
Deep Learning-Based Auto-Segmentation of Spinal Cord Internal Structure of Diffusion Tensor Imaging in Cervical Spondylotic Myelopathy
 ,
,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Population
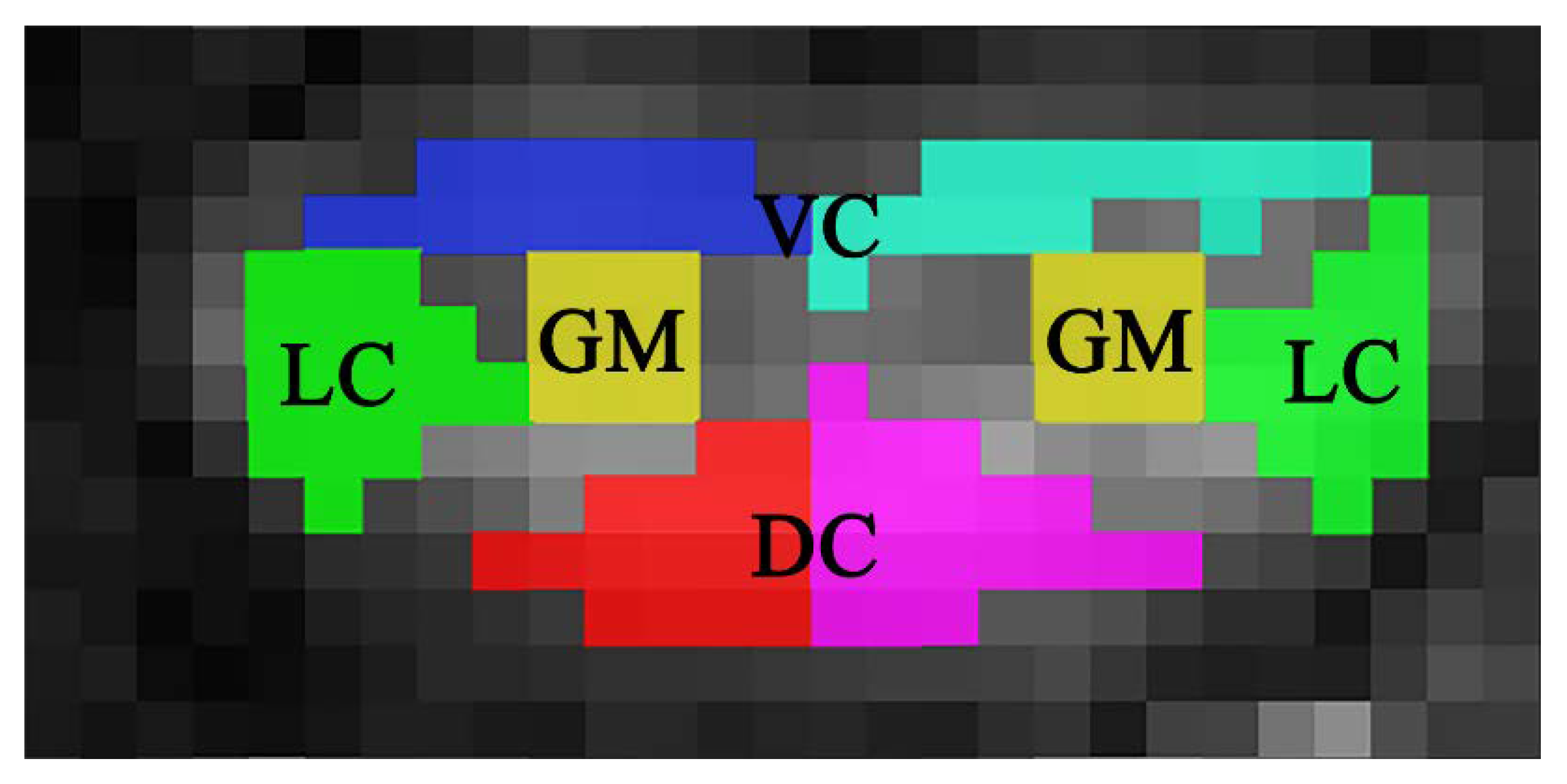
2.2. Manual Segmentation
2.3. Segmentation Models
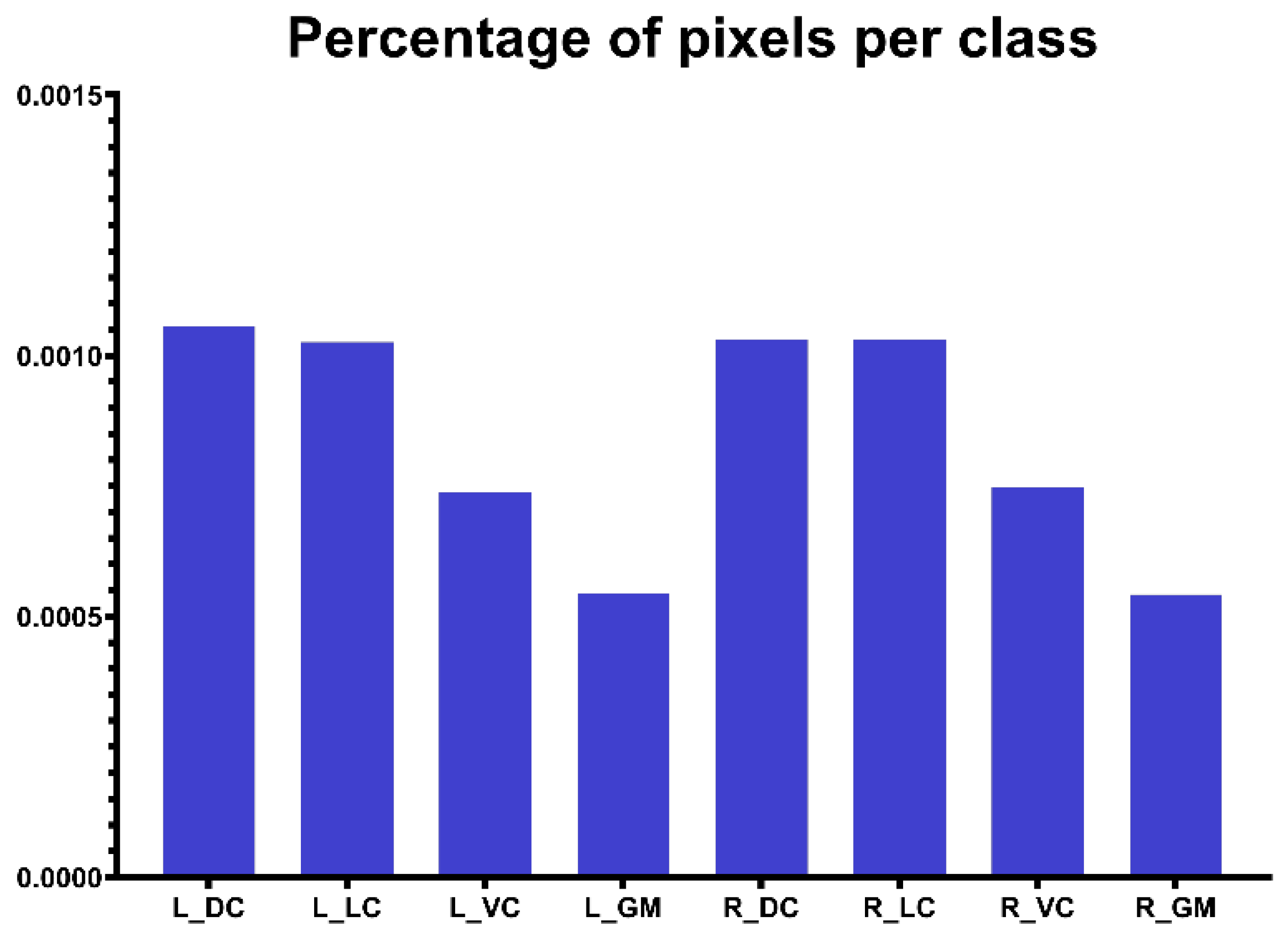
2.4. Training and Evaluation
3. Results
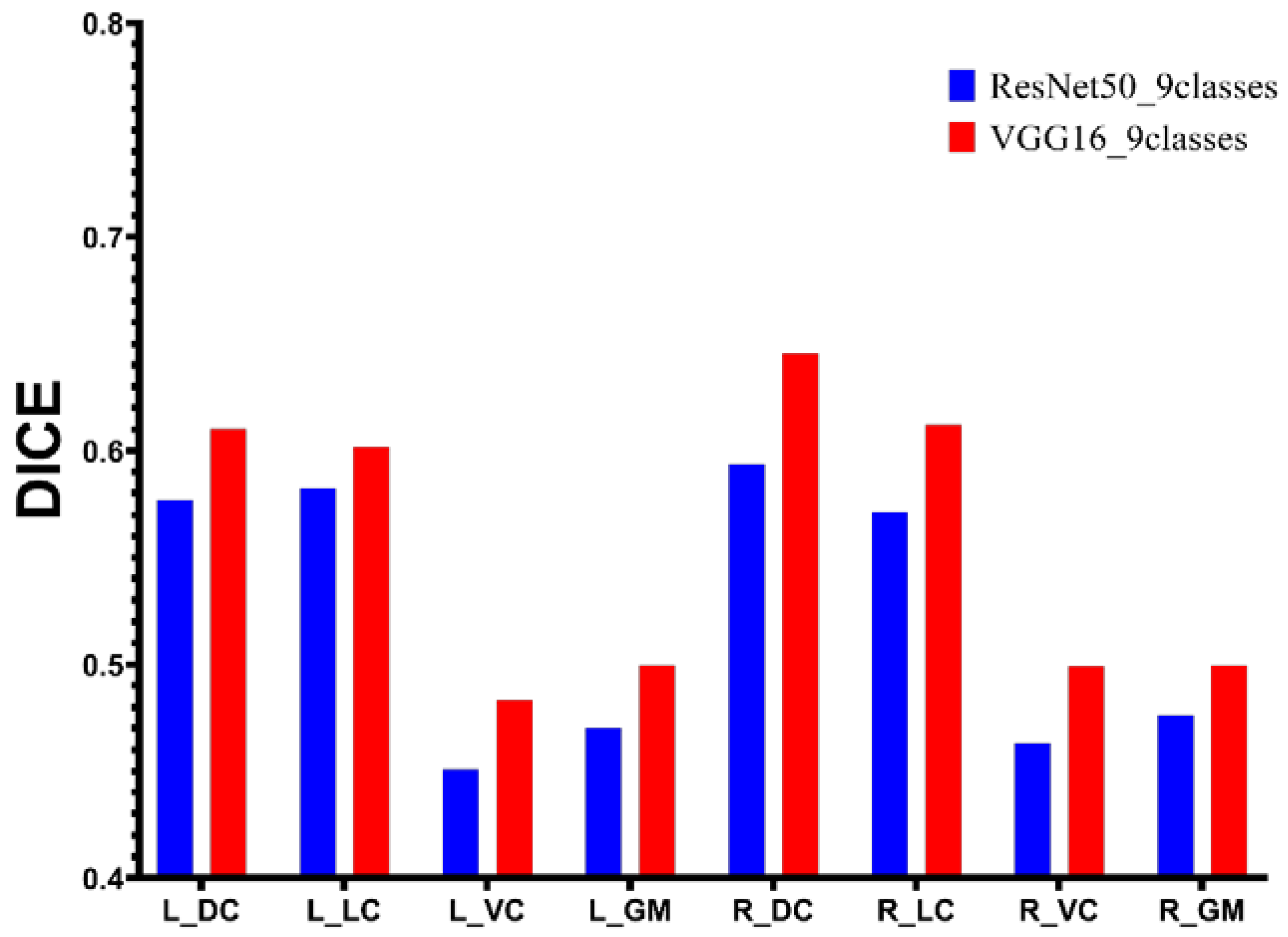
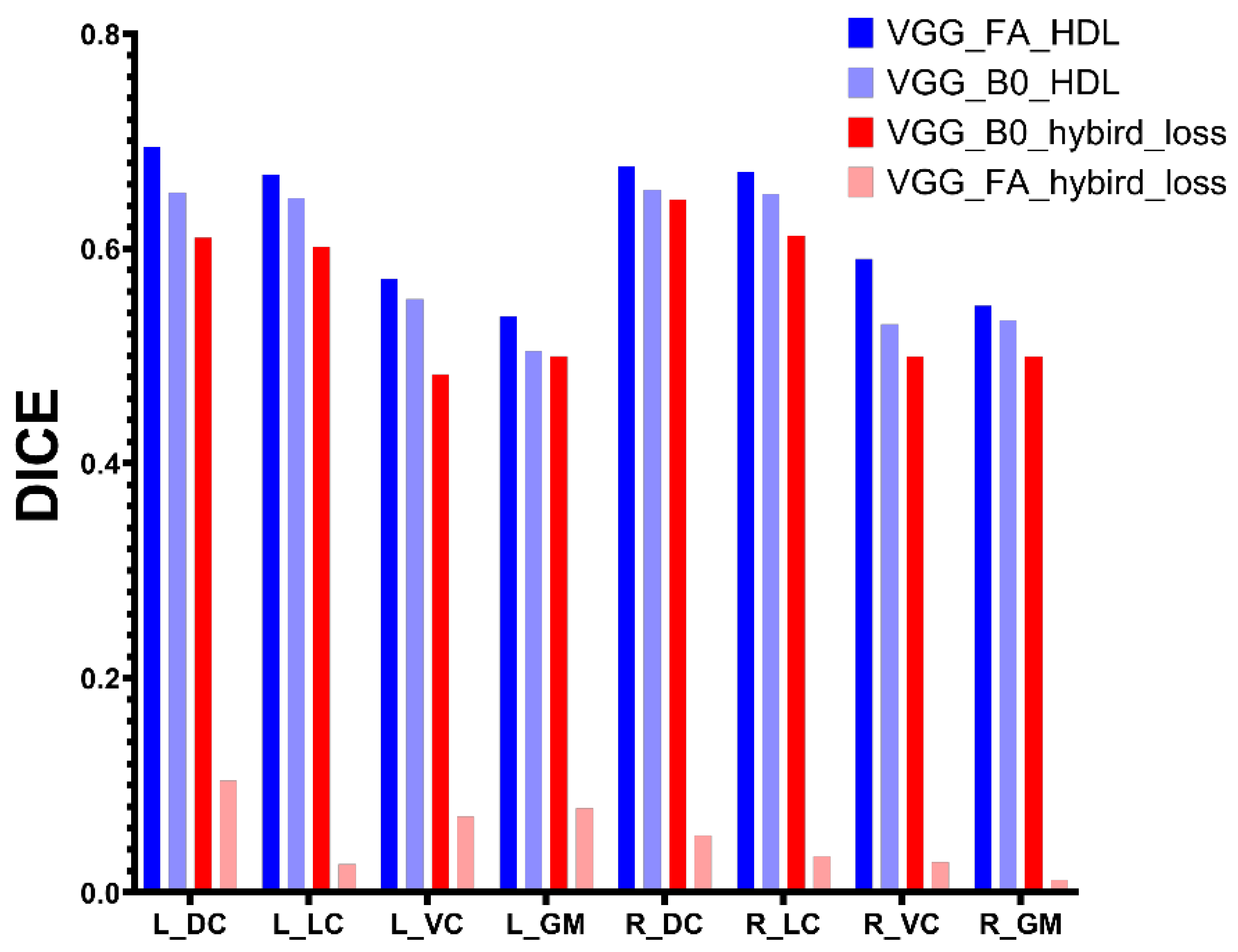
3.1. Encoder Comparison
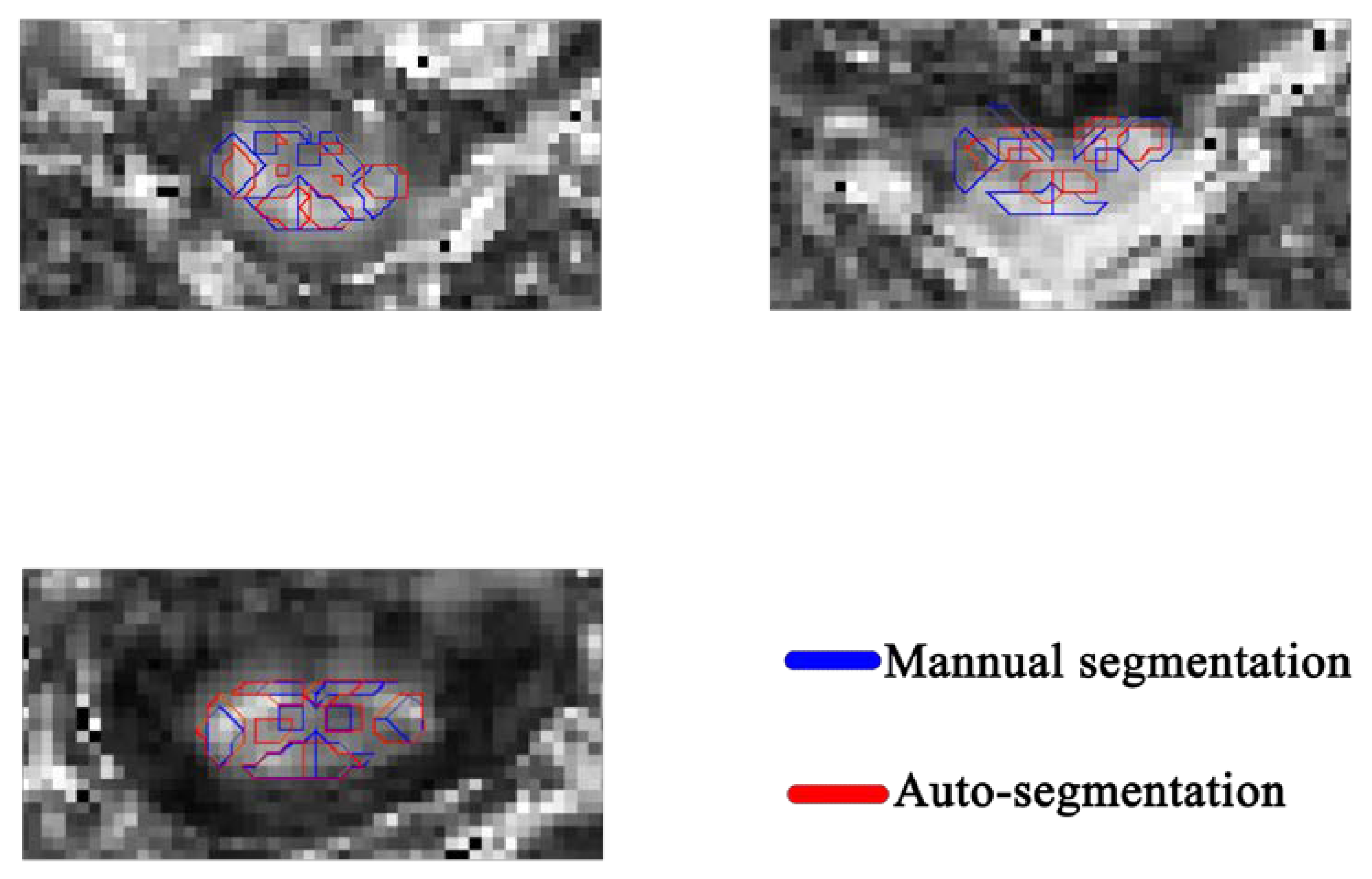
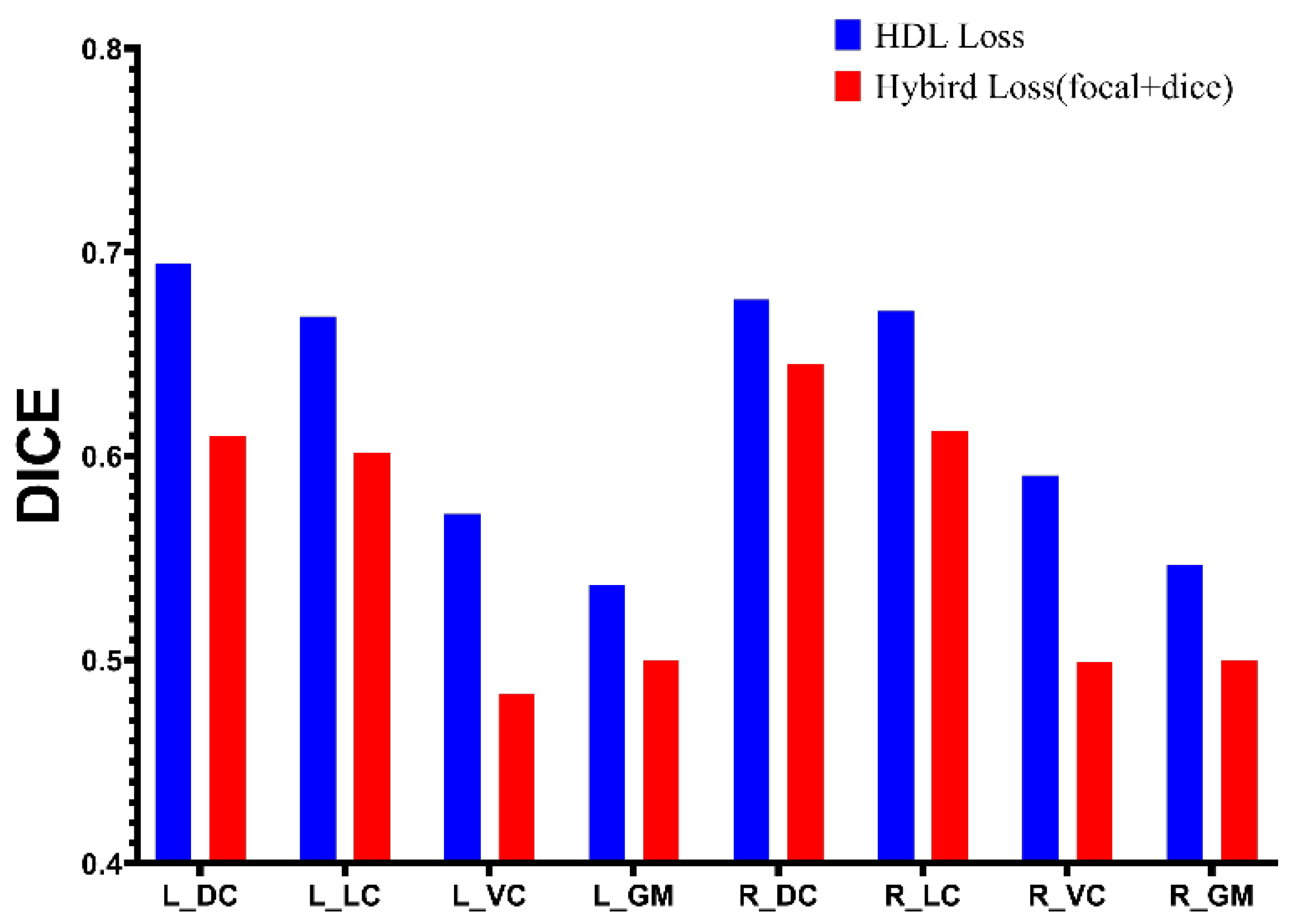
3.2. Model Performance
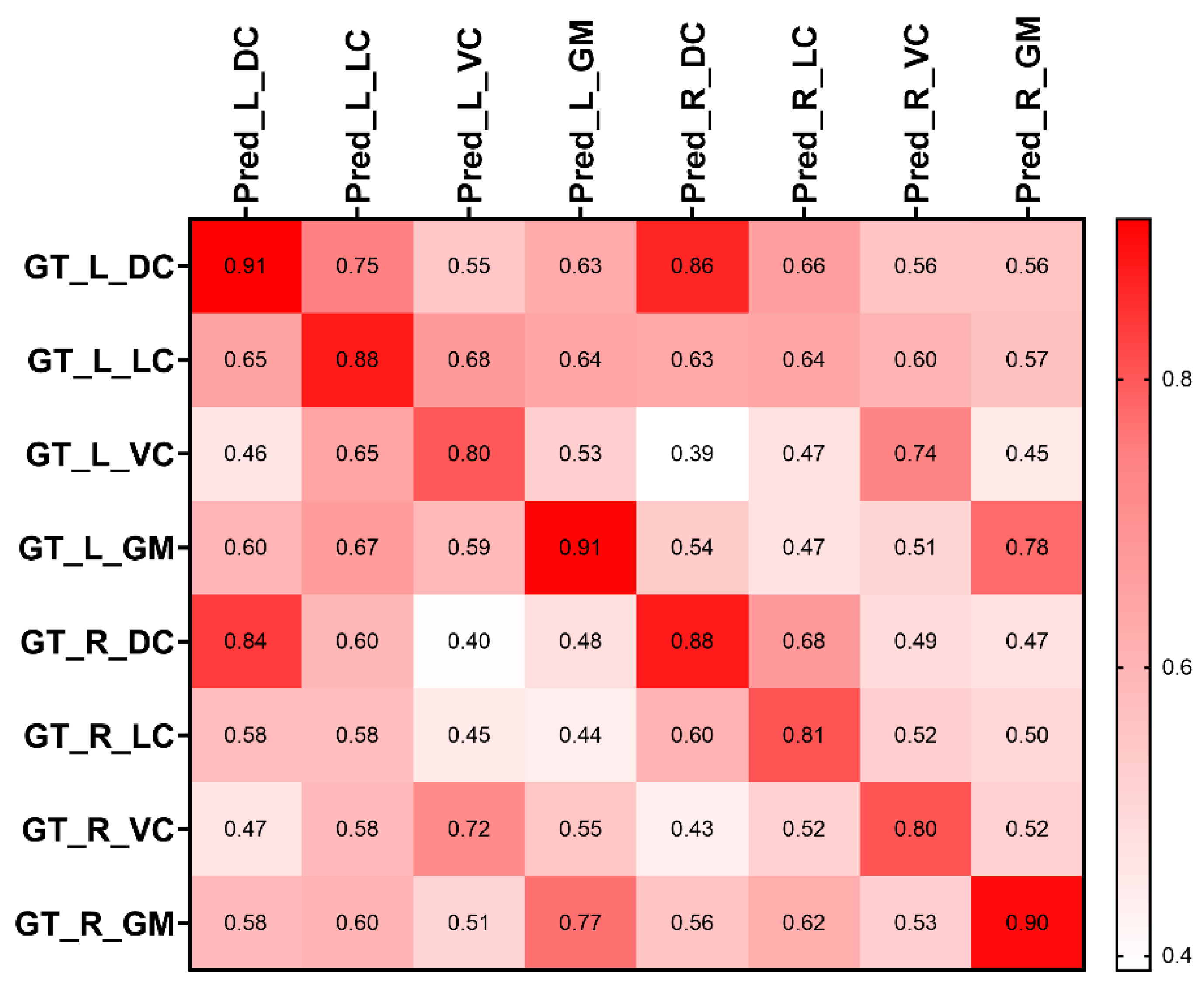
3.3. Accuracy of FA Prediction
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Wang, K.; Chen, Z.; Zhang, F.; Song, Q.-x.; Hou, C.-l.; Tang, Y.-x.; Wang, J.; Chen, S.; Bian, Y.; Hao, Q.; et al. Evaluation of DTI Parameter Ratios and Diffusion Tensor Tractography Grading in the Diagnosis and Prognosis Prediction of Cervical Spondylotic Myelopathy. Spine 2017, 42, E202–E210. [Google Scholar] [CrossRef] [PubMed]
- Shabani, S.; Kaushal, M.; Budde, M.D.; Wang, M.C.; Kurpad, S. Diffusion tensor imaging in cervical spondylotic myelopathy: A review. J. Neurosurg. Spine 2020, 1–8. [Google Scholar] [CrossRef]
- Quencer, R.M. Cervical myelopathy: Imaging/clinical correlations and the application of evolving magnetic resonance imaging techniques in cervical spinal cord abnormalities. Spine (Phila Pa 1976) 2001, 26, 2411–2413. [Google Scholar] [CrossRef] [PubMed]
- Fehlings, M.G.; Martin, A.R.; Tetreault, L.A.; Aarabi, B.; Anderson, P.; Arnold, P.M.; Brodke, D.; Burns, A.S.; Chiba, K.; Dettori, J.R.; et al. A Clinical Practice Guideline for the Management of Patients With Acute Spinal Cord Injury: Recommendations on the Role of Baseline Magnetic Resonance Imaging in Clinical Decision Making and Outcome Prediction. Glob. Spine J. 2017, 7, 221S–230S. [Google Scholar] [CrossRef] [Green Version]
- Fehlings, M.G.; Tetreault, L.A.; Riew, K.D.; Middleton, J.W.; Aarabi, B.; Arnold, P.M.; Brodke, D.S.; Burns, A.S.; Carette, S.; Chen, R.; et al. A Clinical Practice Guideline for the Management of Patients With Degenerative Cervical Myelopathy: Recommendations for Patients With Mild, Moderate, and Severe Disease and Nonmyelopathic Patients With Evidence of Cord Compression. Glob. Spine J. 2017, 7, 70S–83S. [Google Scholar] [CrossRef] [Green Version]
- Kurpad, S.; Martin, A.R.; Tetreault, L.A.; Fischer, D.J.; Skelly, A.C.; Mikulis, D.; Flanders, A.; Aarabi, B.; Mroz, T.E.; Tsai, E.C.; et al. Impact of Baseline Magnetic Resonance Imaging on Neurologic, Functional, and Safety Outcomes in Patients With Acute Traumatic Spinal Cord Injury. Glob. Spine J. 2017, 7, 151S–174S. [Google Scholar] [CrossRef] [Green Version]
- Ahuja, C.S.; Wilson, J.R.; Nori, S.; Kotter, M.R.N.; Druschel, C.; Curt, A.; Fehlings, M.G. Traumatic spinal cord injury. Nat. Rev. Dis. Prim. 2017, 3, 21. [Google Scholar] [CrossRef] [Green Version]
- Talbott, J.F.; Whetstone, W.D.; Readdy, W.J.; Ferguson, A.R.; Bresnahan, J.C.; Saigal, R.; Hawryluk, G.W.J.; Beattie, M.S.; Mabray, M.C.; Pan, J.Z.; et al. The Brain and Spinal Injury Center score: A novel, simple, and reproducible method for assessing the severity of acute cervical spinal cord injury with axial T2-weighted MRI findings. J. Neurosurg.-Spine 2015, 23, 495–504. [Google Scholar] [CrossRef] [Green Version]
- Lee, E.; Lee, J.W.; Bae, Y.J.; Kim, H.J.; Kang, Y.; Ahn, J.M. Reliability of pre-operative diffusion tensor imaging parameter measurements of the cervical spine in patients with cervical spondylotic myelopathy. Sci. Rep. 2020, 10, 17410. [Google Scholar] [CrossRef]
- Cui, J.L.; Cui, J.L.; Wen, C.Y.; Wen, C.Y.; Hu, Y.; Hu, Y.; Mak, K.C.; Mak, K.C.; Mak, K.H.H.; Mak, K.H.H.; et al. Orientation entropy analysis of diffusion tensor in healthy and myelopathic spinal cord. Neuroimage 2011, 58, 1028. [Google Scholar] [CrossRef]
- Jin, R.; Luk, K.D.; Cheung, J.P.Y.; Hu, Y. Prognosis of cervical myelopathy based on diffusion tensor imaging with artificial intelligence methods. NMR Biomed. 2019, 32, e4114. [Google Scholar] [CrossRef] [PubMed]
- Li, X.; Cui, J.-L.; Mak, K.-C.; Luk, K.D.-K.; Hu, Y. Potential Use of Diffusion Tensor Imaging in Level Diagnosis of Multilevel Cervical Spondylotic Myelopathy. Spine 2014, 39, E615–E622. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chan, T.Y.; Li, X.; Mak, K.C.; Cheung, J.P.; Luk, K.D.; Hu, Y. Normal values of cervical spinal cord diffusion tensor in young and middle-aged healthy Chinese. Eur. Spine J. 2015, 24, 2991–2998. [Google Scholar] [CrossRef] [PubMed]
- Jin, R.C.; Hu, Y. Effect of segmentation from different diffusive metric maps on diffusion tensor imaging analysis of the cervical spinal cord. Quant. Imaging Med. Surg. 2019, 9, 292–303. [Google Scholar] [CrossRef]
- Fonov, V.S.; Troter, A.L.; Taso, M.; Leener, B.D.; Lévêque, G.; Benhamou, M.; Sdika, M.; Benali, H.; Pradat, P.; Collins, D.L.; et al. Framework for integrated MRI average of the spinal cord white and gray matter: The MNI–Poly–AMU template. Neuroimage 2014, 102, 817–827. [Google Scholar] [CrossRef]
- El Mendili, M.-M.; Chen, R.; Tiret, B.; Villard, N.; Trunet, S.; Pélégrini-Issac, M.; Lehéricy, S.; Pradat, P.-F.; Benali, H. Fast and Accurate Semi-Automated Segmentation Method of Spinal Cord MR Images at 3T Applied to the Construction of a Cervical Spinal Cord Template. PLoS ONE 2015, 10, e0122224. [Google Scholar] [CrossRef]
- Leener, B.D.; Cohen-Adad, J.; Kadoury, S. Automatic Segmentation of the Spinal Cord and Spinal Canal Coupled With Vertebral Labeling. IEEE Trans. Med. Imaging 2015, 34, 1705–1718. [Google Scholar] [CrossRef]
- Chen, M.; Carass, A.; Oh, J.; Nair, G.; Pham, D.L.; Reich, D.S.; Prince, J.L. Automatic magnetic resonance spinal cord segmentation with topology constraints for variable fields of view. Neuroimage 2013, 83, 1051–1062. [Google Scholar] [CrossRef] [Green Version]
- Horváth, A.; Pezold, S.; Weigel, M.; Parmar, K.; Bieri, O.; Cattin, P.C. Variational Segmentation of the White and Gray Matter in the Spinal Cord Using a Shape Prior. In Computational Methods and Clinical Applications for Spine Imaging; Springer: Cham, Switzerland, 2016. [Google Scholar]
- Prados, F.; Cardoso, M.J.; Yiannakas, M.C.; Hoy, L.R.; Tebaldi, E.; Kearney, H.; Liechti, M.D.; Miller, D.H.; Ciccarelli, O.; Wheeler-Kingshott, C.A.M.; et al. Fully automated grey and white matter spinal cord segmentation. Sci. Rep. 2016, 6, 36151. [Google Scholar] [CrossRef] [Green Version]
- Dostál, M.; Keřkovský, M.; Korit Áková, E.; Němcová, E.; Stulík, J.; Staňková, M.; Bernard, V. Analysis of diffusion tensor measurements of the human cervical spinal cord based on semiautomatic segmentation of the white and gray matter. J. Magn. Reson. Imaging JMRI 2018, 48, 1217–1227. [Google Scholar] [CrossRef]
- Ronneberger, O.; Fischer, P.; Brox, T. U-net: Convolutional networks for biomedical image segmentation. In Proceedings of the International Conference on Medical Image Computing and Computer-Assisted Intervention, Munich, Germany, 5–9 October 2015; pp. 234–241. [Google Scholar]
- Zhang, X.; Li, Y.; Liu, Y.; Tang, S.X.; Liu, X.; Punithakumar, K.; Shi, D. Automatic spinal cord segmentation from axial-view MRI slices using CNN with grayscale regularized active contour propagation. Comput. Biol. Med. 2021, 132, 104345. [Google Scholar] [CrossRef] [PubMed]
- Alsenan, A.; Youssef, B.B.; Alhichri, H. A Deep Learning Model based on MobileNetV3 and UNet for Spinal Cord Gray Matter Segmentation. In Proceedings of the 2021 44th International Conference on Telecommunications and Signal Processing (TSP), Virtual, 26–28 July 2021; pp. 244–248. [Google Scholar]
- De Leener, B.; Lévy, S.; Dupont, S.M.; Fonov, V.S.; Stikov, N.; Louis Collins, D.; Callot, V.; Cohen-Adad, J. SCT: Spinal Cord Toolbox, an open-source software for processing spinal cord MRI data. Neuroimage 2017, 145, 24–43. [Google Scholar] [CrossRef]
- Simonyan, K.; Zisserman, A. Very deep convolutional networks for large-scale image recognition. arXiv 2014, arXiv:1409.1556. [Google Scholar]
- He, K.; Zhang, X.; Ren, S.; Sun, J. Deep residual learning for image recognition. In Proceedings of the IEEE Conference on Computer Vision and Pattern Recognition, Las Vegas, NV, USA, 26 June–1 July 2016; pp. 770–778. [Google Scholar]
- Zhu, W.; Huang, Y.; Zeng, L.; Chen, X.; Liu, Y.; Qian, Z.; Du, N.; Fan, W.; Xie, X. AnatomyNet: Deep learning for fast and fully automated whole-volume segmentation of head and neck anatomy. Med. Phys. 2019, 46, 576–589. [Google Scholar] [CrossRef] [Green Version]
- Tsai, A. Anatomical landmark localization via convolutional neural networks for limb-length discrepancy measurements. Pediatr. Radiol. 2021, 51, 1431–1447. [Google Scholar] [CrossRef] [PubMed]
- Zhu, Q.K.; Du, B.; Yan, P.K. Boundary-Weighted Domain Adaptive Neural Network for Prostate MR Image Segmentation. IEEE Trans. Med. Imaging 2020, 39, 753–763. [Google Scholar] [CrossRef] [PubMed]
- Leener, B.D.; Kadoury, S.; Cohen-Adad, J. Robust, accurate and fast automatic segmentation of the spinal cord. Neuroimage 2014, 98, 528–536. [Google Scholar] [CrossRef]
- Yiannakas, M.C.; Mustafa, A.M.; De Leener, B.; Kearney, H.; Tur, C.; Altmann, D.R.; De Angelis, F.; Plantone, D.; Ciccarelli, O.; Miller, D.H.; et al. Fully automated segmentation of the cervical cord from T1-weighted MRI using PropSeg: Application to multiple sclerosis. NeuroImage. Clin. 2016, 10, 71–77. [Google Scholar] [CrossRef] [Green Version]
- Fouladivanda, M.; Kazemi, K.; Helfroush, M.S.; Shakibafard, A. Morphological active contour driven by local and global intensity fitting for spinal cord segmentation from MR images. J. Neurosci. Methods 2018, 308, 116–128. [Google Scholar] [CrossRef]
- Sabaghian, S.; Dehghani, H.; Batouli, S.A.H.; Khatibi, A.; Oghabian, M.A. Fully automatic 3D segmentation of the thoracolumbar spinal cord and the vertebral canal from T2-weighted MRI using K-means clustering algorithm. Spinal Cord 2020, 58, 811–820. [Google Scholar] [CrossRef]
- Cadotte, A.; Cadotte, D.W.; Livne, M.; Cohen-Adad, J.; Fleet, D.; Mikulis, D.J.; Fehlings, M.G. Spinal Cord Segmentation by One Dimensional Normalized Template Matching: A Novel, Quantitative Technique to Analyze Advanced Magnetic Resonance Imaging Data. PLoS ONE 2015, 10, e0139323. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- van Hecke, W.; Leemans, A.; Sijbers, J.; Vandervliet, E.; Van Goethem, J.W.; Parizel, P.M. A tracking-based diffusion tensor imaging segmentation method for the detection of diffusion-related changes of the cervical spinal cord with aging. J. Magn. Reson. Imaging 2008, 27, 978–991. [Google Scholar] [CrossRef]
- Gros, C.; Leener, B.D.; Badji, A.; Maranzano, J.; Eden, D.; Dupont, S.M.; Talbott, J.F.; Zhuoquiong, R.; Liu, Y.; Granberg, T.; et al. Automatic segmentation of the spinal cord and intramedullary multiple sclerosis lesions with convolutional neural networks. Neuroimage 2019, 184, 901–915. [Google Scholar] [CrossRef] [Green Version]
- Datta, E.; Papinutto, N.; Schlaeger, R.; Zhu, A.H.; Carballido-Gamio, J.; Henry, R.G. Gray matter segmentation of the spinal cord with active contours in MR images. Neuroimage 2017, 147, 788–799. [Google Scholar] [CrossRef] [PubMed]
- Dupont, S.M.; Leener, B.D.; Taso, M.; Troter, A.L.; Nadeau, S.; Stikov, N.; Callot, V.; Cohen-Adad, J. Fully-integrated framework for the segmentation and registration of the spinal cord white and gray matter. Neuroimage 2017, 150, 358–372. [Google Scholar] [CrossRef]
- Prados, F.; Ashburner, J.; Blaiotta, C.; Brosch, T.; Carballido-Gamio, J.; Cardoso, M.J.; Conrad, B.N.; Datta, E.; Dávid, G.; Leener, B.D.; et al. Spinal cord grey matter segmentation challenge. Neuroimage 2017, 152, 312–329. [Google Scholar] [CrossRef] [Green Version]
- Perone, C.S.; Calabrese, E.; Cohen-Adad, J. Spinal cord gray matter segmentation using deep dilated convolutions. Sci. Rep. 2018, 8, 5966. [Google Scholar] [CrossRef] [PubMed]
- Wang, S.Q.; Li, X.; Cui, J.L.; Li, H.X.; Luk, K.D.K.; Hu, Y. Prediction of myelopathic level in cervical spondylotic myelopathy using diffusion tensor imaging. J. Magn. Reson. Imaging 2015, 41, 1682–1688. [Google Scholar] [CrossRef] [Green Version]
- Skotarczak, M.; Dzierzanowski, J.; Kaszubowski, M.; Winklewski, P.J.; Romanowski, A.; Szurowska, E.; Szarmach, A. Diagnostic value of diffusion tensor imaging in patients with clinical signs of cervical spondylotic myelopathy. Neurol. Neurochir. Pol. 2022, 56, 341–348. [Google Scholar] [CrossRef]
- Scholler, K.; Siller, S.; Brem, C.; Lutz, J.; Zausinger, S. Diffusion Tensor Imaging for Surgical Planning in Patients with Cervical Spondylotic Myelopathy. J. Neurol. Surg. Part A 2020, 81, 1–9. [Google Scholar] [CrossRef]
- Ellingson, B.M.; Salamon, N.; Woodworth, D.C.; Yokota, H.; Holly, L.T. Reproducibility, temporal stability, and functional correlation of diffusion MR measurements within the spinal cord in patients with asymptomatic cervical stenosis or cervical myelopathy. J. Neurosurg.-Spine 2018, 28, 472–480. [Google Scholar] [CrossRef] [Green Version]
- Wen, C.Y.; Cui, J.L.; Liu, H.S.; Mak, K.C.; Cheung, W.Y.; Luk, K.D.K.; Hu, Y. Is Diffusion Anisotropy a Biomarker for Disease Severity and Surgical Prognosis of Cervical Spondylotic Myelopathy? Radiology 2014, 270, 197–204. [Google Scholar] [CrossRef]
- Borkowski, K.; Krzyzak, A.T. Assessment of the systematic errors caused by diffusion gradient inhomogeneity in DTI-computer simulations. NMR Biomed. 2019, 32, e4130. [Google Scholar] [CrossRef] [PubMed]
- Ahn, C.B.; Cho, Z.H. ANALYSIS OF THE EDDY-CURRENT INDUCED ARTIFACTS AND THE TEMPORAL COMPENSATION IN NUCLEAR-MAGNETIC-RESONANCE IMAGING. IEEE Trans. Med. Imaging 1991, 10, 47–52. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Pierpaoli, C.; Basser, P.J. Toward a quantitative assessment of diffusion anisotropy. Magn. Reson. Med. 1996, 36, 893–906. [Google Scholar] [CrossRef]
- Borkowski, K.; Krzyżak, A.T. Analysis and correction of errors in DTI-based tractography due to diffusion gradient inhomogeneity. J. Magn. Reson. 2018, 296, 5–11. [Google Scholar] [CrossRef]
- Bammer, R.; Markl, M.; Barnett, A.; Acar, B.; Alley, M.T.; Pelc, N.J.; Glover, G.H.; Moseley, M.E. Analysis and generalized correction of the effect of spatial gradient field distortions in diffusion-weighted imaging. Magn. Reson. Med. 2003, 50, 560–569. [Google Scholar] [CrossRef] [PubMed]
- Tan, E.T.; Marinelli, L.; Slavens, Z.W.; King, K.F.; Hardy, C.J. Improved correction for gradient nonlinearity effects in diffusion-weighted imaging. J. Magn. Reson. Imaging 2013, 38, 448–453. [Google Scholar] [CrossRef]
- Krzyżak, A.T.; Olejniczak, Z. Improving the accuracy of PGSE DTI experiments using the spatial distribution of b matrix. Magn. Reson. Imaging 2015, 33, 286–295. [Google Scholar] [CrossRef]
- Rogers, B.P.; Blaber, J.; Welch, E.B.; Ding, Z.; Anderson, A.W.; Landman, B.A. Stability of Gradient Field Corrections for Quantitative Diffusion MRI. In Proceedings of the SPIE Medical Imaging, Orlando, FL, USA, 11–16 February 2017; Volume 10132. [Google Scholar] [CrossRef] [Green Version]
- Kłodowski, K.; Krzyżak, A.T. Innovative anisotropic phantoms for calibration of diffusion tensor imaging sequences. Magn. Reson. Imaging 2016, 34, 404–409. [Google Scholar] [CrossRef]
- Zhu, T.; Hu, R.; Qiu, X.; Taylor, M.; Tso, Y.; Yiannoutsos, C.; Navia, B.; Mori, S.; Ekholm, S.; Schifitto, G.; et al. Quantification of accuracy and precision of multi-center DTI measurements: A diffusion phantom and human brain study. Neuroimage 2011, 56, 1398–1411. [Google Scholar] [CrossRef] [Green Version]
- Melhem, E.R.; Itoh, R.; Jones, L.; Barker, P.B. Diffusion tensor MR imaging of the brain: Effect of diffusion weighting on trace and anisotropy measurements. Am. J. Neuroradiol. 2000, 21, 1813–1820. [Google Scholar] [PubMed]
- Qin, W.; Yu, C.S.; Zhang, F.; Du, X.Y.; Jiang, H.; Yan, Y.X.; Li, K.C. Effects of Echo Time on Diffusion Quantification of Brain White Matter at 1.5T and 3.0T. Magn. Reson. Med. 2009, 61, 755–760. [Google Scholar] [CrossRef] [PubMed]
- Ni, H.; Kavcic, V.; Zhu, T.; Ekholm, S.; Zhong, J. Effects of number of diffusion gradient directions on derived diffusion tensor imaging indices in human brain. Am. J. Neuroradiol. 2006, 27, 1776–1781. [Google Scholar] [PubMed]
- Widjaja, E.; Mahmoodabadi, S.Z.; Rea, D.; Moineddin, R.; Vidarsson, L.; Nilsson, D. Effects of Gradient Encoding and Number of Signal Averages on Fractional Anisotropy and Fiber Density Index In Vivo at 1.5 Tesla. Acta Radiol. 2009, 50, 106–113. [Google Scholar] [CrossRef] [PubMed]









{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Class | Dice | Recall | Precision |
|---|---|---|---|
| Left dorsal column | 0.69 ± 0.19 | 0.78 ± 0.23 | 0.64 ± 0.2 |
| Left lateral column | 0.67 ± 0.24 | 0.74 ± 0.29 | 0.63 ± 0.23 |
| Left ventral column | 0.57 ± 0.29 | 0.62 ± 0.33 | 0.55 ± 0.28 |
| Left gray matter | 0.54 ± 0.28 | 0.59 ± 0.33 | 0.53 ± 0.28 |
| Right dorsal column | 0.68 ± 0.21 | 0.74 ± 0.25 | 0.65 ± 0.2 |
| Right lateral column | 0.67 ± 0.22 | 0.74 ± 0.26 | 0.65 ± 0.22 |
| Right ventral column | 0.59 ± 0.26 | 0.63 ± 0.29 | 0.58 ± 0.27 |
| Right gray matter | 0.55 ± 0.31 | 0.56 ± 0.34 | 0.57 ± 0.32 |
| Class | Dice | Recall | Precision | Outliers |
|---|---|---|---|---|
| Left dorsal column | 0.69 ± 0.19 | 0.78 ± 0.23 | 0.64 ± 0.2 | 0 |
| Left lateral column | 0.68 ± 0.23 | 0.76 ± 0.27 | 0.64 ± 0.21 | 2% |
| Left ventral column | 0.61 ± 0.25 | 0.67 ± 0.3 | 0.59 ± 0.25 | 7% |
| Left gray matter | 0.57 ± 0.25 | 0.63 ± 0.3 | 0.56 ± 0.25 | 7% |
| Right dorsal column | 0.68 ± 0.2 | 0.74 ± 0.24 | 0.66 ± 0.2 | 1% |
| Right lateral column | 0.69 ± 0.18 | 0.76 ± 0.23 | 0.67 ± 0.19 | 3% |
| Right ventral column | 0.63 ± 0.23 | 0.67 ± 0.26 | 0.61 ± 0.24 | 6% |
| Right gray matter | 0.61 ± 0.27 | 0.63 ± 0.3 | 0.63 ± 0.27 | 10% |
| Class | |
|---|---|
| Left dorsal column | 0.07 ± 0.07 |
| Left lateral column | 0.07 ± 0.11 |
| Left ventral column | 0.11 ± 0.17 |
| Left gray matter | 0.08 ± 0.14 |
| Right dorsal column | 0.07 ± 0.08 |
| Right lateral column | 0.1 ± 0.11 |
| Right ventral column | 0.1 ± 0.23 |
| Right gray matter | 0.07 ± 0.09 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Fei, N.; Li, G.; Wang, X.; Li, J.; Hu, X.; Hu, Y. Deep Learning-Based Auto-Segmentation of Spinal Cord Internal Structure of Diffusion Tensor Imaging in Cervical Spondylotic Myelopathy. Diagnostics 2023, 13, 817. https://doi.org/10.3390/diagnostics13050817
Fei N, Li G, Wang X, Li J, Hu X, Hu Y. Deep Learning-Based Auto-Segmentation of Spinal Cord Internal Structure of Diffusion Tensor Imaging in Cervical Spondylotic Myelopathy. Diagnostics. 2023; 13(5):817. https://doi.org/10.3390/diagnostics13050817
Chicago/Turabian StyleFei, Ningbo, Guangsheng Li, Xuxiang Wang, Junpeng Li, Xiaosong Hu, and Yong Hu. 2023. "Deep Learning-Based Auto-Segmentation of Spinal Cord Internal Structure of Diffusion Tensor Imaging in Cervical Spondylotic Myelopathy" Diagnostics 13, no. 5: 817. https://doi.org/10.3390/diagnostics13050817