The Influence of Calcification Factors and Endothelial-Dysfunction Factors on the Development of Unstable Atherosclerotic Plaques

 , , ,
, , , 
Abstract
:1. Introduction
2. Materials and Methods
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Conflicts of Interest
References
- WHO. Fact Sheet. Available online: https://www.who.int/ru/news-room/fact-sheets/detail/the-top-10-causes-of-death (accessed on 24 May 2018).
- Shaw, L.J.; Giambrone, A.E.; Blaha, M.J.; Knapper, J.T.; Berman, D.S.; Bellam, N.; Quyyumi, A.; Budoff, M.J.; Callister, T.Q.; Min, J.K. Long-term prognosis after coronary artery calcification testing in asymptomatic patients. A cohort study. Ann. Intern. Med. 2015, 163, 14–21. [Google Scholar] [CrossRef] [PubMed]
- Criqui, M.H.; Knox, J.B.; Denenberg, J.O.; Forbang, N.I.; McClelland, R.L.; Novotny, T.E.; Sandfort, V.; Waalen, J.; Blaha, M.J.; Allison, M.A. Coronary artery calcium volume and density: Potential interactions and overall predictive value: The multi-ethnic study of atherosclerosis. JACC Cardiovasc. Imaging 2017, 10, 845–854. [Google Scholar] [CrossRef] [PubMed]
- Puchner, S.B.; Mayrhofer, T.; Park, J.; Lu, M.T.; Liu, T.; Maurovich-Horvat, P.; Ghemigian, K.; Bittner, D.; Fleg, J.L.; Udelson, J.E.; et al. Differences in the association of total versus local coronary artery calcium with acute coronary syndrome and culprit lesions in patients with acute chest pain: The coronary calcium paradox. Atherosclerosis 2018, 274, 251–257. [Google Scholar] [CrossRef] [PubMed]
- Hoffmann, U.; Massaro, J.M.; D’Agostino, R.B.; Kathiresan, S.; Fox, C.S.; O’Donnell, C.J. Cardiovascular Event Prediction and Risk Reclassification by Coronary, Aortic, and Valvular Calcification in the Framingham Heart Study. J. Am. Heart Assoc. 2016, 5, e003144. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Oishi, Y.; Wakatsuki, T.; Nishikado, A.; Oki, T.; Ito, S. Circulating adhesion molecules and severity of coronary atherosclerosis. Coron. Artery Dis. 2000, 11, 77–81. [Google Scholar] [CrossRef] [PubMed]
- Jang, Y.; Lincoff, A.M.; Plow, E.F.; Topol, E.J. Cell adhesion molecules in coronary artery disease. J. Am. Coll. Cardiol. 1994, 24, 1591–1601. [Google Scholar] [CrossRef] [Green Version]
- Kunutsor, S.K.; Bakker, S.J.L.; Dullaart, R.P.F. Soluble Vascular Cell Adhesion Molecules May be Protective of Future Cardiovascular Disease Risk: Findings from the PREVEND Prospective Cohort Study. J Atheroscler. Thromb. 2017, 24, 804–818. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hulok, A.; Sciborski, K.; Marczak, J.; Bańkowski, T.; Poręba, R.; Negrusz-Kawecka, M. Soluble Cell Adhesion Molecules—Does Estimating sVCAM-1 and sICAM-1 Concentration Provide Additional Information About Cardiovascular Risk in Patients with Coronary Artery Disease? Adv. Clin. Exp. Med. 2014, 23, 735–741. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lisowska, A.; Siergiejko, E.; Tycińska, A.; Knapp, M.; Kemona, H.; Musiał, W.J.; Dymicka-Piekarska, V. sVCAM-1 concentration and carotid IMT values in patients with acute myocardial infarction—Atherosclerotic markers of the presence, progress and prognosis. Adv. Med. Sci. 2015, 60, 101–106. [Google Scholar] [CrossRef] [PubMed]
- Lin, J.F.; Wu, S.; Juang, J.J.; Chiang, F.T.; Hsu, L.A.; Teng, M.S.; Cheng, S.T.; Huang, H.L.; Ko, Y.L. Osteoprotegerin and osteopontin levels, but not gene polymorphisms, predict mortality in cardiovascular diseases. Biomark. Med. 2019, 13, 751–760. [Google Scholar] [CrossRef] [PubMed]
- Tousoulis, D.; Siasos, G.; Maniatis, K.; Oikonomou, E.; Kioufis, S.; Zaromitidou, M.; Paraskevopoulos, T.; Michalea, S.; Kollia, C.; Miliou, A.; et al. Serum osteoprotegerin and osteopontin levels are associated with arterial stiffness and the presence and severity of coronary artery disease. Int. J. Cardiol. 2013, 167, 1924–1928. [Google Scholar] [CrossRef] [PubMed]
- Callegari, A.; Coons, M.L.; Ricks, J.L.; Rosenfeld, M.E.; Scatena, M. Increased calcification in osteoprotegerin-deficient smooth muscle cells: Dependence on receptor activator of NF-κB ligand and interleukin 6. J. Vasc. Res. 2014, 51, 118–131. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gadeau, A.P.; Chaulet, H.; Daret, D.; Kockx, M.; Daniel-Lamazière, J.M.; Desgranges, C. Time course of osteopontin, osteocalcin, and osteonectin accumulation and calcification after acute vessel wall injury. J. Histochem. Cytochem. 2001, 49, 79–86. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ciceri, P.; Elli, F.; Cappelletti, L.; Tosi, D.; Savi, F.; Bulfamante, G.; Cozzolino, M. Osteonectin (SPARC) Expression in Vascular Calcification: In Vitro and Ex Vivo Studies. Calcif. Tissue Int. 2016, 99, 472–480. [Google Scholar] [CrossRef] [PubMed]
- Hirota, S.; Imakita, M.; Kohri, K.; Ito, A.; Morii, E.; Adachi, S.; Kim, H.M.; Kitamura, Y.; Yutani, C.; Nomura, S. Expression of osteopontin messenger ma by macrophages in atherosclerotic plaques. A possible association with calcification. Am. J. Pathol. 1993, 143, 1003–1008. [Google Scholar] [PubMed]
- Millar, S.A.; John, S.G.; McIntyre, C.W.; Ralevic, V.; Anderson, S.I.; O’Sullivan, S.E. An Investigation into the Role of Osteocalcin in Human Arterial Smooth Muscle Cell Calcification. Front. Endocrinol. (Lausanne) 2020, 11, 369. [Google Scholar] [CrossRef] [PubMed]
- Rashdan, N.A.; Sim, A.M.; Cui, L.; Phadwal, K.; Roberts, F.L.; Carter, R.; Ozdemir, D.D.; Hohenstein, P.; Hung, J.; Kaczynski, J.; et al. Osteocalcin Regulates Arterial Calcification Via Altered Wnt Signaling and Glucose Metabolism. J. Bone Miner. Res. 2020, 35, 357–367. [Google Scholar] [CrossRef] [PubMed]
- Tacey, A.; Qaradakhi, T.; Brennan-Speranza, T.; Hayes, A.; Zulli, A.; Levinger, I. Potential Role for Osteocalcin in the Development of Atherosclerosis and Blood Vessel Disease. Nutrients 2018, 10, 1426. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zhang, H.; Wang, L.J.; Si, D.L.; Wang, C.; Yang, J.; Jiang, P.; Du, C.; Wang, J. Correlation between osteocalcin-positive endothelial progenitor cells and spotty calcification in patients with coronary artery disease. Clin. Exp. Pharmacol. Physiol. 2015, 42, 734–739. [Google Scholar] [CrossRef] [PubMed]
- Foresta, C.; Strapazzon, G.; De Toni, L.; Fabris, F.; Grego, F.; Gerosa, G.; Vettore, S.; Garolla, A. Platelets express and release osteocalcin and co-localize in human calcified atherosclerotic plaques. J. Thromb. Haemost. 2013, 11, 357–365. [Google Scholar] [CrossRef] [PubMed] [Green Version]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Parameter | Value |
|---|---|
| Age, yeas (M ± SD) | 60.6 ± 7.8 |
| Systolic blood pressure (M ± SD) | 137.9 ± 15.5 |
| Diastolic blood pressure (M ± SD) | 84.2 ± 9.5 |
| Pulse, rate (M ± SD) | 68.9 ± 7.11 |
| Body mass index, kg/m2 (M ± SD) | 29.2 ± 4.9 |
| History of myocardial infarction | 69.4% |
| History of diabetes type 2 | 11.9% |
| Multivascular atherosclerotic lesion of coronary arteries (more than two vessels) | 90.1% |
| History of angina pectoris: | |
| Funcional class I | 0% |
| Funcional class II | 10.9% |
| Funcional class III | 82.6% |
| Funcional class IV | 6.5% |
| Indicator | Stable Plaques (n = 89) | Unstable Plaques (n = 51) | p |
|---|---|---|---|
| Osteoprotegerin, pg/mg protein | 110.7 (43.0; 235.9) | 89.9 (34.4; 249.4) | 0.491 |
| Osteopontin, ng/mg protein | 3.3 (1.4; 8.1) | 1.7 (0.7; 7.6) | 0.120 |
| Osteocalcin, ng/mg protein | 16.9 (2.3; 112.9) | 14.0 (3.7; 100.5) | 0.691 |
| Osteonectin, μg/mg protein | 2.4 (1.4; 4.4) | 1.6 (1.1; 2.9) | 0.024 |
| MCP-1, pg/mg protein | 79.0 (35.4; 169.5) | 85.4 (35.5; 174.1) | 0.904 |
| sVCAM-1, ng/mg protein | 122.9 (45.9; 254.4) | 66.4 (18.5; 161.3) | 0.014 |
| E-selectin, ng/mg protein | 5.43 (1.8; 14.9) | 2.02 (1.1; 3.8) | 0.001 |
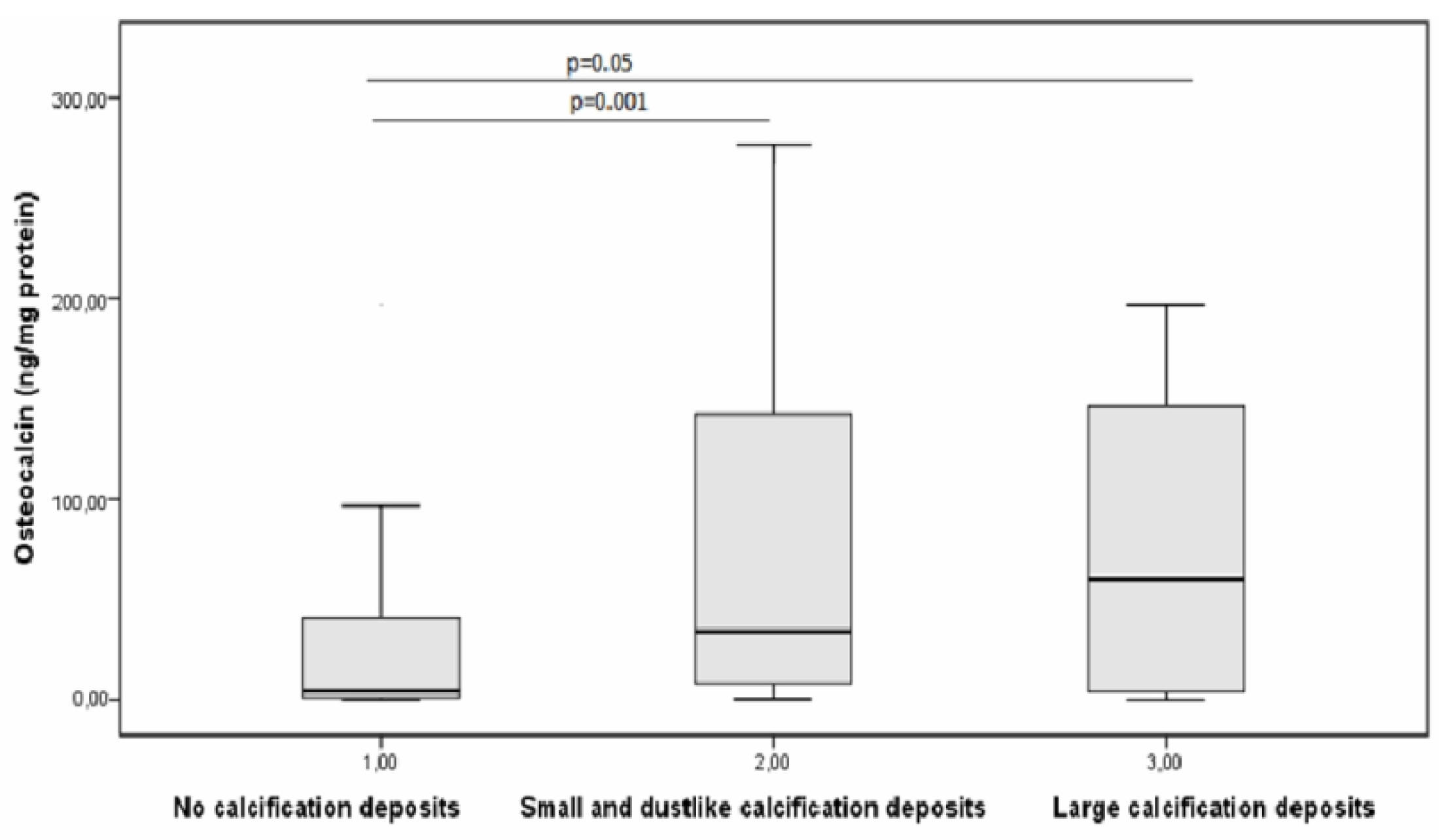
| Indicator | (1) No Calcification Deposits (n = 59) | (2) Small and Dust-like Calcification Deposits (n = 67) | (3) Large Calcification Deposits (n = 14) | Statistical Significance |
|---|---|---|---|---|
| Osteoprotegerin, pg/mg protein | 122.4 (43.8; 194.7) | 115.1 (32.3; 264.0) | 66.7 (40.4; 118.5) | p > 0.05 |
| Osteopontin, ng/mg protein | 4.6 (1.8; 10.2) | 2.3 (0.9; 7.3) | 1.1 (0.3; 3.5) | 1 vs. 2 (p = 0.05) 1 vs. 3 (p = 0.012) |
| Osteonectin, μg/mg protein | 2.3 (1.1; 4.9) | 2.0 (1.3; 3.8) | 1.0 (0.4; 2.1) | 1 vs. 3 (p = 0.016) 2 vs. 3 (p = 0.023) |
| MCP-1, pg/mg protein | 80.2 (35.0; 147.8) | 77.5 (37.2; 174.1) | 148.2 (29.0; 179.3) | p > 0.05 |
| sVCAM-1, ng/mg protein | 115.0 (44.5; 239.2) | 110.9 (34.3; 229.5) | 30.3 (8.1; 52.3) | 1 vs. 3 (p = 0.005) 2 vs. 3 (p = 0.01) |
| E-selectin, ng/mg protein | 4.8 (2.1; 13.0) | 3.1 (1.1; 7.9) | 0.9 (0.2; 2.1) | 1 vs. 2 (p = 0.016) 1 vs. 3 (p = 0.002) 2 vs. 3 (p = 0.048) |
| Parameter | Stable Plaques in Coronary Arteries | An Unstable Plaque Is Present in Coronary Arteries |
|---|---|---|
| Osteoprotegerin (pg/mL) | 60.5 (36.5; 79.9) | 49.0 (43.5; 60.5) |
| Osteopontin (ng/mL) | 28.2 (18.12; 42.1) | 27.5 (17.1; 38.0) |
| Osteocalcin (ng/mL) | 12.0 (8.3; 16.5) | 14.6 (7.8; 17.9) |
| Osteonectin (µg/mL) | 8.9 (8.0; 10.9) | 9.2 (7.5; 10.4) |
| MCP-1 (pg/mL) | 404.6 (283.9; 530.9) | 547.4 (353.9; 625.4) |
| sVCAM-1 (ng/mL) | 838.8 (669.5; 1023.1) | 809.2 (655.6; 935.8) |
| E-selectin (ng/mL) | 47.7 (33.3; 60.2) | 54.5 (38.2; 62.1) |
| Indicator | No Calcified Plaques | Calcified Plaques Are Present |
|---|---|---|
| Osteoprotegerin (pg/mL) | 59.4 (33.9; 78.9) | 52.0 (41.7; 78.4) |
| Osteopontin (ng/mL) | 8.7 (7.2; 10.8) | 9.2 (8.0; 10.422) |
| Osteonectin (µg/mL) | 8.7 (7.2; 10.8) | 9.2 (7.9; 10.4) |
| MCP-1 (pg/mL) | 421.1 (294.7; 563.8) | 467.7 (398.9; 622.8) |
| sVCAM-1 (ng/mL) | 843.5 (695.7; 1003.6) | 838.8 (669.5;1023.1) |
| E-selectin (ng/mL) | 41.8 (33.4; 60.2) | 53.7 (38.9; 62.1) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Polonskaya, Y.V.; Kashtanova, E.V.; Murashov, I.S.; Kurguzov, A.V.; Sadovski, E.V.; Maslatsov, N.A.; Stakhneva, E.M.; Chernyavskii, A.M.; Ragino, Y.I. The Influence of Calcification Factors and Endothelial-Dysfunction Factors on the Development of Unstable Atherosclerotic Plaques. Diagnostics 2020, 10, 1074. https://doi.org/10.3390/diagnostics10121074
Polonskaya YV, Kashtanova EV, Murashov IS, Kurguzov AV, Sadovski EV, Maslatsov NA, Stakhneva EM, Chernyavskii AM, Ragino YI. The Influence of Calcification Factors and Endothelial-Dysfunction Factors on the Development of Unstable Atherosclerotic Plaques. Diagnostics. 2020; 10(12):1074. https://doi.org/10.3390/diagnostics10121074
Chicago/Turabian StylePolonskaya, Yana V., Elena V. Kashtanova, Ivan S. Murashov, Aleksei V. Kurguzov, Evgeny V. Sadovski, Nikolay A. Maslatsov, Ekaterina M. Stakhneva, Alexander M. Chernyavskii, and Yuliya I. Ragino. 2020. "The Influence of Calcification Factors and Endothelial-Dysfunction Factors on the Development of Unstable Atherosclerotic Plaques" Diagnostics 10, no. 12: 1074. https://doi.org/10.3390/diagnostics10121074