A Critical Appraisal of Evidence- and Consensus-Based Guidelines for Actinic Keratosis

 , , ,
, , ,  ,
, {kind=link}
{kind=link}
{kind=link}
Abstract
:1. Introduction
2. Materials and Methods
2.1. Eligibility Criteria
2.2. Search Strategy and Selection of Guidelines
2.3. Data Extraction and Rating of the Guidelines
2.4. Analysis
3. Results
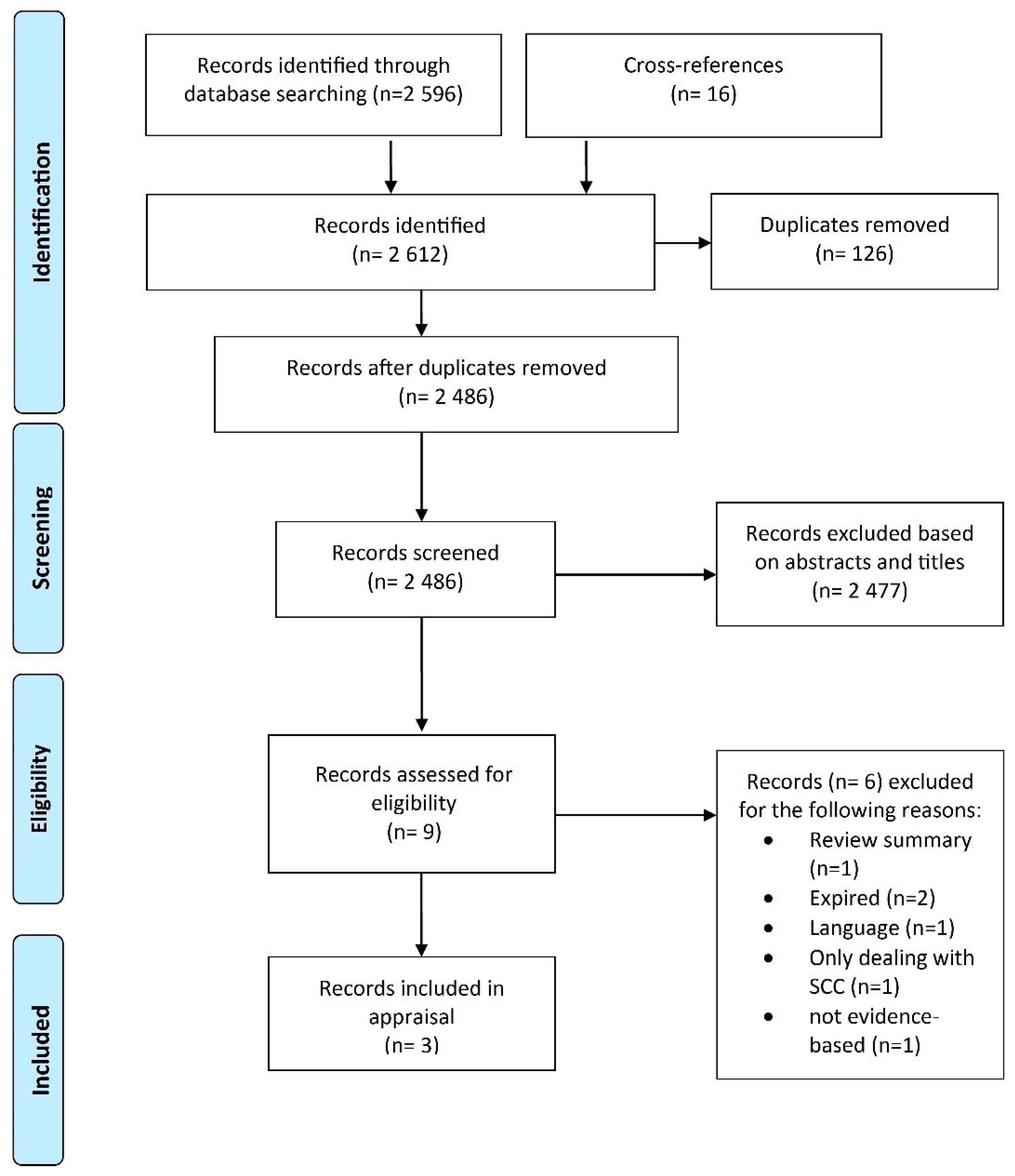
3.1. Guideline Identification
3.2. Evaluation of the Guidelines
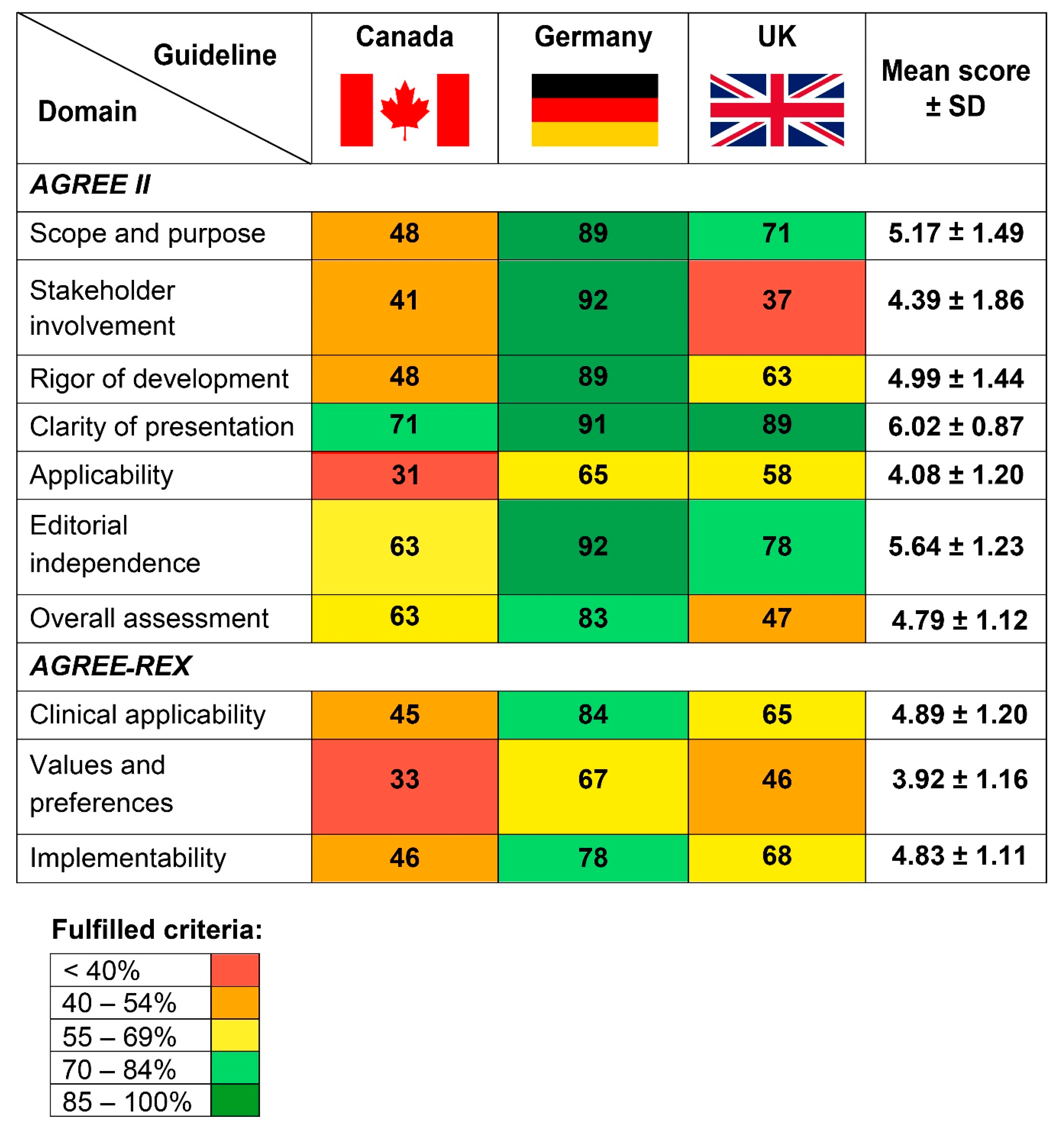
3.3. AGREE II
3.3.1. Scope and Purpose
3.3.2. Stakeholder Involvement
3.3.3. Rigor of Development
3.3.4. Clarity and Presentation
3.3.5. Applicability
3.3.6. Editorial Independence
3.3.7. Overall Assessment
3.4. AGREE-REX
3.4.1. Clinical Applicability
3.4.2. Values and Preferences
3.4.3. Implementability
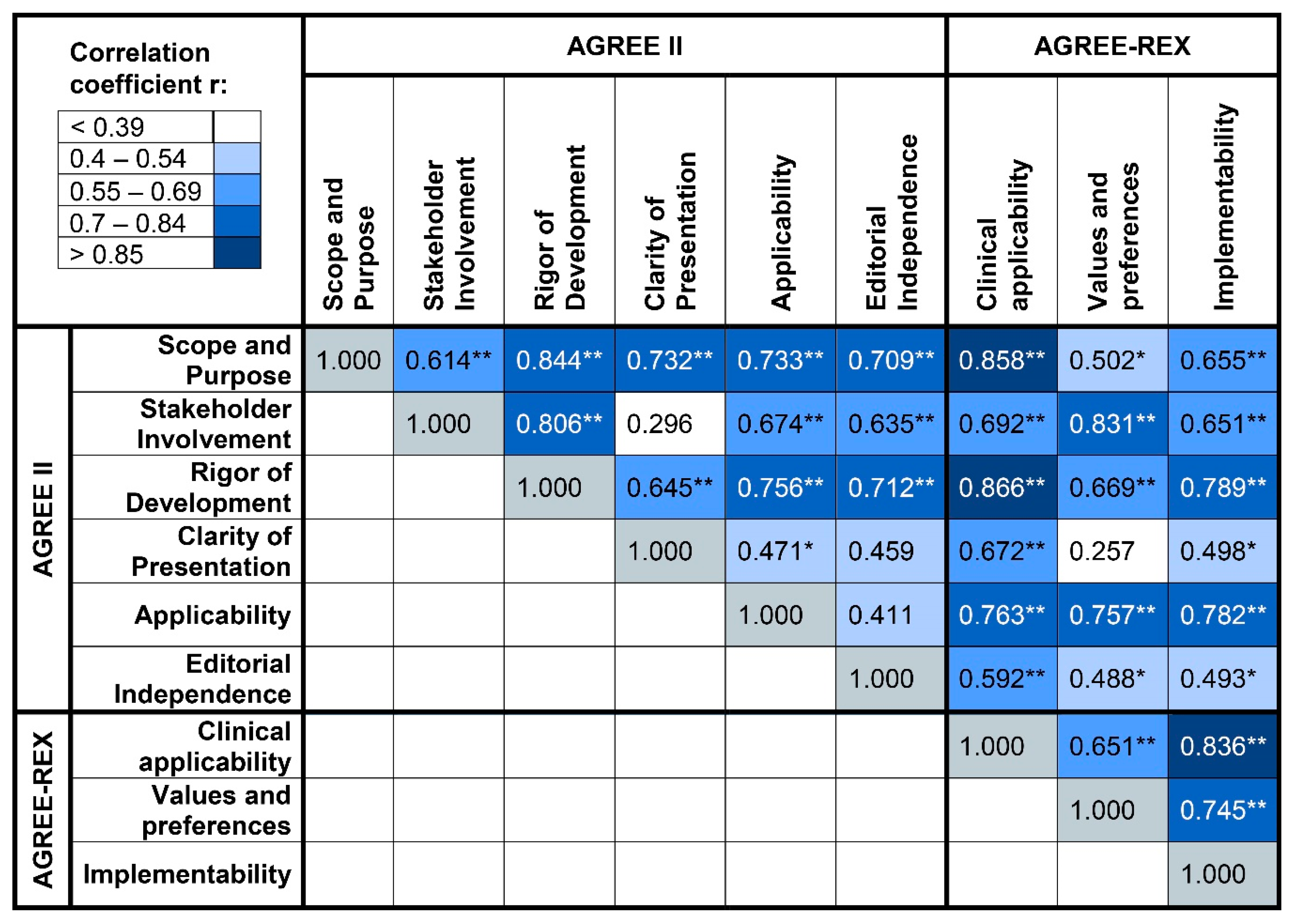
3.5. Correlations of the AGREE II and AGREE-REX Domains
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Cantisani, C.; Paolino, G.; Melis, M.; Faina, V.; Romaniello, F.; Didona, D.; Cardone, M.; Calvieri, S. Actinic Keratosis Pathogenesis Update and New Patents. Recent Pat. Inflamm Allergy Drug Discov. 2016, 10, 40–48. [Google Scholar] [CrossRef] [PubMed]
- Moy, R.L. Clinical presentation of actinic keratoses and squamous cell carcinoma. J. Am. Acad. Derm. 2000, 42, 8–10. [Google Scholar] [CrossRef] [PubMed]
- Criscione, V.D.; Weinstock, M.A.; Naylor, M.F.; Luque, C.; Eide, M.J.; Bingham, S.F.; The Department of Veteran Affairs Topical Tretinoin Chemoprevention Trial Group. Actinic keratoses: Natural history and risk of malignant transformation in the Veterans Affairs Topical Tretinoin Chemoprevention Trial. Cancer 2009, 115, 2523–2530. [Google Scholar] [CrossRef]
- Poulin, Y.; Lynde, C.W.; Barber, K.; Vender, R.; Claveau, J.; Bourcier, M.; Ashkenas, J.; Canadian Non-Melanoma Skin Cancer Guidelines Committee. Non-melanoma Skin Cancer in Canada Chapter 3: Management of Actinic Keratoses. J. Cutan Med. Surg. 2015, 19, 227–238. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Leitlinienprogramm Onkologie (Deutsche Krebsgesellschaft, D.K., AWMF), S3-Leitlinie Aktinische Keratose und Plattenepithelkarzinom der Haut, Langversion 1.1. 2020. AWMF Registernummer: 032/022OL. Available online: https://www.leitlinienprogramm-onkologie.de/leitlinien/aktinische-keratosen-und-plattenepithelkarzinom-der-haut/ (accessed on 28 April 2020).
- de Berker, D.; McGregor, J.M.; Mohd Mustapa, M.F.; Exton, L.S.; Hughes, B.R. British Association of Dermatologists' guidelines for the care of patients with actinic keratosis 2017. Br. J. Derm. 2017, 176, 20–43. [Google Scholar] [CrossRef] [Green Version]
- Del Duca, E.; Manfredini, M.; Petrini, N.; Farnetani, F.; Chester, J.; Bennardo, L.; Schipani, G.; Tamburi, F.; Sannino, M.; Cannarozzo, G.; et al. Daylight Photodynamic Therapy with 5-aminolevulinic acid 5% gel for the treatment of mild-to-moderate inflammatory acne. G Ital. Derm. Venereol. 2019. [Google Scholar] [CrossRef]
- Steeb, T.; Wessely, A.; Leiter, U.; French, L.E.; Berking, C.; Heppt, M.V. The more the better? An appraisal of combination therapies for actinic keratosis. J. Eur. Acad. Derm. Venereol. 2020, 34, 727–732. [Google Scholar] [CrossRef] [Green Version]
- Heppt, M.V.; Steeb, T.; Leiter, U.; Berking, C. Efficacy of photodynamic therapy combined with topical interventions for the treatment of actinic keratosis: A meta-analysis. J. Eur. Acad. Derm. Venereol. 2019, 33, 863–873. [Google Scholar] [CrossRef] [PubMed]
- Heppt, M.V.; Leiter, U.; Steeb, T.; Amaral, T.; Bauer, A.; Becker, J.C.; Breitbart, E.; Breuninger, H.; Diepgen, T.; Dirschka, T.; et al. S3 guideline for actinic keratosis and cutaneous squamous cell carcinoma—Short version, part 1: Diagnosis, interventions for actinic keratoses, care structures and quality-of-care indicators. J. Dtsch. Derm. Ges. 2020, 18, 275–294. [Google Scholar] [CrossRef] [Green Version]
- Heppt, M.V.; Steeb, T.; Ruzicka, T.; Berking, C. Cryosurgery combined with topical interventions for actinic keratosis: A systematic review and meta-analysis. Br. J. Derm. 2019, 180, 740–748. [Google Scholar] [CrossRef] [Green Version]
- Steeb, T.; Schlager, J.G.; Kohl, C.; Ruzicka, T.; Heppt, M.V.; Berking, C. Laser-assisted photodynamic therapy for actinic keratosis: A systematic review and meta-analysis. J. Am. Acad. Derm. 2019, 80, 947–956. [Google Scholar] [CrossRef] [PubMed]
- Steeb, T.; Wessely, A.; von Bubnoff, D.; Dirschka, T.; Drexler, K.; Falkenberg, C.; Hassel, J.C.; Hayani, K.; Huning, S.; Kahler, K.C.; et al. Treatment Motivations and Expectations in Patients with Actinic Keratosis: A German-Wide Multicenter, Cross-Sectional Trial. J. Clin. Med. 2020, 9, 1438. [Google Scholar] [CrossRef]
- Brouwers, M.C.; Kho, M.E.; Browman, G.P.; Burgers, J.S.; Cluzeau, F.; Feder, G.; Fervers, B.; Graham, I.D.; Grimshaw, J.; Hanna, S.E.; et al. AGREE II: Advancing guideline development, reporting and evaluation in health care. CMAJ 2010, 182, E839–E842. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- AGREE-REX Research Team. The Appraisal of Guidelines Research & Evaluation—Recommendation EXcellence (AGREE-REX) [Electronic Version]. Available online: https://www.agreetrust.org/resource-centre/agree-rex-recommendation-excellence/ (accessed on 23 March 2020).
- Steeb, T.; Hayani, K.M.; Forster, P.; Liegl, R.; Toussaint, F.; Schlaak, M.; Berking, C.; Heppt, M.V. Guidelines for uveal melanoma: A critical appraisal of systematically identified guidelines using the AGREE II and AGREE-REX instrument. J. Cancer Res. Clin. Oncol. 2020, 146, 1079–1088. [Google Scholar] [CrossRef] [Green Version]
- AGREE Next Steps Consortium. The AGREE II Instrument [Electronic Version]. Available online: http://www.agreetrust.org (accessed on 23 March 2020).
- Landis, J.R.; Koch, G.G. The measurement of observer agreement for categorical data. Biometrics 1977, 33, 159–174. [Google Scholar] [CrossRef] [Green Version]
- Werner, R.N.; Stockfleth, E.; Connolly, S.M.; Correia, O.; Erdmann, R.; Foley, P.; Gupta, A.K.; Jacobs, A.; Kerl, H.; Lim, H.W.; et al. Evidence- and consensus-based (S3) Guidelines for the Treatment of Actinic Keratosis—International League of Dermatological Societies in cooperation with the European Dermatology Forum—Short version. J. Eur. Acad. Dermatol. Venereol. 2015, 29, 2069–2079. [Google Scholar] [CrossRef] [Green Version]
- Werner, R.N.; Stockfleth, E.; Connolly, S.M.; Correia, O.; Erdmann, R.; Foley, P.; Gupta, A.K.; Jacobs, A.; Kerl, H.; Lim, H.W.; et al. Evidence- and Consensus-Based (S3) Guidelines for the Treatment of Actinic Keratosis—International League of Dermatological Societies in Cooperation with the European Dermatology Forum—Long Version (Online Supplement). Available online: https://onlinelibrary.wiley.com/action/downloadSupplement?doi=10.1111%2Fjdv.13179&file=jdv13179-sup-0001-SuppInfo.pdf (accessed on 19 May 2020).
- Scottish Intercollegiate Guidelines Network (SIGN). Management of Primary Cutaneous Squamous Cell Carcinoma. Available online: https://www.sign.ac.uk/sign-140-management-of-primary-cutaneous-squamous-cell-carcinoma (accessed on 19 May 2020).
- Peris, K.; Calzavara-Pinton, P.G.; Neri, L.; Girolomoni, G.; Malara, G.; Parodi, A.; Piaserico, S.; Rossi, R.; Pellacani, G. Italian expert consensus for the management of actinic keratosis in immunocompetent patients. J. Eur. Acad. Dermatol. Venereol. 2016, 30, 1077–1084. [Google Scholar] [CrossRef]
- Baaten, G.; Buis, P.; Damen, Z.; De Haas, E.; Van der Heide, W.; Opstelten, W.; Smeink, P.; De Vijlder, H. NHG-Standaard Verdachte huidafwijkingen. Available online: https://www.nhg.org/standaarden/samenvatting/verdachte-huidafwijkingen (accessed on 18 May 2020).
- Gutzmer, R.; Wiegand, S.; Kolbl, O.; Wermker, K.; Heppt, M.; Berking, C. Actinic keratosis and cutaneous squamous cell carcinoma—Treatment options. Dtsch. Arztebl. Int. 2019, 116. (In German) [Google Scholar] [CrossRef] [Green Version]
- Leiter, U.; Heppt, M.V.; Steeb, T.; Amaral, T.; Bauer, A.; Becker, J.C.; Breitbart, E.; Breuninger, H.; Diepgen, T.; Dirschka, T.; et al. S3 guideline for actinic keratosis and cutaneous squamous cell carcinoma (cSCC)—Short version, part 2: Epidemiology, surgical and systemic treatment of cSCC, follow-up, prevention and occupational disease. J. Dtsch. Derm. Ges. 2020, 18, 400–413. [Google Scholar] [CrossRef]
- Bickers, D.R.; Lim, H.W.; Margolis, D.; Weinstock, M.A.; Goodman, C.; Faulkner, E.; Gould, C.; Gemmen, E.; Dall, T.; American Academy of Dermatology, A.; et al. The burden of skin diseases: 2004 a joint project of the American Academy of Dermatology Association and the Society for Investigative Dermatology. J. Am. Acad. Derm. 2006, 55, 490–500. [Google Scholar] [CrossRef]
- Werner, R.N.; Marinovic, B.; Rosumeck, S.; Strohal, R.; Haering, N.S.; Weberschock, T.; Dreher, A.C.; Nast, A. The quality of European dermatological guidelines: Critical appraisal of the quality of EDF guidelines using the AGREE II instrument. J. Eur. Acad. Derm. Venereol. 2016, 30, 395–403. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Nast, A.; Spuls, P.H.; Ormerod, A.D.; Reytan, N.; Saiag, P.H.; Smith, C.H.; Rzany, B. A critical appraisal of evidence-based guidelines for the treatment of psoriasis vulgaris: ‘AGREE-ing’ on a common base for European evidence-based psoriasis treatment guidelines. J. Eur. Acad. Derm. Venereol. 2009, 23, 782–787. [Google Scholar] [CrossRef] [PubMed]
- Gras, J. Ingenol mebutate: A new option for actinic keratosis treatment. Drugs Today 2013, 49, 15–22. [Google Scholar] [CrossRef] [PubMed]
- Steeb, T.; Wessely, A.; Drexler, K.; Salzmann, M.; Toussaint, F.; Heinzerling, L.; Reinholz, M.; Berking, C.; Heppt, M.V. The Quality of Practice Guidelines for Melanoma: A Methodologic Appraisal with the AGREE II and AGREE-REX Instruments. Cancers (Basel) 2020, 12, 1613. [Google Scholar] [CrossRef] [PubMed]



Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Wessely, A.; Steeb, T.; Heppt, F.; Hornung, A.; Kaufmann, M.D.; Koch, E.A.T.; Toussaint, F.; Erdmann, M.; Berking, C.; Heppt, M.V. A Critical Appraisal of Evidence- and Consensus-Based Guidelines for Actinic Keratosis. Curr. Oncol. 2021, 28, 950-960. https://doi.org/10.3390/curroncol28010093
Wessely A, Steeb T, Heppt F, Hornung A, Kaufmann MD, Koch EAT, Toussaint F, Erdmann M, Berking C, Heppt MV. A Critical Appraisal of Evidence- and Consensus-Based Guidelines for Actinic Keratosis. Current Oncology. 2021; 28(1):950-960. https://doi.org/10.3390/curroncol28010093
Chicago/Turabian StyleWessely, Anja, Theresa Steeb, Franz Heppt, Annkathrin Hornung, Matthias D. Kaufmann, Elias A. T. Koch, Frédéric Toussaint, Michael Erdmann, Carola Berking, and Markus V. Heppt. 2021. "A Critical Appraisal of Evidence- and Consensus-Based Guidelines for Actinic Keratosis" Current Oncology 28, no. 1: 950-960. https://doi.org/10.3390/curroncol28010093