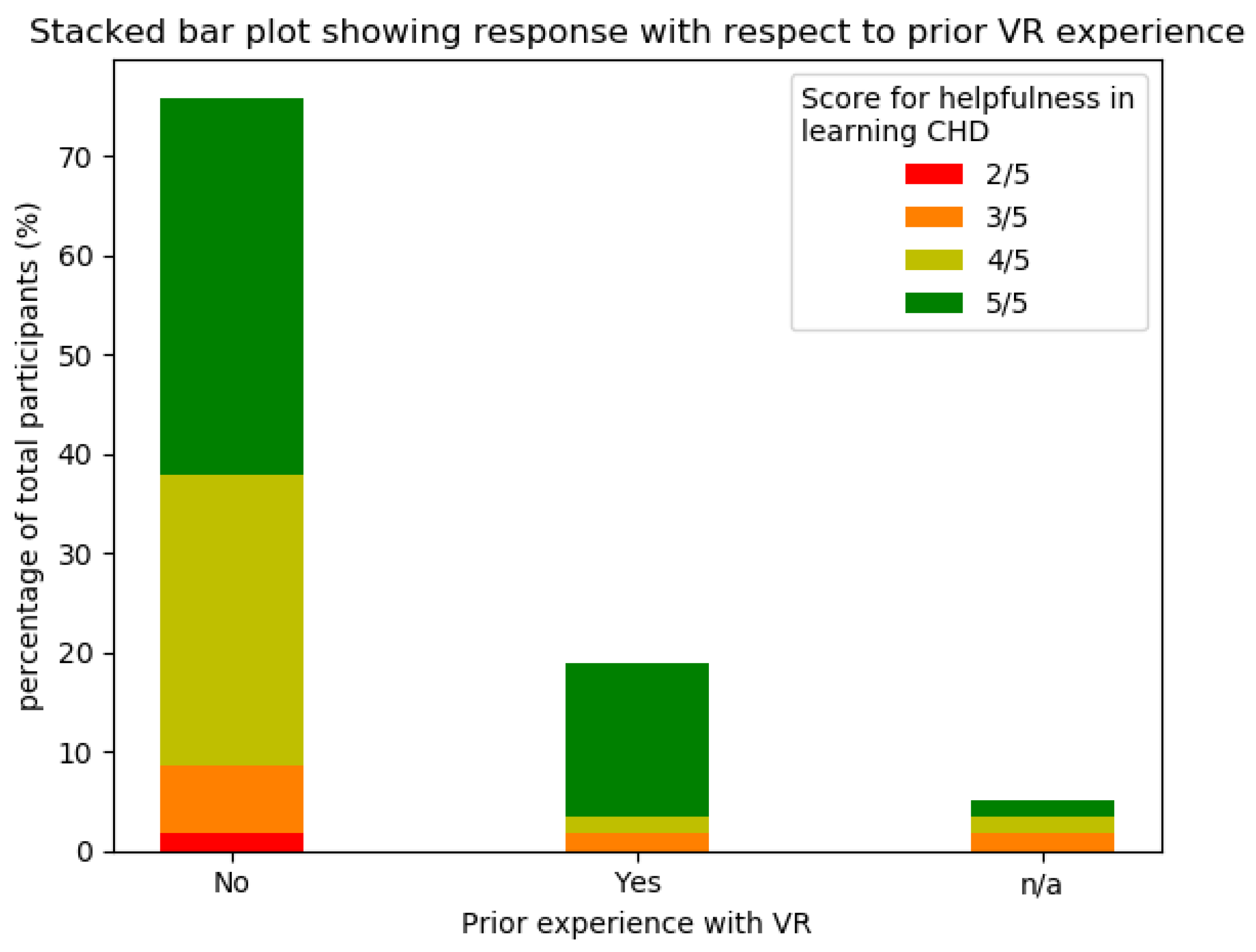
The 58 participants came from a wide array of different healthcare professions, with 20 participants listing their profession to be strongly related to cardiology (i.e., cardiology trainee/registrar/fellow, cardiac sonographer, cardiac intensive care fellow and cardiac surgeon), whilst other commonly reported disciplines included paediatrician (n = 6) and anaesthetist (n = 5). From the 58 participants, 11 had previously tried VR before (Figure 4), with 5 having tried applications related to medicine.
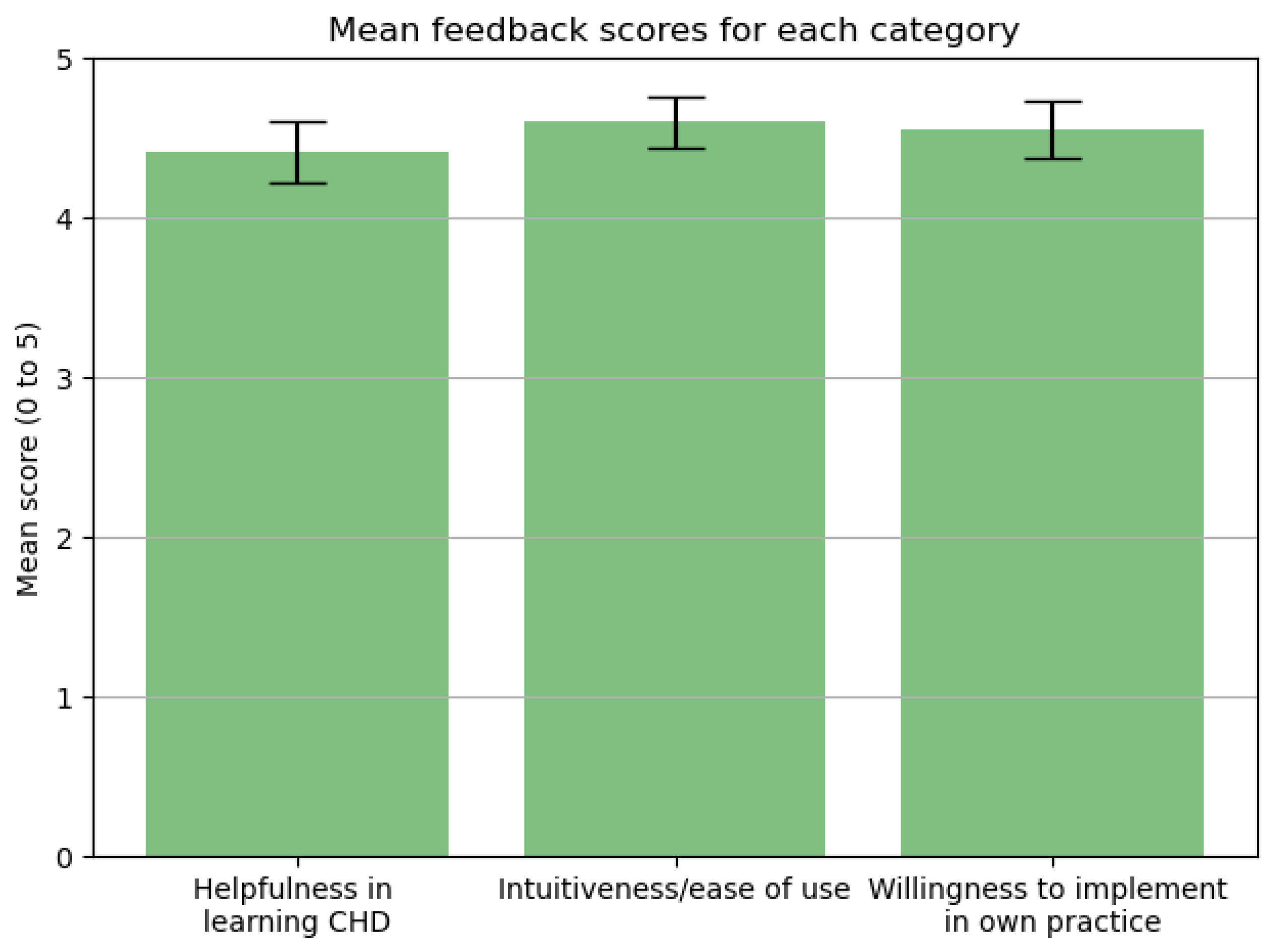
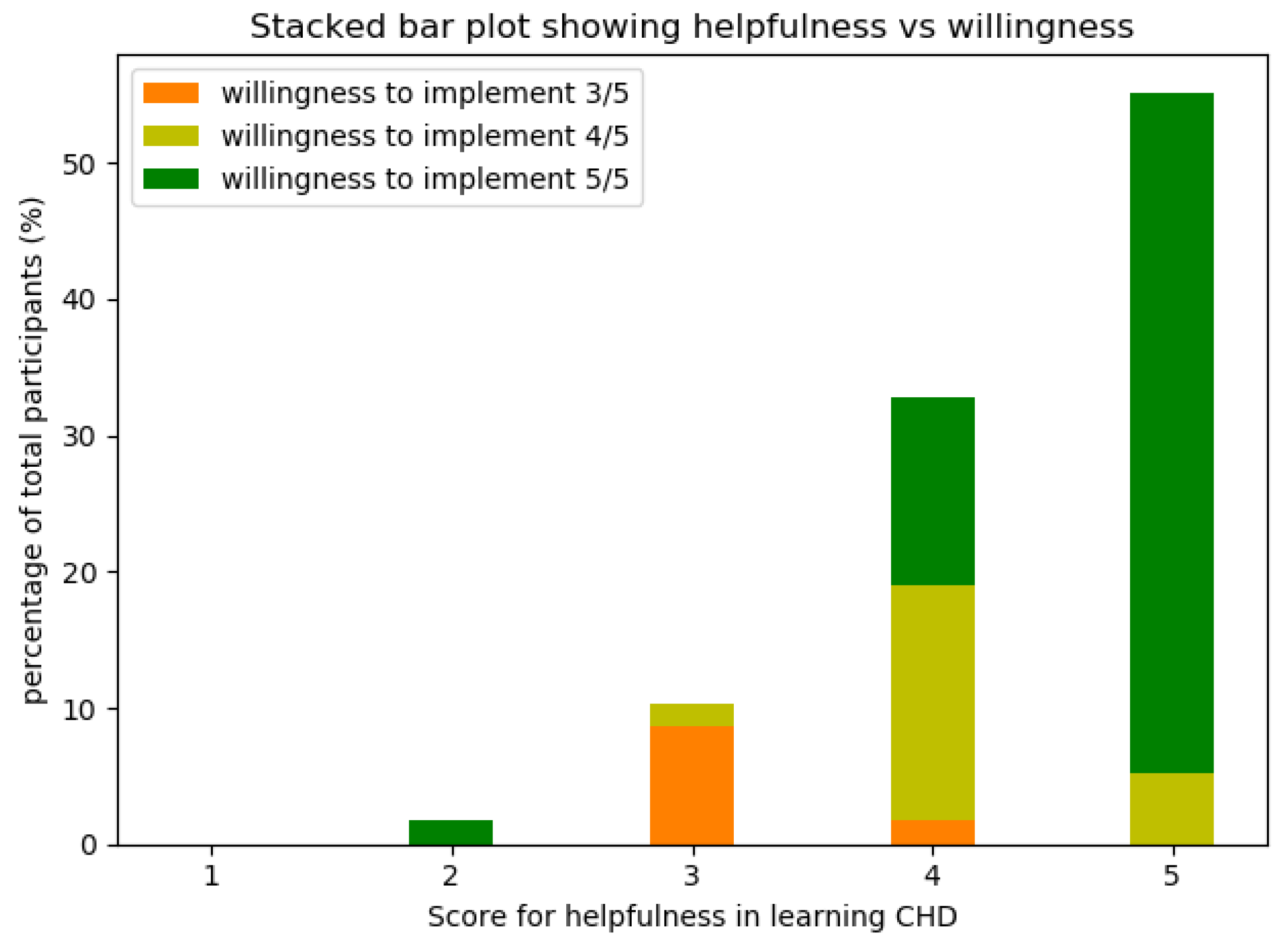
VheaRts was found to be very intuitive to use by 93% of the total participants, with an average score of 4.6 ± 0.8 SD (see Figure 5). The average recorded score for ‘helpfulness of VR’ was 4.4 ± 0.6 SD, with 88% of participants considering VR to be very helpful. Additionally, it was found non-cardiac speciality users found the application more useful than cardiac-speciality users (95% vs. 75%). Over 89% of users declared their willingness to implement VR in their clinical practice. This result is consistent with the ‘helpfulness’ scores recorded (Figure 6). Interestingly, two participants who did not find the app particularly helpful for learning CHD were still willing to incorporate VR into their clinical practice.
A total of 47 participants answered the open-ended question. From this group, 29 contained explicitly positive phrases, such as ‘extremely useful tool’ and ‘very helpful for learning CHD’. One comment was negative, and stated the headset was ‘difficult to adjust, so blurry all the time’. Participants repeatedly reported that the application was useful (n = 14), provided clear understanding of heart anatomy (n = 10) or was intuitive and easy to use (n = 9). Some future requests included: incorporating ultrasound images (n = 5), adding dynamic/beating 3D models (n = 5), improving the rendering/visualisation of intracardiac views and structures (n = 3) and including blood flow (n = 2). It was observed that the most used feature was the slicing tool.
4. Discussion
Our study analysed the feasibility of using a VR application with patient-specific heart models for education in cardiac morphology. Findings indicate that the inclusion of VR in clinical training programmes is both viable and well-received by participants. We recorded an overwhelmingly positive consensus voiced by the majority of attendees in relation to our VR app.
4.1. Virtual Reality
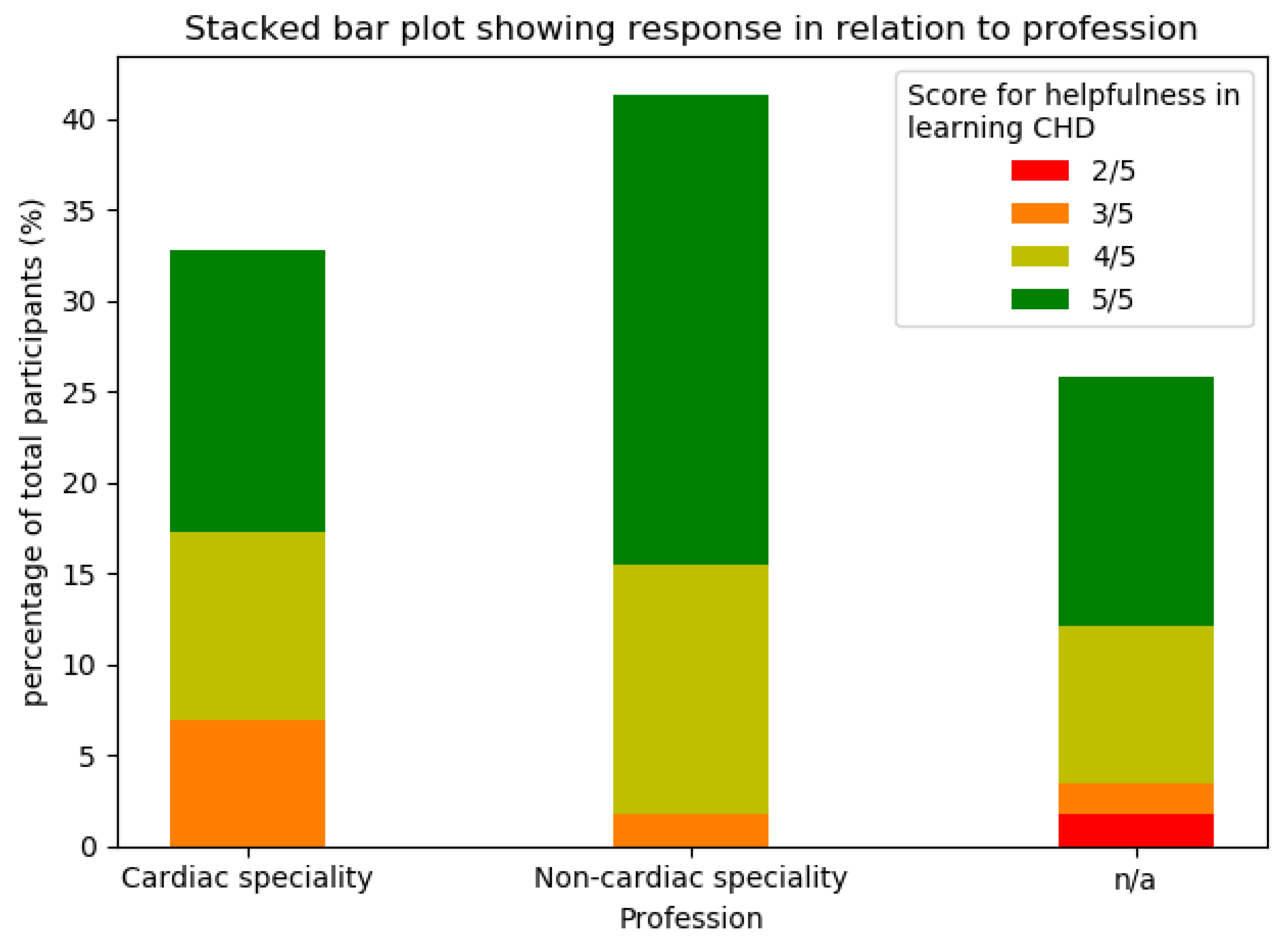
Averages for each metric were highly positive (above 4.4 out of 5). ‘Intuitiveness’ recorded the highest positive result (4.6 ± 0.6), despite 76% of attendees having had no prior experience with VR technologies. ‘Helpfulness for learning CHD’ displayed a lower mean value and a wider range of responses (i.e., 4.4 ± 0.8), likely due to the highly mixed professional backgrounds of the course participants, and therefore the wide range of experience and knowledge in CHD. From Figure 4, 82% of users with prior VR experience voted 5 for ‘helpfulness’ whereas only 50% of users with no prior VR experience voted 5 for ‘helpfulness’. This may suggest that users with VR experience are better prepared to interpret the content, as the initial novelty and unfamiliarity when using VR has been reduced/removed [16]. From Figure 7, it can be seen non-cardiac speciality attendees reported the application to be slightly more helpful on average, which is expected, as they had a weaker foundation in CHD before starting the course.
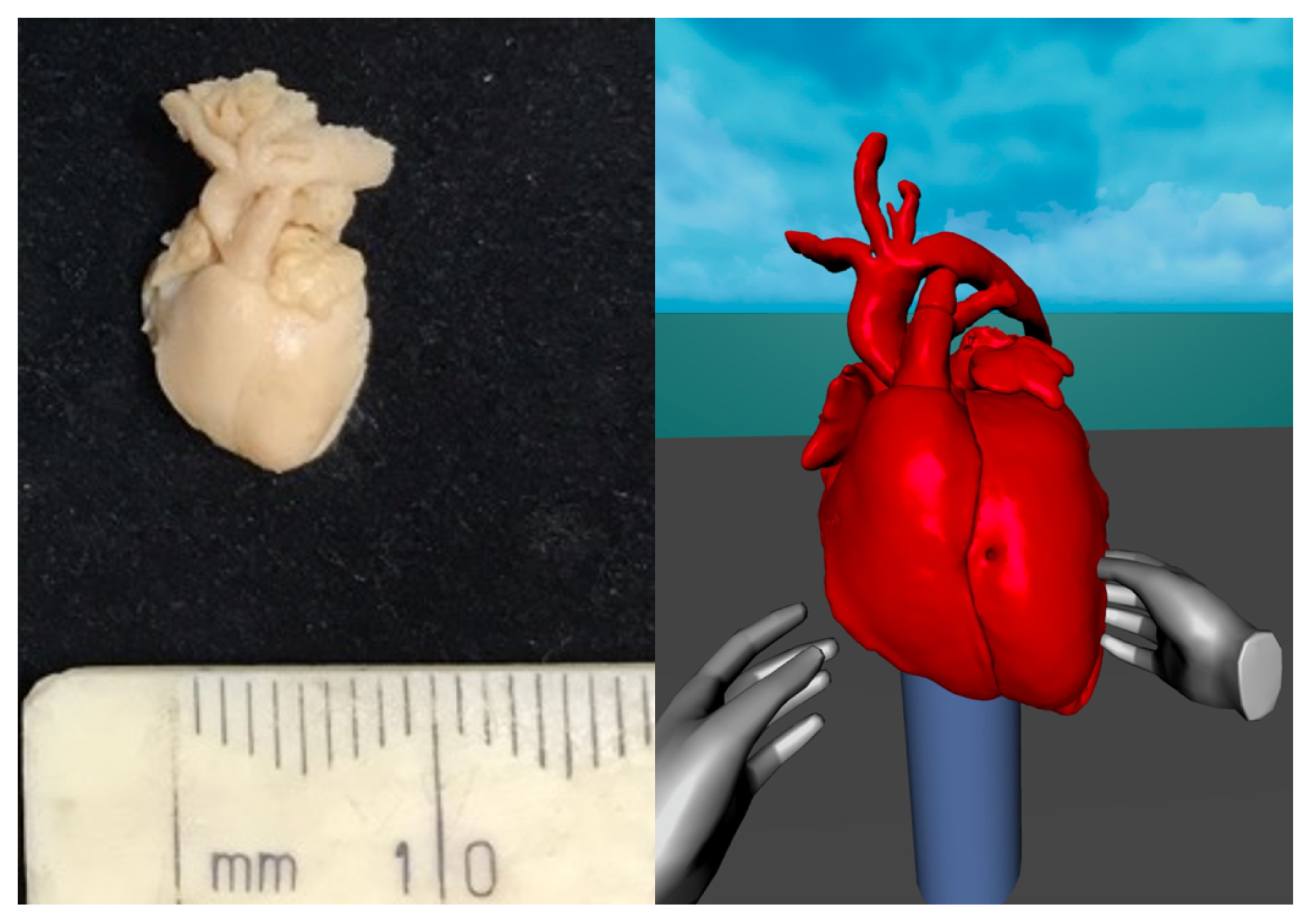
When using the application, users often commented positively on the ability to scale up models multiple times their original size. This is particularly advantageous for fetal heart specimens, which are difficult to fully inspect with the naked eye (Figure 8). Students also appreciated the possibility to easily view the hearts from any perspective, and explore the intracardiac structures in detail with ease. The most frequently used feature was the slicing tool. The ability to orientate the cutting plane with 6 degrees of freedom allowed for complete control over intracardiac exploration. We feel this freedom may enable the student to develop a stronger visual comprehension of the anatomical structures, due to the experience being immersive and self-driven. In the future, technology such as haptic gloves may enable even more realistic physical interactions within VR. This will allow for more believable clinical simulations and training experiences.
4.2. Discovery of Novel Pedagogy in Congenital Heart Disease Using VR
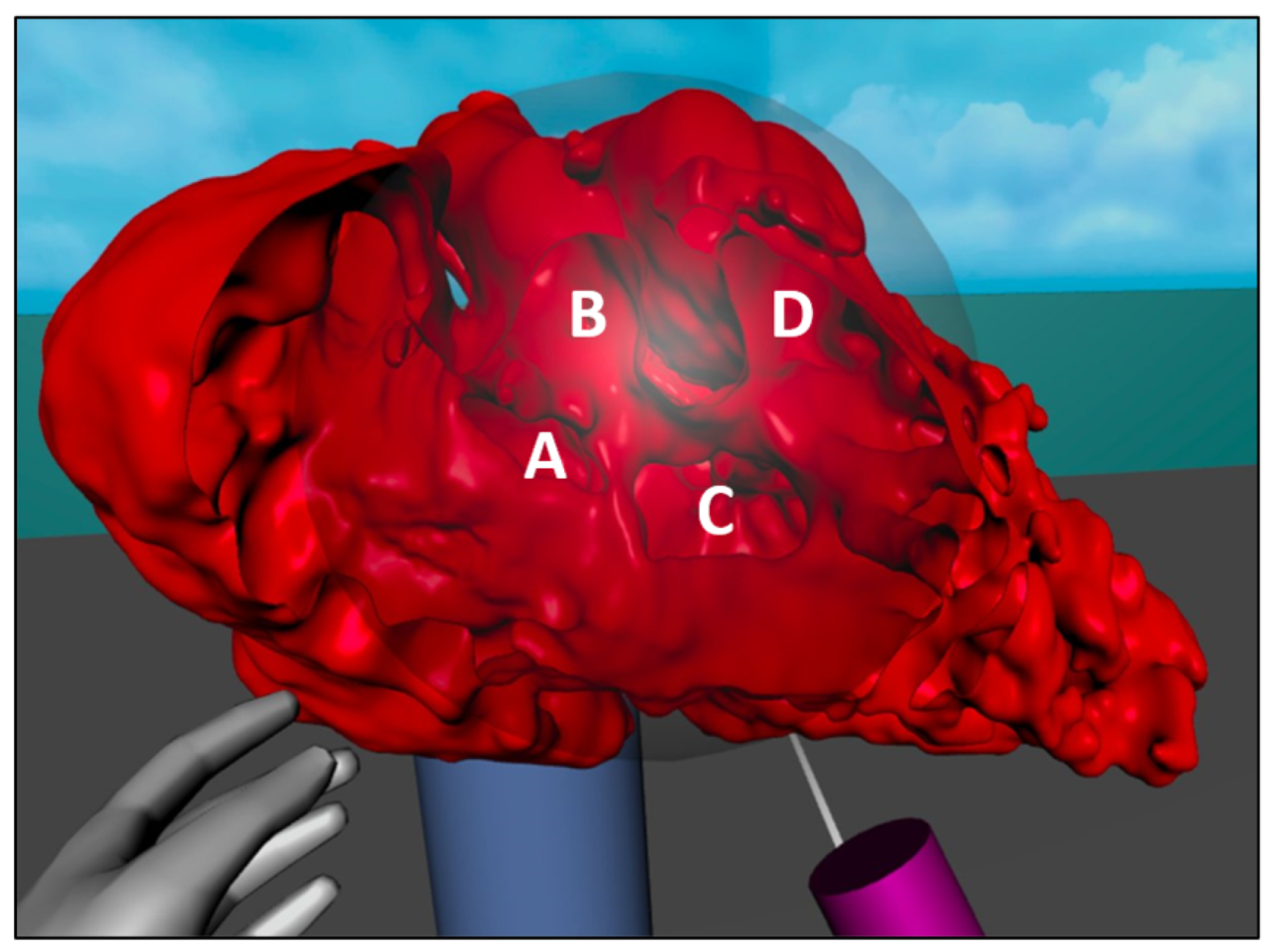
Unexpected educational uses of VR for specific pathologies were observed during the sessions. The three main examples are here reported and commented. Firstly, the sphere slicer was found to be particularly useful in the DORV specimen visualisation, as it allowed observation of ventriculo-arterial (VA) connections and septal defects at once on the curved cutting plane (Figure 9). This is much more intuitive and easy to accomplish in VheaRts than in conventional imaging, where the user may have to manipulate three orthogonal planes to reach an equivalent perspective, while reconstructing the 3D view in their head. Secondly, VheaRts was found to be useful for mapping out the electrical conduction system in the heart with markers, particularly in specimens with uncommon or multiple septal defects such as in the AVSD subject (Figure 10). After tracing the pathway, the heart could be removed to leave only the conduction system tracks drawn in 3D space. Finally, VheaRts demonstrated that it could be used for precisely assessing the origin of the great arteries. In TOF case, tracing the roots of the great vessels showed that the case could be described to be presenting with DORV in addition to TOF. This is because aortic root was found to mostly originate from the right ventricle (Figure 11).
4.3. Limitations of Study
This study reports a pilot single centre experience of using VR in educational settings. Over the course of the VR sessions, certain limitations became evident whilst recording data, and these should be addressed in future studies. First of all, the software is still under development and features will continue to be added to further enhance the learning experience. Feedback collected in this study will be used to shape the future version of the software, which is developed using an approach based open innovation methodologies [17]. Therefore, with certain improvements, greater possibilities of VR can be tested and evaluated as feedback is collated. In addition, the study was conducted on a relatively small group of participants. In the future, we will enlarge the number of respondents and the questions of the survey will more thoroughly investigate the level of added knowledge that VR may contribute to. This will be achieved by assessing two groups, one with access to VR and the other without, in a similar fashion to reports from other centres [14,18]. Furthermore, the Likert-scale questions can be improved, by increasing the point range and adding more detail. For example, more specific questions may be included, such as ‘I feel like I have more concentration when using VR training (rank 1–7)’ [15]. This will help to better understand how and where VR yields the most improvements. Furthermore, the use of VR in medical education should be investigated in other fields, such as for surgical training and interventions [6,19]. Follow-up studies of this kind will help us understand which subsets of clinical training/education are suitable for VR. It will be increasingly important to collect more precise demographic data (e.g., years of experience, profession, age) as more people are recruited, in order to identify more detailed trends.
4.4. The Future of VR in Clinics and Teaching
In this study, we presented a successful application using a digital library of patient-specific models to teach cardiac morphology, heart development and CHD. The creation of a repository of digital models of patient cases and biological specimens has three main advantages. Firstly, it enables the preservation of pathological samples, including highly rare and difficult to acquire fetal cases. Secondly, it makes the models widely accessible to a growing community of practitioners. Finally, 3D models allow for more varied viewing possibilities which may not otherwise be achievable without damaging the sample (applies particularly to fetal specimens). These new opportunities may enable educators of cardiac morphology to develop new pedagogy within CHD.
Digital models of cardiovascular diseases also have the potential to improve clinical diagnosis and personalised treatment pathways; however, complete translation to cardiovascular medicine is still in its infancy. Virtual Reality may yet prove to be an integral component in the pipeline of a ‘digital twin’ model for surgical interventions [20]. In healthcare, the ‘digital twin’ denotes the vision of a comprehensive, virtual tool that integrates coherently and dynamically the clinical data acquired over time for an individual using mechanistic and statistical models [21]. One of the current limitations of VR as a digital twin device in healthcare is the lack of real-time 3D image data, and the requirement for manual data processing to produce segmented models [22]. In the future, Automatic segmentation and computational simulations could be combined with VR to produce a multiscale digital twin model for patient evaluation and pre-operative planning. However, as VR and digital twin technology in healthcare is still emerging, testing these pipelines within clinical settings remains difficult. Therefore, education/training provides a more accessible entry point into the clinical environment. This may open up the possibility to extend VR towards more treatment-based applications in the future. It is predicted that patient-specific modelling will grow to be increasingly important in training, especially if it becomes more accessible through automatic data-processing pipelines [23].
5. Conclusions
In this study, we have recorded and analysed the sentiment of clinical professionals towards VR when learning about cardiac morphology. The feedback retrieved from our surveys displayed an overwhelmingly positive response in all the categories we measured (helpfulness, intuitiveness, willingness for continued use), which is in agreement with our hypothesis. This suggests that VR is a suitable technology for integration within clinical training programmes. The graphical clipping tool was most commonly used by attendees. Non-cardiac speciality participants reported a higher level of satisfaction than cardiac clinical professionals. We have also found three new learning techniques for CHD, which are specific to VR and not possible in post-mortem specimens. Overall, the integration of VR within a specialised course for training was simple to set-up and well-received by students. As VR hardware becomes more affordable, we predict that widespread adoption of VR in anatomical education will become commonplace. Future research in this field should aim to quantify the level of benefit VR provides in teaching CHD.
Author Contributions
Conceptualization, E.P., S.S., E.S., A.C. and C.C.; data curation: E.S., A.C. and C.C.; formal analysis: E.P.; funding acquisition: S.S. and C.C.; resources: A.C.; software: E.P.; supervision: S.S., E.S. and C.C.; writing—original draft: E.P.; writing—review and editing: S.S., E.S., A.C. and C.C. All authors have read and agreed to the published version of the manuscript.
Funding
We acknowledge La Fondation (of Dassault Systemes), British Heart Foundation (BHF), the Engineering and Physical Sciences Research Council (EPSRC) and the European Research Council (ERC) for their funding, contributions and support towards the advancement of this project.
Conflicts of Interest
The authors declare no conflict of interest.
References
- Liu, Y.; Chen, S.; Zühlke, L.; Black, G.C.; Choy, M.K.; Li, N.; Keavney, B.D. Global birth prevalence of congenital heart defects 1970–2017: Updated systematic review and meta-analysis of 260 studies. Int. J. Epidemiol. 2019, 48, 455–463. [Google Scholar] [CrossRef]
- Estai, M.; Bunt, S. Best teaching practices in anatomy education: A critical review. Ann. Anat. Anat. Anz. 2016, 208, 151–157. [Google Scholar] [CrossRef]
- Fung, A.; Manlhiot, C.; Naik, S.; Rosenberg, H.; Smythe, J.; Lougheed, J.; Mondal, T.; Chitayat, D.; McCrindle, B.W.; Mital, S. Impact of prenatal risk factors on congenital heart disease in the current era. J. Am. Heart Assoc. 2013, 2, e000064. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Smerling, J.; Marboe, C.C.; Lefkowitch, J.H.; Pavlicova, M.; Bacha, E.; Einstein, A.J.; Naka, Y.; Glickstein, J.; Farooqi, K.M. Utility of 3D printed cardiac models for medical student education in congenital heart disease: Across a spectrum of disease severity. Pediatr. Cardiol. 2019, 40, 1258–1265. [Google Scholar] [CrossRef]
- Lau, I.; Sun, Z. Three-dimensional printing in congenital heart disease: A systematic review. J. Med Radiat. Sci. 2018, 65, 226–236. [Google Scholar] [CrossRef] [PubMed]
- Sadeghi, A.H.; Bakhuis, W.; Van Schaagen, F.; Oei, F.B.; Bekkers, J.A.; Maat, A.P.; Mahtab, E.A.; Bogers, A.J.; Taverne, Y.J. Immersive 3D virtual reality imaging in planning minimally invasive and complex adult cardiac surgery. Eur. Heart J. Digit. Health 2020, 1, 62–70. [Google Scholar] [CrossRef]
- Milano, E.G.; Pajaziti, E.; Sauvage, E.; Cook, A.; Schievano, S.; Mortensen, K.H.; Taylor, A.M.; Marek, J.; Kostolny, M.; Capelli, C. Taking surgery out of reality: A virtual journey into double outlet right ventricle. Circ. Cardiovasc. Imaging 2019, 12, e009297. [Google Scholar] [CrossRef] [PubMed]
- Sacks, L.D.; Axelrod, D.M. Virtual reality in pediatric cardiology: Hype or hope for the future? Curr. Opin. Cardiol. 2020, 35, 37–41. [Google Scholar] [CrossRef]
- Ong, C.S.; Krishnan, A.; Huang, C.Y.; Spevak, P.; Vricella, L.; Hibino, N.; Garcia, J.R.; Gaur, L. Role of virtual reality in congenital heart disease. Congenit. Heart Dis. 2018, 13, 357–361. [Google Scholar] [CrossRef] [PubMed]
- Kim, B.; Loke, Y.-H.; Mass, P.; Irwin, M.R.; Capeland, C.; Olivieri, L.; Krieger, A. A novel virtual reality medical image display system for group discussions of congenital heart disease: Development and usability testing. JMIR Cardio 2020, 4, e20633. [Google Scholar] [CrossRef] [PubMed]
- UCL. Short Courses, UCL, Hands-on Cardiac Morphology Course. Available online: https://www.ucl.ac.uk/cardiovascular/study/short-courses (accessed on 14 April 2021).
- Wheeler, G.; Deng, S.; Pushparajah, K.; Schnabel, J.A.; Simpson, J.M.; Gomez, A. P1417 Acceptability of a virtual reality system for examination of congenital heart disease patients. Eur. Heart J. Cardiovasc. Imaging 2020, 21, 319–849. [Google Scholar] [CrossRef]
- Loke, Y.H.; Harahsheh, A.S.; Krieger, A.; Olivieri, L.J. Usage of 3D models of tetralogy of Fallot for medical education: Impact on learning congenital heart disease. BMC Med. Educ. 2017, 17, 54. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Iqbal, M.S.; Kipps, A.K.; Axelrod, D.M. Using virtual reality heart models to teach congenital heart disease to trainees. Acad. Pediatr. 2020, 20, e15–e16. [Google Scholar] [CrossRef]
- Tang, Y.M.; Ng, G.W.Y.; Chia, N.H.; So, E.H.K.; Wu, C.H.; Ip, W.H. Application of virtual reality (vr) technology for medical practitioners in type and screen (t&s) training. J. Comput. Assist. Learn. 2021, 37, 359–369. [Google Scholar]
- Moro, C.; Štromberga, Z.; Raikos, A.; Stirling, A. The effectiveness of virtual and augmented reality in health sciences and medical anatomy. Anat. Sci. Educ. 2017, 10, 549–559. [Google Scholar] [CrossRef] [Green Version]
- Nambisan, S.; Siegel, D.; Kenney, M. On open innovation, platforms, and entrepreneurship. Strateg. Entrep. J. 2018, 12, 354–368. [Google Scholar] [CrossRef]
- Maresky, H.S.; Oikonomou, A.; Ali, I.; Ditkofsky, N.; Pakkal, M.; Ballyk, B. Virtual reality and cardiac anatomy: Exploring immersive three-dimensional cardiac imaging, a pilot study in undergraduate medical anatomy education. Clin. Anat. 2019, 32, 238–243. [Google Scholar] [CrossRef]
- Goo, H.W.; Park, S.J.; Yoo, S.J. Advanced medical use of three-dimensional imaging in congenital heart disease: Augmented reality, mixed reality, virtual reality, and three-dimensional printing. Korean J. Radiol. 2020, 21, 133–145. [Google Scholar] [CrossRef]
- Rasheed, A.; San, O.; Kvamsdal, T. Digital twin: Values, challenges and enablers from a modeling perspective. IEEE Access 2020, 8, 21980–22012. [Google Scholar] [CrossRef]
- Corral-Acero, J.; Margara, F.; Marciniak, M.; Rodero, C.; Loncaric, F.; Feng, Y.; Gilbert, A.; Fernandes, J.F.; Bukhari, H.A.; Wajdan, A.; et al. The ‘Digital Twin’ to enable the vision of precision cardiology. Eur. Heart J. 2020, 41, 4556–4564. [Google Scholar] [CrossRef]
- Ahmed, H.; Devoto, L. The potential of a digital twin in surgery. Surg. Innov. 2020. [Google Scholar] [CrossRef] [PubMed]
- Harrison, C.M.; Gosai, J.N. Simulation-based training for cardiology procedures: Are we any further forward in evidencing real-world benefits? Trends Cardiovasc. Med. 2017, 27, 163–170. [Google Scholar] [CrossRef] [PubMed]
Figure 1.
The process of segmentation for producing 3D models from patient images. The region of interest is manually labelled to produce a 3D ‘mask’.
Figure 1.
The process of segmentation for producing 3D models from patient images. The region of interest is manually labelled to produce a 3D ‘mask’.

Figure 2.
The VR application environment, showing a model with anatomical labels (left), and the same model being cropped with the “sphere” slicing tool.
Figure 2.
The VR application environment, showing a model with anatomical labels (left), and the same model being cropped with the “sphere” slicing tool.

Figure 3.
The typical VR set-up used in the Cardiac Morphology teaching sessions.

Figure 4.
Comparing the spread of scores for ‘helpfulness’ between groups with VR experience and groups without VR experience (n = 58).
Figure 4.
Comparing the spread of scores for ‘helpfulness’ between groups with VR experience and groups without VR experience (n = 58).

Figure 5.
Overall mean scores for 3 metrics (maximum = 5) gathered from surveys, with error bars signifying 95% confidence intervals.
Figure 5.
Overall mean scores for 3 metrics (maximum = 5) gathered from surveys, with error bars signifying 95% confidence intervals.

Figure 6.
Stacked bar plot depicting the relationship between scores for ‘helpfulness’ and ‘willingness to implement’ (n = 58).
Figure 6.
Stacked bar plot depicting the relationship between scores for ‘helpfulness’ and ‘willingness to implement’ (n = 58).

Figure 7.
Stacked bar plot showing the difference in responses for ‘helpfulness’ between cardiac vs. non-cardiac speciality groups (n = 58).
Figure 7.
Stacked bar plot showing the difference in responses for ‘helpfulness’ between cardiac vs. non-cardiac speciality groups (n = 58).

Figure 8.
The normal 16 week specimen with roughly 1cm bounds, compared against its 3D model in VheaRts, which can be scaled up freely.
Figure 8.
The normal 16 week specimen with roughly 1cm bounds, compared against its 3D model in VheaRts, which can be scaled up freely.

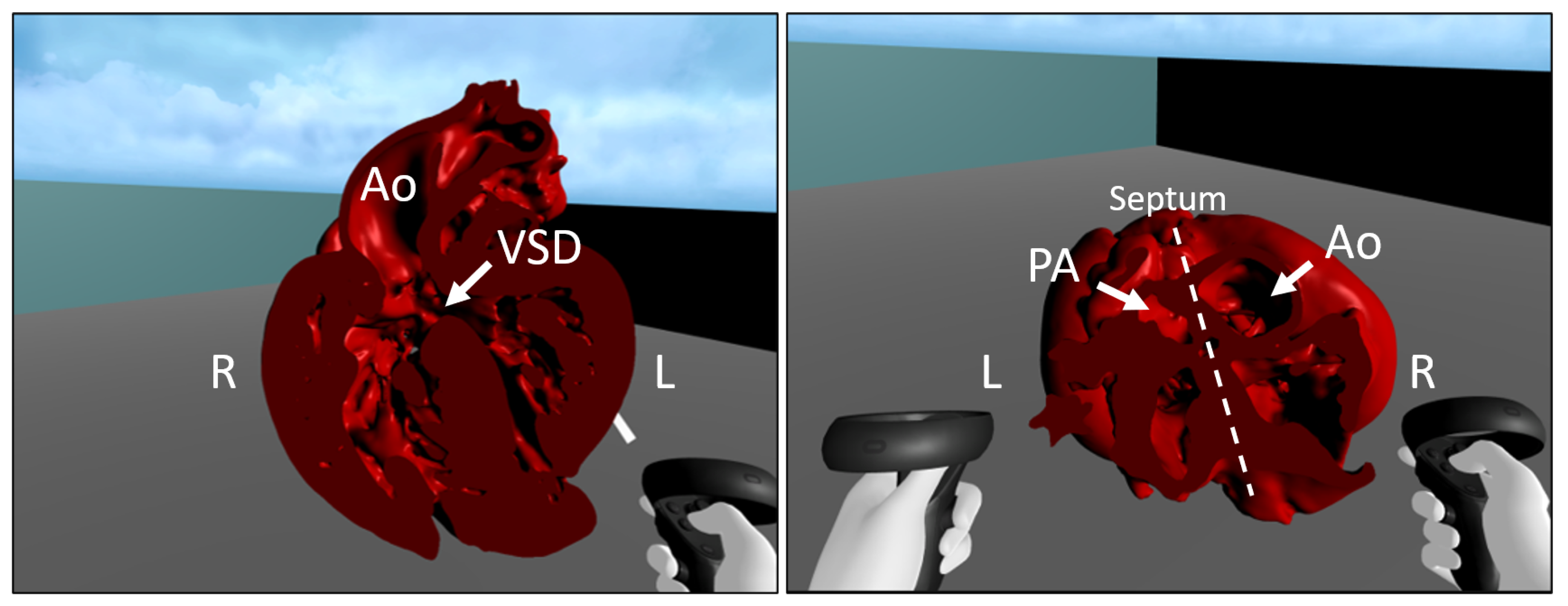
Figure 9.
Using the sphere slicer for a unique right-sided view in DORV. (A) ASD, (B) Aortic root, (C) VSD/interventricular communication, and (IVC) (D) Right ventricular outflow tract and pulmonary artery root.
Figure 9.
Using the sphere slicer for a unique right-sided view in DORV. (A) ASD, (B) Aortic root, (C) VSD/interventricular communication, and (IVC) (D) Right ventricular outflow tract and pulmonary artery root.

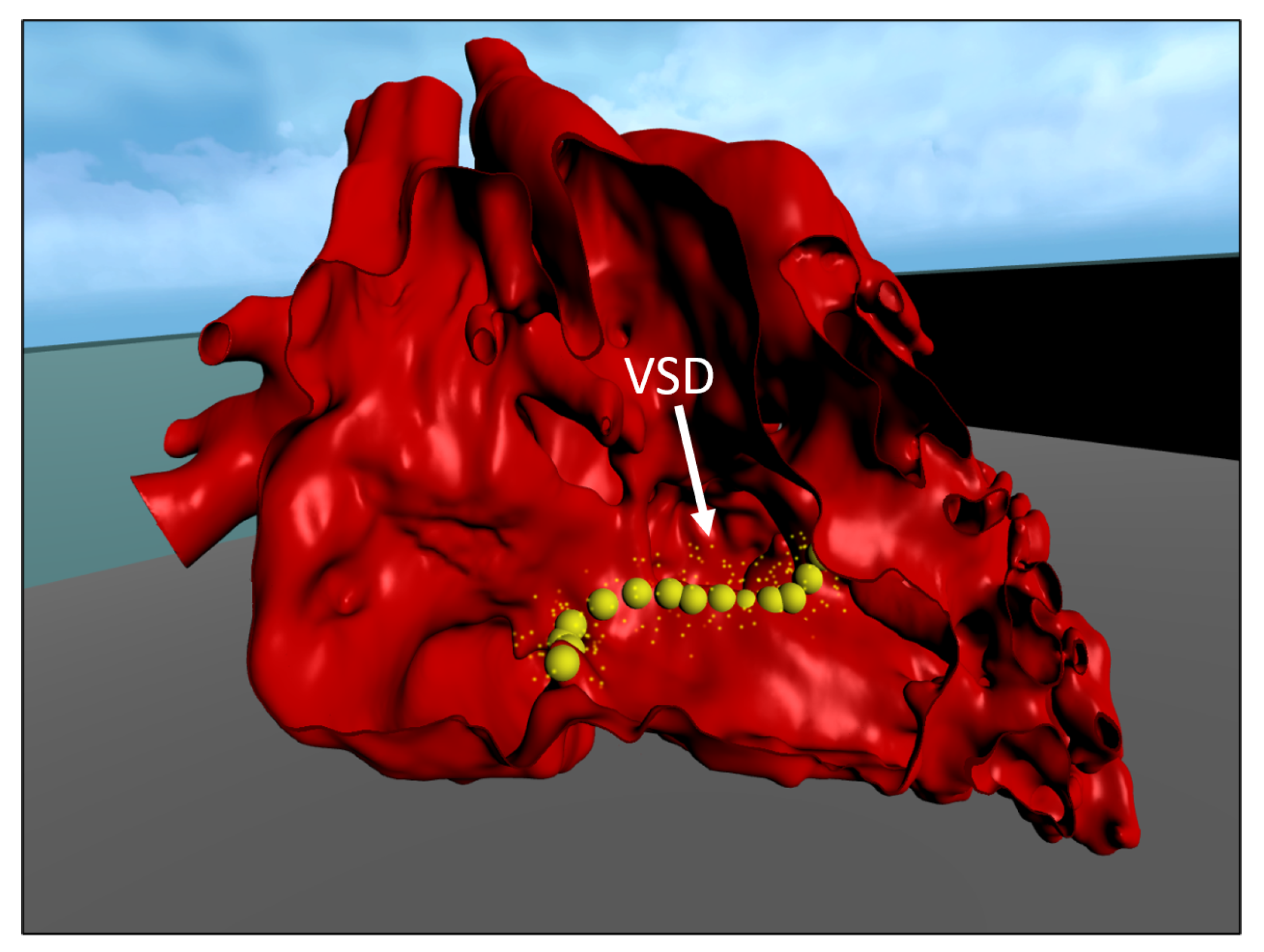
Figure 10.
Possible conduction system routes mapped out around the VSD in 3D for the DORV specimen, achieved using the slicer and marking tools.
Figure 10.
Possible conduction system routes mapped out around the VSD in 3D for the DORV specimen, achieved using the slicer and marking tools.

Figure 11.
Use of the slicer for evaluating VA connections. Left: four chamber view of the Tetralogy of Fallot (TOF) specimen showing how the aorta override is largely positioned over the right ventricle. Right: short-axis view of the same specimen, again showing the aorta to originate predominantly from the right ventricle.
Figure 11.
Use of the slicer for evaluating VA connections. Left: four chamber view of the Tetralogy of Fallot (TOF) specimen showing how the aorta override is largely positioned over the right ventricle. Right: short-axis view of the same specimen, again showing the aorta to originate predominantly from the right ventricle.


{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Table 1.
All image datasets converted into 3D models and used in this study. Note: age of the subject is recorded at time of image acquisition (for non-specimen hearts), otherwise it is the post-mortem age (for specimens).
Table 1.
All image datasets converted into 3D models and used in this study. Note: age of the subject is recorded at time of image acquisition (for non-specimen hearts), otherwise it is the post-mortem age (for specimens).
| Pathology | Specimen | Modality | Age |
|---|---|---|---|
| None (Normal) | Yes | Micro-CT | 16 weeks gestation’ |
| Atrioventricular Septal Defect (AVSD) | Yes | Micro-CT | 16 weeks gestation’ |
| Tetralogy of Fallot (TOF) | Yes | Micro-CT | post-natal |
| Transposition of Great Arteries (TGA) | Yes | Synchrotron | 16 weeks gestation’ |
| Double Outlet Right Ventricle (DORV) | No | CT | 4 months |
| Patent Ductus Arteriosus (PDA) | No | CT | 12 months |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
MDPI and ACS Style
Pajaziti, E.; Schievano, S.; Sauvage, E.; Cook, A.; Capelli, C. Investigating the Feasibility of Virtual Reality (VR) for Teaching Cardiac Morphology. Electronics 2021, 10, 1889. https://doi.org/10.3390/electronics10161889
AMA Style
Pajaziti E, Schievano S, Sauvage E, Cook A, Capelli C. Investigating the Feasibility of Virtual Reality (VR) for Teaching Cardiac Morphology. Electronics. 2021; 10(16):1889. https://doi.org/10.3390/electronics10161889
Chicago/Turabian StylePajaziti, Endrit, Silvia Schievano, Emilie Sauvage, Andrew Cook, and Claudio Capelli. 2021. "Investigating the Feasibility of Virtual Reality (VR) for Teaching Cardiac Morphology" Electronics 10, no. 16: 1889. https://doi.org/10.3390/electronics10161889
Note that from the first issue of 2016, this journal uses article numbers instead of page numbers. See further details here.