
Analysis of Optical Coherence Tomography (OCT) and Optical Coherence Tomography Angiography (OCTA) Parameters in Young Adults after SARS-CoV-2 Infection (COVID-19) Compared with Healthy Young Controls
 , , , , , ,
, , , , , ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Ethics
2.2. Study Design
2.3. Participants
2.4. Data Acquisition
- OCT (structural):
- ○
- Macula cube scan (6.4 mm × 6.4 mm): Retinal thickness (THK) from internal limiting membrane (ILM) to Bruch’s membrane (BM), retinal volume (VOL) from ILM to BM
- ○
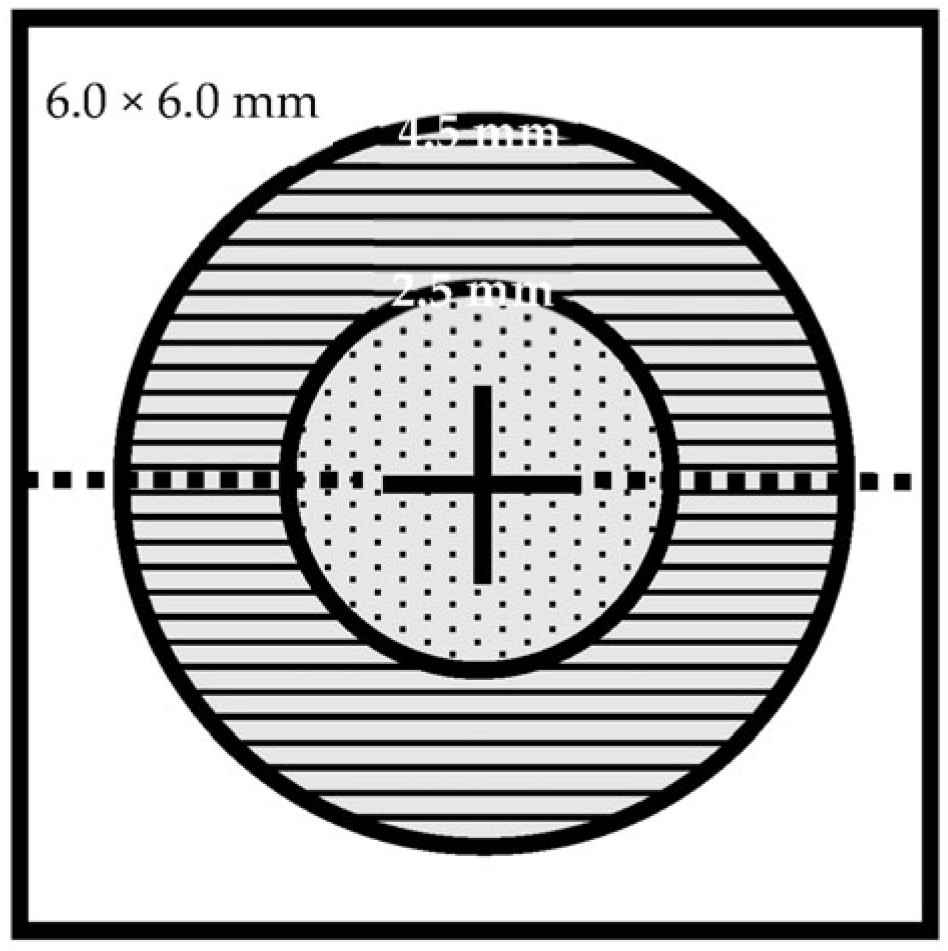
- Optic disc cube scan (6 mm × 6 mm): Retinal nerve fiber layer (RNFL) rim THK from ILM to RNFL, rim VOL
- OCTA:
- ○
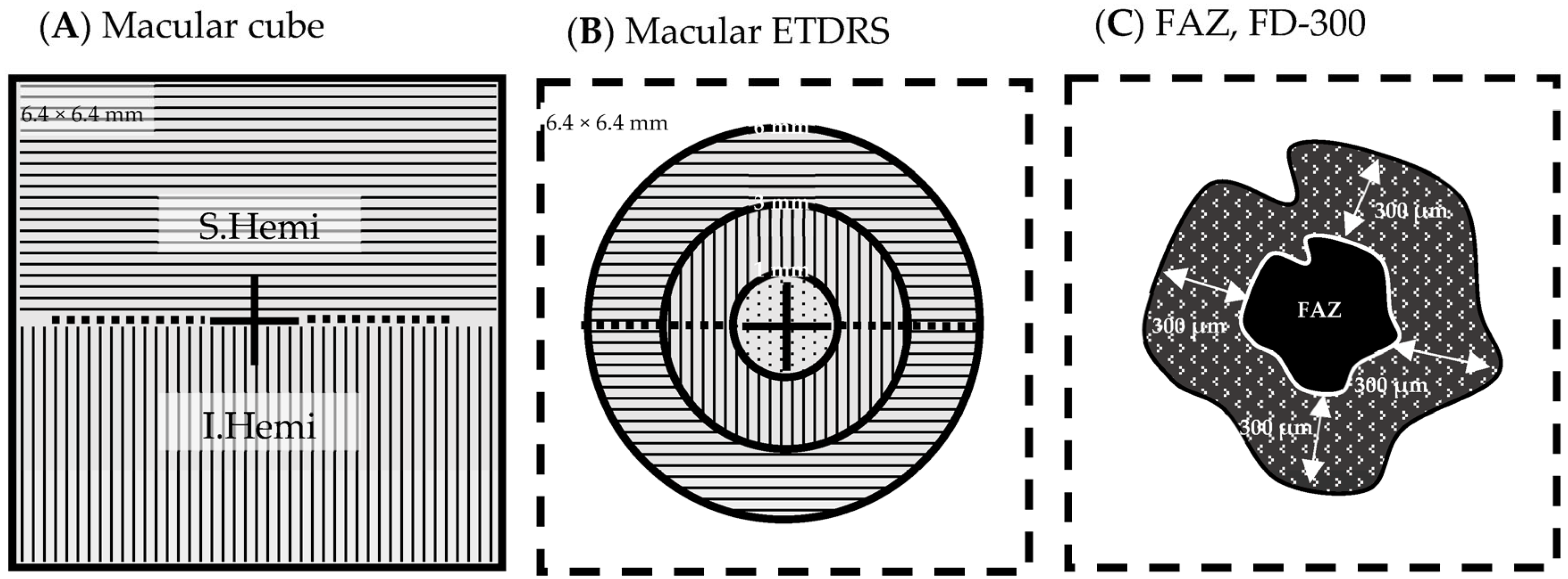
- Macula cube scan (6.4 mm × 6.4 mm) vessel density:
- ⯀
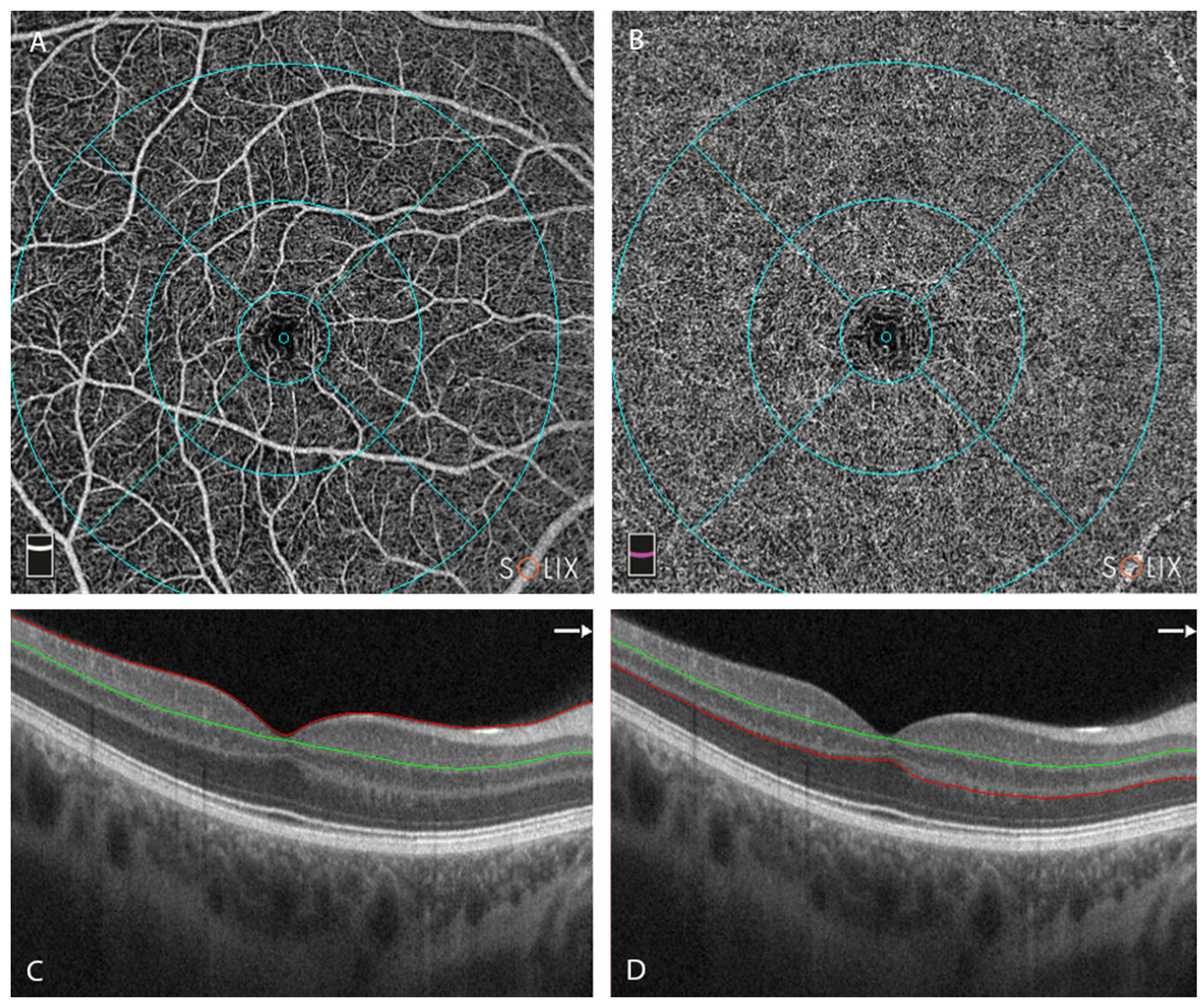
- Superficial retinal capillary plexus (SRCP) (Figure 3A,C):
- whole image (WI) (6.4 mm × 6.4 mm) (%)
- whole image superior hemifield (S.Hemi) (3.0 mm × 6.4 mm) (%)
- whole image inferior hemifield (I.Hemi) (3.0 mm × 6.4 mm) (%)
- ETDRS whole image (0–6 mm diameter) (%)
- ETDRS fovea (0–1 mm diameter circle) (%)
- ETDRS parafovea whole (1–3 mm diameter ring) (%)
- ○
- parafovea S.Hemi (%)
- ○
- parafovea I.Hemi (%)
- ETDRS perifovea whole (3–6 mm diameter ring) (%)
- ○
- parafovea S.Hemi (%)
- ○
- parafovea I.Hemi (%)
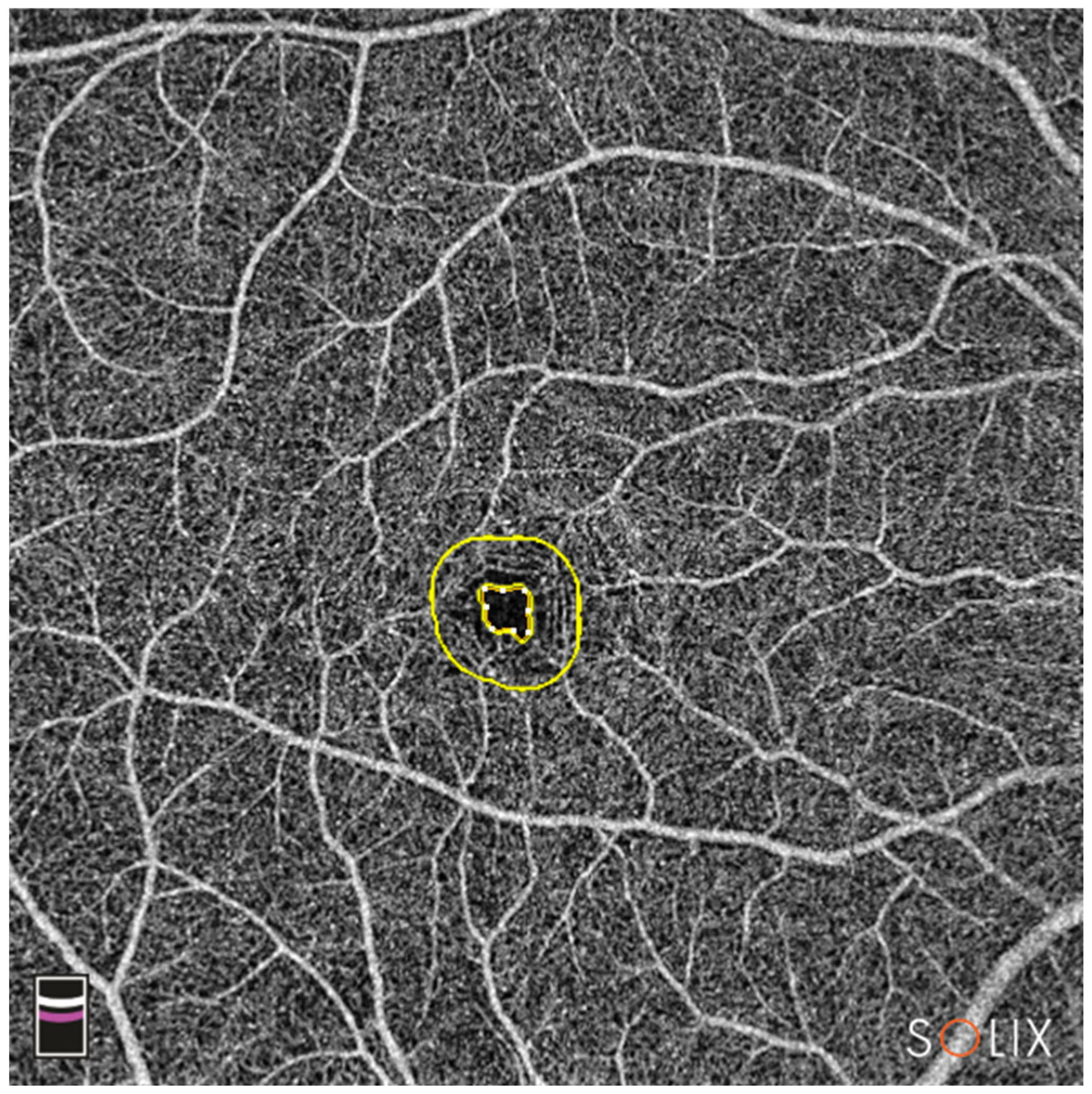
- Foveal avascular zone (FAZ) area (mm2) calculation
- FAZ perimeter (mm) calculation
- FD.300: vessel density of the 300 µm ring surrounding the FAZ (%) (Figure 4)
- ⯀
- Deep retinal capillary plexus (DRCP) (Figure 3B,D): same parameters as for SRCP.
- ○
- Optic disc cube scan (6 mm × 6 mm): radial peripapillary capillaries (RPC) for the whole image all vessels, whole image capillary, inside disc all vessels, inside disc capillary, peripapillary all vessels, peripapillary capillary.
2.5. Statistical Analysis
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Deuel, J.W.; Lauria, E.; Lovey, T.; Zweifel, S.; Meier, M.I.; Zust, R.; Gultekin, N.; Stettbacher, A.; Schlagenhauf, P. Persistence, prevalence, and polymorphism of sequelae after COVID-19 in unvaccinated, young adults of the Swiss Armed Forces: A longitudinal, cohort study (LoCoMo). Lancet Infect. Dis. 2022, 22, 1694–1702. [Google Scholar] [CrossRef] [PubMed]
- Bajka, A.; Wiest, M.R.J.; Hamann, T.; Toro, M.D.; Zweifel, S.A. Assessment of Patients’ Confidence Regarding a New Triage Concept in a Medical Retina Clinic during the First COVID-19 Outbreak. Int. J. Environ. Res. Public Health 2021, 18, 5846. [Google Scholar] [CrossRef] [PubMed]
- Toro, M.D.; Brezin, A.P.; Burdon, M.; Cummings, A.B.; Evren Kemer, O.; Malyugin, B.E.; Prieto, I.; Teus, M.A.; Tognetto, D.; Tornblom, R.; et al. Early impact of COVID-19 outbrea.ak on eye care: Insights from EUROCOVCAT group. Eur. J. Ophthalmol. 2020, 31, 5–9. [Google Scholar] [CrossRef] [PubMed]
- Lai, T.H.T.; Tang, E.W.H.; Li, K.K.W. The Implications of COVID-19 to Ophthalmology. Adv. Exp. Med. Biol. 2021, 1318, 637–655. [Google Scholar] [CrossRef]
- Ng, X.L.; Betzler, B.K.; Testi, I.; Ho, S.L.; Tien, M.; Ngo, W.K.; Zierhut, M.; Chee, S.P.; Gupta, V.; Pavesio, C.E.; et al. Ocular Adverse Events After COVID-19 Vaccination. Ocul. Immunol. Inflamm. 2021, 29, 1216–1224. [Google Scholar] [CrossRef]
- Azarcon, C.P.; Ranche, F.K.T.; Santiago, D.E. Tele-Ophthalmology Practices and Attitudes in the Philippines in Light of the COVID-19 Pandemic: A Survey. Clin. Ophthalmol. 2021, 15, 1239–1247. [Google Scholar] [CrossRef]
- Prager, K.M.; Dagi Glass, L.R.; Wang, M.; Chen, R.W.S.; Liebmann, J.M.; Cioffi, G.A. Ophthalmology and Ethics in the COVID-19 Era. Am. J. Ophthalmol. 2021, 224, 158–162. [Google Scholar] [CrossRef]
- Lim, L.W.; Yip, L.W.; Tay, H.W.; Ang, X.L.; Lee, L.K.; Chin, C.F.; Yong, V. Sustainable practice of ophthalmology during COVID-19: Challenges and solutions. Graefes Arch. Clin. Exp. Ophthalmol. 2020, 258, 1427–1436. [Google Scholar] [CrossRef] [Green Version]
- Jin, Y.P.; Trope, G.E.; El-Defrawy, S.; Liu, E.Y.; Buys, Y.M. Ophthalmology-focused publications and findings on COVID-19: A systematic review. Eur. J. Ophthalmol. 2021, 31, 1677–1687. [Google Scholar] [CrossRef]
- Sethi, K.; Levine, E.S.; Roh, S.; Marx, J.L.; Ramsey, D.J. Modeling the impact of COVID-19 on Retina Clinic Performance. BMC Ophthalmol. 2021, 21, 206. [Google Scholar] [CrossRef]
- Wiersinga, W.J.; Rhodes, A.; Cheng, A.C.; Peacock, S.J.; Prescott, H.C. Pathophysiology, Transmission, Diagnosis, and Treatment of Coronavirus Disease 2019 (COVID-19): A Review. JAMA 2020, 324, 782–793. [Google Scholar] [CrossRef]
- Singh, S.P.; Pritam, M.; Pandey, B.; Yadav, T.P. Microstructure, pathophysiology, and potential therapeutics of COVID-19: A comprehensive review. J. Med. Virol. 2021, 93, 275–299. [Google Scholar] [CrossRef] [PubMed]
- Jin, Y.; Yang, H.; Ji, W.; Wu, W.; Chen, S.; Zhang, W.; Duan, G. Virology, Epidemiology, Pathogenesis, and Control of COVID-19. Viruses 2020, 12, 372. [Google Scholar] [CrossRef] [Green Version]
- Mohamadian, M.; Chiti, H.; Shoghli, A.; Biglari, S.; Parsamanesh, N.; Esmaeilzadeh, A. COVID-19: Virology, biology and novel laboratory diagnosis. J. Gene Med. 2021, 23, e3303. [Google Scholar] [CrossRef]
- Merad, M.; Blish, C.A.; Sallusto, F.; Iwasaki, A. The immunology and immunopathology of COVID-19. Science 2022, 375, 1122–1127. [Google Scholar] [CrossRef] [PubMed]
- Turker, I.C.; Dogan, C.U.; Guven, D.; Kutucu, O.K.; Gul, C. Optical coherence tomography angiography findings in patients with COVID-19. Can. J. Ophthalmol. 2021, 56, 83–87. [Google Scholar] [CrossRef] [PubMed]
- Gonzalez-Zamora, J.; Bilbao-Malave, V.; Gandara, E.; Casablanca-Pinera, A.; Boquera-Ventosa, C.; Landecho, M.F.; Zarranz-Ventura, J.; Garcia-Layana, A. Retinal Microvascular Impairment in COVID-19 Bilateral Pneumonia Assessed by Optical Coherence Tomography Angiography. Biomedicines 2021, 9, 247. [Google Scholar] [CrossRef]
- Cennamo, G.; Reibaldi, M.; Montorio, D.; D’Andrea, L.; Fallico, M.; Triassi, M. Optical coherence tomography angiography features in post COVID-19 pneumonia patients: A pilot study. Am. J. Ophthalmol. 2021, 227, 182–190. [Google Scholar] [CrossRef] [PubMed]
- Chua, J.; Chin, C.W.L.; Tan, B.; Wong, S.H.; Devarajan, K.; Le, T.T.; Ang, M.; Wong, T.Y.; Schmetterer, L. Impact of systemic vascular risk factors on the choriocapillaris using optical coherence tomography angiography in patients with systemic hypertension. Sci. Rep. 2019, 9, 5819. [Google Scholar] [CrossRef] [Green Version]
- Jevnikar, K.; Lapajne, L.; Petrovic, D.; Meglic, A.; Logar, M.; Vidovic Valentincic, N.; Globocnik Petrovic, M.; Cilensek, I.; Mekjavic, P.J. The Role of ACE, ACE2, and AGTR2 Polymorphisms in COVID-19 Severity and the Presence of COVID-19-Related Retinopathy. Genes 2022, 13, 1111. [Google Scholar] [CrossRef]
- Shiroma, H.F.; Lima, L.H.; Shiroma, Y.B.; Kanadani, T.C.; Nobrega, M.J.; Andrade, G.; de Moraes Filho, M.N.; Penha, F.M. Retinal vascular occlusion in patients with the COVID-19 virus. Int. J. Retin. Vitr. 2022, 8, 45. [Google Scholar] [CrossRef]
- Abrishami, M.; Daneshvar, R.; Emamverdian, Z.; Saeedian, N.; Tohidinezhad, F.; Eslami, S.; Ansari-Astaneh, M.R. Spectral-domain optical coherence tomography assessment of retinal and choroidal changes in patients with coronavirus disease 2019: A case-control study. J. Ophthalmic Inflamm. Infect. 2022, 12, 18. [Google Scholar] [CrossRef]
- Chen, T.C.; Cense, B.; Pierce, M.C.; Nassif, N.; Park, B.H.; Yun, S.H.; White, B.R.; Bouma, B.E.; Tearney, G.J.; de Boer, J.F. Spectral domain optical coherence tomography: Ultra-high speed, ultra-high resolution ophthalmic imaging. Arch. Ophthalmol. 2005, 123, 1715–1720. [Google Scholar] [CrossRef]
- Huang, D.; Swanson, E.A.; Lin, C.P.; Schuman, J.S.; Stinson, W.G.; Chang, W.; Hee, M.R.; Flotte, T.; Gregory, K.; Puliafito, C.A.; et al. Optical coherence tomography. Science 1991, 254, 1178–1181. [Google Scholar] [CrossRef] [Green Version]
- de Carlo, T.E.; Romano, A.; Waheed, N.K.; Duker, J.S. A review of optical coherence tomography angiography (OCTA). Int. J. Retin. Vitr. 2015, 1, 5. [Google Scholar] [CrossRef] [Green Version]
- Spaide, R.F.; Fujimoto, J.G.; Waheed, N.K.; Sadda, S.R.; Staurenghi, G. Optical coherence tomography angiography. Prog. Retin. Eye Res. 2018, 64, 1–55. [Google Scholar] [CrossRef]
- Muth, D.R.; Toro, M.D.; Bajka, A.; Jonak, K.; Rieder, R.; Kohler, M.M.; Gunzinger, J.M.; Souied, E.H.; Engelbert, M.; Freund, K.B.; et al. Correlation between Macular Neovascularization (MNV) Type and Druse Type in Neovascular Age-Related Macular Degeneration (AMD) Based on the CONAN Classification. Biomedicines 2022, 10, 2370. [Google Scholar] [CrossRef]
- Wiest, M.R.J.; Toro, M.D.; Nowak, A.; Baur, J.; Fasler, K.; Hamann, T.; Al-Sheikh, M.; Zweifel, S.A. Globotrioasylsphingosine Levels and Optical Coherence Tomography Angiography in Fabry Disease Patients. J. Clin. Med. 2021, 10, 1093. [Google Scholar] [CrossRef]
- Optovue Inc. SOLIX User Manual; P/N 580-53958-001 B; Bayview Drive: Fremont, CA, USA, 2019. [Google Scholar]
- Arumuganathan, N.; Wiest, M.R.J.; Toro, M.D.; Hamann, T.; Fasler, K.; Zweifel, S.A. Acute and subacute macular and peripapillary angiographic changes in choroidal and retinal blood flow post-intravitreal injections. Sci. Rep. 2021, 11, 19381. [Google Scholar] [CrossRef]
- Gunzinger, J.M.; Ibrahimi, B.; Baur, J.; Wiest, M.R.J.; Piccirelli, M.; Pangalu, A.; Straumann, D.; Nietlispach, F.; Moarof, I.; Zweifel, S.A. Assessment of Retinal Capillary Dropout after Transcatheter Aortic Valve Implantation by Optical Coherence Tomography Angiography. Diagnostics 2021, 11, 2399. [Google Scholar] [CrossRef]
- Wiest, M.R.J.; Bajka, A.; Hamann, T.; Foa, N.; Toro, M.; Barthelmes, D.; Zweifel, S. Differences in Mean Values and Variance in Quantitative Analyses of Foveal OCTA Imaging. Klin. Monbl. Augenheilkd. 2022, 239, 513–517. [Google Scholar] [CrossRef]
- Wiest, M.R.J.; Hamann, T.; Zweifel, S. Effect of Valsalva Maneuver on Choriocapillary Retinal Microvasculature. Klin. Monbl. Augenheilkd. 2022, 239, 523–526. [Google Scholar] [CrossRef] [PubMed]
- Hamann, T.; Wiest, M.R.J.; Brinkmann, M.; Toro, M.; Fasler, K.; Baur, J.; Freund, K.B.; Zweifel, S. Assessment of the microvasculature in poppers maculopathy. Graefes Arch. Clin. Exp. Ophthalmol. 2022, 260, 1299–1306. [Google Scholar] [CrossRef]
- Szumilas, M. Explaining odds ratios. J. Can. Acad. Child. Adolesc. Psychiatry 2010, 19, 227–229. [Google Scholar] [PubMed]
- Azar, G.; Bonnin, S.; Vasseur, V.; Faure, C.; Salviat, F.; Clermont, C.V.; Titah, C.; Fares, S.; Boulanger, E.; Derrien, S.; et al. Did the COVID-19 Pandemic Increase the Incidence of Acute Macular Neuroretinopathy? J. Clin. Med. 2021, 10, 5038. [Google Scholar] [CrossRef] [PubMed]
- Vinzamuri, S.; Pradeep, T.G.; Kotian, R. Bilateral paracentral acute middle maculopathy and acute macular neuroretinopathy following COVID-19 vaccination. Indian J. Ophthalmol. 2021, 69, 2862–2864. [Google Scholar] [CrossRef]
- Jonathan, G.L.; Scott, F.M.; Matthew, K.D. A Case of Post-COVID-19-Associated Paracentral Acute Middle Maculopathy and Giant Cell Arteritis-Like Vasculitis. J. Neuroophthalmol. 2021, 41, 351–355. [Google Scholar] [CrossRef]
- Savastano, M.C.; Gambini, G.; Cozzupoli, G.M.; Crincoli, E.; Savastano, A.; De Vico, U.; Culiersi, C.; Falsini, B.; Martelli, F.; Minnella, A.M.; et al. Retinal capillary involvement in early post-COVID-19 patients: A healthy controlled study. Graefes Arch. Clin. Exp. Ophthalmol. 2021, 259, 2157–2165. [Google Scholar] [CrossRef] [PubMed]
- Abrishami, M.; Emamverdian, Z.; Shoeibi, N.; Omidtabrizi, A.; Daneshvar, R.; Saeidi Rezvani, T.; Saeedian, N.; Eslami, S.; Mazloumi, M.; Sadda, S.; et al. Optical coherence tomography angiography analysis of the retina in patients recovered from COVID-19: A case-control study. Can. J. Ophthalmol. 2021, 56, 24–30. [Google Scholar] [CrossRef]
- Invernizzi, A.; Torre, A.; Parrulli, S.; Zicarelli, F.; Schiuma, M.; Colombo, V.; Giacomelli, A.; Cigada, M.; Milazzo, L.; Ridolfo, A.; et al. Retinal findings in patients with COVID-19: Results from the SERPICO-19 study. EClinicalMedicine 2020, 27, 100550. [Google Scholar] [CrossRef]
- Erogul, O.; Gobeka, H.H.; Dogan, M.; Akdogan, M.; Balci, A.; Kasikci, M. Retinal microvascular morphology versus COVID-19: What to anticipate? Photodiagn. Photodyn. Ther. 2022, 39, 102920. [Google Scholar] [CrossRef]
- Abrishami, M.; Hassanpour, K.; Hosseini, S.; Emamverdian, Z.; Ansari-Astaneh, M.R.; Zamani, G.; Gharib, B.; Abrishami, M. Macular vessel density reduction in patients recovered from COVID-19: A longitudinal optical coherence tomography angiography study. Graefes Arch. Clin. Exp. Ophthalmol. 2022, 260, 771–779. [Google Scholar] [CrossRef] [PubMed]
- Aydemir, E.; Aydemir, G.A.; Atesoglu, H.I.; Goker, Y.S.; Ozcelik, K.C.; Kiziltoprak, H. The Impact of Coronavirus Disease 2019 (COVID-19) on Retinal Microcirculation in Human Subjects. Klin. Monbl. Augenheilkd. 2021, 238, 1305–1311. [Google Scholar] [CrossRef] [PubMed]
- Abrishami, M.; Daneshvar, R.; Emamverdian, Z.; Shoeibi, N.; Sedighi, S.; Rezvani, T.S.; Saeedian, N.; Eslami, S. Optic Nerve Head Optical Coherence Tomography Angiography Findings after Coronavirus Disease. J. Ophthalmic Vis. Res. 2021, 16, 592–601. [Google Scholar] [CrossRef] [PubMed]







{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Long Post-COVID-19 (>180 d) | Recent Post- COVID-19 (≤180 d) | Asymptomatic Post-COVID-19 | Control Group (SARS-CoV-2 Negative) | p | |
|---|---|---|---|---|---|
| Group size (n) | 168 | 19 | 46 | 233 | N/A |
| COVID vaccination status: At least 1 SARS-CoV-2 vaccine prior to study | 118 (70%) | 10 (53%) | 30 (65%) | 191 (82%) | N/A |
| Time (d) from COVID diagnosis to study start (median (25%; 75% quantile) | 317 (272; 414) | 101 (83; 155) | N/A | N/A | N/A |
| Age (years) (mean ± SD (95% CI) | median) | 22.5 ± 2.5 (22.1; 22.9) | 22 | 21.3 ± 1.2 (20.8; 21.9) | 21 | 21.8 ± 2.0 (21.2; 22.4) | 21 | 21.7 ± 1.6 (21.5; 21.9) | 21 | 0.07423 |
| Sex ratio female:male | 8 (5%):160 (95%) | 1 (5%):18 (95%) | 3 (7%):43 (93%) | 13 (6%):220 (94%) | N/A |
| Roche Anti-SARS-CoV-2 test cobas.S (mean ± SD (95% CI)) | 185.33660 ± 96.30346 (170.66782; 200.00538) | 172.30579 ± 94.23907 (126.88401; 217.72757) | 207.35870 ± 78.80898 (183.95532; 230.76207) | 178.79528 ± 108.96684 (164.73040; 192.86016) | 0.60617 |
| Roche Anti-SARS-CoV-2 test cobas.N (mean ± SD (95% CI)) | 8.58670 ± 15.09939 (6.28678; 10.88661) | 28.70184 ± 43.61160 (7.68173; 49.72196) | 8.88696 ± 16.08435 (4.11049; 13.66342) | 0.30860 ± 2.02638 (0.04704; 0.57015) | <0.00001 * |
| CVA OD (logMAR) (mean ± SD (95% CI)) | −0.09 ± 0.08 (−0.10; −0.08) | −0.08 ± 0.08 (−0.08 ± 0.08) | −0.06 ± 0.07 (−0.09; −0.04) | −0.08 ± 0.08 (−0.09; −0.07) | 0.18882 |
| CVA OS (logMAR) (mean ± SD (95% CI)) | −0.10 ± 0.08 (−0.11; −0.08) | −0.08 ± 0.09 (−0.12; −0.04) | −0.09 ± 0.10 (−0.12; −0.06) | −0.08 ± 0.10 (−0.09; −0.06) | 0.53837 |
| IOP OD (mmHg) (mean ± SD (95% CI)) | 14.7 ± 2.5 (14.3; 15.1) | 14.5 ± 2.4 (13.4; 15.7) | 14.9 ± 2.9 (14.0; 15.7) | 14.8 ± 2.8 (14.4; 15.1) | 0.92173 |
| IOP OS (mmHg) (mean ± SD (95% CI)) | 14.8 ± 2.8 (14.3; 15.2) | 15.3 ± 3.1 (13.8; 16.8) | 14.8 ± 2.8 (13.9; 15.6) | 15.4 ± 8.1 (14.3; 16.4) | 0.85845 |
| SE OD (D) (mean ± SD (95% CI)) | −0.49 ± 1.34 (−0.70; −0.29) | −0.22 ± 1.37 (−0.88; 0.45) | −0.86 ± 2.05 (−1.47; −0.25) | −0.49 ± 1.34 (−0.67; −0.32) | 0.82620 |
| SE OS (D) (mean ± SD (95% CI)) | −0.48 ± 1.43 (−0.70; −0.26) | −0.70 ± 1.65 (−1.49; 0.10) | −0.88 ± 1.93 (−1.45; −0.30) | −0.47 ± 1.30 (−0.64; −0.30) | 0.76287 |
| Smoking status: Never Ex-smoker Active smoker Unknown | 108 (64%) 20 (12%) 33 (20%) 7 (4%) | 12 (63%) 0 (0%) 7 (37%) 0 (0%) | 30 (65%) 3 (7%) 11 (24%) 2 (4%) | 158 (68%) 13 (6%) 51 (22%) 11 (5%) | 0.88565 |
| Body height (cm) (mean ± SD (95% CI)) | 179.16 ± 11.58 (177.09; 181.24) | 179.71 ± 9.02 (174.51; 184.92) | 178.63 ± 6.79 (176.18; 181.07) | 178.77 ± 7.47 (177.73; 179.81) | 0.82543 |
| Body weight (kg) (mean ± SD (95% CI)) | 79.21 ± 15.81 (76.38 82.05) | 74.50 ± 11.47 (67.88; 81.12) | 79.55 ± 16.85 (73.47; 85.62) | 75.63 ± 11.48 (74.04; 77.23) | 0.21742 |
| Control Group (Mean (95% CI)) | All-COVID-19 Group (Mean (95% CI)) | p-Value | |
|---|---|---|---|
| OCTA quality index (QI) | |||
| OD__OCTA_Macula_6.4×6.4__Quality.Index.QI | 9.00 (6.00;10.0) | 9.00 (6.00;10.0) | 0.845 |
| OS__OCTA_Macula_6.4×6.4__Quality.Index.QI | 9.00 (6.00;10.0) | 9.00 (6.00;10.0) | 0.800 |
| OCTA MACULA superior retinal capillary plexus (SRCP) vessel density (%) | |||
| OD__OCTA_Macula_6.4×6.4__SRCP_Whole.Image | 49.6 (43.0;51.8) | 49.5 (43.7;52.1) | 0.495 |
| OD__OCTA_Macula_6.4×6.4__SRCP_Whole.Image.S.Hemi | 49.6 (42.4;53.7) | 49.6 (43.9;51.9) | 0.722 |
| OD__OCTA_Macula_6.4×6.4__SRCP_Whole.Image.I.Hemi | 49.7 (43.7;52.3) | 49.5 (43.3;52.4) | 0.302 |
| OD__OCTA_Macula_6.4×6.4__SRCP_Whole.ETDRS | 49.3 (41.9;51.6) | 49.2 (42.9;51.9) | 0.462 |
| OD__OCTA_Macula_6.4×6.4__SRCP_Fovea | 31.2 (15.7;40.2) | 31.2 (12.8;42.9) | 0.965 |
| OD__OCTA_Macula_6.4×6.4__SRCP_ParaFovea | 51.1 (37.7;54.6) | 50.9 (42.0;54.0) | 0.509 |
| OD__OCTA_Macula_6.4×6.4__SRCP_Para.S.Hemi | 51.0 (37.5;54.7) | 51.2 (41.6;53.9) | 0.952 |
| OD__OCTA_Macula_6.4×6.4__SRCP_Para.I.Hemi | 51.1 (37.9;55.2) | 50.8 (41.1;54.8) | 0.189 |
| OD__OCTA_Macula_6.4×6.4__SRCP_PeriFovea | 49.4 (43.9;52.0) | 49.3 (43.9;52.0) | 0.488 |
| OD__OCTA_Macula_6.4×6.4__SRCP_Peri.S.Hemi | 49.4 (42.9;52.6) | 49.4 (43.0;51.9) | 0.750 |
| OD__OCTA_Macula_6.4×6.4__SRCP_Peri.I.Hemi | 49.6 (44.4;52.4) | 49.3 (43.6;52.6) | 0.314 |
| OS__OCTA_Macula_6.4×6.4__SRCP_Density.Whole.Image | 49.6 (43.7;52.0) | 49.5 (43.5;52.1) | 0.973 |
| OS__OCTA_Macula_6.4×6.4__SRCP_Whole.Image.S.Hemi | 49.7 (43.0;52.2) | 49.5 (43.8;52.0) | 0.775 |
| OS__OCTA_Macula_6.4×6.4__SRCP_Whole.Image.I.Hemi | 49.5 (44.5;52.4) | 49.6 (43.2;52.5) | 0.706 |
| OS__OCTA_Macula_6.4×6.4__SRCP_Whole.ETDRS | 49.1 (43.0;51.7) | 49.2 (42.8;51.9) | 0.767 |
| OS__OCTA_Macula_6.4×6.4__SRCP_Fovea | 31.2 (15.8;40.4) | 31.2 (17.0;42.0) | 0.932 |
| OS__OCTA_Macula_6.4×6.4__SRCP_ParaFovea | 50.6 (39.6;54.4) | 50.9 (39.5;54.7) | 0.259 |
| OS__OCTA_Macula_6.4×6.4__SRCP_Para.S.Hemi | 50.7 (40.9;54.8) | 50.8 (39.2;55.0) | 0.209 |
| OS__OCTA_Macula_6.4×6.4__SRCP_Para.I.Hemi | 50.7 (38.3;54.1) | 50.7 (39.9;54.8) | 0.453 |
| OS__OCTA_Macula_6.4×6.4__SRCP_PeriFovea | 49.3 (44.4;51.8) | 49.3 (44.1;51.9) | 0.937 |
| OS__OCTA_Macula_6.4×6.4__SRCP_Peri.S.Hemi | 49.1 (43.1;52.3) | 49.3 (43.0;52.2) | 0.987 |
| OS__OCTA_Macula_6.4×6.4__SRCP_Peri.I.Hemi | 49.3 (44.4;52.5) | 49.4 (43.3;52.2) | 0.968 |
| OU__OCTA_Macula_6.4×6.4__SRCP_Whole.Image | 49.5 (43.0;51.6) | 49.5 (45.8;51.6) | 0.781 |
| OU__OCTA_Macula_6.4×6.4__SRCP_Whole.Image.S.Hemi | 49.4 (42.4;52.1) | 49.5 (45.4;51.9) | 0.740 |
| OU__OCTA_Macula_6.4×6.4__SRCP_Whole.Image.I.Hemi | 49.3 (43.7;51.8) | 49.4 (44.8;51.7) | 0.901 |
| OU__OCTA_Macula_6.4×6.4__SRCP_Whole.ETDRS | 49.1 (41.9;51.6) | 49.2 (44.3;51.3) | 0.974 |
| OU__OCTA_Macula_6.4×6.4__SRCP_Fovea | 31.1 (18.7;40.2) | 31.0 (16.9;42.4) | 0.955 |
| OU__OCTA_Macula_6.4×6.4__SRCP_ParaFovea | 50.7 (37.7;53.9) | 50.8 (42.0;53.5) | 0.553 |
| OU__OCTA_Macula_6.4×6.4__SRCP_Para.S.Hemi | 50.7 (37.5;53.9) | 50.8 (42.8;54.2) | 0.346 |
| OU__OCTA_Macula_6.4×6.4__SRCP_Para.I.Hemi | 50.8 (37.9;54.1) | 50.6 (41.2;54.5) | 0.935 |
| OU__OCTA_Macula_6.4×6.4__SRCP_PeriFovea | 49.3 (43.9;51.7) | 49.3 (45.5;51.5) | 0.807 |
| OU__OCTA_Macula_6.4×6.4__SRCP_Peri.S.Hemi | 49.2 (42.9;52.0) | 49.3 (45.0;51.8) | 0.967 |
| OU__OCTA_Macula_6.4×6.4__SRCP_Peri.I.Hemi | 49.3 (45.0;52.2) | 49.2 (44.8;51.6) | 0.675 |
| OCTA MACULA deep retinal capillary plexus (DRCP) vessel density (%) | |||
| OD__OCTA_Macula_6.4×6.4__DRCP_Density.Whole.Image | 54.1 (46.7;55.4) | 54.1 (47.1;55.6) | 0.814 |
| OD__OCTA_Macula_6.4×6.4__DRCP_Whole.Image.S.Hemi | 53.9 (47.3;55.7) | 54.0 (45.5;56.2) | 0.703 |
| OD__OCTA_Macula_6.4×6.4__DRCP_Whole.Image.I.Hemi | 54.2 (45.0;55.8) | 54.2 (44.0;55.9) | 0.803 |
| OD__OCTA_Macula_6.4×6.4__DRCP_Whole.ETDRS | 54.0 (48.9;55.6) | 54.0 (48.1;55.8) | 0.781 |
| OD__OCTA_Macula_6.4×6.4__DRCP_Fovea | 31.1 (14.7;45.3) | 31.5 (11.6;46.0) | 0.732 |
| OD__OCTA_Macula_6.4×6.4__DRCP_ParaFovea | 54.7 (51.3;57.1) | 54.8 (50.2;57.3) | 0.496 |
| OD__OCTA_Macula_6.4×6.4__DRCP_Para.S.Hemi | 54.5 (50.2;57.4) | 54.6 (49.8;57.4) | 0.683 |
| OD__OCTA_Macula_6.4×6.4__DRCP_Para.I.Hemi | 54.8 (50.5;58.0) | 55.0 (49.2;57.8) | 0.538 |
| OD__OCTA_Macula_6.4×6.4__DRCP_PeriFovea | 54.5 (48.7;56.6) | 54.5 (47.6;56.8) | 0.859 |
| OD__OCTA_Macula_6.4×6.4__DRCP_Peri.S.Hemi | 54.4 (49.3;56.9) | 54.5 (48.2;57.4) | 0.336 |
| OD__OCTA_Macula_6.4×6.4__DRCP_Peri.I.Hemi | 54.5 (46.9;56.9) | 54.5 (42.9;56.7) | 0.652 |
| OD__OCTA_Macula_6.4×6.4__FD.300.Area.Density | 51.8 (33.5;59.5) | 52.2 (40.6;59.7) | 0.957 |
| OD__OCTA_Macula_6.4×6.4__FD.300.Length.Density | 17.3 (14.4;19.0) | 17.3 (14.7;18.9) | 0.625 |
| OS__OCTA_Macula_6.4×6.4__DRCP_Density.Whole.Image | 54.0 (42.0;55.9) | 53.9 (46.6;55.9) | 0.733 |
| OS__OCTA_Macula_6.4×6.4__DRCP_Whole.Image.S.Hemi | 53.9 (41.6;55.9) | 53.9 (45.7;56.0) | 0.489 |
| OS__OCTA_Macula_6.4×6.4__DRCP_Whole.Image.I.Hemi | 53.9 (42.5;56.0) | 53.9 (46.3;56.0) | 0.717 |
| OS__OCTA_Macula_6.4×6.4__DRCP_Whole.ETDRS | 53.8 (44.6;56.1) | 53.8 (48.9;56.2) | 0.535 |
| OS__OCTA_Macula_6.4×6.4__DRCP_Fovea | 31.6 (17.4;46.5) | 31.7 (14.9;45.0) | 0.773 |
| OS__OCTA_Macula_6.4×6.4__DRCP_ParaFovea | 54.6 (50.1;57.1) | 54.8 (50.5;56.6) | 0.331 |
| OS__OCTA_Macula_6.4×6.4__DRCP_Para.S.Hemi | 54.5 (49.9;57.3) | 54.7 (50.6;57.7) | 0.234 |
| OS__OCTA_Macula_6.4×6.4__DRCP_Para.I.Hemi | 54.7 (49.9;58.0) | 54.7 (49.3;57.7) | 0.829 |
| OS__OCTA_Macula_6.4×6.4__DRCP_PeriFovea | 54.4 (43.7;56.8) | 54.3 (48.4;57.0) | 0.336 |
| OS__OCTA_Macula_6.4×6.4__DRCP_Peri.S.Hemi | 54.5 (44.6;57.0) | 54.2 (47.8;57.3) | 0.116 |
| OS__OCTA_Macula_6.4×6.4__DRCP_Peri.I.Hemi | 54.4 (42.7;56.8) | 54.4 (43.5;56.8) | 0.900 |
| OS__OCTA_Macula_6.4×6.4__FD.300.Area.Density | 51.6 (35.7;59.4) | 52.2 (33.8;59.7) | 0.085 |
| OS__OCTA_Macula_6.4×6.4__FD.300.Length.Density | 17.1 (14.4;19.0) | 17.1 (14.9;18.9) | 0.330 |
| OU__OCTA_Macula_6.4×6.4__DRCP_Density.Whole.Image | 53.8 (46.7;55.3) | 54.0 (48.9;55.5) | 0.694 |
| OU__OCTA_Macula_6.4×6.4__DRCP_Whole.Image.S.Hemi | 53.7 (46.7;55.5) | 53.9 (48.1;55.5) | 0.679 |
| OU__OCTA_Macula_6.4×6.4__DRCP_Whole.Image.I.Hemi | 53.9 (45.0;55.2) | 53.9 (49.0;55.5) | 0.752 |
| OU__OCTA_Macula_6.4×6.4__DRCP_Whole.ETDRS | 53.8 (49.1;55.2) | 53.8 (50.2;55.3) | 0.919 |
| OU__OCTA_Macula_6.4×6.4__DRCP_Fovea | 31.2 (16.0;46.5) | 31.4 (14.0;43.8) | 0.834 |
| OU__OCTA_Macula_6.4×6.4__DRCP_ParaFovea | 54.6 (51.4;56.5) | 54.7 (51.6;56.5) | 0.194 |
| OU__OCTA_Macula_6.4×6.4__DRCP_Para.S.Hemi | 54.4 (50.9;56.6) | 54.5 (51.8;56.5) | 0.179 |
| OU__OCTA_Macula_6.4×6.4__DRCP_Para.I.Hemi | 54.7 (51.0;57.0) | 54.7 (51.1;56.8) | 0.467 |
| OU__OCTA_Macula_6.4×6.4__DRCP_PeriFovea | 54.3 (48.7;55.9) | 54.3 (49.4;56.4) | 0.844 |
| OU__OCTA_Macula_6.4×6.4__DRCP_Peri.S.Hemi | 54.2 (49.7;56.0) | 54.3 (50.8;56.7) | 0.970 |
| OU__OCTA_Macula_6.4×6.4__DRCP_Peri.I.Hemi | 54.3 (46.9;56.0) | 54.3 (47.7;56.0) | 0.840 |
| OU__OCTA_Macula_6.4×6.4__FD.300.Area.Density | 51.6 (33.5;57.8) | 52.0 (43.3;58.5) | 0.263 |
| OU__OCTA_Macula_6.4×6.4__FD.300.Length.Density | 17.2 (14.7;18.8) | 17.2 (15.6;18.7) | 0.247 |
| OCTA DISC radial peripapillary capillary (RPC) | |||
| OD__OCTA_Disc_6×6_RPC__Density.Whole.Image | 54.6 (48.2;59.7) | 55.0 (48.4;60.3) | 0.034 * |
| OD__OCTA_Disc_6×6_RPC__Whole.Image.Capillary | 47.6 (41.2;53.6) | 47.9 (41.4;53.2) | 0.021 * |
| OD__OCTA_Disc_6×6_RPC__Inside.Disc.All | 65.6 (47.1;82.2) | 65.6 (37.8;79.1) | 0.618 |
| OD__OCTA_Disc_6×6_RPC__Inside.Disc.Capillary | 55.5 (28.9;75.5) | 55.5 (21.5;75.4) | 0.235 |
| OD__OCTA_Disc_6×6_RPC__Peripapillary.All | 55.9 (47.3;60.7) | 56.2 (48.9;61.1) | 0.163 |
| OD__OCTA_Disc_6×6_RPC__Peripapillary.Capillary | 48.3 (42.0;54.8) | 48.6 (43.2;57.2) | 0.099 |
| OS__OCTA_Disc_6×6_RPC__Density.Whole.Image | 54.5 (45.9;58.6) | 54.8 (49.9;61.3) | 0.326 |
| OS__OCTA_Disc_6×6_RPC__Whole.Image.Capillary | 47.4 (37.1;54.3) | 47.8 (42.2;56.4) | 0.240 |
| OS__OCTA_Disc_6×6_RPC__Inside.Disc.All | 65.4 (41.8;78.3) | 65.4 (31.1;84.8) | 0.854 |
| OS__OCTA_Disc_6×6_RPC__Inside.Disc.Capillary | 54.5 (26.3;71.8) | 55.1 (17.9;73.0) | 0.953 |
| OS__OCTA_Disc_6×6_RPC__Peripapillary.All | 55.6 (47.2;60.6) | 56.0 (48.0;61.8) | 0.308 |
| OS__OCTA_Disc_6×6_RPC__Peripapillary.Capillary | 48.2 (39.1;53.3) | 48.6 (43.0;58.1) | 0.257 |
| OU__OCTA_Disc_6×6_RPC__Density.Whole.Image | 54.6 (47.7;58.9) | 55.0 (50.2;58.6) | 0.071 |
| OU__OCTA_Disc_6×6_RPC__Whole.Image.Capillary | 47.6 (39.2;52.6) | 48.1 (42.6;52.3) | 0.031 * |
| OU__OCTA_Disc_6×6_RPC__Inside.Disc.All | 65.2 (46.4;74.9) | 65.0 (31.1;84.8) | 0.738 |
| OU__OCTA_Disc_6×6_RPC__Inside.Disc.Capillary | 55.1 (33.5;66.4) | 54.5 (17.9;73.0) | 0.321 |
| OU__OCTA_Disc_6×6_RPC__Peripapillary.All | 55.9 (49.0;60.0) | 56.2 (48.5;59.3) | 0.134 |
| OU__OCTA_Disc_6×6_RPC__Peripapillary.Capillary | 48.4 (40.7;53.4) | 48.7 (43.3;53.7) | 0.093 |
| OCTA MACULA foveal avascular zone (FAZ, mm2) and perimeter (mm) | |||
| OD__OCTA_Macula_6.4×6.4__FAZ.Area | 0.21 (0.04;0.56) | 0.20 (0.03;0.64) | 0.901 |
| OD__OCTA_Macula_6.4×6.4__Perimeter | 1.78 (0.73;2.92) | 1.76 (0.65;3.13) | 0.900 |
| OS__OCTA_Macula_6.4×6.4__FAZ.Area | 0.20 (0.03;0.53) | 0.20 (0.02;0.57) | 0.873 |
| OS__OCTA_Macula_6.4×6.4__Perimeter | 1.74 (0.71;2.83) | 1.73 (0.61;2.95) | 0.782 |
| OU__OCTA_Macula_6.4×6.4__FAZ.Area | 0.21 (0.04;0.55) | 0.20 (0.04;0.59) | 0.932 |
| OU__OCTA_Macula_6.4×6.4__Perimeter | 1.76 (0.72;2.88) | 1.74 (0.79;2.95) | 0.809 |
| OCT MACULA thickness (Thk) (microns, µm) | |||
| OD__OCT_Macula_Thk_ILM_BRM.um.__All.field. | 298 (137;563) | 299 (182;329) | 0.669 |
| OS__OCT_Macula_Thk_ILM_BRM.um.__All.field. | 299 (178;330) | 299 (222;464) | 0.682 |
| OU__OCT_Macula_Thk_ILM_BRM.um.__All.field. | 299 (217;563) | 299 (234;383) | 0.639 |
| OCT MACULA volume (Vol, mm3) | |||
| OD__OCT_Macula_Vol_ILM_BRM.mm.3.__All.field. | 31.3 (14.4;59.1) | 31.4 (19.2;34.5) | 0.609 |
| OS__OCT_Macula_Vol_ILM_BRM.mm.3.__All.field. | 31.5 (18.7;34.7) | 31.4 (23.4;48.7) | 0.645 |
| OU__OCT_Macula_Vol_ILM_BRM.mm.3.__All.field. | 31.5 (22.8;59.1) | 31.4 (24.6;40.2) | 0.629 |
| OCT DISC thickness (Thk) (microns, µm) measured within the slab of internal limiting membrane (ILM) to nerve fiber layer (NFL) | |||
| OD__OCT_Disc_Cube_6×6__Thk_ILM_NFL.all_sectors.um. | 93.6 (0.00;142) | 93.1 (0.00;128) | 0.589 |
| OS__OCT_Disc_Cube_6×6__Thk_ILM_NFL.all_sectors.um. | 93.0 (32.5;764) | 92.2 (31.5;205) | 0.435 |
| OU__OCT_Disc_Cube_6×6__Thk_ILM_NFL.all_sectors.um. | 93.2 (42.2;427) | 92.3 (15.8;153) | 0.510 |
| OCT DISC volume (Vol, mm3) | |||
| OD__OCT_Disc_Cube_6×6__Rim.Volume.mm.3. | 0.25 (0.00;1.03) | 0.23 (0.00;1.27) | 0.242 |
| OS__OCT_Disc_Cube_6×6__Rim.Volume.mm.3. | 0.24 (0.00;1.52) | 0.24 (0.03;1.67) | 0.092 |
| OU__OCT_Disc_Cube_6×6__Rim.Volume.mm.3. | 0.24 (0.02;1.03) | 0.24 (0.06;1.39) | 0.280 |
| PubMed Search Term | No. Search Hits Total | No. Search Hits 2019 | No. Search Hits 2020 | No. Search Hits 2021 | No. Search Hits 2022-10 |
|---|---|---|---|---|---|
| COVID | 304,677 | 50 | 91,258 | 136,733 | 107,167 |
| COVID + eye | 3686 | 0 | 1114 | 1710 | 1286 |
| COVID + retina | 527 | 0 | 135 | 246 | 208 |
| COVID + retina + vessel | 80 | 0 | 6 | 46 | 40 |
| OCTA Macula: Superficial Capillary Plexus (SRCP) | OCTA Macula: Deep Capillary Plexus (DRCP) | OCTA Disc: Radial Peripapillary Capillary (RPC), Layer: RNFL to ILM | |||
|---|---|---|---|---|---|
| Sig. Parameter | Publication (COVID-19 Cohort Size) | Sig. Parameter | Publication (COVID-19 Cohort Size) | Sig. Parameter | Publication (COVID-19 Cohort Size) |
| Whole image (WI) | Ergul et al. 2022 (n = 32) (PMID: 35597442) [42] Cennamo et al. 2021 (n = 40) (PMID: 33781767) [18] Abrishami et al. 2021 (n = 31) (PMID: 33249111) [40] | Whole image (WI) | Abrishami et al. 2022 (n = 18) (PMID: 34636996) [43] Cennamo et al. 2021 (n = 40) (PMID: 33781767) [18] Abrishami et al. 2021 (n = 31) (PMID: 33249111) [40] | Whole image (WI) | Cennamo et al. 2021 (n = 40) (PMID: 33781767) [18] |
| WI hemifields | Aydemir et al. 2021 (n = 39) (PMID: 34587629) [44] Abrishami et al. 2021 (n = 31) (PMID: 33249111) [40] | WI hemifields | Abrishami et al. 2021 (n = 31) (PMID: 33249111) [40] | Small Vessels Inside Disc | Abrishami 2021 (n = 25) (PMID: 34840682) [45] |
| Fovea | Ergul et al. 2022 (n = 32) (PMID: 35597442) [42] Abrishami et al. 2021 (n = 31) (PMID: 3324911) [40] | Fovea | Ergul et al. 2022 (n = 32) (PMID: 35597442) [42] Cennamo et al. 2021 (n = 40) (PMID: 33781767) [18] Abrishami et al. 2021 (n = 31) (PMID: 33249111) [40] | Small Vessels Peripapillary (whole) | Abrishami 2021 (n = 25) (PMID: 34840682) [45] |
| Parafovea | Ergul et al. 2022 (n = 32) (PMID: 35597442) [42] Aydemir et al. 2021 (n = 39) (PMID: 34587629) [44] Abrishami et al. 2021 (n = 31) (PMID: 33249111) [40] | Parafovea | Abrishami et al. 2022 (n = 18) (PMID: 34636996) [43] Cennamo et al. 2021 (n = 40) (PMID: 33781767) [18] Abrishami et al. 2021 (n = 31) (PMID: 33249111) [40] | Small Vessels Peripapillary (sectoral) | Abrishami 2021 (n = 25) (PMID: 34840682) [45] |
| Perifovea | Ergul et al. 2022 (n = 32) (PMID: 35597442) [42] Abrishami et al. 2022 (n = 18) (PMID: 34636996) [43] | Perifovea | Abrishami et al. 2022 (n = 18) (PMID: 34636996) [43] | ||
| FAZ area/FAZ FD-300 | Ergul et al. 2022 (n = 32) (PMID: 35597442) [42] | ||||
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Bajka, A.; Muth, D.R.; Wiest, M.R.J.; Said, S.; Rejdak, M.; Sidhu, S.; Foa, N.; Blaser, F.; Barthelmes, D.; Toro, M.D.; et al. Analysis of Optical Coherence Tomography (OCT) and Optical Coherence Tomography Angiography (OCTA) Parameters in Young Adults after SARS-CoV-2 Infection (COVID-19) Compared with Healthy Young Controls. Diagnostics 2023, 13, 1283. https://doi.org/10.3390/diagnostics13071283
Bajka A, Muth DR, Wiest MRJ, Said S, Rejdak M, Sidhu S, Foa N, Blaser F, Barthelmes D, Toro MD, et al. Analysis of Optical Coherence Tomography (OCT) and Optical Coherence Tomography Angiography (OCTA) Parameters in Young Adults after SARS-CoV-2 Infection (COVID-19) Compared with Healthy Young Controls. Diagnostics. 2023; 13(7):1283. https://doi.org/10.3390/diagnostics13071283
Chicago/Turabian StyleBajka, Anahita, Daniel Rudolf Muth, Maximilian Robert Justus Wiest, Sadiq Said, Magdalena Rejdak, Sophia Sidhu, Nastasia Foa, Frank Blaser, Daniel Barthelmes, Mario Damiano Toro, and et al. 2023. "Analysis of Optical Coherence Tomography (OCT) and Optical Coherence Tomography Angiography (OCTA) Parameters in Young Adults after SARS-CoV-2 Infection (COVID-19) Compared with Healthy Young Controls" Diagnostics 13, no. 7: 1283. https://doi.org/10.3390/diagnostics13071283