Pain and Cortisol in Patients with Fibromyalgia: Systematic Review and Meta-Analysis

 , , , and
, , , and
Abstract
:1. Introduction
2. Materials and Methods
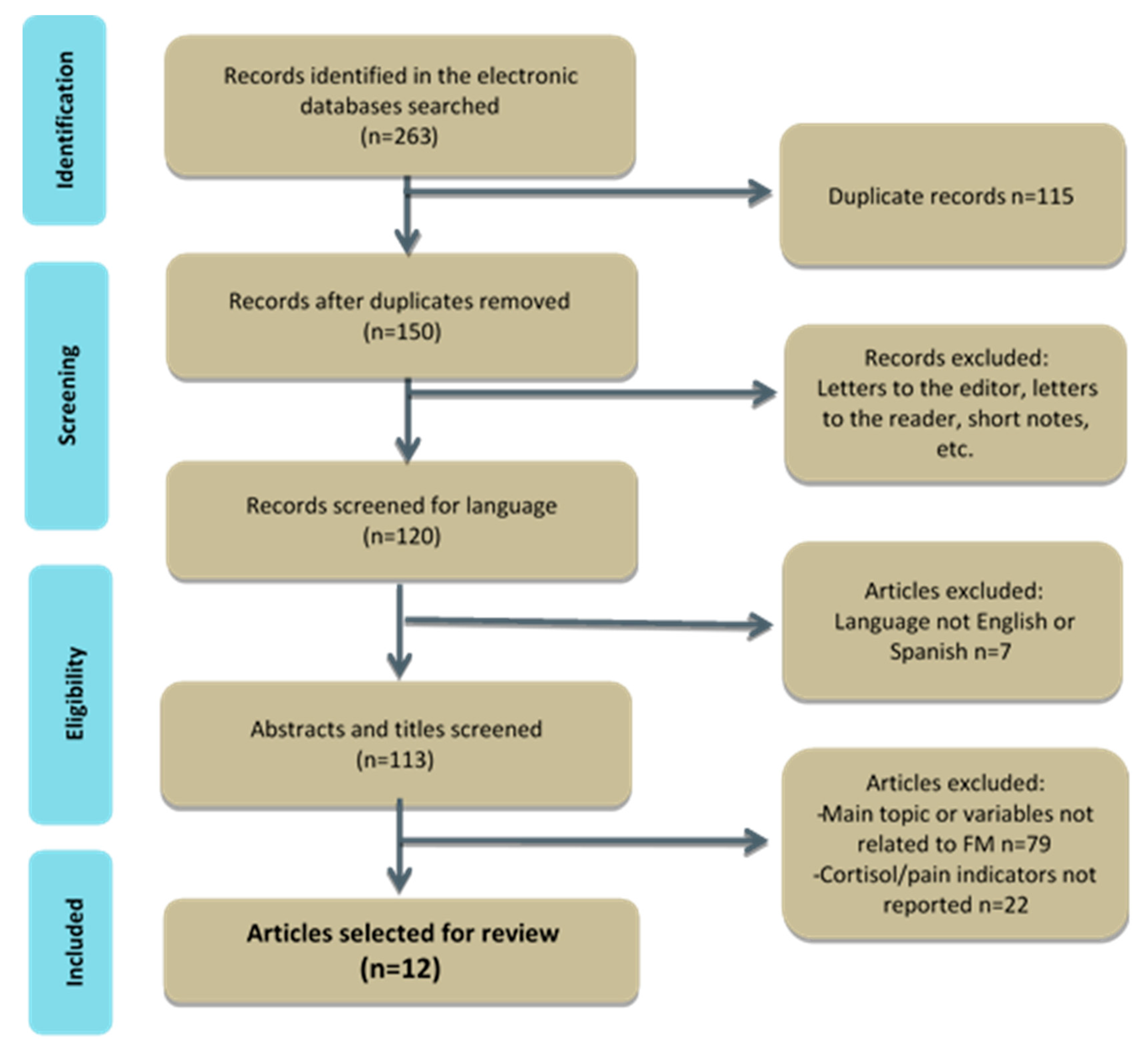
2.1. Data Acquisition, Search Strategy and Eligibility
2.2. Methodological Quality
2.3. Statistical Analysis
3. Results
3.1. Data Synthesis
3.2. Methodological Quality
3.3. Data Extraction and Analysis
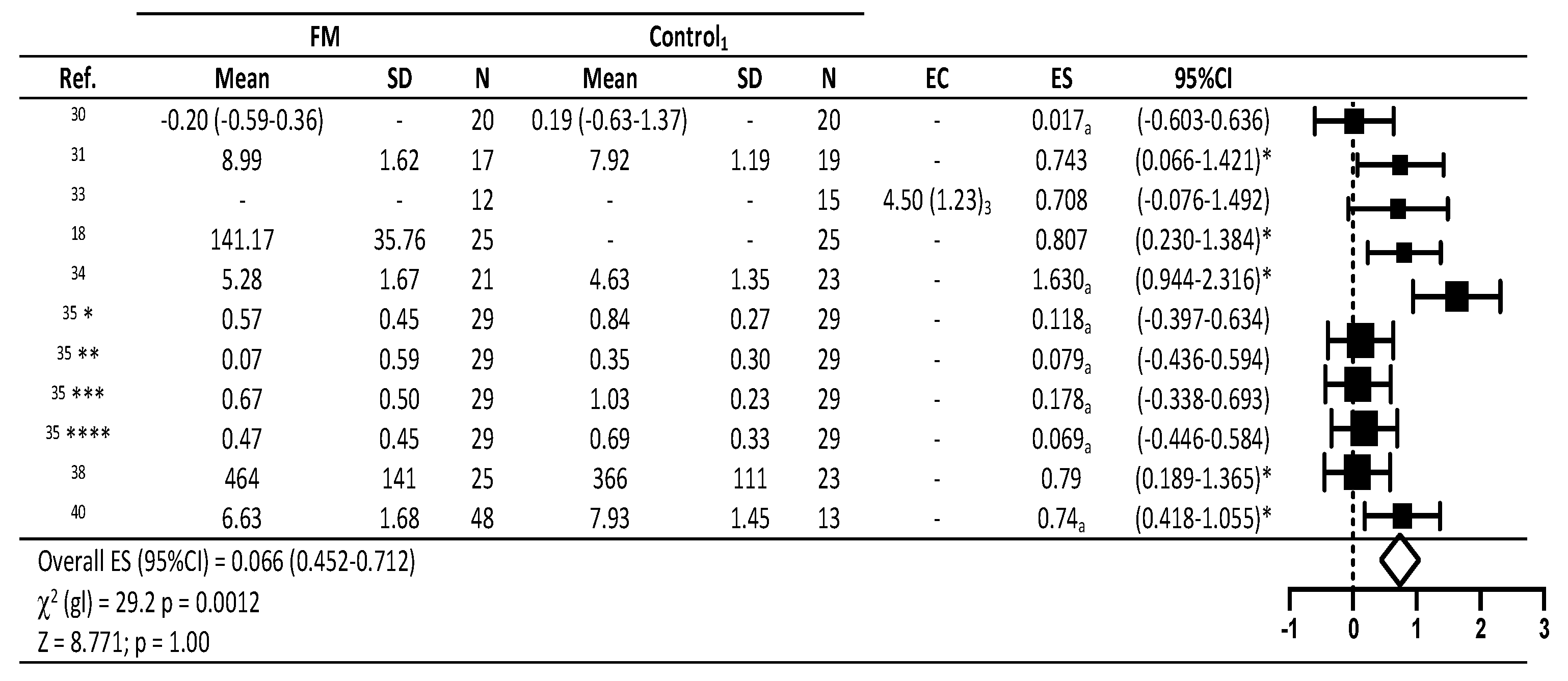
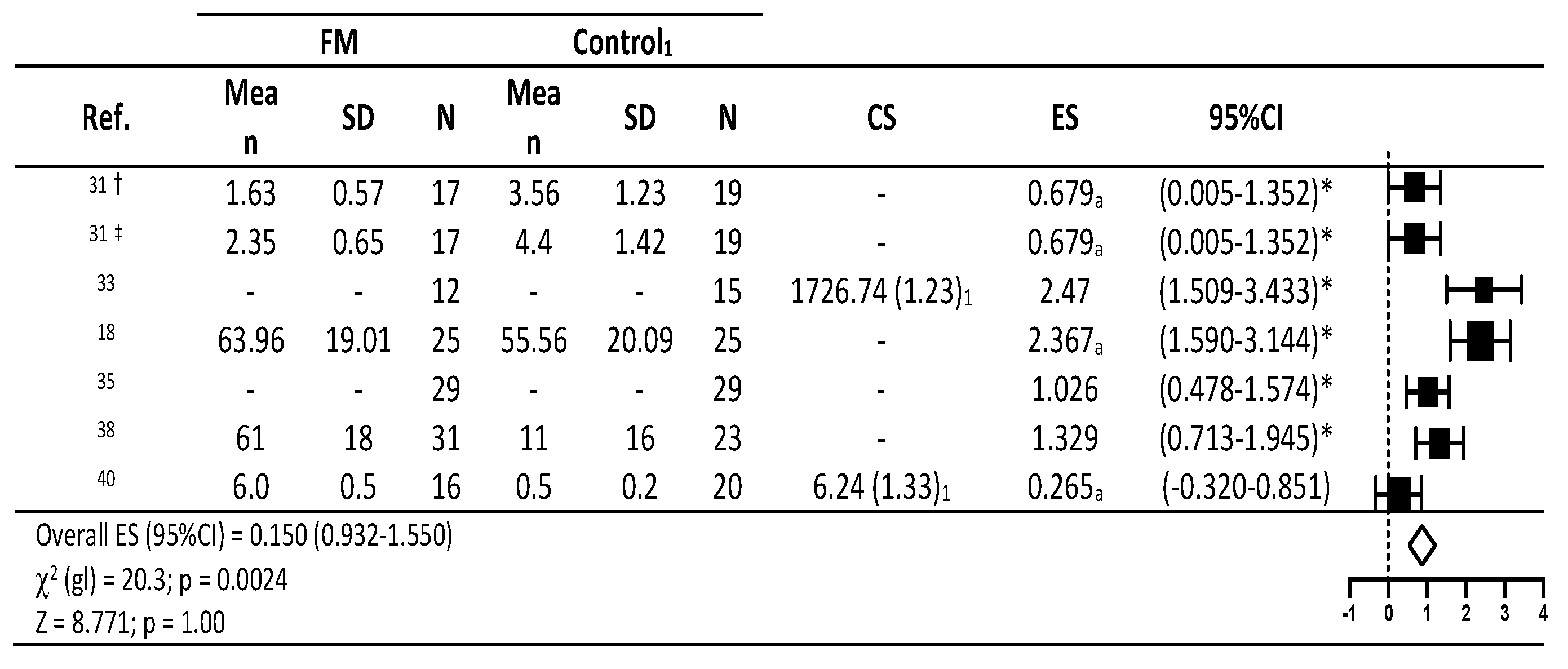
3.4. Combined Effects of Outcome Measures
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Conflicts of Interest
References
- Laroche, F. Fibromialgia. EMC Apar. Locomot. 2014, 47, 1–9. [Google Scholar] [CrossRef]
- Sifuentes-Giraldo, W.; Morell-Hita, J. Fibromialgia. Med. Programa Form. Médica Contin. Acreditado 2017, 12, 1586–1595. [Google Scholar] [CrossRef]
- Aman, M.M.; Yong, R.J.; Kaye, A.D.; Urman, R.D. Evidence-Based Non-Pharmacological Therapies for Fibromyalgia. Curr. Pain Headache Rep. 2018, 22, 33. [Google Scholar] [CrossRef] [PubMed]
- Arnold, L.M.; Bennett, R.M.; Crofford, L.J.; Dean, L.E.; Clauw, D.J.; Goldenberg, D.L.; Fitzcharles, M.-A.; Paiva, E.S.; Staud, R.; Sarzi-Puttini, P.; et al. AAPT Diagnostic Criteria for Fibromyalgia. J. Pain 2019, 20, 611–628. [Google Scholar] [CrossRef] [Green Version]
- Fillingim, R.B.; Bruehl, S.; Dworkin, R.H.; Dworkin, S.F.; Loeser, J.D.; Turk, D.C.; Widerstrom-Noga, E.; Arnold, L.; Bennett, R.; Edwards, R.R.; et al. The ACTTION-American Pain Society Pain Taxonomy (AAPT): An Evidence-Based and Multidimensional Approach to Classifying Chronic Pain Conditions. J. Pain 2014, 15, 241–249. [Google Scholar] [CrossRef] [Green Version]
- Kaltsas, G.; Tsiveriotis, K. Fibromyalgia. In Endotext [Internet]; MDText.com, Inc.: South Dartmouth, MA, USA, 2020. Available online: https://www.ncbi.nlm.nih.gov/sites/books/NBK279092/ (accessed on 28 October 2019).
- Goodin, B.R.; Smith, M.T.; Quinn, N.B.; King, C.D.; McGuire, L. Poor sleep quality and exaggerated salivary cortisol reactivity to the cold pressor task predict greater acute pain severity in a non-clinical sample. Biol. Psychol. 2012, 91, 36–41. [Google Scholar] [CrossRef] [Green Version]
- Raff, H. Utility of Salivary Cortisol Measurements in Cushing’s Syndrome and Adrenal Insufficiency. J. Clin. Endocrinol. Metab. 2009, 94, 3647–3655. [Google Scholar] [CrossRef] [Green Version]
- Chan, S.; Debono, M. Review: Replication of cortisol circadian rhythm: New advances in hydrocortisone replacement therapy. Ther. Adv. Endocrinol. Metab. 2010, 1, 129–138. [Google Scholar] [CrossRef]
- McBeth, J.; Chiu, Y.H.; Silman, A.J.; Ray, D.W.; Morriss, R.; Dickens, C.; Gupta, A.; Macfarlane, G.J. Hypothalamic-pituitary-adrenal stress axis function and the relationship with chronic widespread pain and its antecedents. Arthritis Res. Ther. 2005, 7, R992–R1000. [Google Scholar] [CrossRef] [Green Version]
- Neeck, G.; Reidel, W. Hormonal perturations in fibromyalgia syndrome. Ann. N. Y. Acad. Sci. 1999, 879, 325–338. [Google Scholar] [CrossRef]
- Úbeda-D’Ocasar, E. Mejora en la Calidad de Vida y Disminución del Dolor en Pacientes con Fibromialgia Tratadas Mediante Terapia Manual EUD. Cuest. Fisioter. 2014, 43, 183–195. Available online: http://www.cuestionesdefisioterapia.com/index.php/es/main/articulos/article/43/3/3 (accessed on 28 October 2019).
- Fischer, S.; Doerr, J.M.; Strahler, J.; Mewes, R.; Thieme, K.; Nater, U.M. Stress exacerbates pain in the everyday lives of women with fibromyalgia syndrome—The role of cortisol and alpha-amylase. Psychoneuroendocrinology 2016, 63, 68–77. [Google Scholar] [CrossRef]
- Carnes, D.; Parsons, S.; Ashby, D.; Breen, A.; Foster, N.E.; Pincus, T.; Vogel, S.; Underwood, M. Chronic musculoskeletal pain rarely presents in a single body site: Results from a UK population study. Rheumatology 2007, 46, 1168–1170. [Google Scholar] [CrossRef] [Green Version]
- Al’Absi, M.; Petersen, K.L.; Wittmers, L.E. Adrenocortical and hemodynamic predictors of pain perception in men and women. Pain 2002, 96, 197–204. [Google Scholar] [CrossRef]
- Geiss, A.; Varadi, E.; Steinbach, K.; Bauer, H.W.; Anton, F. Psychoneuroimmunological correlates of persisting sciatic pain in patients who underwent discectomy. Neurosci. Lett. 1997, 237, 65–68. [Google Scholar] [CrossRef]
- Penney, L.S.; Ritenbaugh, C.; Elder, C.; Schneider, J.; Deyo, R.A.; DeBar, L.L. Primary care physicians, acupuncture and chiropractic clinicians, and chronic pain patients: A qualitative analysis of communication and care coordination patterns. BMC Complement. Altern. Med. 2015, 16, 30. [Google Scholar] [CrossRef] [Green Version]
- Genc, A.; Tur, B.S.; Aytur, Y.K.; Öztuna, D.; Erdoğan, M.F. Does aerobic exercise affect the hypothalamic-pituitary-adrenal hormonal response in patients with fibromyalgia syndrome? J. Phys. Ther. Sci. 2015, 27, 2225–2231. [Google Scholar] [CrossRef] [Green Version]
- Li, X.; Hu, L. The Role of Stress Regulation on Neural Plasticity in Pain Chronification. Neural Plast. 2016, 2016, 1–9. [Google Scholar] [CrossRef]
- Galvez-Sánchez, C.M.; Duschek, S.; Del Paso, G.A.R. Psychological impact of fibromyalgia: Current perspectives. Psychol. Res. Behav. Manag. 2019, 12, 117–127. [Google Scholar] [CrossRef] [Green Version]
- Liberati, A.; Altman, D.G.; Tetzlaff, J.; Mulrow, C.; Gøtzsche, P.C.; Ioannidis, J.P.A.; Clarke, M.; Devereaux, P.J.; Kleijnen, J.; Moher, D. The PRISMA Statement for Reporting Systematic Reviews and Meta-Analyses of Studies That Evaluate Health Care Interventions: Explanation and Elaboration. PLoS Med. 2009, 6, e1000100. [Google Scholar] [CrossRef]
- Urrútia, G.; Bonfill, X. Declaración PRISMA: Una propuesta para mejorar la publicación de revisiones sistemáticas y metaanálisis. Med. Clín. 2010, 135, 507–511. [Google Scholar] [CrossRef] [PubMed]
- Furlan, A.D.; Malmivaara, A.; Chou, R.; Maher, C.G.; Deyo, R.A.; Schoene, M.; Bronfort, G.; Van Tulder, M.W. 2015 Updated Method Guideline for Systematic Reviews in the Cochrane Back and Neck Group. Spine 2015, 40, 1660–1673. [Google Scholar] [CrossRef] [PubMed]
- De Morton, N.A. The PEDro scale is a valid measure of the methodological quality of clinical trials: A demographic study. Aust. J. Physiother. 2009, 55, 129–133. [Google Scholar] [CrossRef] [Green Version]
- Maher, C.G.; Sherrington, C.; Herbert, R.D.; Moseley, A.M.; Elkins, M. Reliability of the PEDro Scale for Rating Quality of Randomized Controlled Trials. Phys. Ther. 2003, 83, 713–721. [Google Scholar] [CrossRef] [Green Version]
- Lipsey, M.W.; Wilson, D.B. Practical Meta-Analysis; Sage Publications, Inc.: Thousand Oaks, CA, USA, 2001. [Google Scholar]
- Hedges, L.V. Estimation of effect size from a series of independent experiments. Psychol. Bull. 1982, 92, 490–499. [Google Scholar] [CrossRef]
- Cohen, J. Statistical Power Analysis for the Behavioral Sciences; NJ Erihaum: Hillsdale, MI, USA, 1988. [Google Scholar]
- Moseley, A.M.; Herbert, R.D.; Sherrington, C.; Maher, C.G. Evidence for physiotherapy practice: A survey of the Physiotherapy Evidence Database (PEDro). Aust. J. Physiother. 2002, 48, 43–49. [Google Scholar] [CrossRef] [Green Version]
- Alp, A.; Oral, A.; Ocakoğlu, G.; Dirican, M.; Yurtkuran, M. Evidence of Defective Growth Hormone Response and Adaptive Hormonal Changes in Fibromyalgia. Phys. Med. Rehabil. Kurortmed. 2014, 24, 14–20. [Google Scholar] [CrossRef]
- Freitas, R.P.D.A.; Lemos, T.; Spyrides, M.H.C.; De Sousa, M.B.C. Influence of cortisol and DHEA-S on pain and other symptoms in post menopausal women with fibromyalgia. J. Back Musculoskelet. Rehabil. 2012, 25, 245–252. [Google Scholar] [CrossRef] [Green Version]
- Garrido, M.; Castaño, M.; Biehl-Printes, C.; Gomez, M.; Branco, J.; Tomas-Carus, P.; Rodriguez, A. Effects of a respiratory functional training program on pain and sleep quality in patients with fibromyalgia: A pilot study. Complement. Ther. Clin. Pr. 2017, 28, 116–121. [Google Scholar] [CrossRef]
- Geiss, A.; Rohleder, N.; Anton, F. Evidence for an association between an enhanced reactivity of interleukin-6 levels and reduced glucocorticoid sensitivity in patients with fibromyalgia. Psychoneuroendocrinology 2012, 37, 671–684. [Google Scholar] [CrossRef]
- Pernambuco, A.P.; Carvalho, L.D.S.C.; Schetino, L.P.L.; Polese, J.C.; Viana, R.D.S.; Reis, D.D. Ávila Effects of a health education program on cytokines and cortisol levels in fibromyalgia patients: A randomized controlled trial. Adv. Rheumatol. 2018, 58, 21. [Google Scholar] [CrossRef]
- Riva, R.; Mork, P.J.; Westgaard, R.H.; Rø, M.; Lundberg, U. Fibromyalgia Syndrome is Associated with Hypocortisolism. Int. J. Behav. Med. 2010, 17, 223–233. [Google Scholar] [CrossRef]
- De Oliveira, F.R.; Gonçalves, L.C.V.; Borghi, F.; Da Silva, L.G.R.V.; Gomes, A.E.; Trevisan, G.; De Souza, A.L.; Grassi-Kassisse, D.M.; Crege, D.R.X.D.O. Massage therapy in cortisol circadian rhythm, pain intensity, perceived stress index and quality of life of fibromyalgia syndrome patients. Complement. Ther. Clin. Pr. 2018, 30, 85–90. [Google Scholar] [CrossRef] [PubMed]
- Schertzinger, M.; Wesson-Sides, K.; Parkitny, L.; Younger, J. Daily Fluctuations of Progesterone and Testosterone Are Associated with Fibromyalgia Pain Severity. J. Pain 2018, 19, 410–417. [Google Scholar] [CrossRef] [Green Version]
- Stehlik, R.; Ulfberg, J.; Zou, D.; Hedner, J.; Grote, L. Morning cortisol and fasting glucose are elevated in women with chronic widespread pain independent of comorbid restless legs syndrome. Scand. J. Pain 2018, 18, 187–194. [Google Scholar] [CrossRef] [PubMed]
- Tanwar, S.; Mattoo, B.; Kumar, U.; Gupta, N.; Bhatia, R. Is fibromyalgia a syndrome of hormonal imbalance? Asian J. Pharm. Clin. Res. 2018, 11, 416–420. [Google Scholar] [CrossRef]
- Torgrimson-Ojerio, B.; Ross, R.L.; Dieckmann, N.F.; Avery, S.; Bennett, R.; Jones, K.D.; Guarino, A.J.; Wood, L.J.; Dieckmann, N.F. Preliminary evidence of a blunted anti-inflammatory response to exhaustive exercise in fibromyalgia. J. Neuroimmunol. 2014, 277, 160–167. [Google Scholar] [CrossRef] [Green Version]
- D’Agnelli, S.; Arendt-Nielsen, L.; Gerra, M.C.; Zatorri, K.; Boggiani, L.; Baciarello, M.; Bignami, E. Fibromyalgia: Genetics and epigenetics insights may provide the basis for the development of diagnostic biomarkers. Mol. Pain 2018, 15. [Google Scholar] [CrossRef] [PubMed]
- Sosa-Reina, M.D.; Nunez-Nagy, S.; Gallego-Izquierdo, T.; Pecos-Martín, D.; Monserrat, J.; Álvarez-Mon, M. Effectiveness of Therapeutic Exercise in Fibromyalgia Syndrome: A Systematic Review and Meta-Analysis of Randomized Clinical Trials. BioMed Res. Int. 2017, 2017, 2356346. [Google Scholar] [CrossRef] [PubMed]
- Cabo-Meseguer, A.; Cerdá-Olmedo, G.; Trillo-Mata, J.L. Fibromyalgia: Prevalence, epidemiologic profiles and economic costs. Med. Clín. 2017, 149, 441–448. [Google Scholar] [CrossRef]
- Arout, C.A.; Sofuoglu, M.; Bastian, L.A.; Rosenheck, R. Gender Differences in the Prevalence of Fibromyalgia and in Concomitant Medical and Psychiatric Disorders: A National Veterans Health Administration Study. J. Women’s Heal. 2018, 27, 1035–1044. [Google Scholar] [CrossRef]
- Heredia-Jimenez, J.; Orantes-Gonzalez, E. Gender differences in patients with fibromyalgia: A gait analysis. Clin. Rheumatol. 2018, 38, 513–522. [Google Scholar] [CrossRef]
- Úbeda-D’Ocasar, E.; Gallego-Sendarrubias, G.M.; Guodemar-Pérez, J.; Hervás-Pérez, J.P. Differences Between Men and Women with Fibromyalgia. Phys. Med. Rehabil. Kurortmed. 2020. [Google Scholar] [CrossRef]
- Álvarez-Gallardo, I.C.; Bidonde, J.; Busch, A.; Westby, M.; Kenny, G.P.; Delgado-Fernández, M.; Carbonell-Baeza, A.; Rahman, P.; De Angelis, G.; Brosseau, L. Therapeutic validity of exercise interventions in the management of fibromyalgia. J. Sports Med. Phys. Fit. 2019, 59, s0022–s4707. [Google Scholar] [CrossRef]
- Basavakumar, D.; Flegg, M.; Eccles, J.A.; Ghezzi, P. Accuracy, completeness and accessibility of online information on fibromyalgia. Rheumatol. Int. 2019, 39, 735–742. [Google Scholar] [CrossRef] [Green Version]
- Gur, A.; Cevik, R.; Sarac, A.J.; Colpan, L.; Em, S. Hypothalamic-pituitary-gonadal axis and cortisol in young women with primary fibromyalgia: The potential roles of depression, fatigue, and sleep disturbance in the occurrence of hypocortisolism. Ann. Rheum. Dis. 2004, 63, 1504–1506. [Google Scholar] [CrossRef] [Green Version]
- Bonnabesse, A.L.F.; Cabon, M.; L’Heveder, G.; Kermarrec, A.; Quinio, B.; Woda, A.; Marchand, S.; Dubois, A.; Giroux-Metges, M.-A.; Rannou, F.; et al. Impact of a specific training programme on the neuromodulation of pain in female patient with fibromyalgia (DouFiSport): A 24-month, controlled, randomised, double-blind protocol. BMJ Open 2019, 9, e023742. [Google Scholar] [CrossRef] [PubMed]
- Roerink, M.E.; Roerink, S.H.P.P.; Skoluda, N.; Van Der Schaaf, M.E.; Hermus, A.R.; Van Der Meer, J.W.; Knoop, H.; Nater, U.M. Hair and salivary cortisol in a cohort of women with chronic fatigue syndrome. Horm. Behav. 2018, 103, 1–6. [Google Scholar] [CrossRef]
- Papandreou, M.; Philippou, A.; Taso, O.; Koutsilieris, M.; Kaperda, A. The effect of treatment regimens on salivary cortisol levels in patients with chronic musculoskeletal disorders. J. Bodyw. Mov. Ther. 2019, 24, 100–108. [Google Scholar] [CrossRef]
- Tak, L.M.; Cleare, A.J.; Ormel, J.; Manoharan, A.; Kok, I.C.; Wessely, S.; Rosmalen, J.G. Meta-analysis and meta-regression of hypothalamic-pituitary-adrenal axis activity in functional somatic disorders. Biol. Psychol. 2011, 87, 183–194. [Google Scholar] [CrossRef] [PubMed]
- Herane-Vives, A.; Papadopoulos, A.; De Angel, V.; Chua, K.-C.; Chalder, T.; Young, A.H.; Cleare, A.J. Cortisol levels in chronic fatigue syndrome and atypical depression measured using hair and saliva specimens. J. Affect. Disord. 2020, 267, 307–314. [Google Scholar] [CrossRef]
- Riva, R.; Mork, P.J.; Westgaard, R.H.; Lundberg, U. Comparison of the cortisol awakening response in women with shoulder and neck pain and women with fibromyalgia. Psychoneuroendocrinology 2012, 37, 299–306. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
| Reference | Study Type | PEDro | |||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| S | 2 | 3 | 4 | 5 | 6 | 7 | 8 | 9 | 10 | 11 | TOTAL | ||
| Genc et al., 2015 [18] | Randomized controlled | + | + | + | + | - | - | - | + | + | + | + | 7 |
| Alp et al., 2014 [30] | Non-randomized controlled | + | - | - | + | + | - | - | + | + | + | + | 6 |
| de Abreu et al., 2012 [31] | Observational cross-sectional | + | - | - | + | - | - | - | + | + | + | + | 5 |
| Garrido et al., 2017 [32] | Observation longitudinal | + | - | - | + | - | - | - | + | + | + | + | 5 |
| Geis et al., 2012 [33] | Non-randomized controlled | + | - | - | + | - | - | - | + | + | + | + | 5 |
| Pernambuco et al., 2018 [34] | Clinical randomized controlled | + | + | + | + | - | - | + | + | + | + | + | 8 |
| Riva et al., 2010 [35] | Non-randomized controlled | + | - | - | + | - | - | - | + | + | + | + | 5 |
| de Oliveira et al., 2018 [36] | Non-randomized controlled | + | - | - | + | - | - | - | + | + | + | + | 5 |
| Schertzinger et al., 2018 [37] | Longitudinal | + | - | - | - | - | - | - | - | + | + | + | 3 |
| Stehlik et al., 2018 [38] | Case-control | + | - | - | + | - | - | - | + | + | + | + | 5 |
| Tanwar et al., 2018 [39] | Non-randomized controlled | + | - | - | - | - | - | - | + | - | + | + | 3 |
| Torgrimson-Ojerio et al., 2014 [40] | Pilot | + | - | - | - | - | + | - | + | + | + | + | 5 |
| Ref. | Demographics | Objectives | Intervention | Outcome Measures | Results (p Values) |
|---|---|---|---|---|---|
| [35] | FM: n = 29 52.1 ± 8.9 years BMI 27.1 ± 5.9 Control: n = 29 52.7 ± 8.4 years BMI 25.0 ± 3.5 | To determine salivary cortisol and pain levels in different conditions such as stress, upon awakening, 30 min, 60 min after awakening, etc. | Collection of saliva eight times at the time points: arrival at the hospital (4:45 pm), late afternoon, late evening, CAR and after leaving the hospital the next day (5:05 pm) | -Salivary cortisol -Pain (VAS) | Patients in FM showed declining cortisol levels over the day, most pronounced in the morning (CAR). Cortisol levels lower in FM versus Control. Differences significant between groups in 1st, 2nd, 5th and 8th measurement (p = 0.010, p = 0.035, p = 0.001 and p = 0.050 respectively) Difference between groups in pain perception |
| [31] | FM: n = 17 53 ± 7.98 (42–69 years) Control: n = 19 53.32 ± 6.46 years | To examine changes produced in cortisol and their correlation with pain, depression and quality of life in postmenopausal women with fibromyalgia | Blood cortisol measured after 8 h of sleep along with pain threshold and pain tolerance | -Cortisol levels measured over three alternate days -Algometry post blood collection on 18 Tender Points (TPs) (kg/cm2) until participant reports “starting to feel pain” and “can’t take it anymore” | Pain threshold p > 0.0001 between groups Pain tolerance p > 0.0001 between groups α = 5% Significant difference between groups No link between cortisol levels and pain threshold or tolerance |
| [33] | FM: n = 12 50 ± 2.07 years BMI 26.30 ± 0.363 Control: n = 15 41 ± 2.98 years BMI 26.47 ± 1.01 | To determine cortisol and IL-6 responses after measuring PPT at TPs | 4-day study: measurements at baseline and after low dose overnight dexamethasone (0.5 mg) | -Blood cortisol -PPT -TP count | Cortisol levels significantly increased post PPT measurement p < 0.04 PPT measurement led to higher pain levels when measures were analyzed post hoc |
| [30] | FM: n = 19 51 (25–64 years) BMI 27.1 Control: n = 20 48 (36–54 years) BMI 26.5 | To assess the effects of balneotherapy on the hypothalamic-pituitary axis | 3-week balneotherapy program consisting 20-min sessions 5 days/week | -Blood cortisol (g/dL) Pre/Post intervention -TP count | Cortisol levels fell (p = 0.002) after the Week 3 balneotherapy session compared to baseline levels on Day 1 in controls. Cortisol levels rose by 19% in the Week 3 session compared to Day 1 in the FM group (p = 0.005), and fell by 20% in the control group. TP count fell by 7% (p = 0.02) in FM |
| [40] | FM: n = 20 52.0 ± 1.4 years Control: n = 16 4852.2 ± 1.5 years | To determine cortisol levels associated with pain following an exhaustive exercise test | Fasting treadmill exercise to V02 peak of some 20 min duration | -Blood cortisol -PTT | PPT reduced in FM (p = 0.001) No significant differences in cortisol pre and post exercise (p = 0.10) |
| [18] | FM1: n = 25 36.9 years FM2: n = 25 35.1 years | To assess pain and blood cortisol levels following a home stretching and aerobic exercise program | 6 weeks of home exercise or 6 weeks home + aerobic exercise | -Blood cortisol -PTT -TP count | Pain reductions observed in FMI (p < 0.025) and FM 2 (p < 0.001) TP count reduced Significant differences in cortisol levels from baseline to first and second measurement (p = 0.014) Post-hoc contrast statistic increased from 1st to 2nd measurement |
| [32] | FM: n = 14 51.07 ± 12.38 years BMI 23.65 ± 4.00 TPs 17.10 ± 0.05 | To examine the effects of functional respiratory training on pain and their correlation with cortisol levels | Diaphragm breathing exercise intervention. Measurements made over 12 weeks: first 4 weeks control followed by 8 weeks of exercise. | -Sleep quality -Algometry pain tolerance threshold (PTT) -Urine cortisol | Significant increases produced in PTT between week 4 and 12 (p < 0.05) in occiput, low cervical and 2nd rib No changes in cortisol levels during intervention |
| [34] | FM: n = 21 51.43 ± 11.26 years BMI 26.51 ± 5.18 Control: n = 23 48.26 ± 11.03 years BMI 26.82 ± 4.22 | To assess salivary cortisol, pain (FIQ) and TPs | Health Education program | -Salivary cortisol -Pain (FIQ) -TP count | Cortisol levels rose in FM (p = 0.02), but not in Control. Pain scores improved in FM (p < 0.02) but remained the same in Control |
| [36] | FM: n = 24 45.9 ± 2.89 years BMI 26.04 ± 2.52 | To determine salivary cortisol levels and pain after a 3-month Swedish massage program | Massage program = 24 × 40 min sessions (2 afternoon sessions/week) | -Salivary cortisol -Pain (FIQ) | No significant differences before and after the 3- month intervention. Pre- post intervention differences significant for first session and first month (p < 0.001), but significance lost after 2nd and 3rd month |
| [38] | FM: n = 31 57 ± 8 years BMI 28.4 ± 5.7 Control: n = 23 57 ± 10 years BMI 27.4 ± 5.4 | To correlate chronic pain with morning blood cortisol levels and leg pain | Comparative study | -Blood cortisol -Pain (VAS) | Differences significant between groups in cortisol levels (p = 0.01) and pain perception (p < 0.001) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Úbeda-D’Ocasar, E.; Jiménez Díaz-Benito, V.; Gallego-Sendarrubias, G.M.; Valera-Calero, J.A.; Vicario-Merino, Á.; Hervás-Pérez, J.P. Pain and Cortisol in Patients with Fibromyalgia: Systematic Review and Meta-Analysis. Diagnostics 2020, 10, 922. https://doi.org/10.3390/diagnostics10110922
Úbeda-D’Ocasar E, Jiménez Díaz-Benito V, Gallego-Sendarrubias GM, Valera-Calero JA, Vicario-Merino Á, Hervás-Pérez JP. Pain and Cortisol in Patients with Fibromyalgia: Systematic Review and Meta-Analysis. Diagnostics. 2020; 10(11):922. https://doi.org/10.3390/diagnostics10110922
Chicago/Turabian StyleÚbeda-D’Ocasar, Edurne, Victor Jiménez Díaz-Benito, Gracia María Gallego-Sendarrubias, Juan Antonio Valera-Calero, Ángel Vicario-Merino, and Juan Pablo Hervás-Pérez. 2020. "Pain and Cortisol in Patients with Fibromyalgia: Systematic Review and Meta-Analysis" Diagnostics 10, no. 11: 922. https://doi.org/10.3390/diagnostics10110922