

Treatment of Melasma on Darker Skin Types: A Scoping Review

 ,
,  ,
,  and
and
Abstract
:1. Introduction
2. Methods and Materials
2.1. Overview
2.1.1. Identifying the Research Question
2.1.2. Identifying Appropriate Studies
- Evidence of facial melasma
- Evidence of facial melasma treatment interventions;
- Evidence of facial melasma prevalence;
- Evidence of facial melasma’s impact on quality of life.
2.1.3. Selecting Studies
2.1.4. Charting the Data
2.2. Quality Appraisal
2.3. Results Collection, Summarisation, and Reporting
2.4. Ethical Consideration
3. Results
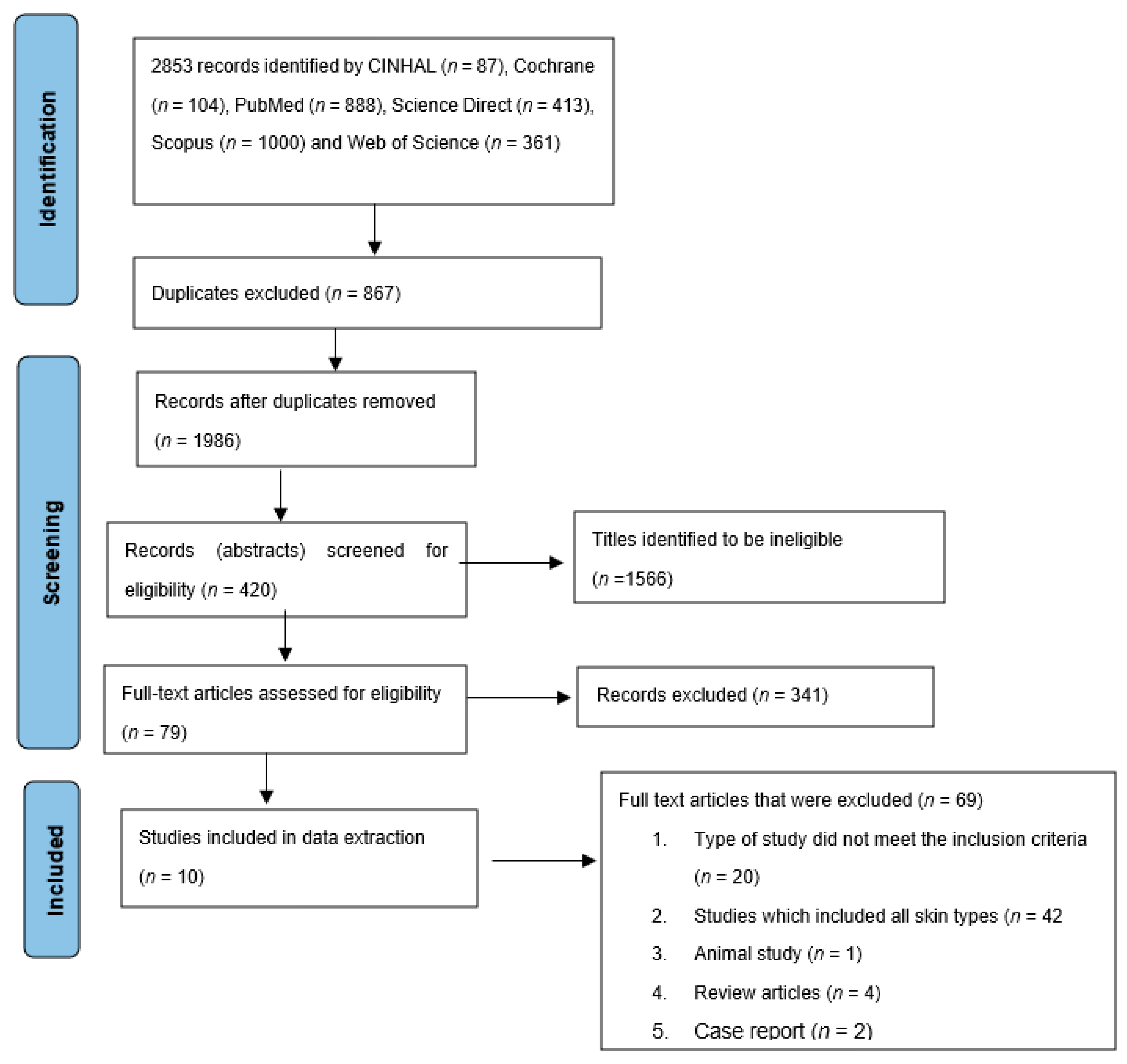
3.1. Screening Results
3.2. Characteristics of the Studies Included
3.3. The Level of Evidence
3.4. Main Findings
3.4.1. Topical Treatments
Azelaic acid (AZA) Cream
Retinol/Tretinoin
3.4.2. Chemical Peels
3.4.3. Lasers and Lights
3.4.4. Tranexamic Acid
4. Discussion
4.1. Topical Treatments
4.2. Chemical Peels
4.3. Lasers and Lights
4.4. Tranexamic Acid
4.5. Sun Protection
4.5.1. Implication for Research and Practice
4.5.2. Strengths and Limitations
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Vachiramon, V.; Iamsumang, W.; Chanasumon, N.; Thadanipon, K.; Triyangkulsri, K. A study of efficacy and safety of high-intensity focused ultrasound for the treatment of melasma in Asians: A single-blinded, randomized, split-face, pilot study. J. Cosmet. Dermatol. 2020, 19, 375–381. [Google Scholar] [CrossRef] [PubMed]
- Gupta, M.; Mahajan, V.K. Clinical profile of 300 men with facial hypermelanosis. J. Dermatol. Case Rep. 2017, 11, 20–24. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wanitphakdeedecha, R.; Sy-Alvarado, F.; Patthamalai, P.; Techapichetvanich, T.; Eimpunth, S.; Manuskiatti, W. The efficacy in treatment of facial melasma with thulium 1927-nm fractional laser-assisted topical tranexamic acid delivery: A split-face, double-blind, randomized controlled pilot study. Lasers Med. Sci. 2020, 35, 2015–2021. [Google Scholar] [CrossRef] [PubMed]
- Sarkar, R.; Ailawadi, P.; Garg, S. Melasma in men: A review of clinical, etiological, and management issues. J. Clin. Aesthet. Dermatol. 2018, 11, 53–59. [Google Scholar]
- Minni, K.; Poojary, S. Efficacy and safety of oral tranexamic acid as an adjuvant in Indian patients with melasma: A prospective, interventional, single-centre, triple-blind, randomized, placebo-control, parallel group study. J. Eur. Acad. Dermatol. Venereol. 2020, 34, 2636–2644. [Google Scholar] [CrossRef]
- Sarkar, R.; Garg, V.; Bansal, S.; Sethi, S.; Gupta, C. Comparative Evaluation of Efficacy and Tolerability of Glycolic Acid, Salicylic Mandelic Acid, and Phytic Acid Combination Peels in Melasma. Dermatol. Surg. 2016, 42, 384–391. [Google Scholar] [CrossRef]
- Khunger, N.; Sarkar, R.; Jain, R.K. Tretinoin peels versus glycolic acid peels in the treatment of Melasma in dark-skinned patients. Dermatol. Surg. 2004, 30, 756–760. [Google Scholar] [CrossRef]
- Saka, S.; Rao, G.R.R.; Komaram, R.B.; Kotha, S.; Tatavarthi, R.; Chitturi, L.P. Efficacy of 10% topical tranexamic acid in melasma—A randomized placebo-controlled split face study. Int. J. Pharm. Sci. Res. 2019, 10, 2583–2586. [Google Scholar] [CrossRef]
- Dlova, N.C.; Akintilo, L.O.; Taylor, S.C. Prevalence of pigmentary disorders: A cross-sectional study in public hospitals in Durban, South Africa. Int. J. Women’s Dermatol. 2019, 5, 345–348. [Google Scholar] [CrossRef]
- Soliman, M.M.; Ramadan, S.A.; Bassiouny, D.A.; Abdelmalek, M. Combined trichloroacetic acid peel and topical ascorbic acid versus trichloroacetic acid peel alone in the treatment of melasma: A comparative study. J. Cosmet. Dermatol. 2007, 6, 89–94. [Google Scholar] [CrossRef]
- Sharma, R.; Mahajan, V.K.; Mehta, K.S.; Chauhan, P.S.; Rawat, R.; Shiny, T.N. Therapeutic efficacy and safety of oral tranexamic acid and that of tranexamic acid local infiltration with microinjections in patients with melasma: A comparative study. Clin. Exp. Dermatol. 2017, 42, 728–734. [Google Scholar] [CrossRef] [PubMed]
- Regazetti, C.; Sormani, L.; Debayle, D.; Bernerd, F.; Tulic, M.K.; De Donatis, G.M.; Chignon-Sicard, B.; Rocchi, S.; Passeron, T. Melanocytes Sense Blue Light and Regulate Pigmentation through Opsin-3. J. Investig. Dermatol. 2018, 138, 171–178. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mpofana, N.; Chibi, B.; Gqaleni, N.; Mohammed, A.H.; Finlayson, A.J.; Kgarosi, K.; Dlova, N.C. The Prevalence and Treatment Options of Melasma as Well as its Association with Quality of Life in Darker Skin Types: A Scoping Review Protocol. Res. Square 2021, preprint. [Google Scholar] [CrossRef]
- Sarkar, R.; Kaur, C.; Bhalla, M.; Kanwar, A.J. The combination of glycolic acid peels with a topical regimen in the treatment of melasma in dark-skinned patients: A comparative study. Dermatol. Surg. 2002, 28, 828–832. [Google Scholar] [CrossRef] [PubMed]
- Mpofana, N.; Abrahamse, H. The Management of Melasma on Skin Types V and VI Using Light Emitting Diode Treatment. Photomed. Laser Surg. 2018, 36, 522–529. [Google Scholar] [CrossRef] [PubMed]
- Mpofana, N.; Abrahamse, H. Natural options for management of melasma, a review. J. Cosmet. Laser Ther. 2018, 20, 470–481. [Google Scholar] [CrossRef]
- Kwon, S.H.; Na, J.I.; Choi, J.Y.; Park, K.C. Melasma: Updates and perspectives. Exp. Dermatol. 2019, 28, 704–708. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Jiang, J.; Akinseye, O.; Tovar-Garza, A.; Pandya, A. The effect of melasma on self-esteem: A pilot study. Int. J. Women’s Dermatol. 2018, 4, 38–42. [Google Scholar] [CrossRef] [PubMed]
- Arora, P.; Meena, N.; Sharma, P.; Raihan, M. Impact of melasma on quality of life in Indian patients. Pigment Int. 2017, 4, 92. [Google Scholar] [CrossRef]
- Uyanikoglu, H.; Aksoy, M. Quality of life in patients with melasma in Turkish women. Dermatol. Rep. 2017, 9, 7340. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Pawaskar, M.D.; Parikh, P.; Markowski, T.; Mcmichael, A.J.; Feldman, S.R.; Balkrishnan, R. Melasma and its impact on health-related quality of life in Hispanic women. J. Dermatol. Treat. 2007, 18, 5–9. [Google Scholar] [CrossRef] [PubMed]
- Zhu, Y.; Zeng, X.; Ying, J.; Cai, Y.; Qiu, Y.; Xiang, W. Evaluating the quality of life among melasma patients using the MELASQoL scale: A systematic review and meta-analysis. PLoS ONE 2022, 17, e0262833. [Google Scholar] [CrossRef] [PubMed]
- Cestari, T.F.; Hexsel, D.; Viegas, M.L.; Azulay, L. Validation of a melasma quality of life questionnaire for Brazilian Portuguese language: The MelasQoL-BP study and improvement of QoL of melasma patients after triple combination therapy. Br. J. Dermatol. 2006, 156, 13–20. [Google Scholar] [CrossRef]
- Balkrishnan, R.; McMichael, A.; Camacho, F.; Saltzberg, F.; Housman, T.; Grummer, S.; Feldman, S.; Chren, M.M. Development and validation of a health-related quality of life instrument for women with melasma. Br. J. Dermatol. 2003, 149, 572–577. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ikino, J.K.; Nunes, D.H.; da Silva, V.P.M.; Fröde, T.S.; Sens, M.M. Melasma and assessment of the quality of life in Brazilian women. An. Bras. Dermatol. 2015, 90, 196–200. [Google Scholar] [CrossRef]
- Rafi, S.; Iftikhar, U.; Rani, Z.; Hussain, I. Comparison of efficacy and safety of topical hydroquinone 2% and oral tranexamic acid 500 mg in patients of melasma. J. Pak. Assoc. Dermatol. 2017, 27, 204–213. [Google Scholar]
- Elkamshoushi, A.M.; Romisy, D.; Omar, S.S. Oral tranexamic acid, hydroquinone 4% and low-fluence 1064 nm Q-switched Nd: YAG laser for mixed melasma: Clinical and dermoscopic evaluation. J. Cosmet. Dermatol. 2022, 21, 657–668. [Google Scholar] [CrossRef]
- Ranjkesh, M.; Azizifard, S.; Khosroshahi, N.G. Comparison of effects of 5% hydroquinone cream plus non-ablative fractional 1540 erbium YAG laser and 5% hydroquinone cream alone in the treatment of melasma. Med. J. Tabriz Univ. Med. Sci. 2021, 43, 29–34. [Google Scholar] [CrossRef]
- Sarkar, R.; Arsiwala, S.; Dubey, N.; Sonthalia, S.; Das, A.; Arya, L.; Gokhale, N.; Torsekar, R.G.; Somani, V.K.; Majid, I.; et al. Chemical peels in melasma: A review with consensus recommendations by Indian pigmentary expert group. Indian J. Dermatol. 2017, 62, 578. [Google Scholar] [CrossRef]
- Cheng, J.; Vashi, N.A. Chemical Peels in Ethnic Skin. In Dermatoanthropology of Ethnic Skin and Hair; Springer: Boston, MA, USA, 2017; pp. 437–448. [Google Scholar]
- Ahsan, U.; Uzair, M.; Aamir, H. Comparison of safety and efficacy of 20% salicylic acid with Jessner’s solution in chemical peeling for melasma in Asian skin. Our Dermatol. Online 2021, 2. [Google Scholar] [CrossRef]
- Sahu, P.; Dayal, S. Most worthwhile superficial chemical peel for melasma of skin of color: Authors’ experience of glycolic, trichloroacetic acid, and lactic peel. Dermatol. Ther. 2021, 34, e14693. [Google Scholar] [CrossRef] [PubMed]
- Dunbar, S.; Posnick, D.; Bloom, B.; Elias, C.; Zito, P.; Goldberg, D.J. Energy-based device treatment of melasma: An update and review of the literature. J. Cosmet. Laser Ther. 2017, 19, 2–12. [Google Scholar] [CrossRef] [PubMed]
- Kamal, T.; Iftikhar, U. Low-fluence Q-switched neodymium-doped yttrium aluminum garnet (1064nm) laser for the treatment of facial melasma in local population. J. Pak. Assoc. Dermatol. 2017, 27, 164–168. [Google Scholar]
- Lee, M.-C.; Lin, Y.-F.; Hu, S.; Huang, Y.-L.; Chang, S.-L.; Cheng, C.-Y.; Chang, C.-S. A split-face study: Comparison of picosecond alexandrite laser and Q-switched Nd: YAG laser in the treatment of melasma in Asians. Lasers Med. Sci. 2018, 33, 1733–1738. [Google Scholar] [CrossRef]
- Kaushik, S.B.; Alexis, A.F. Nonablative fractional laser resurfacing in skin of color: Evidence-based review. J. Clin. Aesthet. Dermatol. 2017, 10, 51–67. [Google Scholar] [PubMed]
- Chalermchai, T.; Rummaneethorn, P. Effects of a fractional picosecond 1,064 nm laser for the treatment of dermal and mixed type melasma. J. Cosmet. Laser Ther. 2018, 20, 134–139. [Google Scholar] [CrossRef]
- Micek, I.; Pawlaczyk, M.; Kroma, A.; Seraszek-Jaros, A.; Urbańska, M.; Gornowicz-Porowska, J. Treatment of melasma with a low-fluence 1064 nm Q-switched Nd: YAG laser: Laser toning in Caucasian women. Lasers Surg. Med. 2022, 54, 366–373. [Google Scholar] [CrossRef]
- Karrabi, M.; David, J.; Sahebkar, M. Clinical evaluation of efficacy, safety and tolerability of cysteamine 5% cream in comparison with modified Kligman’s formula in subjects with epidermal melasma: A randomized, double-blind clinical trial study. Skin Res. Technol. 2021, 27, 24–31. [Google Scholar] [CrossRef]
- Tahoun, A.I.; Mostafa, W.Z.; Amer, M.A. Dermoscopic evaluation of tranexamic acid versus Vitamin C, with microneedling in the treatment of melasma: A comparative, split-face, single-blinded study. J. Dermatol. Treat. 2021, 33, 1623–1629. [Google Scholar] [CrossRef]
- Ahramiyanpour, N.; Saki, N.; Akbari, Z.; Shamsi-Meymandi, S.; Amiri, R.; Heiran, A. Efficacy of topical cysteamine hydrochloride in treating melasma: A systematic review. J. Cosmet. Dermatol. 2021, 20, 3593–3602. [Google Scholar] [CrossRef]
- Cantelli, M.; Ferrillo, M.; Donnarumma, M.; Emanuele, E.; Fabbrocini, G. A new proprietary gel containing glabridin, andrographolide, and apolactoferrin improves the appearance of epidermal melasma in adult women: A 6-month pilot, uncontrolled open-label study. J. Cosmet. Dermatol. 2020, 19, 1395–1398. [Google Scholar] [CrossRef] [PubMed]
- Rendon, M.I.; Barkovic, S. Clinical Evaluation of a 4% Hydroquinone + 1% Retinol Treatment Regimen for Improving Melasma and Photodamage in Fitzpatrick Skin Types III–VI. J. Drugs Dermatol. 2016, 15, 1435–1441. [Google Scholar] [PubMed]
- Lueangarun, S.; Namboonlue, C.; Tempark, T. Postinflammatory and rebound hyperpigmentation as a complication after treatment efficacy of telangiectatic melasma with 585 nanometers Q-switched Nd: YAG laser and 4% hydroquinone cream in skin phototypes III-V. J. Cosmet. Dermatol. 2021, 20, 1700–1708. [Google Scholar] [CrossRef] [PubMed]
- Feng, X.; Su, H.; Xie, J. Efficacy and safety of tranexamic acid in the treatment of adult melasma: An updated meta-analysis of randomized controlled trials. J. Clin. Pharm. Ther. 2021, 46, 1263–1273. [Google Scholar] [CrossRef] [PubMed]
- Xing, M.; Wang, X.; Zhao, L.; Zhou, Z.; Liu, H.; Wang, B.; Cheng, A.; Zhang, S.; Gao, Y. Novel dissolving microneedles preparation for synergistic melasma therapy: Combined effects of tranexamic acid and licorice extract. Int. J. Pharm. 2021, 600, 120406. [Google Scholar] [CrossRef]
- El Hadidi, H.; Mosaad, R.; Ragab, N. The efficacy of oral vs different dilutions of intradermal tranexamic acid microinjections in melasma—A randomized clinical trial. Dermatol. Ther. 2021, 34, e14924. [Google Scholar] [CrossRef]
- Agamia, N.; Apalla, Z.; Salem, W.; Abdallah, W. A comparative study between oral tranexamic acid versus oral tranexamic acid and Q-switched Nd-YAG laser in melasma treatment: A clinical and dermoscopic evaluation. J. Dermatol. Treat. 2021, 32, 819–826. [Google Scholar] [CrossRef]
- Thibane, V.; Ndhlala, A.; Abdelgadir, H.; Finnie, J.; van Staden, J. The cosmetic potential of plants from the Eastern Cape Province traditionally used for skincare and beauty. S. Afr. J. Bot. 2019, 122, 475–483. [Google Scholar] [CrossRef]
- Langat, M.K.; Dlova, N.C.; Mulcahy-Ryan, L.E.; Schwikkard, S.L.; Opara, E.I.; Crouch, N.R.; Hiles, J.D.; Mulholland, D.A. The effect of isolates from Cassipourea flanaganii (Schinz) alston, a plant used as a skin lightning agent, on melanin production and tyrosinase inhibition. J. Ethnopharmacol. 2021, 264, 113272. [Google Scholar] [CrossRef]
- Madikizela, L.M.; Nkwentsha, N.; Mlunguza, N.Y.; Mdluli, P.S. Physicochemical characterization and In vitro evaluation of the sun protection factor of cosmetic products made from natural clay material. S. Afr. J. Chem. 2017, 70, 113–119. [Google Scholar] [CrossRef] [Green Version]
- Lima, P.; Dias, J.; Esposito, A.; Miot, L.; Miot, H. French maritime pine bark extract (pycnogenol) in association with triple combination cream for the treatment of facial melasma in women: A double-blind, randomized, placebo-controlled trial. J. Eur. Acad. Dermatol. Venereol. 2021, 35, 502–508. [Google Scholar] [CrossRef] [PubMed]
- Arksey, H.; O’Malley, L. Scoping studies: Towards a methodological framework. Int. J. Soc. Res. Methodol. 2005, 8, 19–32. [Google Scholar] [CrossRef] [Green Version]
- Peters, M.D.; Marnie, C.; Tricco, A.C.; Pollock, D.; Munn, Z.; Alexander, L.; McInerney, P.; Godfrey, C.M.; Khalil, H. Updated methodological guidance for the conduct of scoping reviews. JBI Evid. Synth. 2020, 18, 2119–2126. [Google Scholar] [CrossRef] [PubMed]
- Tricco, A.C.; Lillie, E.; Zarin, W.; O’Brien, K.K.; Colquhoun, H.; Levac, D.; Moher, D.; Peters, M.D.J.; Horsley, T.; Weeks, L.; et al. PRISMA extension for scoping reviews (PRISMA-ScR): Checklist and explanation. Ann. Int. Med. 2018, 169, 467–473. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Porta, M. A Dictionary of Epidemiology; Oxford University Press: Oxford, UK, 2014; ISBN 0199390045. [Google Scholar]
- Hong, Q.; Pluye, P.; Fàbregues, S.; Bartlett, G.; Boardman, F.; Cargo, M. Mixed Methods Appraisal Tool (MMAT), Version 2018. Available online: http://mixedmethodsappraisaltoolpublic.pbworks.com/w/page/127425845/Download%20the%20MMAT (accessed on 21 October 2021).
- Cohen, J. A coefficient of agreement for nominal scales. Educ. Psychol. Meas. 1960, 20, 37–46. [Google Scholar] [CrossRef]
- Sarkar, R.; Bhalla, M.; Kanwar, A.J. A comparative study of 20% azelaic acid cream monotherapy versus a sequential therapy in the treatment of melasma in dark-skinned patients. Dermatology 2002, 205, 249–254. [Google Scholar] [CrossRef] [PubMed]
- Kumari, R.; Thappa, D.M. Comparative study of trichloroacetic acid versus glycolic acid chemical peels in the treatment of melasma. Indian J. Dermatol. Venereol. Leprol. 2010, 76, 447. [Google Scholar] [CrossRef]
- Dev, T.; Sreenivas, V.K.; Sharma, V.; Sahni, K.; Bhari, N.; Sethuraman, G. A split-face randomized controlled trial comparing 1064 nm Q-switched Nd-YAG laser and modified Kligman’s formulation in darker skinned patients with melasma. Br. J. Dermatol. 2018, 179, 66. [Google Scholar] [CrossRef]
- Kimbrough-Green, C.K.; Griffiths, C.E.; Finkel, L.J.; Hamilton, T.A.; Bulengo-Ransby, S.M.; Ellis, C.N.; Voorhees, J.J. Topical retinoic acid (tretinoin) for melasma in black patients. A vehicle-controlled clinical trial. Arch. Dermatol. 1994, 130, 727–733. [Google Scholar] [CrossRef]
- Polnikorn, N.; Tanghetti, E. Treatment of refractory melasma in Asians with the picosecond alexandrite laser. Dermatol. Surg. 2020, 46, 1651–1656. [Google Scholar] [CrossRef]
- Chun, E.Y.; Lee, J.B.; Lee, K.H. Focal trichloroacetic acid peel method for benign pigmented lesions in dark-skinned patients. Dermatol. Surg. 2004, 30, 512–516. [Google Scholar] [CrossRef] [PubMed]
- Chen, Y.T.; Lin, E.T.; Chang, C.C.; Lin, B.S.; Chiang, H.M.; Huang, Y.H.; Lin, H.Y.; Wang, K.Y.; Chang, T.M. Efficacy and Safety Evaluation of Picosecond Alexandrite Laser with a Diffractive Lens Array for Treatment of Melasma in Asian Patients by VISIA Imaging System. Photobiomodulation Photomed. Laser Surg. 2019, 37, 559–566. [Google Scholar] [CrossRef] [PubMed]
- KrupaShankar, D.S.R.; Somani, V.K.; Kohli, M.; Sharad, J.; Ganjoo, A.; Kandhari, S.; Mysore, V.R.; Aurangabadkar, S.; Malakar, S.; Vedamurthy, M.; et al. A Cross-Sectional, Multicentric Clinico-Epidemiological Study of Melasma in India. Dermatol. Ther. 2014, 4, 71–81. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Abdel-Raouf Mohamed, H.; Ali Nasif, G.; Saad Abdel-Azim, E.; Abd El-Fatah Ahmed, M. Comparative study of fractional Erbium: YAG laser vs combined therapy with topical steroid as an adjuvant treatment in melasma. J. Cosmet. Dermatol. 2019, 18, 517–523. [Google Scholar] [CrossRef] [PubMed]
- Mahajan, R.; Kanwar, A.J.; Parsad, D.; Kumaran, M.S.; Sharma, R. Glycolic acid peels/azelaic acid 20% cream combination and low potency triple combination lead to similar reduction in melasma severity in ethnic skin: Results of a randomized controlled study. Indian J. Dermatol. 2015, 60, 147–152. [Google Scholar] [CrossRef]
- Nanda, S.; Grover, C.; Reddy, B.S. Efficacy of hydroquinone (2%) versus tretinoin (0.025%) as adjunct topical agents for chemical peeling in patients of melasma. Dermatol. Surg. 2004, 30, 385–388. [Google Scholar] [CrossRef]
- Nordlund, J.; Grimes, P.; Ortonne, J.P. The safety of hydroquinone. J. Eur. Acad. Dermatol. Venereol. 2006, 20, 781–787. [Google Scholar] [CrossRef]
- Bulengo-Ransby, S.M.; Griffiths, C.E.; Kimbrough-Green, C.K.; Finkel, L.J.; Hamilton, T.A.; Ellis, C.N.; Voorhees, J.J. Topical tretinoin (retinoic acid) therapy for hyperpigmented lesions caused by inflammation of the skin in black patients. N. Engl. J. Med. 1993, 328, 1438–1443. [Google Scholar] [CrossRef]
- Choi, J.E.; Lee, D.W.; Seo, S.H.; Ahn, H.H.; Kye, Y.C. Low-fluence Q-switched Nd:YAG laser for the treatment of melasma in Asian patients. J. Cosmet. Dermatol. 2018, 17, 1053–1058. [Google Scholar] [CrossRef]
- Garg, S.; Vashisht, K.R.; Makadia, S. A prospective randomized comparative study on 60 Indian patients of melasma, comparing pixel Q-switched NdYAG (1064 nm), super skin rejuvenation (540 nm) and ablative pixel erbium YAG (2940 nm) lasers, with a review of the literature. J. Cosmet. Laser Ther. 2019, 21, 297–307. [Google Scholar] [CrossRef]
- Tse, T.W.; Hui, E. Tranexamic acid: An important adjuvant in the treatment of melasma. J. Cosmet. Dermatol. 2013, 12, 57–66. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| Criteria | Determinants |
|---|---|
| Population | Darker-skin-type people (skin types IV–VI) with diagnosed epidermal, dermal, or mixed melasma. |
| Exposure | All types of treatment for melasma, e.g., self-applied topical interventions or combinations of topical interventions and oral interventions. |
| Outcome | (1) Was the treatment effective? (2) Was the treatment safe? (3) Reported toxicity or relapse. |
| Date of Search | Electronic Data base | Keywords searched | Number of publications retrieved |
|---|---|---|---|
| 12/10/21 | PubMed | ((“melanosis”[MeSH Terms] OR Melasma [Text Word] OR melanosis [Text Word] OR “skin pigmentation”[MeSH Terms] OR Skin Pigmentation [Text Word] OR dyschromia [Text Word] OR “hyperpigmentation”[MeSH Terms] OR hyperpigmentation [Text Word] OR Chloasma [Text Word] AND (humans[Filter])) AND ((“Quality of Life”[Mesh]) OR “Prevalence”[Mesh] OR “quality of life”[TW] OR prevalence[tw] OR “therapy”[Subheading] OR “therapeutics”[MeSH Terms] OR treatment[Text Word] AND (Fitzpatrick skin IV to VI[TW] OR Fitzpatrick skin IV—VI[TW] OR Fitzpatrick VI[TW] OR Fitzpatrick IV[TW] OR Black[TW] OR Indian[TW] OR “mixed ancestry”[TW] OR “darker skin type*”[TW] OR “African Continental Ancestry Group”[Mesh] OR “mixed race”[TW] | 888 |
| 15/10/21 | Scopus | melanosis OR Melasma OR “skin pigmentation” OR dyschromia OR hyperpigmentation OR Chloasma AND “Fitzpatrick skin IV to VI” OR “Fitzpatrick skin IV—VI” OR “Fitzpatrick VI” OR “Fitzpatrick IV” OR Black OR Indian OR “Mixed ancestry” OR “darker skin types” OR “African Continental Ancestry Group" OR “mixed race" AND “quality of life” OR prevalence OR therapy OR therapeutics OR treatment | 1000 |
| 15/10/21 | CINAHL | AB (melanosis OR Melasma OR “skin pigmentation" OR dyschromia OR hyperpigmentation OR Chloasma) AND AB (Black OR Indian OR “Mixed ancestry” OR “darker skin type*” OR “African Continental Ancestry Group” OR “mixed race”) AND AB (“quality of life” OR prevalence OR therapy OR therapeutics OR treatment) | 87 |
| 15/10/21 | ScienceDirect | (Melasma OR hyperpigmentation) AND (“quality of life” OR prevalence OR treatment) AND (“Mixed ancestry” OR “darker skin type) | 413 |
| 15/10/21 | Web of Science Core Collection | melanosis OR Melasma OR “skin pigmentation" OR dyschromia OR hyperpigmentation OR Chloasma (Topic) AND “Fitzpatrick skin IV to VI” OR “Fitzpatrick skin IV—VI” OR “Fitzpatrick VI” OR “Fitzpatrick IV” OR Black OR Indian OR “Mixed ancestry” OR “darker skin types” OR “African Continental Ancestry Group" OR “mixed race" (Topic) AND “quality of life" OR prevalence OR therapy OR therapeutics OR treatment (Topic) | 361 |
| 15/10/21 | Cochrane Library | melanosis OR Melasma OR “skin pigmentation" OR dyschromia OR hyperpigmentation OR Chloasma [in Title Abstract Keyword] AND “Fitzpatrick skin IV to VI” OR “Fitzpatrick skin IV—VI” OR “Fitzpatrick VI” OR “Fitzpatrick IV” OR Black OR Indian OR “Mixed ancestry” OR “darker skin types" OR “African Continental Ancestry Group" OR “mixed race" [in Title Abstract Keyword] AND “quality of life” OR prevalence OR therapy OR therapeutics OR treatment [in Title Abstract Keyword]—(Word variations have been searched) | 104 |
| Author (Year) | Title of the Study | Aim of the Study | Country | Study Design, N | Study Setting | Population and Ethnicity | Gender | Age | Skin Types |
|---|---|---|---|---|---|---|---|---|---|
| Chen 2019 [65] | Efficacy and Safety Evaluation of Picosecond Alexandrite Laser with a Diffractive Lens Array for Treatment of Melasma in Asian Patients by VISIA Imaging System | To evaluate the efficacy and safety of ps 755-nm alexandrite laser with a DLA-generating, laser-induced optical breakdown, which may be beneficial for melasma treatment. | China | Prospective, pilot study, 20 | Dermatology centre | Asian | Female (n= 20) | 27–55 | IV |
| Dev 2018 [61] | A Split Face Randomized Controlled Trial Comparing 1064 Nm Q-Switched Nd-YAG Laser and Modified Kligman’s Formulation in Patients with Melasma in Darker Skin. | To compare the efficacy and safety of QSNYL and Kingman’s TC in the treatment of melasma in Fitzpatrick skin types IV and V. More specifically, is QS Nd-YAG laser more efficacious than modified Kligman’s formulation in patients with melasma in darker skin types? | India | Split-face randomised controlled trial, 38 | Hospital | Indian | Female (n= 38) | 20–50 | IV–V |
| CHUN 2004 [64] | Focal Trichloroacetic Acid Peel Method for Benign Pigmented Lesions in Dark-Skinned Patients | To evaluate the clinical effects of focal TCA peel on pigmented lesions in dark-skinned patients. | Korea | Experimental, 20 | Hospital | Korean | Female and male (gender ratio not specified) | 24–73 | IV–V |
| Mpofana and Abrahamse 2018 [15] | The Management of Melasma on Skin Types V and VI Using Light Emitting Diode Treatment | This study investigated LED treatment for patients with melasma on darker skin types. | South Africa | Experimental, 60 | An aesthetic laser clinic at Life Hospital | Black, Indian, mixed ancestry | Female (n = 60) | 25–60 | V–VI |
| Polnikorn 2020 [63] | Treatment of Refractory Melasma in Asians with the Picosecond Alexandrite Laser | The ps alexandrite laser was studied in practice with the DLA and flat optic to treat melasma. | Thailand | Experimental, 60 | Hospital | Asian | Female (n = 60) | Not stated | IV–VI |
| Sarkar et al. 2016 [6] | Comparative Evaluation of Efficacy and Tolerability of Glycolic Acid, Salicylic Mandelic Acid, and Phytic Acid Combination Peels in Melasma | To compare the therapeutic efficacy and tolerability of GA (35%) versus SM acid (20% salicylic/10% mandelic acid) versus phytic combination peels in Indian patients with melasma. | India | Prospective, randomised, single-blinded, 90 | Outpatient clinic of Lok Nayak Hospital | Indian | Female (n = 61) and male (n = 11) | 18–60 | IV–V |
| Sarkar, 2002 [59] | A Comparative Study of 20% Azelaic Acid Cream Monotherapy versus a Sequential Therapy in the Treatment of Melasma in Dark-Skinned Patients | To evaluate the usefulness of a sequential therapy of potent topical steroids +20% AZA cream versus only 20% AZA cream in the treatment of melasma | India | Prospective, single-blind, right–left comparison pilot study, 40 | Not stated | Indian | Female (n = 25) and male (n = 5) | 21- 45 | IV–V |
| Kimbrough-green, 1994 [62] | Topical Retinoic Acid (Tretinoin) for Melasma in Black Patients. A Vehicle-Controlled Clinical Trial. | To investigate the efficacy of topical 0.1% all-trans-retinoic acid (tretinoin) in the treatment of melasma in Black patients. | United States | Randomised vehicle-controlled clinical trial, 30 | University medical centre | Black | Female (n = 29) and male (n = 1) | 44–67 | V–VI |
| Kumari and Thappa 2010 [60] | Comparative Study of Trichloroacetic Acid versus Glycolic Acid Chemical Peels in the Treatment of Melasma | To compare the therapeutic response of melasma in Indian women to GA 20–35% versus TCA 10–20% for chemical peeling. | India | Comparative study, 30 | Hospital | Indian | Female (n = 38) and male (n = 2) | 18 -53 | IV–VI |
| Sharma et al. 2017 [11] | Therapeutic Efficacy and Safety of Oral Tranexamic Acid and that of Tranexamic Acid Local Infiltration with Microinjections in Patients with Melasma: A Comparative Study | To ascertain the comparative efficacy of different routes of administration of TXA. | India | Randomised, comparative study, 100 | Dr RP Govt Medical College | Indian | Female (n = 92) and male (n = 8 | 18–55 | IV |
| Treatment Intervention (Author, Year) | Study Design | Skin Types | Tx Period | Outcome (s) | Follow-Up Period | Side Effects | Recurrences |
|---|---|---|---|---|---|---|---|
| Group A: 250 mg oral TXA twice daily. Group B: TXA intradermal microinjections 4 mg/mL once every 4 weeks. Sharma et al. 2017 [11]. | Randomised, comparative | IV | 12 weeks | Reduction in MASI 4, 8, and 12 weeks was 21.29 ± 17.24%, 53.32 ± 16.50%, and 77.96 ± 09.39%, respectively, in group A, and 18.27 ±15.34%, 51.32 ± 17.20%, and 79.00 ± 09.64% in group B. Comparison between pre- and post-treatment clinical photographs showed overall improvement in both groups | 24 weeks | Mild epigastric discomfort, hypomenorrhea, headache, and injection-site pain. | Two patients in group A had re-lapses at 24 weeks. |
| Group A: 35% GA, once every 2 weeks. Group B: 20% salicylic and 10% mandelic acid, once every 2 weeks. Group C: 50% phytic acid combination peel, once every 2 weeks. Sarkar et al. 2016 [6]. | Prospective, randomised, single-blinded | IV–V | 12 weeks | Reduction in MASI scoring after 12 weeks was 62.36% in GA group A, 60.98% in SM group B, and 44.71% in phytic acid group C. | 20 weeks | Mild cutaneous persistent erythema, superficial desquamation, post-peel hyperpigmentation, burning sensation, herpes simplex. | N/A |
| Group A: 20% AZA cream, twice-daily application to one half of the face for 24 weeks. Group B: 0.05% clobetasol propionate cream, applied for 8 weeks only and then to be followed by 20% AZA cream only for the next 16 weeks on the other half of the face. Sarkar, 2002 [59]. | Prospective, single-blind, right–left comparison pilot | IV–V | 24 weeks | At 4, 8, and 16 weeks, the lightening of melasma was significantly more marked on the side receiving the sequential therapy rather than the side receiving only 20% AZA cream (p < 0.001). However, at 24 weeks, although the difference was still significant (p = 0.0052), as many as 96.7 and 90% of patients of each group (sequential therapy and AZA) had good to excellent responses to treatment | 24 weeks | Atrophy, telangiectasia, burning, erythema itching, acneiform eruptions. | Three patients did not experience any changes. |
| Group A skin type V: twice-weekly LED 633 nm followed by an 830 nm treatment 2 days later. Group B skin type VI: twice-weekly LED 633 nm followed by an 830 nm treatment 2 days later. Mpofana and Abrahamse, 2018 [15]. | Experimental | V–VI | 12 weeks | Decreased MASI mean from 40.66% at baseline to 26.85%. Improved MHGS scores as shown by a p-value of 0.000 at a <0.05 level of significance. VISIA complexion analysis as well as histology images showed improvement of melasma. Response graded by patients as being “Excellent Response” | 36 weeks | N/A | N/A |
| Group A: two-week pre-peel program of daily application of 12% GA cream followed by 20–35% GA, then treated with graded concentrations of 20–35% GA. Group B: two-week pre-peel program of daily application of 0.1% tretinoin at night, followed by 10–20% TCA facial peel. Kumari and Thappa, 2010 [60]. | Comparative | IV–VI | 12 weeks | Reduction in MASI scoring after 12 weeks was by 79% (from 26.6 to 5.6) in GA group A and by 73% in TCA group B (from a mean MASI of 29.1 to 8.2) but this difference was not significant. Subjective response, as graded by the patient, showed good or very good response in 75% in the GA group and 65% in the TCA group. | Moderate to severe burning, erythema, post-peel cracking. | N/A | |
| Group A: 0.1% tretinoin cream application of “pea-sized” amount of cream and slowly increase the amount used every night to increase tolerance. Group B: identical-appearing, colour-matched vehicle cream, application of “pea-sized” amount of cream and slowly increase the amount used every night to increase tolerance. Kimbrough-Green [62]. | Randomised vehicle-controlled clinical trial | V–VI | 24 weeks | After 40 weeks, the average MASI score of the tretinoin-treated group decreased by 32%, from 15.0± 1.8 at baseline to 10.2 ± 2.0, compared with a 10% decrease from 15.5 ± 2.4 to 13.9 ± 2.7 in the vehicle group. Colourimetric analysis revealed an increase in L* in the tretinoin-treated group, from 45.5 ± 1.4 U at baseline to 48.7 ± 1.6 U at week 40, i.e., a lightening of 3.2 ± 0.9 U, compared with a change of 42.5 ± 1.6 to 42.8 ± 1.8 U in the vehicle-treated group, a lightening of 0.3 ± 0.9 U (p = 0.02). Histology produced an 8% decrease in epidermal pigmentation compared with a 55% increase with vehicle treatment (p = 0.0007). Dermal pigment decreased by 18% in the tretinoin-treated group and increased by 11% in the vehicle group. Significant increases in stratum corneum compaction and granular layer thickness were noted in the tretinoin vs the vehicle group after 40 weeks of treatment. | 40 weeks | Erythema, peeling, retinoid dermatitis. | N/A |
| Group A: QSNYL once every week. Group B: daily application of modified Kligman’s triple combination consisting of hydroquinone 4%, tretinoin 0.05%, and fluocinolone acetonide 0.01%. along with a broad-spectrum sunscreen. Dev, 2018 [61]. | Split-face randomised controlled trial | IV–V | 12 weeks | The mean baseline MI in groups A and B was 50.6 ± 5.9 and 49.9 ± 6.1, respectively. That significantly decreased to 48.3 ± 5.9 (p < 0.001) and 47.8 ± 5.4 (p < 0.01), and the mean baseline mMASI in group A and group B was 3.3 ± 1.9 and 3.3 ± 2.0, which decreased to 2.7 ± 1.5 (p < 0.05) and 2.3 ± 1.6, respectively, (p < 0.001) after 12 weeks. Photographic assessment showed an overall significant improvement of 17.3% (95 CI%: 6.7–27.9) in group A and 20.9% (95% CI: 10.2–31.6%) in group B at the end of 12 weeks of intervention. | 12 weeks | Group A developed acute urticaria, group B encountered erythema and telangiectasia. | All patients had a reappearance of pigmentation by the end of follow-up. |
| Group A: 10% to 50% TCA, low -potency topical corticosteroid (hydrocortisone lotion), antibiotic ointment. Group B: a focal TCA peel was performed every 4–8 weeks. Chun, 2004 [64]. | Experimental | IV–V | 12 weeks | Eleven of twenty (55%) patients with melasma experienced a good clinical response. Patient and physician satisfaction rates, recorded from interviews conducted 6 months after the last treatment, were absolutely and moderately satisfied with this therapy, respectively. | 24 weeks | Mild erythema, transient post-inflammatory hyperpigmentation occurred in two patients. | N/A |
| Ps 755 nm alexandrite laser with DLA. The pulse duration was 750 ps. An 8-mm spot size and fluence of 0.4 J/cm2 was used over the target area with 2 passes per treatment area and around 2000–2500 passes in total. The repetition rate was 10 Hz. Treatments were performed in 4- to 6-week intervals. Chen, 2019 [65]. | Prospective, pilot | IV | N/A | The mean MASI score of 20 patients was 9.4 ± 4.7 at baseline, which improved significantly to 6.9 ± 3.7 after 3 sessions of ps laser therapy (p< 0.001). The VISIA analysis showed improvement on the forehead, although only spots (p = 0.007) and porphyrins (p = 0.032) were markedly improved. In both malar regions, VISIA analysis showed significant improvement in UV spots (p = 0.044), brown spots (p = 0.017), and porphyrins (p = 0.02). | 24 weeks | Erythema (25%), pruritus (20%), and scaling (20%). One patient (5%) developed mild PIH. | N/A |
| Group A: flat optic cases were treated with the ps alexandrite laser flat optic, 1.02 to 1.5 J/cm2, 3 to 4 mm spot size x1 pass, treatments occurred every 2 weeks. Group B: ps alexandrite laser with DLA, 0.4 J/cm2, 8 mm spot size (230 micro beams) with 1 pass, treatments occurred every 2 weeks. Polnikorn, 2020 [63]. | Experimental | IV–VI | 12 weeks | MSI score for Group 1 was 8.63, which improved to an average score of 3.16 at the 6-month follow-up. The MSI score was 2.4 pre-treatment, 6.8 after the first month, and 1.2 (50% improvement) at 6 months. There was an average improvement of 57.2% (636.1%) seen in the flat optic group, which was statistically significant (p < 0.001, 2-tailed paired t-test). Group 2 had an average baseline MSI score of 6.22, which improved to an average of 1.48 at the 6-month follow-up. Subjects treated with the DLA had an average improvement of 75.7% (647.1%), which was statistically significant (p < 0.001, 2-tailed paired t-test). | 24 weeks | In Group 1, 3 cases (16%) developed darkening of melasma and macular hypopigmentation. Group 2, with DLA on the ps alexandrite laser, immediately after treatment, there was mild, transient erythema, and patients experienced a mild heating sensation. | At 6 months, there was a recurrence of melasma in 5% of the cases. Recurrence in 16% of the cases in the flat optic group and transient macular hyper-pigmentation in 21% of the cases. |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Mpofana, N.; Chibi, B.; Visser, T.; Paulse, M.; Finlayson, A.J.; Ghuman, S.; Gqaleni, N.; Hussein, A.A.; Dlova, N.C. Treatment of Melasma on Darker Skin Types: A Scoping Review. Cosmetics 2023, 10, 25. https://doi.org/10.3390/cosmetics10010025
Mpofana N, Chibi B, Visser T, Paulse M, Finlayson AJ, Ghuman S, Gqaleni N, Hussein AA, Dlova NC. Treatment of Melasma on Darker Skin Types: A Scoping Review. Cosmetics. 2023; 10(1):25. https://doi.org/10.3390/cosmetics10010025
Chicago/Turabian StyleMpofana, Nomakhosi, Buyisile Chibi, Tronel Visser, Michael Paulse, Avenal Jane Finlayson, Shanaz Ghuman, Nceba Gqaleni, Ahmed A. Hussein, and Ncoza Cordelia Dlova. 2023. "Treatment of Melasma on Darker Skin Types: A Scoping Review" Cosmetics 10, no. 1: 25. https://doi.org/10.3390/cosmetics10010025