Noninvasive Skin Barrier Assessment: Multiparametric Approach and Pilot Study


Department of Dermatology, Radboud University Medical Center, PO Box 9101, 6500 HB Nijmegen, The Netherlands
*
Author to whom correspondence should be addressed.
§
Both authors contributed equally to this work.
Cosmetics 2019, 6(1), 20; https://doi.org/10.3390/cosmetics6010020
Submission received: 8 February 2019
/
Revised: 1 March 2019
/
Accepted: 13 March 2019
/
Published: 15 March 2019
(This article belongs to the Special Issue Skin Barrier Function)
Abstract
:The epidermal barrier function is disrupted in various inflammatory skin diseases. Accurate methods to measure skin barrier function are needed to assess the effect of therapeutic agents. Therefore, we developed a noninvasive multiparametric approach to measure four different parameters regarding the skin barrier. In the current pilot study, we evaluate this method in 14 healthy volunteers. We assessed erythema, transepidermal water loss (TEWL), water content, and epidermal thickness at both cheeks before and 30 min after application of Lanette and Vaseline-Lanette cream. For this, we used spectrophotometry, the Aquaflux device, the Epsilon device, and reflection confocal microscopy, respectively. Stratum corneum (SC) thickness was significantly increased after application of both creams (p < 0.05), and this increase was larger after Lanette cream compared to after Vaseline-Lanette cream (p = 0.035). Erythema, TEWL, and water content did not significantly change after cream application. Our multiparametric approach is promising and offers a feasible and practical way to quickly obtain multifaceted information about skin barrier function. Further exploration of this approach after prolonged use of cream and in conditions of disrupted skin barrier are recommended areas for future research.
1. Introduction
The skin barrier acts as a first-order shield to protect the human body against micro-organisms, ultraviolet (UV) light, and mechanical injury, and also helps regulate temperature and water flux [1,2]. It is predominantly formed by the outermost layer of human epithelial cells, the stratum corneum (SC) [3]. The skin barrier function is disrupted in inflammatory skin diseases like rosacea and atopic dermatitis [4,5,6,7,8,9,10]. An impaired skin barrier is characterized by increased transepidermal water loss (TEWL) and reduced epidermal hydration, and predisposes one to cutaneous inflammation [2]. Conversely, skin moisturizers can improve the skin barrier and help prevent inflammation [2,9,11,12,13,14]. However, not all moisturizers are beneficial to the skin barrier, and, for unknown reasons, some topical ointments may exacerbate symptoms in inflammatory skin disease [15,16].
The skin barrier function is most often assessed using methods that quantify water content and TEWL. Unfortunately, these are single-device methods that measure only one or a few parameters, while a multiparametric approach is preferred to better assess subtle features of skin damage and restoration in the very complex environment of the skin. In order to better understand the mechanisms of skin therapeutic agents, accurate, objective, and reliable methods to measure skin barrier function are needed. In addition to water content and TEWL, other skin parameters may influence skin barrier function, such as natural moisturizing factor (NMF), SC thickness, dermal vasodilatation (erythema), intracellular lipids, and pH [2,4,15]. A wide array of noninvasive biophysical and imaging methods are available to assess most of these parameters [17]. In the current pilot study, we demonstrate the feasibility of combining a quartet of biophysical/imaging devices to measure the following four skin parameters noninvasively: erythema, TEWL, water content, and epidermal thickness. These four skin parameters were selected for their ability to be measured in the face and for their practical use. To the best of our knowledge, this combination of parameters was never previously studied in skin barrier assessment. We quantify these parameters before and after the application of two different creams.
2. Materials and Methods
2.1. Study Subjects
Fourteen healthy Caucasian volunteers (12 women and two men; mean age, 24 years; range, 21–26 years) with skin types I to III were included in the study after providing written informed consent. The study was approved by the local medical ethics committee and conducted according to the principles of the Declaration of Helsinki. Measurements were performed in October 2018 at the department of Dermatology, Radboud University Medical Center, Nijmegen, the Netherlands. The following exclusion criteria were adopted: age < 18 years, signs of skin disease at measurement sites, known hypersensitivity reaction to Vaseline/Lanette cream, use of immunosuppressive medication, or a diagnosis of inflammatory skin disease. Subjects did not use cream, body lotion, make-up, or perfume on the day of measurements and refrained from physical exercise within three hours before measurements.
2.2. Products
We applied two widely used vehicles that are able to penetrate the skin within 30 min: Lanette cream and Vaseline-Lanette cream (Table 1).
2.3. Study Procedures and Technical Device Specifications
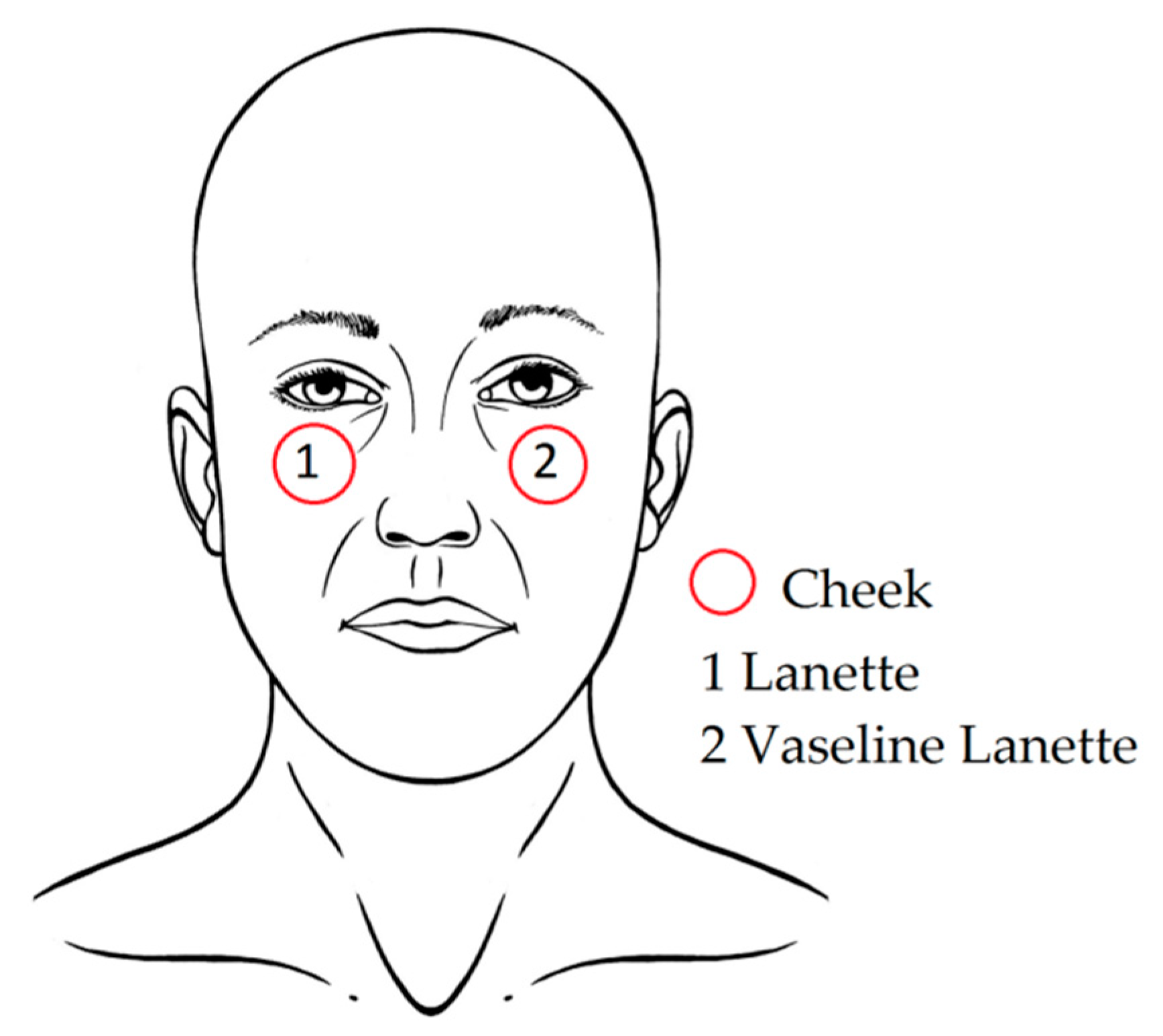
Measurements of the four skin barrier parameters (erythema, TEWL, water content, and SC and epidermal thickness) were performed on both cheeks. Firstly, measurement locations were demarcated with a surgical pen (Figure 1). Table 2 shows a detailed overview of the measurement principles of the four devices used to measure the skin barrier parameters. Facial skin was acclimatized to the ambient air for at least 10 min before the start of the measurements, and room temperature and air humidity were kept constant at 20–23 °C and 38–55%, respectively. Volunteers were laid down in supine position during the acclimatization period and measurement period to prevent possible orthostatic interactions.
Firstly, erythema was measured with a spectrophotometer (CM-2600d, Konica Minolta, Ramsey, NJ, USA). Using the principle of diffuse reflectance spectroscopy, light absorption from primary chromophores in the skin (melanin, oxyhemoglobin, and deoxy-hemoglobin) was measured [19]. Before each measuring session, calibration to a standard white plate provided with the meter was performed. After pressing the calibrate button, three calibration measurements were automatically taken. Next, three measurements on each cheek were taken; the device was lifted and gently reapplied between each recording. The average of the three consecutive erythema measurements was automatically calculated by the device. The measuring head was kept steady and perpendicular to the skin surface with very light pressure against the skin during measurements to prevent minor venous congestion. More detailed information about measurement requirements can be found in Fullerton et al. [18].
Next, TEWL was measured with the Aquaflux (AF200, Biox, London, UK). After calibration, three measurements per cheek were performed with standard settings and a maximum measurement time of 180 s. The average of the three measurements per cheek side was calculated. Also, the Aquaflux device was kept steady and perpendicular to the skin surface with very light skin pressure during measurements.
Thirdly, water content was determined by performing one measurement per cheek with the Epsilon (E100, Biox, London, UK), a new-generation corneometer. Compared to conventional single-sensor corneometers, the Epsilon contains 76,800 sensors; thus, multiple measurements take place at once [25]. Moreover, analysis software is integrated into the device, and water-content-based images can be obtained. The burst mode option was used with a 5-s measurement delay after first skin contact to rule out initial variation in skin occlusion. A frame interval of 1 s and a total measurement window of 30 s was selected. To keep contact with the skin surface, moderate pressure was applied.
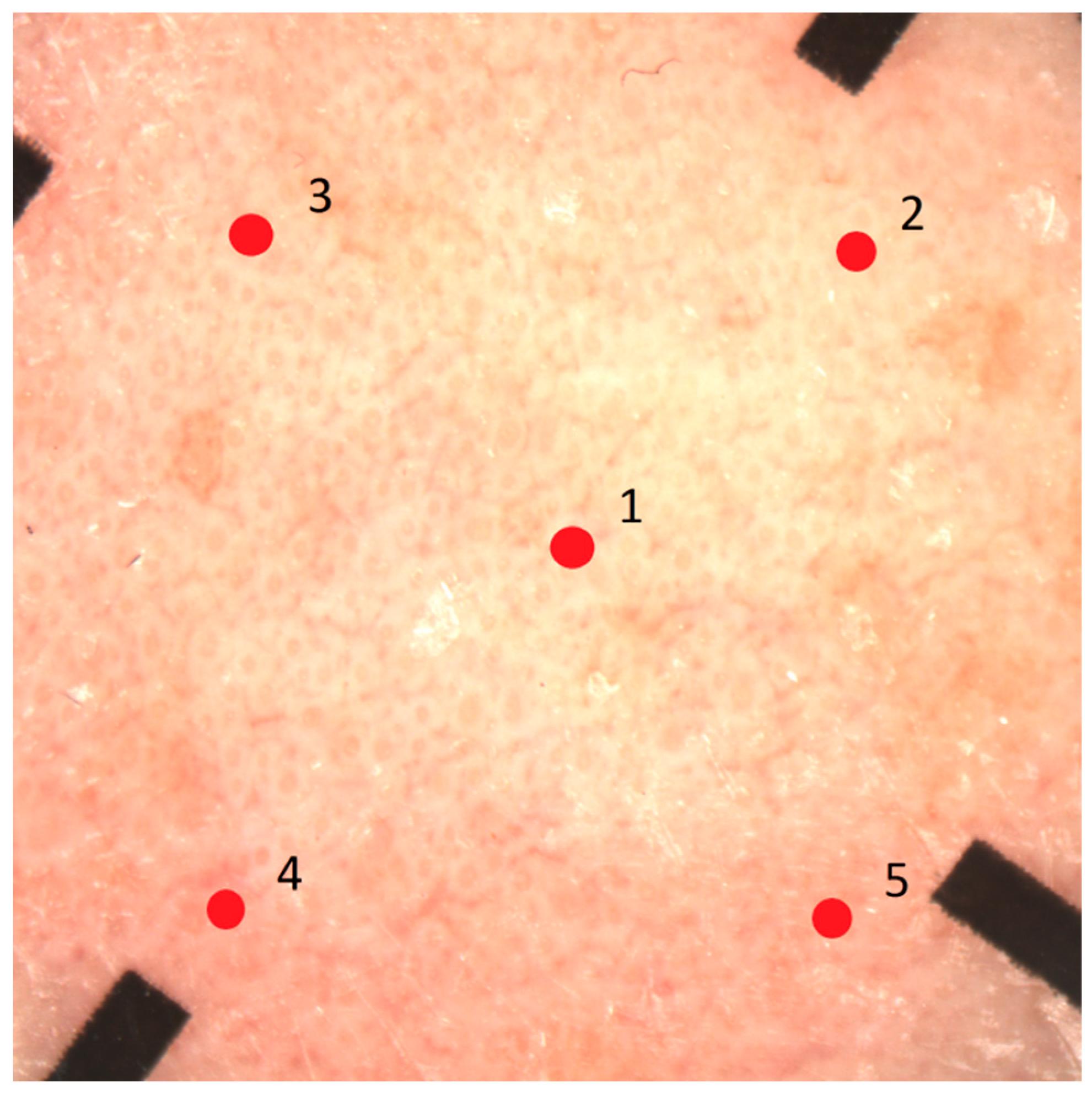
Lastly, the reflectance confocal microscope (RCM; Vivascope 1500, Mavig, Munich, Germany) was used to determine skin thickness. For each cheek, one dermoscopic image (VivaCam) was obtained and used as map. Next, five vertical mappings (VivaStacks) were performed at the center and at the four outer corners of the image (Figure 2). Series of images of 0.5 mm × 0.5 mm were obtained, starting from the skin surface up to a depth of 100 µm with interval steps of 3 µm. With a standardized protocol (Figure S1, Supplementary Materials) all VivaStack images were evaluated by one researcher to determine thickness of the SC and the viable epidermis (without SC).
After baseline measurements, the Lanette cream was applied to the right cheek, and the Vaseline-Lanette cream was applied to the left cheek (Figure 1). One finger-tip unit (FTU) of cream was used per cheek side, according to the finger-tip method [28]. One FTU corresponds to 0.5 g. After 30 min, the creams were completely absorbed into the skin, and all skin parameter measurements (erythema, TEWL, water content, and epidermal thickness) were repeated as described above.
2.4. Analysis
Burst mode values from the Epsilon measurements were used to create regression functions, and intersections with the y-axis were calculated. Statistical analysis was performed with SPSS (SPSS statistics 25, IBM Corporation, Armonk, NY, USA). Possible baseline differences of the skin barrier parameters between the right and left cheek were explored with the Wilcoxon signed-rank test. The Wilcoxon signed-rank test was also used to demonstrate significant differences between skin barrier parameters before and after application of both creams. A relationship between the skin parameters and environmental factors was investigated using Spearman’s correlation. For the results, p-values below 0.05 were considered significant.
3. Results
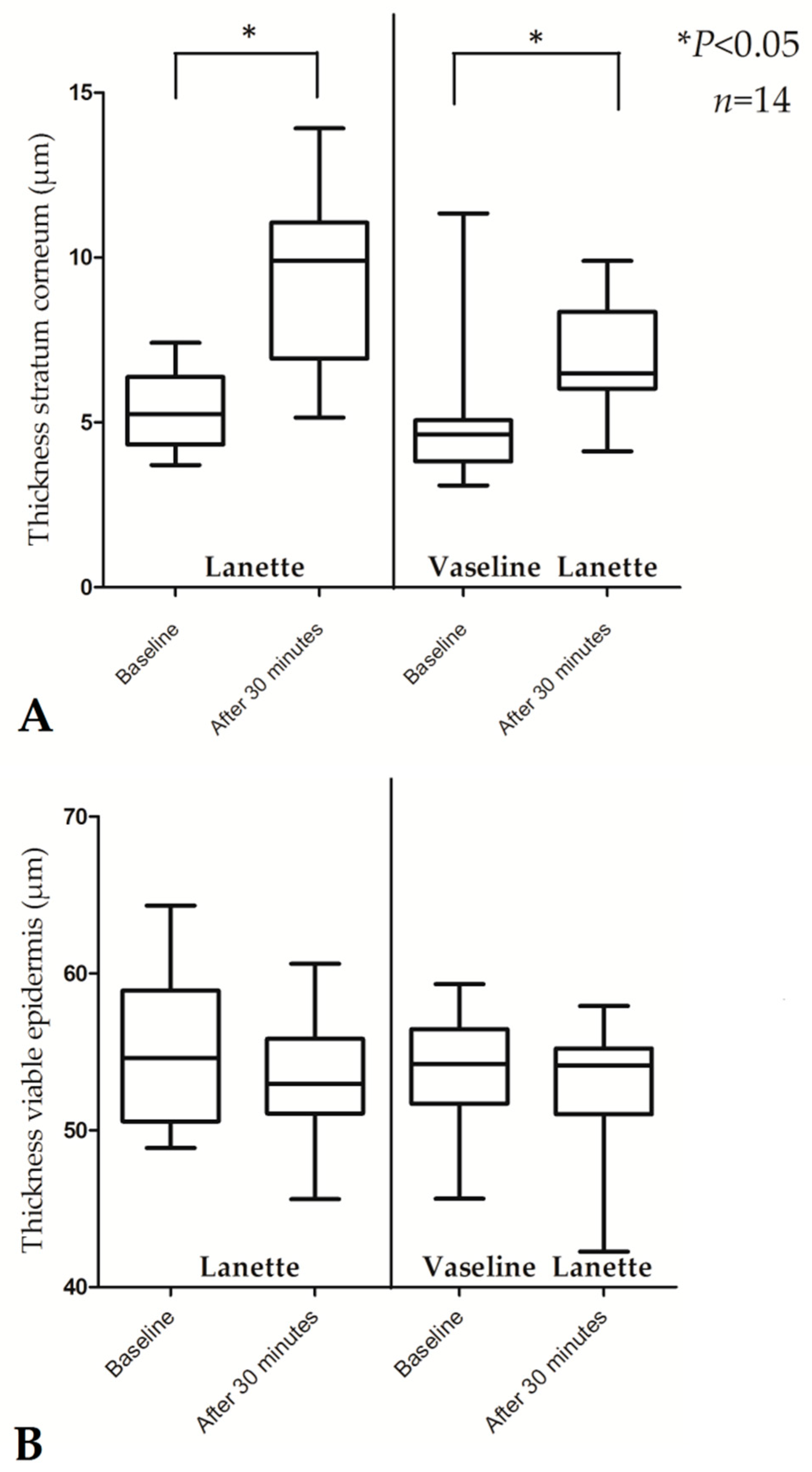
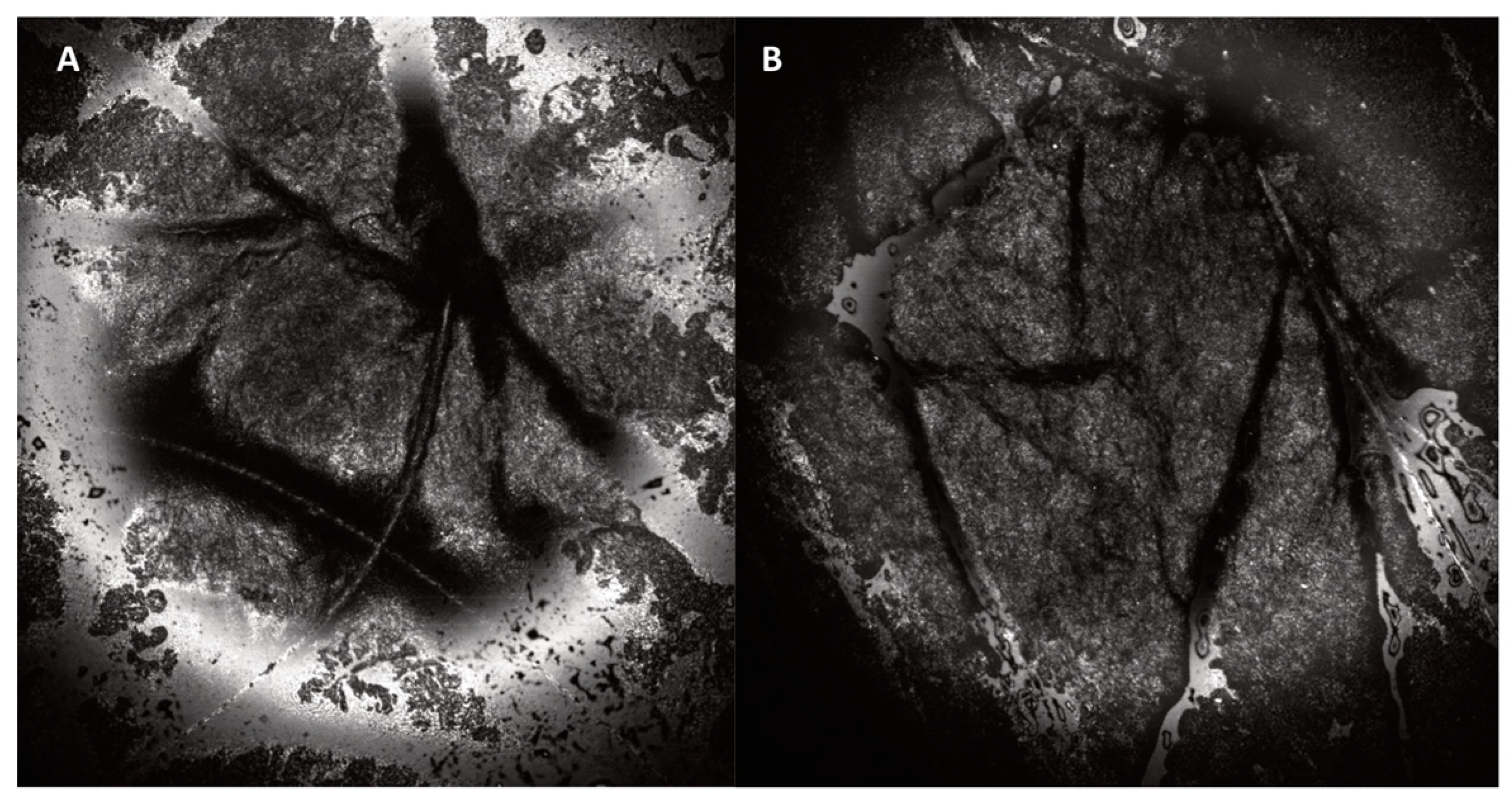
Compared to baseline, the thickness of the SC increased significantly after application of both creams (p < 0.05, Figure 3 and Table 3). The absolute difference of the SC thickness before and after application was significantly larger for Lanette cream compared to Vaseline-Lanette cream (p = 0.035). Figure 4 shows no morphological changes of corneocytes in the SC after cream application with the RCM. Erythema, TEWL, water content, and thickness of the viable epidermis did not significantly change after application of Lanette cream and Vaseline-Lanette cream. Additionally, relatively large interindividual variations among skin parameters were seen. Values of all skin parameters at baseline compared to 30 min after cream application per subject are displayed in Figure S2 and Table S1 (Supplementary Materials). No significant differences in median baseline values of erythema, TEWL, water content, and thickness of the SC and the viable epidermis were found between the right and left cheek among subjects (p > 0.050 for all values).
There were no significant relationships between the four skin parameters. Additionally, no biologically relevant correlations between the skin parameters and environmental factors were found (data not shown).
4. Discussion
This is the first study that combines the noninvasive measurements of erythema, TEWL, water content, and epidermal thickness to assess the effects of indifferent creams on the healthy skin barrier. Cream application did not affect erythema, TEWL, and water content 30 min after application on the cheeks, but did lead to increased SC thickness. The four modalities used in this study (spectrophotometer, Aquaflux, Epsilon, RCM) can monitor the same facial skin location over time without discomfort, damage, or alteration. All devices are portable and easy to use, and measurements are painless and rapid (15 min total).
To measure TEWL, we used the Aquaflux, a condenser closed-chamber system. Earlier research showed that this chamber system is the most sensitive TEWL system, allowing continuous measurements, and is the least vulnerable to environmental influences [21,29]. However, some drawbacks have to be taken into account. The device glides easily on the skin during measurements; manual fixation is recommended, which we did. Start-up time including calibration takes relatively long (15 min); thus, this should be prepared before measurements. Additionally, repeated measurements on exactly the same location are challenging due to the small probe. This might have resulted in small intraindividual variations, because TEWL values can vary between facial areas [30,31,32].
Water content was measured with the Epsilon, a state-of-the-art corneometer using multi-sensor skin mapping technology with correction for skin occlusive effects [24,25]. The sensing depth of the Epsilon is restricted to the less hydrated SC, in contrast to earlier model conventional corneometers that measure the deeper, more hydrated epidermis [32,33]; this potentially leads to more accurate water content values. The Epsilon showed significant variations in water content at different anatomical skin locations [25]; however, the size of the probe head (ca. 4 cm × 3 cm) restricts measurements to non-recessed body parts.
Lastly, epidermal thickness was assessed using RCM. The images with cellular resolution allow very detailed measurements of the epidermal layer [27]. Earlier work showed very good correspondence of RCM and histology for epidermal thickness measurements [34]. Limitations for use in daily practice are the high device cost and limited imaging depth, as imaging resolution decreases substantially below 150 µm (superficial dermis). In addition, measuring facial skin may be challenging. The transition from epidermis to dermis differs from other anatomical locations; in facial skin, interpapillary processes do not or barely exist due to sun exposure, and the dermal–epidermal junction is low refractive in skin types I/II because of limited melanin content in the basal layer [35,36]. Therefore, knowledge about skin morphology is recommended for evaluation of the images. Of all imaging tools, RCM is superior for noninvasive skin thickness measurements. Possible alternatives are high-frequency ultrasound, near-infrared spectroscopy, optical coherence tomography, or Raman spectroscopy; however, these devices have lower resolution and are also expensive [17,37,38,39]. Moreover, they may not all be suitable for facial imaging due to their size (e.g., Raman spectroscopy).
It is already known that the application of moisturizers increases SC thickness, probably due to the absorption of water (indicating increased water-binding capacity), corneocyte swelling, or reorganization in the lipid bilayer [15,40,41]. Surprisingly, we did not measure increased water content after cream application. Moreover, the RCM images showed no morphological changes of corneocytes in the SC after cream application. This suggests that increased SC thickness in our study may not be due to increased hydration or corneocyte swelling, but rather due to cream components other than water [24]. Alternatively, it could be that we did not find increased SC water content because water may have diffused into deeper layers of the epidermis in the 30 min after cream application, or it could be that repeated use of moisturizers is needed to significantly increase epidermal water content [14,15,40,42,43,44].
Given the explorative design, our study consisted of a small number of young volunteers with female predominance. It would be interesting to investigate our method with prolonged use of topical creams in a larger population, at various facial locations and to include an untreated reference area. Moreover, measurements in subjects after controlled skin barrier perturbation (e.g. tape-stripping [21]) or in patients with disturbed skin barrier function could provide more insight into the effect of cream application. It would also be interesting to expand our method with other skin-barrier-related parameters (sebum, pH).
In conclusion, we combined the noninvasive measurements of erythema, TEWL, water content, and epidermal thickness to assess the effect of different creams on the healthy facial skin barrier. Cream application did not affect erythema, TEWL, and water content, but did lead to increased SC thickness. Our multiparametric approach is promising and offers a feasible and practical way to quickly obtain multifaceted information about skin barrier function. Further exploration of this approach after prolonged use of cream and in conditions of disrupted skin barriers are recommended areas for future research.
Supplementary Materials
The following are available online at https://www.mdpi.com/2079-9284/6/1/20/s1: Figure S1: Protocol used for VivaStack evaluation to determine thickness of the stratum corneum (SC) and epidermis with reflectance confocal microscopy (adapted from Ardigo et al. [26]), with examples to distinguish the boundaries between the different skin layers. The central part of the images was used to determine the transition of the different skin layers, to rule out variation in depth (skin layers) within the images; Figure S2, Table S1: Differences in erythema, transepidermal water loss, water content, and skin thickness between baseline and 30 min after cream application per volunteer.
Author Contributions
Conceptualization, J.G.M.L. and P.E.J.v.E.; formal analysis, J.G.M.L. and J.I.O.; investigation, J.I.O.; methodology, J.G.M.L., J.I.O., and P.E.J.v.E.; project administration, J.G.M.L., W.W.-v.d.W., and P.E.J.v.E.; supervision, J.G.M.L., W.W.-v.d.W., and P.E.J.v.E.; validation, J.G.M.L., J.I.O., W.W.-v.d.W., and P.E.J.v.E.; visualization, J.G.M.L. and J.I.O.; writing—original draft, J.G.M.L. and J.I.O.; writing—review and editing, J.G.M.L., J.I.O., W.W.-v.d.W., and P.E.J.v.E.
Funding
This research received no external funding.
Conflicts of Interest
The authors declare no conflicts of interest.
Abbreviations
| FTU | Finger-tip unit |
| NMF | Natural moisturizing factor |
| RCM | Reflectance confocal microscope |
| SC | Stratum corneum |
| TEWL | Transepidermal water loss |
References
- Yousef, H.; Sharma, S. Anatomy, Skin (Integument), Epidermis. In StatPearls. Treasure Island (FL); StatPearls Publishing LLC.: St. Petersburg, FA, USA, 2018. [Google Scholar]
- Loden, M. Role of topical emollients and moisturizers in the treatment of dry skin barrier disorders. Am. J. Clin. Dermatol. 2003, 4, 771–788. [Google Scholar] [CrossRef] [PubMed]
- Rawlings, A.V.; Harding, C.R. Moisturization and skin barrier function. Dermatol. Ther. 2004, 17 (Suppl. 1), 43–48. [Google Scholar] [CrossRef] [PubMed]
- Addor, F.A. Skin barrier in rosacea. Anais Brasileiros de Dermatologia 2016, 91, 59–63. [Google Scholar] [CrossRef] [PubMed]
- Two, A.M.; Wu, W.; Gallo, R.L.; Hata, T.R. Rosacea: Part I. Introduction, categorization, histology, pathogenesis, and risk factors. J. Am. Acad. Dermatol. 2015, 72, 749–758. [Google Scholar] [CrossRef] [PubMed]
- Woo, Y.R.; Lim, J.H.; Cho, D.H.; Park, H.J. Rosacea: Molecular Mechanisms and Management of a Chronic Cutaneous Inflammatory Condition. Int. J. Mol. Sci. 2016, 17, 1562. [Google Scholar] [CrossRef] [PubMed]
- Addor, F.A.; Aoki, V. Skin barrier in atopic dermatitis. Anais Brasileiros de Dermatologia 2010, 85, 184–194. [Google Scholar] [CrossRef] [PubMed]
- Dirschka, T.; Tronnier, H.; Folster-Holst, R. Epithelial barrier function and atopic diathesis in rosacea and perioral dermatitis. Br. J. Dermatol. 2004, 150, 1136–1141. [Google Scholar] [CrossRef] [PubMed]
- Tsakok, T.; Woolf, R.; Smith, C.H.; Weidinger, S.; Flohr, C. Atopic dermatitis: The skin barrier and beyond. Br. J. Dermatol. 2019, 180, 464–474. [Google Scholar] [CrossRef] [PubMed]
- Elias, P.M. Primary role of barrier dysfunction in the pathogenesis of atopic dermatitis. Exp. Dermatol. 2018, 27, 847–851. [Google Scholar] [CrossRef] [PubMed]
- Levin, J.; Miller, R. A Guide to the Ingredients and Potential Benefits of Over-the-Counter Cleansers and Moisturizers for Rosacea Patients. J. Clin. Aesthet. Dermatol. 2011, 4, 31–49. [Google Scholar] [PubMed]
- Hon, K.L.; Kung, J.S.C.; Ng, W.G.G.; Leung, T.F. Emollient treatment of atopic dermatitis: Latest evidence and clinical considerations. Drugs Context 2018, 7, 212530. [Google Scholar] [CrossRef] [PubMed]
- Moss, J. The effect of 3 moisturisers on skin surface hydration: Electrical conductance (Skicon-200), capacitance (Corneometer CM420), and transepidermal water loss (TEWL). Skin Res. Technol. 1996, 2, 32–36. [Google Scholar] [CrossRef] [PubMed]
- Young, D.L.; Chakravarthy, D. A controlled laboratory comparison of 4 topical skin creams moisturizing capability on human subjects. J. Wound Ostomy Cont. Nurs. 2014, 41, 168–174. [Google Scholar] [CrossRef] [PubMed]
- Loden, M. Effect of moisturizers on epidermal barrier function. Clin. Dermatol. 2012, 30, 286–296. [Google Scholar] [CrossRef] [PubMed]
- Elias, P.M.; Wakefield, J.S.; Man, M.Q. Moisturizers versus Current and Next-Generation Barrier Repair Therapy for the Management of Atopic Dermatitis. Skin Pharmacol. Physiol. 2019, 32, 1–7. [Google Scholar] [CrossRef] [PubMed]
- van Erp, P.E.J.; Peppelman, M.; Falcone, D. Noninvasive analysis and minimally invasive in vivo experimental challenges of the skin barrier. Exp. Dermatol. 2018, 27, 867–875. [Google Scholar] [CrossRef] [PubMed]
- Fullerton, A.; Fischer, T.; Lahti, A.; Wilhelm, K.P.; Takiwaki, H.; Serup, J. Guidelines for measurement of skin colour and erythema. A report from the Standardization Group of the European Society of Contact Dermatitis. Contact Dermat. 1996, 35, 1–10. [Google Scholar] [CrossRef]
- Stamatas, G.N.; Zmudzka, B.Z.; Kollias, N.; Beer, J.Z. Non-invasive measurements of skin pigmentation in situ. Pigment Cell Res. 2004, 17, 618–626. [Google Scholar] [CrossRef] [PubMed]
- Imhof, R.E.; De Jesus, M.E.; Xiao, P.; Ciortea, L.I.; Berg, E.P. Closed-chamber transepidermal water loss measurement: Microclimate, calibration and performance. Int. J. Cosmet. Sci. 2009, 31, 97–118. [Google Scholar] [CrossRef] [PubMed]
- Alexander, H.; Brown, S.; Danby, S.; Flohr, C. Research Techniques Made Simple: Transepidermal Water Loss Measurement as a Research Tool. J. Investig. Dermatol. 2018, 138, 2295–3000.e1. [Google Scholar] [CrossRef] [PubMed]
- Pinnagoda, J.; Tupker, R.A.; Agner, T.; Serup, J. Guidelines for transepidermal water loss (TEWL) measurement. A report from the Standardization Group of the European Society of Contact Dermatitis. Contact Dermat. 1990, 22, 164–178. [Google Scholar] [CrossRef]
- Imhof, B. Stratum corneum hydration measurement using capacitance contact imaging. Presented at the COMET 2017, Cergy Pontoise, France, 6–7 June 2017. [Google Scholar]
- Zhang, X.; Bontozoglou, C.; Chirikhina, E.; Lane, M.; Xiao, P. Capacitive Imaging for Skin Characterizations and Solvent Penetration Measurements. Cosmetics 2018, 5, 52. [Google Scholar] [CrossRef]
- Logger, J.G.M.; Munchhoff, C.U.; Olydam, J.I.; Peppelman, M.; Van Erp, P.E.J. Anatomical site variation of water content in human skin measured by the Epsilon: A pilot study. Skin Res. Technol. 2019. [Google Scholar] [CrossRef] [PubMed]
- Ardigo, M.; Longo, C.; Gonzalez, S. Multicentre study on inflammatory skin diseases from The International Confocal Working Group: Specific confocal microscopy features and an algorithmic method of diagnosis. Br. J. Dermatol. 2016, 175, 364–374. [Google Scholar] [CrossRef] [PubMed]
- Levine, A.; Markowitz, O. Introduction to reflectance confocal microscopy and its use in clinical practice. JAAD Case Rep. 2018, 4, 1014–1023. [Google Scholar] [CrossRef] [PubMed]
- Finlay, A.Y.; Edwards, P.H.; Harding, K.G. “Fingertip unit” in dermatology. Lancet 1989, 2, 155. [Google Scholar] [CrossRef]
- Farahmand, S.; Tien, L.; Hui, X.; Maibach, H.I. Measuring transepidermal water loss: A comparative in vivo study of condenser-chamber, unventilated-chamber and open-chamber systems. Skin Res. Technol. 2009, 15, 392–398. [Google Scholar] [CrossRef] [PubMed]
- Voegeli, R.; Rawlings, A.V.; Seroul, P.; Summers, B. A novel continuous colour mapping approach for visualization of facial skin hydration and transepidermal water loss for four ethnic groups. Int. J. Cosmet. Sci. 2015, 37, 595–605. [Google Scholar] [CrossRef] [PubMed]
- Marrakchi, S.; Maibach, H.I. Biophysical parameters of skin: Map of human face, regional, and age-related differences. Contact Dermat. 2007, 57, 28–34. [Google Scholar] [CrossRef] [PubMed]
- Wa, C.V.; Maibach, H.I. Mapping the human face: Biophysical properties. Skin Res. Technol. 2010, 16, 38–54. [Google Scholar] [CrossRef] [PubMed]
- Tagami, H. Location-related differences in structure and function of the stratum corneum with special emphasis on those of the facial skin. Int. J. Cosmet. Sci. 2008, 30, 413–434. [Google Scholar] [CrossRef] [PubMed]
- Peppelman, M.; Wolberink, E.A.; Gerritsen, M.J.; van de Kerkhof, P.C.; van Erp, P.E. Application of leukotriene B4 and reflectance confocal microscopy as a noninvasive in vivo model to study the dynamics of skin inflammation. Skin Res. Technol. 2015, 21, 232–240. [Google Scholar] [CrossRef] [PubMed]
- Robertson, K.; Rees, J.L. Variation in epidermal morphology in human skin at different body sites as measured by reflectance confocal microscopy. Acta Derm. Venereol. 2010, 90, 368–373. [Google Scholar] [PubMed]
- Puig, S.C.C.; Lovato, L. Reflectance Confocal Microscopy for Skin Diseases; Springer: Berlin/Hedelberg, Germany, 2012. [Google Scholar]
- Van Mulder, T.J.; de Koeijer, M.; Theeten, H.; Willems, D.; Van Damme, P.; Demolder, M.; De Meyer, G.; Beyers, K.C.; Vankerckhoven, V. High frequency ultrasound to assess skin thickness in healthy adults. Vaccine 2017, 35, 1810–1815. [Google Scholar] [CrossRef] [PubMed]
- Miyamae, Y.; Kawabata, M.; Yamakawa, Y.; Tsuchiya, J.; Ozaki, Y. Non-Invasive Estimation of Skin Thickness by near Infrared Diffuse Reflection Spectroscopy—Separate Determination of Epidermis and Dermis Thickness. J. Near Infrared Spectrosc. 2012, 20, 617–622. [Google Scholar] [CrossRef]
- Pena, A.; Arronte, M.; De Posada, E.; Ponce, L.; Flores, T. Non-invasive optical method for epidermal thickness estimation. OnLine J. Biol. Sci. 2014, 14, 163–166. [Google Scholar]
- Crowther, J.M.; Sieg, A.; Blenkiron, P.; Marcott, C.; Matts, P.J.; Kaczvinsky, J.R.; Rawlings, A.V. Measuring the effects of topical moisturizers on changes in stratum corneum thickness, water gradients and hydration in vivo. Br. J. Dermatol. 2008, 159, 567–577. [Google Scholar] [PubMed]
- Manfredini, M.; Mazzaglia, G.; Ciardo, S.; Simonazzi, S.; Farnetani, F.; Longo, C.; Pellacani, G. Does skin hydration influence keratinocyte biology? In vivo evaluation of microscopic skin changes induced by moisturizers by means of reflectance confocal microscopy. Skin Res. Technol. 2013, 19, 299–307. [Google Scholar] [PubMed]
- Nolan, K.; Marmur, E. Moisturizers: Reality and the skin benefits. Dermatol. Ther. 2012, 25, 229–233. [Google Scholar] [CrossRef] [PubMed]
- Constantin, M.M.; Poenaru, E.; Poenaru, C.; Constantin, T. Skin Hydration Assessment through Modern Non-Invasive Bioengineering Technologies. Maedica (Buchar) 2014, 9, 33–38. [Google Scholar] [PubMed]
- Pierre, J.; Francois, G.; Benize, A.M.; Rubert, V.; Coutet, J.; Flament, F. Mapping, in vivo, the uniformity of two skin properties alongside the human face by a 3D virtual approach. Int. J. Cosmet. Sci. 2018, 40, 482–487. [Google Scholar] [CrossRef] [PubMed]
Figure 1.
Measurement locations for erythema, transepidermal water loss (TWLE), water content, and skin thickness per cheek.
Figure 1.
Measurement locations for erythema, transepidermal water loss (TWLE), water content, and skin thickness per cheek.

Figure 2.
Dermoscopic image of the cheek made using the reflectance confocal microscope. The red dots show the exact locations were the VivaStacks were performed.
Figure 2.
Dermoscopic image of the cheek made using the reflectance confocal microscope. The red dots show the exact locations were the VivaStacks were performed.

Figure 3.
Thickness of stratum corneum (A) and viable epidermis (B) measured by the reflectance confocal microscope at baseline and 30 min after cream application. Values are expressed as medians with interquartile ranges and ranges (minimum–maximum).
Figure 3.
Thickness of stratum corneum (A) and viable epidermis (B) measured by the reflectance confocal microscope at baseline and 30 min after cream application. Values are expressed as medians with interquartile ranges and ranges (minimum–maximum).

Figure 4.
Representative reflectance confocal microscopy images of the stratum corneum at baseline (A) and 30 min after cream application (B).
Figure 4.
Representative reflectance confocal microscopy images of the stratum corneum at baseline (A) and 30 min after cream application (B).


{kind=link}
{kind=link}
{kind=link}
{kind=link}
Table 1.
Ingredients of investigational products.
| Product | Ingredients (in Order of Percentage of Cream Content) |
|---|---|
| Lanette cream I FNA | Purified water, decyloleate, cetostearyl alcohol, B emulsifying, sorbitol solution, sorbic acid |
| Vaseline-Lanette cream FNA | Cetostearyl alcohol, B emulsifying, cetiol V, sorbic acid, sorbitol solution, white petrolatum (vaseline), purified water |
FNA: Formularium der Nederlandse Apothekers.
Table 2.
Overview of the four devices used for the skin barrier function measurements.
| Device Skin Parameter Assessed | Measurement Principle | Output | Measurement Time | References |
|---|---|---|---|---|
| Spectrophotometer (Konica CM-2600d) Erythema | Intense white light from a xenon lamp is emitted by a probe. The device is placed onto the skin. The color of the reflected light is analyzed by three photocells filtering the primary colors (blue: 450 nm, green: 550 nm, red: 610 nm). This allows measurement of the absorbance and reflectance spectrum in the 400–700-nm range. | Color expressed as L*a*b color space. This is a three-dimensional coordinate system with an L*axis (brightness) and two orthogonal axes representing chromaticity, namely a*axis (red-green) and b*axis (yellow-blue). The a* value from the measurement locations is obtained after repeated calibration on a white surface before each measuring session (0.00). | 1.5 s | [17,18,19] |
| Aquaflux (Biox) TEWL | A probe consisting of a closed chamber with a condenser and sensors for relative temperature and humidity is applied onto the skin surface. The flux of vapor is calculated due to increasing temperature and humidity rate. | Flux density of water vapor (g/m2/h). | Max. 180 s | [20,21,22] |
| Epsilon (Biox) Water content | A probe consisting of 76,800 sensors with a sensing area of 1.3 cm × 1.5 cm, a resolution of 50 µm, and a measurement depth of 20 µm is placed onto the skin. The electrical capacitance of the skin surface is calculated. | Calibrated dielectric permittivity (ε) through the SC. Moreover, capacitive contact images can be obtained (brighter color = higher dielectric constant; darker color = lower dielectric constant) for skin surface hydration mapping, taking skin relief and variable distribution of sweat glands into account. | 30 s | [23,24,25] |
| Reflectance Confocal Microscope (VivaScope 1500) Thickness of SC and epidermis | Laser light at 830 nm is focused onto the skin with maximum imaging depth of 200 µm below skin surface (papillary dermis). Due to different refractive indexes between the cell structures and the surrounding tissue, en face images at 30× magnification of morphological and cellular resolution are obtained. Horizontal resolution: 0.5–1 µm, vertical resolution: 3–5 µm. | Black and white images showing skin morphology. Options: - VivaCam: dermoscopic image. - Confocal: basic image of 500 µm × 500 µm. - VivaBlock: multiple confocals acquired at the same level, stitched together to create one larger image (max. 8 mm × 8 mm). - VivaStack: multiple confocals along depth at a certain location, with interval steps of 3–5 µm. - Movie: e.g., to view blood flow in the superficial dermis. | 2–3 min | [17,26,27] |
SC, stratum corneum; TEWL, transepidermal water loss.
Table 3.
Skin parameters measured at baseline and at 30 min after cream application.
| Skin Parameter | Lanette | Vaseline-Lanette | ||||
|---|---|---|---|---|---|---|
| Baseline | 30 min after cream application | p-Value | Baseline | 30 minafter cream application | p-Value | |
| Erythema (a*) | 48.40 (46.20–50.80) § | 48.00 (46.10–50.60) | 0.362 | 47.95 (44.60–49.80) | 48.05 (43.20–49.80) | 0.965 |
| TEWL (g/m2/h) | 19.28 (14.05–25.31) | 19.09 (15.87–26.71) | 0.363 | 18.81 (13.67–27.22) | 19.00 (14.61–24.54) | 0.300 |
| Water content (ε) | 20.16 (14.86–33.94) | 23.29 (15.89–28.33) | 0.730 | 21.11 (16.31–47.02) | 21.79 (14.03–40.02) | 0.363 |
| Thickness SC (µm) | 5.25 (3.71–7.42) | 9.90 (5.15–13.92) | 0.001 * | 4.64 (3.09–11.34) | 6.49 (4.12–9.90) | 0.016 * |
| Thickness viable epidermis (µm) | 54.59 (48.86–64.32) | 52.96 (45.61–60.61) | 0.551 | 54.22 (45.64–59.31) | 54.12 (42.26–57.91) | 0.638 |
§ Median (range). * p < 0.05 (baseline vs. 30 min after cream application).
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
MDPI and ACS Style
Logger, J.G.M.; Olydam, J.I.; Woliner-van der Weg, W.; van Erp, P.E.J. Noninvasive Skin Barrier Assessment: Multiparametric Approach and Pilot Study. Cosmetics 2019, 6, 20. https://doi.org/10.3390/cosmetics6010020
AMA Style
Logger JGM, Olydam JI, Woliner-van der Weg W, van Erp PEJ. Noninvasive Skin Barrier Assessment: Multiparametric Approach and Pilot Study. Cosmetics. 2019; 6(1):20. https://doi.org/10.3390/cosmetics6010020
Chicago/Turabian StyleLogger, Jade G. M., Jill I. Olydam, Wietske Woliner-van der Weg, and Piet E. J. van Erp. 2019. "Noninvasive Skin Barrier Assessment: Multiparametric Approach and Pilot Study" Cosmetics 6, no. 1: 20. https://doi.org/10.3390/cosmetics6010020
Note that from the first issue of 2016, this journal uses article numbers instead of page numbers. See further details here.