
Feasibility Study of an Internet-Based Platform for Tele-Neuropsychological Assessment of Elderly in Remote Areas

 ,
,  , and
, and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Participants and Protocol
2.2. Procedure/Protocol
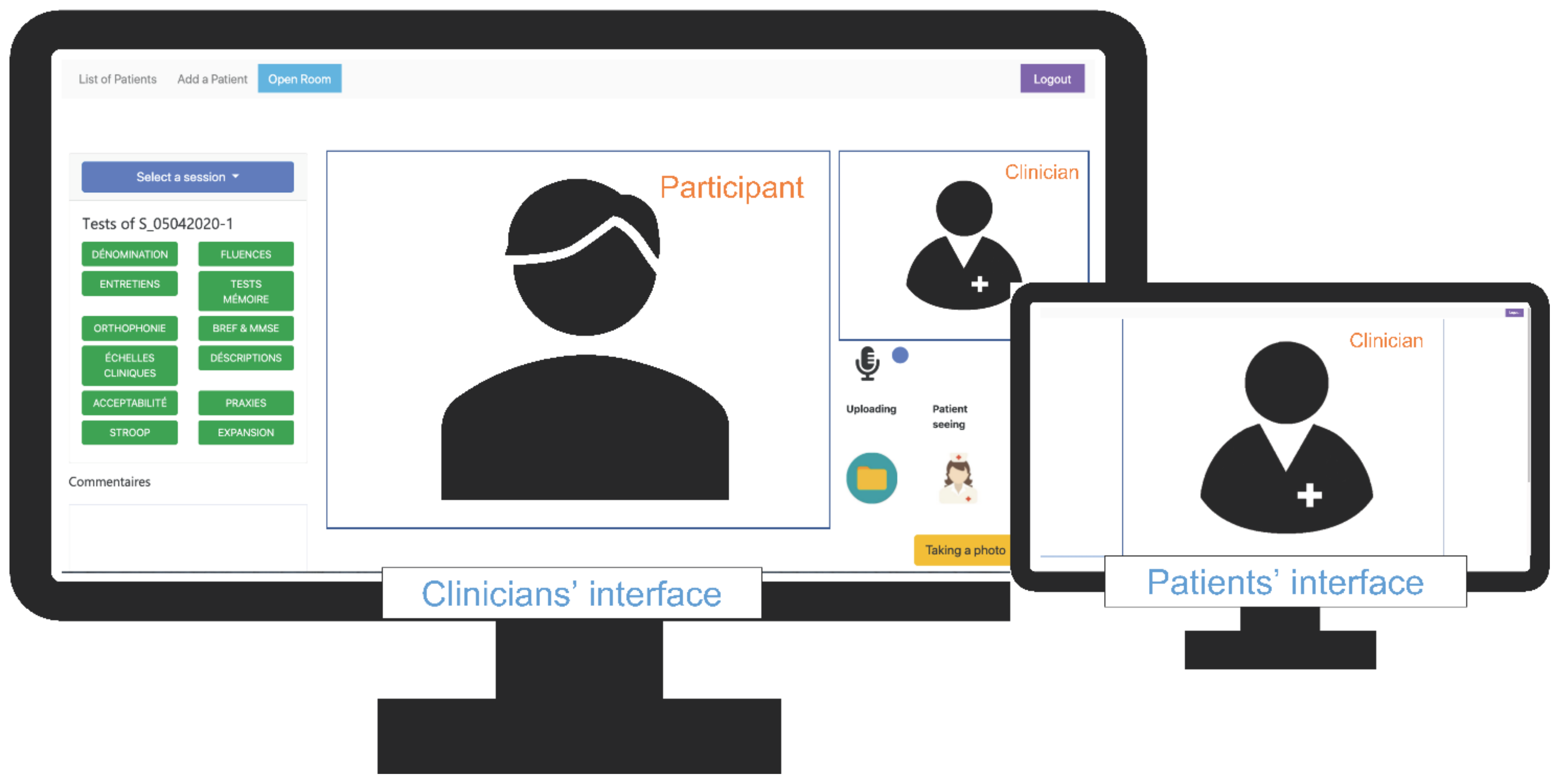
2.3. The Tele-Neuropsychology System: PsyTime
2.4. Acceptability Evaluation
2.5. Data Analysis
2.6. Data Collection and Availability
3. Results
4. Discussion
5. Limitations
6. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Legendre, B. En 2018, Les Territoires Sous-Dotés En Médecins Généralistes Concernent Près De 6% De La Population. In DREES; France. 2020; p. 6. Available online: https://drees.solidarites-sante.gouv.fr/ (accessed on 6 April 2022).
- Helmer, C.; Berr, C.; Dartigues, J.F. Epidémiologie des Démences et Facteurs de Risque Modifiables. In Démences; Doin Editions: Ballan-Miré, France, 2015; p. 33. [Google Scholar]
- Geddes, M.R.; O’Connell, M.E.; Fisk, J.D.; Gauthier, S.; Camicioli, R.; Ismail, Z. Remote cognitive and behavioral assessment: Report of the Alzheimer Society of Canada Task Force on dementia care best practices for COVID-19. Alzheimer’s Dement. Diagn. Assess. Dis. Monit. 2020, 12, e12111. [Google Scholar] [CrossRef] [PubMed]
- Marra, D.E.; Hamlet, K.M.; Bauer, R.M.; Bowers, D. Validity of teleneuropsychology for older adults in response to COVID-19: A systematic and critical review. Clin. Neuropsychol. 2020, 34, 1411–1452. [Google Scholar] [CrossRef] [PubMed]
- Brearly, T.W.; Shura, R.D.; Martindale, S.L.; Lazowski, R.A.; Luxton, D.D.; Shenal, B.V.; Rowland, J.A. Neuropsychological Test Administration by Videoconference: A Systematic Review and Meta-Analysis. Neuropsychol. Rev. 2017, 27, 174–186. [Google Scholar] [CrossRef] [PubMed]
- Genoud-Prachex, T.; Perrenoud, M.P.; Guevara, A.B.; Bieler-Aeschlimann, M.; Moser, C.; Rouaud, O.; Démonet, J.-F. Télé-neuropsychologie: Nouvelles technologies et outils évaluatifs. Rev. Neuropsychol. 2020, 12, 341–350. [Google Scholar]
- Tornatore, J.B.; Hill, E.; Anne Laboff, J.; Mary McGann, M.E. Self-Administered Screening for Mild Cognitive Impairment: Initial Validation of a Computerized Test Battery. J. Neuropsychiatry Clin. Neurosci. 2005, 17, 98–105. [Google Scholar] [CrossRef] [PubMed]
- Germine, L.; Reinecke, K.; Chaytor, N.S. Digital neuropsychology: Challenges and opportunities at the intersection of science and software. Clin. Neuropsychol. 2019, 33, 271–286. [Google Scholar] [CrossRef] [PubMed]
- Kitaigorodsky, M.; Loewenstein, D.; Curiel Cid, R.; Crocco, E.; Gorman, K.; González-Jiménez, C. A Teleneuropsychology Protocol for the Cognitive Assessment of Older Adults During COVID-19. Front. Psychol. 2021, 12, 1684. [Google Scholar] [CrossRef] [PubMed]
- Owens, A.P.; Ballard, C.; Beigi, M.; Kalafatis, C.; Brooker, H.; Lavelle, G.; Brønnick, K.K.; Sauer, J.; Boddington, S.; Velayudhan, L.; et al. Implementing Remote Memory Clinics to Enhance Clinical Care During and After COVID-19. Front. Psychiatry. 2020, 11, 1–15. [Google Scholar] [CrossRef] [PubMed]
- Folstein, M.F.; Robins, L.N.; Helzer, J.E. The Mini-Mental State Examination. Arch. Gen. Psychiatry. 1983, 40, 812. [Google Scholar] [CrossRef] [PubMed]
- Van der Linden, M.; Coyette, F.; Poitrenaud, J.; Kalafat, M.; Calacis, F.; Wyns, C.; Adam, S.; Members of GREMEM. L’épreuve de rappel libre/rappel indicé à 16 items (RL/RI-16. In L’évaluation des Troubles de la Mémoire: Présentation de Quatre Tests de Mémoire Episodique (Avec LEUR Etalonnage); Van der Liden, M., Adam, S., Agniel, A., Baisset Mouly, C., Eds.; Solal: Marseille, France, 2004; pp. 25–47. [Google Scholar]
- Stroop, J.R. Studies of interference in serial verbal reactions. J. Exp. Psychol. 1935, 18, 643–662. [Google Scholar] [CrossRef]
- Cardebat, D.; Doyon, B.; Puel, M.; Goulet, P.; Joanette, Y. Evocation lexicale formelle et sémantique chez des sujets normaux. Performances et dynamiques de production en fonction du sexe, de l’âge et du niveau d’étude. Acta Neurol. Belg. 1990, 90, 207–217. [Google Scholar]
- de Partz de Courtray, M.P.; Bilocq, V.; De Wilde, V.; Seron, X.; Agnesa, P. Lexis. In Tests Pour Le Diagnostic des Troubles Lexicaux Chez le Patient Aphasique; Solal: Marseille, France, 2001; p. 81. ISBN 978-2-90558-001-6. [Google Scholar]
- Mahieux-Laurent, F.; Fabre, C.; Galbrun, E.; Dubrulle, A.; Moroni, C. Validation of a brief screening scale evaluating praxic abilities for use in memory clinics. Evaluation in 419 controls, 127 mild cognitive impairment and 320 demented patients. Rev. Neurol. 2009, 165, 560–567. [Google Scholar] [CrossRef]
- Cummings, L. Describing the cookie theft picture: Sources of breakdown in alzheimer’s dementia. Pragmat. Soc. 2019, 10, 153–176. [Google Scholar] [CrossRef]
- König, A.; Linz, N.; Zeghari, R.; Klinge, X.; Tröger, J.; Alexandersson, J.; Robert, P. Detecting apathy in older adults with cognitive disorders using automatic speech analysis. J. Alzheimer’s Dis. 2019, 69, 1183–1193. [Google Scholar] [CrossRef] [PubMed]
- Baddeley, A.D.; Emslie, H.; Nimmo-Smith, I. Doors and People: A Test of Visual and Verbal Recall and Recognition; Thames Valley Test: Bury St. Edmunds, UK, 1994. [Google Scholar]
- Brooke, J. SUS: A “Quick and Dirty” Usability Scale. In Usability Evaluation in Industry; Jordan, B.P., Thomas, W., Weerdmeester, B.A., McClelland, I.L., Eds.; Taylor and Francis: London, UK, 1996; pp. 189–194. [Google Scholar]
- Koo, T.K.; Li, M.Y. A guideline of selecting and reporting intraclass correlation coefficients for reliability research. J. Chiropr. Med. 2016, 15, 155–163. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lam, K.; Lu, A.D.; Shi, Y.; Covinsky, K.E. Assessing Telemedicine Unreadiness Among Older Adults in the United States During the COVID-19 Pandemic. JAMA Intern. Med. 2020, 180, 1389–1391. [Google Scholar] [CrossRef] [PubMed]
- Parks, A.C.; Davis, J.; Spresser, C.D.; Stroescu, I.; Ecklund-Johnson, E. Validity of In-Home Teleneuropsychological Testing in the Wake of COVID-19. Arch. Clin. Neuropsychol. 2021, 36, 887–896. [Google Scholar] [CrossRef] [PubMed]
- Molloy, D.W.; Alemayehu, E.; Roberts, R. Reliability of a standardized mini-mental state examination compared with the traditional mini-mental state examination. Am. J. Psychiatry. 1991, 148, 102–105. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| Cognitive Functions | Cognitive Tests |
|---|---|
| Global cognitive functioning | MMSE [11] |
| Memory | Free and Cued Selective Reminding Test (FCSRT) [12] |
| Executive functions | STROOP test [13] |
| Language and Semantic Memory | Semantic and Phonological Verbal Fluency (SVF and PVF) [14] |
| Naming task (Lexis) [15] | |
| Praxis | Brief screening scale evaluating praxis abilities [16] |
| N | 50 | |||
|---|---|---|---|---|
| Sex | ||||
| Females, n (%) | 33 | (66%) | ||
| Males, n (%) | 17 | (34%) | ||
| Education | ||||
| Primary n (%) | 14 | (28%) | ||
| Secondary, n (%) | 18 | (36%) | ||
| High, n (%) | 18 | (36%) | ||
| Min | Max | |||
| Age, years Mean (SD) | 73.32 | (9.89) | 40 | 86 |
| Time delay between two assessments, in days Mean (SD) | 15.72 | (3.43) | 12 | 31 |
| MMSE Mean (SD) | 28.24 | (2.01) |
| Cognitive Tests | N | TNP | FTF | p * | ||
|---|---|---|---|---|---|---|
| MMSE 1, total score | 50 | 26.42 | (3.57) | 28.24 | (2.01) | 0.000 |
| FCSRT 2 | ||||||
| Total recall score | 42 | 43.91 | (4.65) | 42.91 | (7.12) | 0.872 |
| Delayed recall | 42 | 15.16 | (1.67) | 15.07 | (1.88) | 0.648 |
| Recognition score | 41 | 15.70 | (1.52) | 15.69 | (1.02) | 0.852 |
| Lexis, total score | 46 | 56.74 | (5.71) | 58.34 | (5.56) | 0.002 |
| Stroop | ||||||
| Color, duration (s) | 42 | 77.14 | (24.32) | 72.62 | (18.50) | 0.127 |
| Reading, duration (s) | 42 | 54.10 | (15.95) | 59.22 | (21.32) | 0.021 |
| Interference, duration (s) | 40 | 153.44 | (53.83) | 152.52 | (61.30) | 0.132 |
| SVF (z-score) | 47 | −0.33 | (1.28) | 0.34 | (3.34) | 0.256 |
| PVF (z-score) | 48 | 0.00 | (1.15) | 0.36 | (1.02) | 0.005 |
| Praxis Total score | 50 | 19.96 | (2.32) | 22.24 | (1.45) | 0.000 |
| Cognitive Tests | ICC | ||||
|---|---|---|---|---|---|
| Coefficient | Lower Bound | Upper Bound | p | ||
| MMSE | Total Score | 0.371 | 0.080 | 0.598 | 0.001 |
| FCSRT | Total recall score | 0.487 | 0.216 | 0.688 | 0.001 |
| Delayed recall | 0.269 | −0.040 | 0.529 | 0.043 | |
| Recognition score | −0.048 | −0.357 | 0.266 | 0.615 | |
| Lexis | Total score | 0.862 ** | 0.715 | 0.929 | 0.000 |
| STROOP | Color, duration (s) | 0.569 * | 0.327 | 0.741 | 0.000 |
| Reading, duration(s) | 0.439 | 0.163 | 0.652 | 0.002 | |
| Interference, duration (s) | 0.643 * | 0.421 | 0.793 | 0.000 | |
| Verbal fluency | Semantic (z-score) | 0.084 | −0.199 | 0.356 | 0.283 |
| Phonological (z-score) | 0.445 | 0.192 | 0.644 | 0.000 | |
| Praxis | Total score | 0.335 | −0.093 | 0.643 | 0.000 |
| N | Mean | (SD) | |
|---|---|---|---|
| Q1. Globally, I’m satisfied with this experience “I thought it would be more difficult for me” “The sound should be adjusted to avoid echo, reverberation” | 50 | 6.56 | (0.84) |
| Q2. Globally, the system was easy to use “childish”, “concentration was more difficult for me” “Yes, the system is easy to use” | 50 | 6.5 | (0.71) |
| Q3. Instructions were clear “But not clear enough because of the sound” “Very clear and in an accessible language.” | 50 | 6.71 | (0.59) |
| Q4. I would repeat this experience in the future “Yes, if it is necessary” “Without any problem or apprehension” | 47 | 6.53 | (1.06) |
| Q5. On a scale from 1 to 10, how likely would I recommend this assessment method? | 48 | 9.06 | (1.67) |
| Answers from the Subjects’ Experience of the TNP |
|---|
| Q8. What was missing or disappointing during your experience? (n = 23) Technical Issues “Sound problem”—“computer bug”—“computer stress”—“computer shut down to perform updates” Lack of human presence “Drink water”—“human presence” Other comments “Nothing” (n = 10)—“no rather pleasantly surprised puts a distance which is rather facilitating”—« very good experience »“” |
| Q9. What did you like most/least about this process? (n = 19) Like “I felt free in front of the computer (gestures or body postures “for me” to focus)” “The kindness of the people that took care of me” “Real size of the clinician’s face” Dislike “Quite difficult”—“Lack of proximity to the interlocutor” “Gaze, I felt less presence” |
| Q10. What would be the way to improve the system? (n = 15) “To systematize it through the mutual insurance companies” “Computer placement (screen) hurts the eye” ”Very good internet connectivity” |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Zeghari, R.; Guerchouche, R.; Tran-Duc, M.; Bremond, F.; Langel, K.; Ramakers, I.; Amiel, N.; Lemoine, M.P.; Bultingaire, V.; Manera, V.; et al. Feasibility Study of an Internet-Based Platform for Tele-Neuropsychological Assessment of Elderly in Remote Areas. Diagnostics 2022, 12, 925. https://doi.org/10.3390/diagnostics12040925
Zeghari R, Guerchouche R, Tran-Duc M, Bremond F, Langel K, Ramakers I, Amiel N, Lemoine MP, Bultingaire V, Manera V, et al. Feasibility Study of an Internet-Based Platform for Tele-Neuropsychological Assessment of Elderly in Remote Areas. Diagnostics. 2022; 12(4):925. https://doi.org/10.3390/diagnostics12040925
Chicago/Turabian StyleZeghari, Radia, Rachid Guerchouche, Minh Tran-Duc, François Bremond, Kai Langel, Inez Ramakers, Nathalie Amiel, Maria Pascale Lemoine, Vincent Bultingaire, Valeria Manera, and et al. 2022. "Feasibility Study of an Internet-Based Platform for Tele-Neuropsychological Assessment of Elderly in Remote Areas" Diagnostics 12, no. 4: 925. https://doi.org/10.3390/diagnostics12040925