Tumor Doubling Time Using CT Volumetric Segmentation in Metastatic Adrenocortical Carcinoma

 ,
,
Abstract
:1. Introduction
2. Materials and Methods
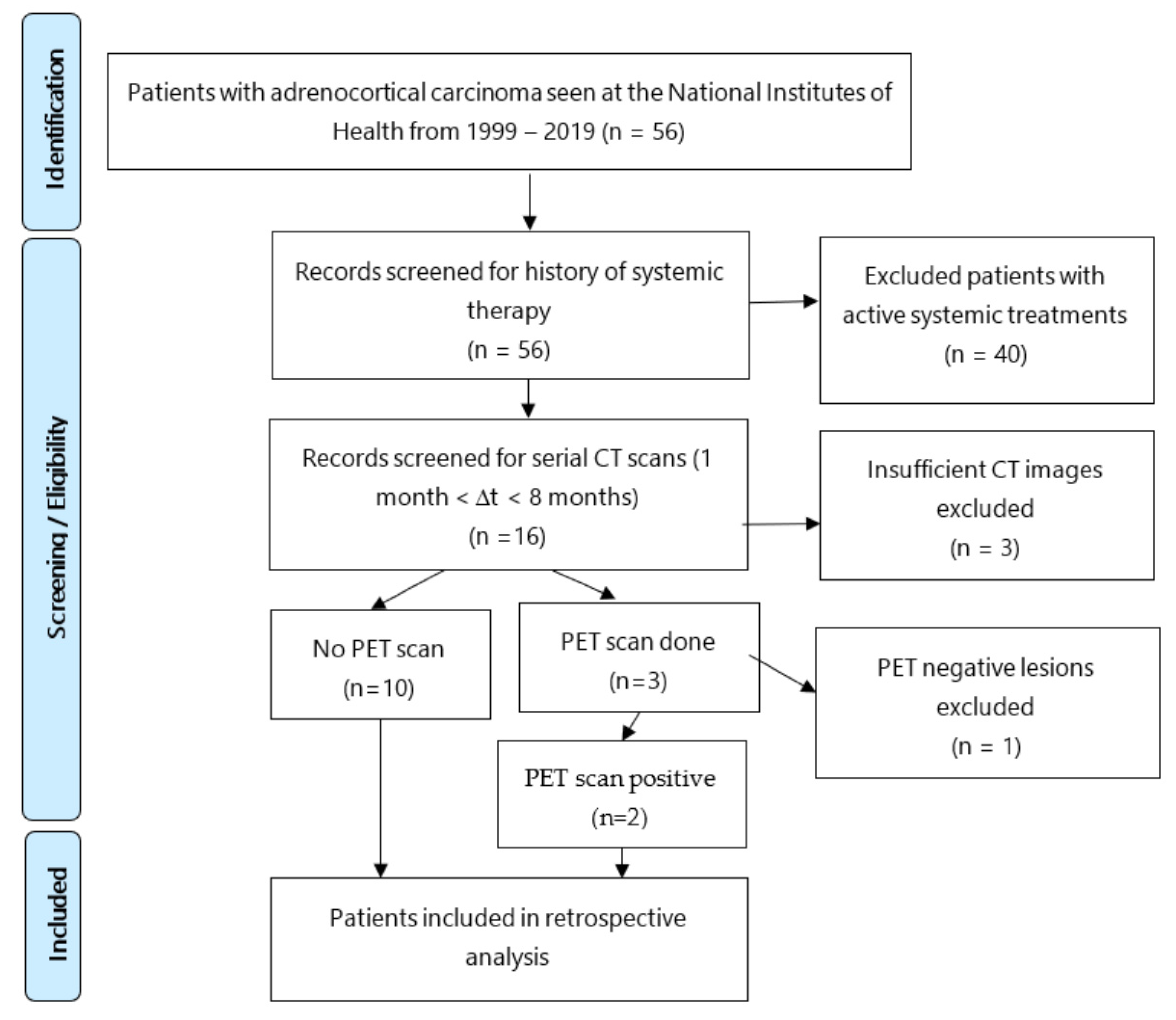
2.1. Patient Selection
2.2. Imaging Analysis
2.3. Statistical Analysis
3. Results
4. Discussion
Limitations
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Brennan, M.F. Adrenocortical carcinoma. CA Cancer J. Clin. 1987, 37, 348–365. [Google Scholar] [CrossRef]
- Else, T.; Kim, A.C.; Sabolch, A.; Raymond, V.M.; Kandathil, A.; Caoili, E.M.; Jolly, S.; Miller, B.S.; Giordano, T.J.; Hammer, G.D. Adrenocortical carcinoma. Endocr. Rev. 2014, 35, 282–326. [Google Scholar] [CrossRef] [Green Version]
- McDuffie, L.A.; Aufforth, R.D. Adrenocortical carcinoma: Modern management and evolving treatment strategies. Int. J. Endocr. Oncol. 2016, 3, 161–174. [Google Scholar] [CrossRef] [Green Version]
- Allolio, B.; Hahner, S.; Weismann, D.; Fassnacht, M. Management of adrenocortical carcinoma. Clin. Endocrinol. 2004, 60, 273–287. [Google Scholar] [CrossRef] [PubMed]
- Fassnacht, M.; Terzolo, M.; Allolio, B.; Baudin, E.; Haak, H.; Berruti, A.; Welin, S.; Schade-Brittinger, C.; Lacroix, A.; Jarząb, M.; et al. Combination Chemotherapy in Advanced Adrenocortical Carcinoma. N. Engl. J. Med. 2012, 366, 2189–2197. [Google Scholar] [CrossRef]
- Livhits, M.; Li, N.; Yeh, M.W.; Harari, A. Surgery is associated with improved survival for adrenocortical cancer, even in metastatic disease. Surgery 2014, 156, 1531–1540, discussion 1540–1. [Google Scholar] [CrossRef] [Green Version]
- Kemp, C.D.; Ripley, R.T.; Mathur, A.; Steinberg, S.M.; Nguyen, D.M.; Fojo, T.; Schrump, D.S. Pulmonary Resection for Metastatic Adrenocortical Carcinoma: The National Cancer Institute Experience. Ann. Thorac. Surg. 2011, 92, 1195–1200. [Google Scholar] [CrossRef]
- Gaujoux, S.; Al-Ahmadie, H.; Allen, P.J.; Gonen, M.; Shia, J.; D’Angelica, M.; Dematteo, R.; Fong, Y.; Blumgart, L.; Jarnagin, W.R. Resection of adrenocortical carcinoma liver metastasis: Is it justified? Ann. Surg. Oncol. 2012, 19, 2643–2651. [Google Scholar] [CrossRef] [PubMed]
- Baur, J.; German Adrenocortical Carcinoma Study Group; Büntemeyer, T.-O.; Megerle, F.; Deutschbein, T.; Spitzweg, C.; Quinkler, M.; Nawroth, P.; Kroiss, M.; Germer, C.-T.; et al. Outcome after resection of Adrenocortical Carcinoma liver metastases: A retrospective study. BMC Cancer 2017, 17, 522. [Google Scholar] [CrossRef] [Green Version]
- Winkel, J.O.D.; Pfannschmidt, J.; Muley, T.; Grünewald, C.; Dienemann, H.; Fassnacht, M.; Allolio, B. Metastatic Adrenocortical Carcinoma: Results of 56 Pulmonary Metastasectomies in 24 Patients. Ann. Thorac. Surg. 2011, 92, 1965–1970. [Google Scholar] [CrossRef] [PubMed]
- Else, T.; Williams, A.R.; Sabolch, A.; Jolly, S.; Miller, B.S.; Hammer, G.D. Adjuvant Therapies and Patient and Tumor Characteristics Associated with Survival of Adult Patients with Adrenocortical Carcinoma. J. Clin. Endocrinol. Metab. 2014, 99, 455–461. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Megerle, F.; Herrmann, W.; Schloetelburg, W.; Ronchi, C.L.; Pulzer, A.; Quinkler, M.; Beuschlein, F.; Hahner, S.; Kroiss, M.; Fassnacht, M.; et al. Mitotane monotherapy in patients with advanced adrenocortical carcinoma. J. Clin. Endocrinol. Metab. 2018, 103, 1686–1695. [Google Scholar] [CrossRef]
- Sabra, M.M.; Sherman, E.J.; Tuttle, R.M. Tumor volume doubling time of pulmonary metastases predicts overall survival and can guide the initiation of multikinase inhibitor therapy in patients with metastatic, follicular cell-derived thyroid carcinoma. Cancer 2017, 123, 2955–2964. [Google Scholar] [CrossRef] [PubMed]
- Poullis, M.; Littler, J.; Gosney, J. Biology of colorectal pulmonary metastasis: Implications for surgical resection. Interact. Cardiovasc. Thorac. Surg. 2012, 14, 140–142. [Google Scholar] [CrossRef] [PubMed]
- Nomura, K.; Miyagawa, S.; Harada, H.; Kitamura, H.; Seki, H.; Shimada, R.; Kobayashi, A.; Noike, T.; Kawasaki, S. Relationship between doubling time of liver metastases from colorectal carcinoma and residual primary cancer. Dig. Surg. 1998, 15, 21–24. [Google Scholar] [CrossRef] [PubMed]
- Mantatzis, M.; Kakolyris, S.; Amarantidis, K.; Karayiannakis, A.; Prassopoulos, P. Treatment response classification of liver metastatic disease evaluated on imaging. Are RECIST unidimensional measurements accurate? Eur. Radiol. 2009, 19, 1809–1816. [Google Scholar] [CrossRef]
- Hayes, S.; Pietanza, M.; O’Driscoll, D.; Zheng, J.; Moskowitz, C.; Kris, M.; Ginsberg, M. Comparison of CT volumetric measurement with RECIST response in patients with lung cancer. Eur. J. Radiol. 2016, 85, 524–533. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Goldmacher, G.V.; Conklin, J. The use of tumour volumetrics to assess response to therapy in anticancer clinical trials. Br. J. Clin. Pharmacol. 2012, 73, 846–854. [Google Scholar] [CrossRef] [PubMed]
- Anderson, O.; Kidd, A.; Goatman, K.; Weir, A.; Voisey, J.; Dilys, V.; Siebert, J.; Blyth, K. Fully Automated Volumetric Measurement of Malignant Pleural Mesothelioma from Computed Tomography Images by Deep Learning: Preliminary Results of an Internal Validation. Bioimaging 2020, 2, 64–73. [Google Scholar] [CrossRef]
- Mozley, P.D.; Schwartz, L.H.; Bendtsen, C.; Zhao, B.; Petrick, N.; Buckler, A. Change in lung tumor volume as a biomarker of treatment response: A critical review of the evidence. Ann. Oncol. 2010, 21, 1751–1755. [Google Scholar] [CrossRef]
- Salman, Y. Modified technique for volumetric brain tumor measurements. J. Biomed. Sci. Eng. 2009, 02, 16–19. [Google Scholar] [CrossRef] [Green Version]
- Shetty, I.; Fuller, S.; Raygada, M.; Merino, M.J.; Thomas, B.J.; Widemann, B.C.; Reilly, K.M.; Pacak, K.; Del Rivero, J. Adrenocortical carcinoma masquerading as pheochromocytoma: A histopathologic dilemma. Endocrinol. Diabetes Metab. Case Rep. 2020, 2020, 19-0147. [Google Scholar] [CrossRef] [PubMed]
- Boland, G.W.L.; Dwamena, B.; Sangwaiya, M.J.; Goehler, A.G.; Blake, M.A.; Hahn, P.F.; Scott, J.A.; Kalra, M.K. Characterization of Adrenal Masses by Using FDG PET: A Systematic Review and Meta-Analysis of Diagnostic Test Performance. Radiology 2011, 259, 117–126. [Google Scholar] [CrossRef] [PubMed]
- Elaini, A.B.; Shetty, S.K.; Chapman, V.M.; Sahani, D.V.; Boland, G.W.; Sweeney, A.T.; Maher, M.M.; Slattery, J.T.; Mueller, P.R.; Blake, M.A. Improved Detection and Characterization of Adrenal Disease with PET-CT. RadioGraphics 2007, 27, 755–767. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wong, K.K.; Miller, B.S.; Viglianti, B.L.; Dwamena, B.A.; Gauger, P.G.; Cook, G.J.; Colletti, P.M.; Rubello, D.; Gross, M.D. Molecular imaging in the management of adrenocortical cancer: A systematic review. Clin. Nucl. Med. 2016, 41, e368–e382. [Google Scholar] [CrossRef] [PubMed]
- Ripley, R.T.; Kemp, C.D.; Davis, J.L.; Langan, R.C.; Royal, R.E.; Libutti, S.K.; Steinberg, S.M.; Wood, B.J.; Kammula, U.S.; Fojo, T.; et al. Liver resection and ablation for metastatic adrenocortical carcinoma. Ann. Surg. Oncol. 2011, 18, 1972–1979. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mauda-Havakuk, M.; Levin, E.; Levy, E.B.; Krishnasamy, V.P.; Anderson, V.; Jain, N.; Amalou, H.; Fojo, T.; Edgerly, M.; Wakim, P.G.; et al. Long-term outcomes in patients with advanced adrenocortical carcinoma after image-guided locoregional ablation or embolization. Cancer Med. 2021, 10, 2259–2267. [Google Scholar] [CrossRef] [PubMed]
- Assié, G.; Antoni, G.; Tissier, F.; Caillou, B.; Abiven, G.; Gicquel, C.; Leboulleux, S.; Travagli, J.-P.; Dromain, C.; Bertagna, X.; et al. Prognostic Parameters of Metastatic Adrenocortical Carcinoma. J. Clin. Endocrinol. Metab. 2007, 92, 148–154. [Google Scholar] [CrossRef]
- Ayabe, R.I.; Narayan, R.R.; Ruff, S.M.; Wach, M.M.; Lo, W.; Nierop, P.M.; Steinberg, S.M.; Ripley, R.T.; Davis, J.L.; Koerkamp, B.G.; et al. Disease-free interval and tumor functional status can be used to select patients for resection/ablation of liver metastases from adrenocortical carcinoma: Insights from a multi-institutional study. HPB (Oxford) 2019, 22, 169–175. [Google Scholar] [CrossRef]
- Tanaka, K.; Shimada, H.; Miura, M.; Fujii, Y.; Yamaguchi, S.; Endo, I.; Sekido, H.; Togo, S.; Ike, H. Metastatic Tumor Doubling Time: Most Important Prehepatectomy Predictor of Survival and Nonrecurrence of Hepatic Colorectal Cancer Metastasis. World J. Surg. 2004, 28, 263–270. [Google Scholar] [CrossRef]
- Nathani, P.; Gopal, P.; Rich, N.; Yopp, A.; Yokoo, T.; John, B.; Marrero, J.; Parikh, N.; Singal, A.G. Hepatocellular carcinoma tumour volume doubling time: A systemic review and meta-analysis. Gut 2020, 70, 401–407. [Google Scholar] [CrossRef] [PubMed]
- Miura, K.; Hamanaka, K.; Koizumi, T.; Kawakami, S.; Kobayashi, N.; Ito, K.-I. Solid component tumor doubling time is a prognostic factor in non-small cell lung cancer patients. J. Cardiothorac. Surg. 2019, 14, 57. [Google Scholar] [CrossRef]
- Joseph, W.L.; Morton, D.L.; Adkins, P.C. Variation in tumor doubling time in patients with pulmonary metastatic disease. J. Surg. Oncol. 1971, 3, 143–149. [Google Scholar] [CrossRef]
- Kim, J.K.; Kim, H.; Jun, M.; Yun, S.-C.; Shim, J.H.; Lee, H.C.; Lee, D.; An, J.; Lim, Y.-S.; Chung, Y.-H.; et al. Tumor Volume Doubling Time as a Dynamic Prognostic Marker for Patients with Hepatocellular Carcinoma. Dig. Dis. Sci. 2017, 62, 2923–2931. [Google Scholar] [CrossRef]
- Mehran, R.J. Resection for Pulmonary Metastases, in Medical Management of the Thoracic Surgery Patient; Elsevier Inc.: Philadelphia, PA, USA, 2010; pp. 308–310. [Google Scholar]
- Nakamura, T.; Matsumine, A.; Takao, M.; Nakatsuka, A.; Matsubara, T.; Asanuma, K.; Sudo, A. Impact of tumor volume doubling time on post-metastatic survival in bone or soft-tissue sarcoma patients treated with metastasectomy and/or radiofrequency ablation of the lung. Onco. Targ. Ther. 2017, 10, 559–564. [Google Scholar] [CrossRef] [Green Version]
- Oh, S.Y.; Lee, J.H.; Lee, H.J.; Kim, T.H.; Huh, Y.-J.; Ahn, H.-S.; Suh, Y.-S.; Kong, S.-H.; Kim, G.H.; Ahn, S.J.; et al. Natural History of Gastric Cancer: Observational Study of Gastric Cancer Patients Not Treated During Follow-Up. Ann. Surg. Oncol. 2019, 26, 2905–2911. [Google Scholar] [CrossRef] [PubMed]
- Eisenhauer, E.A.; Therasse, P.; Bogaerts, J.; Schwartz, L.; Sargent, D.; Ford, R.; Dancey, J.; Arbuck, S.; Gwyther, S.; Mooney, M.; et al. New response evaluation criteria in solid tumours: Revised RECIST guideline (version 1.1). Eur. J. Cancer 2009, 45, 228–238. [Google Scholar] [CrossRef] [PubMed]




{kind=link}
{kind=link}
{kind=link}
| ID | Sex and Age at Diagnosis | Metastatic Lesions Per Organ | ∆T * (Days) | Mitotane | Mitotane Levels (µg/mL) | Systemic Therapy Treatment History | |||
|---|---|---|---|---|---|---|---|---|---|
| Liver | Lung | Lymph Nodes | Other | ||||||
| 1 | M33 | 0 | 4 | 2 | 0 | 63 | Yes | 3.3 | PSC VALS 5CY, mitotane Velban × 5 cycles, |
| 2 | M31 | 0 | 5 | 0 | 0 | 55 | Yes | 3.7 | Records unclear, possibly on MAVE from June 1999–Feb 2000 |
| 4 | F46 | 0 | 4 | 1 | 0 | 56 | Yes | 4.1 | Tariquidar/MAVE (mitotane, Adriamycin, vincristine, and etoposide) × 6 cyclesGemcitabine and cisplatin × 6 cycles. |
| 5 | M32 | 5 | 0 | 0 | 0 | 36 | Yes | 1.1 | None prior |
| 6 | F58 | 0 | 2 | 0 | 0 | 175 | No | - | None prior |
| 7 | F36 | 1 | 0 | 1 | 1 | 60 | Yes | 1.1 | None prior |
| 8 | M55 | 0 | 3 | 0 | 1 | 171 | Yes | 5.9 | None prior |
| 9 | M67 | 2 | 0 | 0 | 0 | 100 | Yes | 5.0 | Mitotane likely held with subtherapeutic levels, medical records unclear |
| 10 | F57 | 0 | 4 | 0 | 0 | 91 | No | - | None during measurement period |
| 11 | F57 | 0 | 0 | 1 | 0 | 191 | Yes | <1.0 | None prior |
| 12 | F70 | 2 | 5 | 0 | 0 | 33 | No | - | None prior |
| 14 | M61 | 1 | 0 | 1 | 0 | 90 | No | - | None prior |
| Lesion | Estimate | 95% CI | Diff from L | 95% CI |
|---|---|---|---|---|
| L | 0.341 | (0.177, 0.504) | - | - |
| N | 0.095 | (0.058, 0.132) | 0.246 | (0.034, 0.458) |
| P | 0.101 | (0.071, 0.130) | 0.240 | (0.029, 0.451) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Fuller, S.N.; Shafiei, A.; Venzon, D.J.; Liewehr, D.J.; Mauda Havanuk, M.; Ilanchezhian, M.G.; Edgerly, M.; Anderson, V.L.; Levy, E.B.; Hoang, C.D.; et al. Tumor Doubling Time Using CT Volumetric Segmentation in Metastatic Adrenocortical Carcinoma. Curr. Oncol. 2021, 28, 4357-4366. https://doi.org/10.3390/curroncol28060370
Fuller SN, Shafiei A, Venzon DJ, Liewehr DJ, Mauda Havanuk M, Ilanchezhian MG, Edgerly M, Anderson VL, Levy EB, Hoang CD, et al. Tumor Doubling Time Using CT Volumetric Segmentation in Metastatic Adrenocortical Carcinoma. Current Oncology. 2021; 28(6):4357-4366. https://doi.org/10.3390/curroncol28060370
Chicago/Turabian StyleFuller, Sarah N., Ahmad Shafiei, David J. Venzon, David J. Liewehr, Michal Mauda Havanuk, Maran G. Ilanchezhian, Maureen Edgerly, Victoria L. Anderson, Elliot B. Levy, Choung D. Hoang, and et al. 2021. "Tumor Doubling Time Using CT Volumetric Segmentation in Metastatic Adrenocortical Carcinoma" Current Oncology 28, no. 6: 4357-4366. https://doi.org/10.3390/curroncol28060370