
Quality of Life among Patients with Acute Coronary Syndromes Receiving Care from Public and Private Health Care Systems in Brazil

 , , , , ,
, , , , ,  ,
,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design and Locations
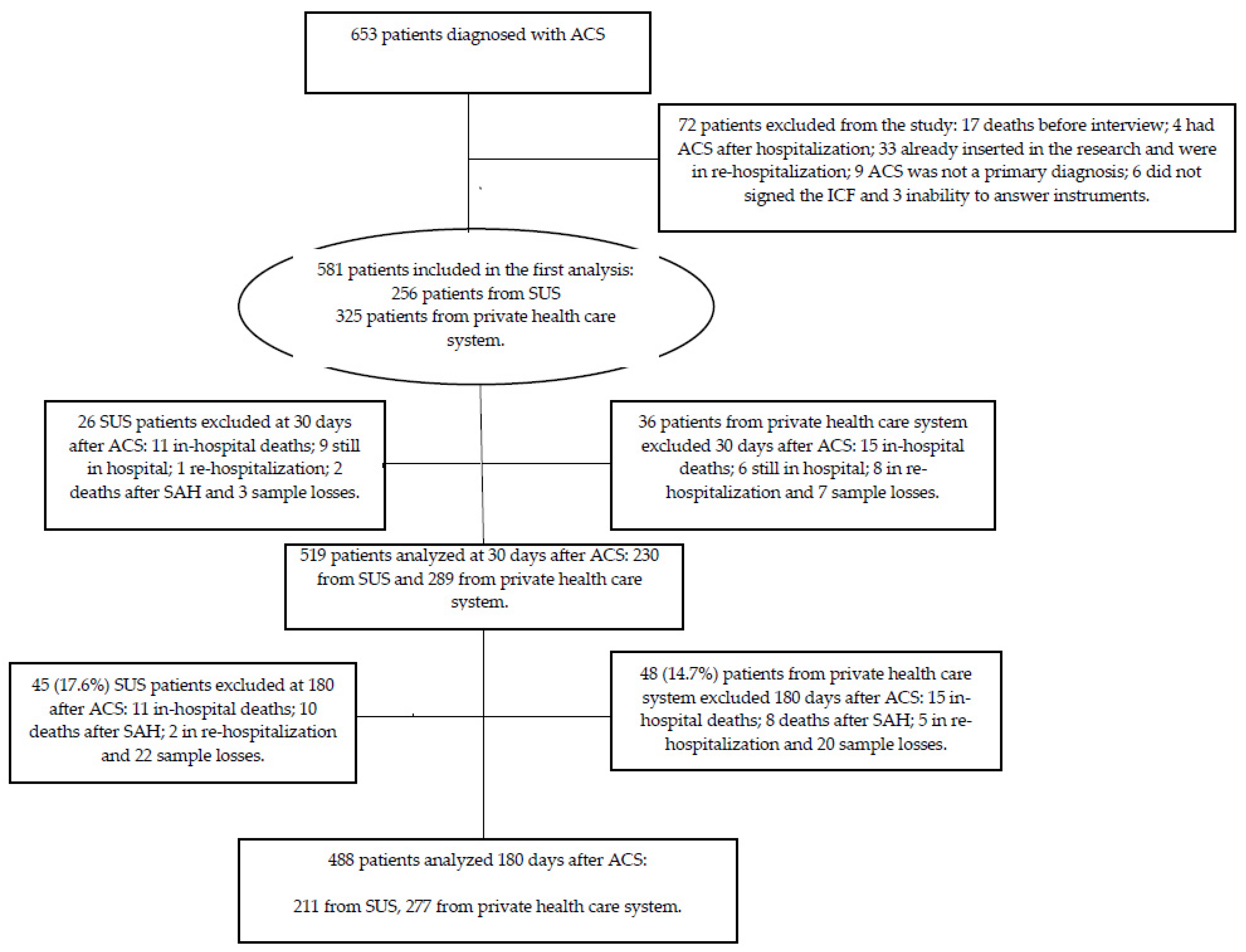
2.2. Study Sample
2.3. Data Collection
2.4. Data Analysis
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Conflicts of Interest
References
- Nicolau, J.C.; Feitosa-Filho, G.; Petriz, J.L.; Furtado, R.H.M.; Précoma, D.B.; Lemke, W.; Lopes, R.D.; Timerman, A.; Neto, J.A.M.; Neto, L.B.; et al. Brazilian Society of Cardiology Guidelines on Unstable Angina and Acute Myocardial Infarction without STSegment Elevation—2021. Arq. Bras. Cardiol. 2021, 117, 181–264. [Google Scholar] [CrossRef]
- Marasigan, V.; Perry, I.; Bennett, K.; Balanda, K.; Capewell, S.; Flaherty, M.O.; Kabir, Z. Explaining the fall in Coronary Heart Disease mortality in the Republic of Ireland between 2000 and 2015-IMPACT modelling study. Int. J. Cardiol. 2020, 310, 159–161. [Google Scholar] [CrossRef] [PubMed]
- Oliveira, J.C.; Oliveira, L.C.S.; Oliveira, J.C.; Barreto, I.D.D.C.; Almeida-Santos, M.A.; Lima, T.C.R.M.; Arcelino, L.A.M.; Silva, I.S.B.S.; Sousa, A.C.S.; Barreto-Filho, J.A.S. Disparidades no Uso de Stents Farmacológicos para Pacientes Diabéticos com Infarto Agudo do Miocárdio com Supradesnivelamento do Segmento ST Assistidos na Rede Pública versus Privada—Registro VICTIM. Arq. Bras. Cardiol. 2019, 112, 564–570. [Google Scholar] [CrossRef] [PubMed]
- Widimsky, P.; Crea, F.; Binder, R.K.; Lüscher, T.F. The year in cardiology 2018: Acute coronary Syndromes. Eur. Heart J. 2019, 40, 271–283. [Google Scholar] [CrossRef] [PubMed]
- Vallabhajosyula, S.; Dunlay, S.M.; Barsness, G.W.; Rihal, C.S.; Holmes-Junior, D.R.; Prasad, A. Hospital-level disparities in the outcomes of acute myocardial infarction with cardiogenic shock. Am. J. Cardiol. 2019, 124, 491–498. [Google Scholar] [CrossRef] [PubMed]
- Sakalaki, M.; Barywani, S.; Rosengren, A.; Bjorck, L.; Fu, M. Determinants of suboptimal long-term secondary prevention of acute myocardial infarction: The structural interview method and physical examinations. BMC Cardiovasc. Disord. 2019, 19, 243. [Google Scholar] [CrossRef]
- McDonagh, T.A.; Metra, M.; Adamo, M.; Gardner, R.S.; Baumbach, A.; Böhm, M.; Burri, H.; Butler, J.; Čelutkienė, J.; Chioncel, O.; et al. 2021 ESC Guidelines for the diagnosis and treatment of acute and chronic heart failure. European Association of Preventive Cardiology (EAPC). Eur. Heart J. 2021, 42, 3599–3726. [Google Scholar] [CrossRef]
- Lawton, J.S.; Tamis-Holland, J.E.; Bangalore, S.; Bates, E.R.; Beckie, T.M.; Bischoff, J.M.; Bittl, J.A.; Cohen, M.G.; DiMaio, J.M.; Don, C.W.; et al. 2021 ACC/AHA/SCAI guideline for coronary artery revascularization: A report of the American College of Cardiology/American Heart Association Joint Committee on Clinical Practice Guidelines. J. Am. Coll. Cardiol. 2021, 79, 21–129. [Google Scholar] [CrossRef]
- de Bakker, M.; Uijl, I.D.; ter Hoeve, N.; van Domburg, R.T.; Geleijnse, M.L.; Berg-Emons, R.J.V.D.; Boersma, E.; Sunamura, M. The Association between Exercise Capacity and Health-Related Quality of Life during and after Cardiac Rehabilitation in Acute Coronary Syndrome Patients: A substudy of the OPTICARE Randomized Controlled Trial. Arch. Phys. Med. Rehabil. 2020, 101, 650–657. [Google Scholar] [CrossRef]
- Soto, M.; Failde, I.; Márquez, S.; Benítez, E.; Ramos, I.; Barba, A.; López, F. Physical and mental component summaries score of the SF-36 in coronary patients. Qual. Life Res. 2005, 14, 759–768. [Google Scholar] [CrossRef]
- WHOQOL Group. The Development of the World Health Organization Quality of Life Assessment Instrument (the WHOQOL). In Quality of Life Assessment: International Perspectives; Springer: Berlin/Heidelberg, Germany, 1994; pp. 41–57. [Google Scholar]
- Ciconelli, M.R.; Bosi, M.; Santos, W.; Meinão, I.; Rodrigues, M. Tradução para língua portuguesa e validação do questionário genérico de avalição de qualidade de vida SF-36 (Brasil SF-36). Rev. Bras. Reumatol. 1999, 39, 143–150. [Google Scholar]
- Pirhonen, L.; Bolin, K.; Olofsson, E.H.; Fors, A.; Ekman, I.; Swedberg, K.; Gyllensten, H. Person-Centred Care in Patients with Acute Coronary Syndrome: Cost-Effectiveness Analysis Alongside a Randomised Controlled Trial. Pharm. Econ. Open. 2019, 3, 495–504. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Brazil Services and Information. Adequação Do Atendimento Pode Reduzir Mortes Por Infarto. Portal Brasil. Abril de 2012. Available online: http://www.brasil.gov.br/saude/2012/04/adequacao-do-atendimento-pode-reduzir-mortes-por-infarto (accessed on 8 November 2017).
- Brasil. Sistema Único de Saúde (SUS). Portal Ministério da Saúde. Janeiro de 2018. Available online: http://www.portalms.saude.gov.br/sistema-unico-de-saude/sistema-unico-de-saude (accessed on 3 January 2017).
- Costa, I.M.N.B.D.C.; da Silva, D.G.; Filho, J.A.S.B.; Oliveira, J.L.M.; Silva, J.R.S.; Buarque, M.D.B.M.; Nascimento, T.; Jorge, J.D.G.; Almeida, A.S.; Almeida-Santos, M.A.; et al. Diet quality of patients with acute coronary syndrome receiving public and private health care. Nutrition 2019, 59, 131–137. [Google Scholar] [CrossRef] [PubMed]
- Smolderen, K.; Spertus, J.A.; Tang, F.; Oetgen, W.; Borden, W.B.; Ting, H.H.; Chan, P.S. Treatment differences by health insurance among outpatients with coronary artery disease: Insights from the national cardiovascular data registry. J. Am. Coll. Cardiol. 2013, 61, 1069–1075. [Google Scholar] [CrossRef] [Green Version]
- Pons, A.; Whalley, G.; Sneddon, K.; Williams, M.; Coffey, S. Predictors of quality of life after revascularization for ischemic heart disease: A systematic review. Health Sci. Rev. 2022, 2, 100017. [Google Scholar] [CrossRef]
- Malta, M.; Cardoso, L.O.; Bastos, F.I.; Magnanini, M.M.F.; Silva, C.M.F.P. Iniciativa STROBE: Subsídios para a comunicação de estudos observacionais. Rev. Saúde Pública 2010, 44, 559–565. [Google Scholar] [CrossRef] [Green Version]
- Eisen, A.; Giugliano, R.; Braunwald, E. Updates on Acute Coronary Syndrome. JAMA Cardiol. 2016, 1, 718–730. [Google Scholar] [CrossRef]
- Committee IPAQR. Guidelines for Data Processing and Analysis of the International Physical Activity Questionnaire (IPAQ). Retrieved 15 November 2005. 2010. Available online: https://www.ipaq.ki.se/scoring.pdf (accessed on 14 May 2014).
- Matsudo, S.; Araújo, T.; Marsudo, V.; Andrade, D.; Andrade, E.; Braggion, G. Questionário Internacional de Atividade Física (IPAQ): Estudo de validade e reprodutibilidade no Brasil. Rev. Bras. Ativid. Fís. Saúde 2001, 6, 5–12. [Google Scholar] [CrossRef]
- Slater, B.; Philippi, S.T.; Marchioni, D.M.; Fisberg, R.M. Validação de Questionários de Freqüência Alimentar-QFA: Considerações metodológicas. Rev. Bras. Epidemiol. 2003, 6, 200–208. [Google Scholar] [CrossRef] [Green Version]
- Chiuve, S.E.; Fung, T.T.; Rimm, E.B.; Hu, F.B.; McCullough, M.L.; Wang, M.; Stampfer, M.J.; Willett, W.C. Alternative dietary indices both strongly predict risk of chronic disease. J. Nutr. 2012, 142, 1009–18222. [Google Scholar] [CrossRef] [Green Version]
- Ministério da Saúde. Guia Alimentar Para a População Brasileira: Promovendo a Alimentação Saudável; Ministério da Saúde: Brasília, Brazil, 2006. Available online: https://bvsms.saude.gov.br/bvs/publicacoes/guia_alimentar_populacao_brasileira_2008.pdf (accessed on 8 November 2016).
- ABEP. Associação Brasileira de Empresa e Pesquisa. CCEB. Critério de Classificação Econômica Brasil. 2008. Available online: http://www.abep.org.br (accessed on 17 June 2022).
- Ware, J.E., Jr.; Sherbourne, C.D. The MOS 36-item short-form health survey (SF-36): I. Conceptual framework and item selection. Med. Care 1992, 30, 473–483. [Google Scholar] [CrossRef]
- Weinberger, M.; Oddone, E.Z.; Samsa, G.P.; Landsman, P.B. Are health-related quality-of-life measures affected by the mode of administration? J. Clin. Epidemiol. 1996, 49, 135–140. [Google Scholar] [CrossRef]
- Almeida, R.M. Remodelamento reverso cirúrgico do ventrículo esquerdo: Seguimento de 111 meses. Rev. Bras. Cirurg. Cardiovasc. 2009, 24, 470–477. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- World Health Organization—WHO. Obesity: Preventing and Managing the Global Epidemic: Report of a WHO Consultation; World Health Organization: Geneva, Switzerland, 2000. [Google Scholar]
- Jalali-Farahani, S.; Amiri, P.; Fakhredin, H.; Torshizi, K.; Cheraghi, L.; Khalili, D.; Azizi, F. Health-related quality of life in men and women who experienced cardiovascular diseases: Tehran Lipid and Glucose Study. Health Qual. Life Outcomes 2021, 19, 225–234. [Google Scholar] [CrossRef]
- Olomu, A.B.; Corser, W.D.; Stommel, M.; Xie, Y.; Holmes-Rovner, M. Do self-report and medical record comorbidity data predict longitudinal functional capacity and quality of life health outcomes similarly? BMC Health Serv. Res. 2012, 12, 398. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mujica-Mota, R.E.; Roberts, M.; Abel, G.; Elliott, M.; Lyratzopoulos, G.; Roland, M.; Campbell, J. Common patterns of morbidity and multi-morbidity and their impact on health-related quality of life: Evidence from a national survey. Qual. Life Res. 2015, 24, 909–918. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Schulman-Marcus, J.; Boden, W.E. A PROMISE Fulfilled That Quality-of-Life Assessments Afford Incremental Value to Coronary Artery Disease Management. Circulation 2016, 133, 1989–1991. [Google Scholar] [CrossRef] [Green Version]
- Adriaanse, M.C.; Drewes, H.W.; van der Heide, I.; Struijs, J.N.; Baan, C.A. The impact of comorbid chronic conditions on quality of life in type 2 diabetes patients. Qual. Life Res. 2016, 25, 175–182. [Google Scholar] [CrossRef] [Green Version]
- Kang, K.; Gholizadeh, L.; Han, H.R. Health-related Quality of Life and Its Predictors in Korean Patients with Myocardial Infarction in the Acute Phase. Clin. Nurs. Res. 2021, 30, 161–170. [Google Scholar] [CrossRef]
- Herdy, A.H.; López-Jiménez, F.; Terzic, C.; Milani, M.; Stein, R.; Carvalho, T.; Serra, S.; Araujo, C.G.; Zeballos, P.C.; Anchique, C.V.; et al. Diretriz sul-americana de prevenção e reabilitação cardiovascular. Arq. Bras. Cardiol. 2014, 103, 1–31. [Google Scholar]
- Desai, N.R.; Choudhry, N.K. Impediments to adherence to post myocardial infarction medications. Curr. Cardiol. Rep. 2013, 15, 322. [Google Scholar] [CrossRef] [PubMed]
- Anderson, L.; Oldridge, N.; Thompson, D.R.; Zwisler, A.-D.; Rees, K.; Martin, N.; Taylor, R.S. Exercise-based cardiac rehabilitation for coronary heart disease: Cochrane systematic review and meta-analysis. J. Am. Coll. Cardiol. 2016, 67, 1–12. [Google Scholar] [CrossRef] [PubMed] [Green Version]


{kind=link}
| Categorical Variables | Valid Patients | Type of Healthcare | p | |
|---|---|---|---|---|
| SUS (%) | PHCS (%) | |||
| Age Group (years) from 18 to 49 from 50 to59 from 60 to 69 from 70 to79 ≥80 | 581 | 51 (19.9) 68 (26.6) 88 (34.4) 38 (14.8) 11 (4.3) | 24 (7.4) 76 (23.4) 109 (33.5) 70 (21.5) 46 (14.2) | <0.001 |
| Sex Male | 581 | 181 (70.7) | 189 (58.2) | 0.002 |
| Schooling (years) No schooling or <1 year from 1 to 3 from 4 to 8 9 years or more | 581 | 32 (12.5) 64 (25.0) 99 (38.7) 61 (23.8) | 12 (3.7) 20 (6.1) 79 (24.3) 214 (65.9) | <0.001 |
| Family income Per Capita (Minimum Wage) ≤1 >1 and ≤3 >3 ≤5 >5 | 576 | 196 (76.9) 54 (21.1) 3 (1.2) 2 (0.8) | 52 (16.2) 162 (50.5) 47 (14.6) 60 (18.7) | <0.001 |
| ABEP Classification Class A Classes B1 and B2 Class C1 and C2 Classes D–E | 50 179 207 145 | 3 (1.17) 26 (10.16) 101 (39.45) 126 (49.22) | 47 (14.46) 153 (47.08) 106 (32.62) 19 (5.85) | <0.001 |
| ACS Classification UA NSTEMI STEMI | 581 | 20 (7.8) 47 (18.4) 189 (73.8) | 81 (24.9) 166 (51.1) 78 (24.0) | <0.001 |
| Systemic Arterial Hypertension | 581 | 194 (75.8) | 270 (83.1) | 0.037 |
| Diabetes Mellitus | 581 | 76 (29.7) | 132 (40.6) | 0.008 |
| Dyslipidemia | 581 | 104 (40.6) | 218 (67.1) | <0.001 |
| Overweight | 576 | 153 (60.5) | 237 (73.4) | 0.001 |
| Abdominal Obesity | 568 | 171 (68.1) | 257 (81.1) | <0.001 |
| Sedentary lifestyle | 581 | 131 (51.2) | 180 (55.4) | 0.353 |
| Alcoholism | 581 | 39 (15.2) | 31 (9.5) | 0.049 |
| Smoking No Yes Ex-smoker | 581 | 100 (39.1) 63 (24.6) 93 (36.3) | 168 (51.7) 36 (11.1) 121 (37.2) | <0.001 |
| Cardiovascular outcomes at 180 days after ACS3 Acute Coronary Syndrome Stroke Congestive heart failure Cardiac Arrest | 581 | 45 (17.6) 32 (12.5) 5 (2.0) 7 (2.7) 1 (0.4) | 54 (16.6) 36 (11.1) 4 (1.2) 8 (2.5) 6 (1.8) | 0.845 0.689 0.516 0.987 0.141 |
| Adherence to Physical Activity at 180 days after ACS Sedentary Active | 488 | 133 (63.0) 78 (37.0) | 147 (53.1) 130 (46.9) | 0.034 |
| Adherence to pharmacotherapy at 180 days after ACS No Yes | 488 | 88 (41.7) 123 (58.3) | 73 (26.4) 204 (73.6) | 0.001 |
| Smoking Cessation Yes No | 488 | 14 (6.6) 197 (93.4) | 11 (4.0) 266 (96.0) | 0.264 |
| Diet Quality at 180 days after ACS A | 488 | 47.79 (7.90) | 53.71 (8.98) | <0.001 |
| Hospitalization Time (days)A | 581 | 11.44 (11.6) | 9.42 (10.6) | <0.001 |
| SF–36 Domains | Hospitalization | 30 Days after ACS | 180 Days after ACS | p D | |||
|---|---|---|---|---|---|---|---|
| Mean | SD | Mean | SD | Mean | SD | ||
| Functional Capacity | 54.1 A | 32.0 | 36.9 C | 23.4 | 49.5 B | 25.0 | <0.001 |
| Physical Aspect | 41.3 A | 42.5 | 4.5 B | 11.0 | 40.4 A | 36.6 | <0.001 |
| Pain | 47.7 B | 30.0 | 40.3 C | 19.2 | 63.0 A | 14.8 | <0.001 |
| General Health Status | 57.3 A | 22.3 | 53.0 C | 19.1 | 54.8 B | 17.5 | 0.002 |
| Vitality | 59.9 A | 24.3 | 53.9 B | 17.6 | 62.4 A | 13.3 | <0.001 |
| Social Aspect | 67.8 B | 29.0 | 57.4 C | 19.8 | 79.9 A | 17.0 | <0.001 |
| Emotional Aspect | 59.8 C | 44.2 | 64.0 B | 40.7 | 83.6 A | 30.1 | <0.001 |
| Mental Health | 68.2 A | 22.5 | 64.7 B | 17.3 | 69.9 A | 12.7 | <0.001 |
| SF–36 Domains | Time of Evaluation | Type of Healthcare | p | |
|---|---|---|---|---|
| SUS Mean (±SD) | PCHS Mean (±SD) | |||
| Functional Capacity | Hospitalization 30 days after ACS 180 days after ACS | 54.5 (32.2) 35.2 (22.5) 46.8 (23.8) | 53.7 (32.7) 38.2 (24.0) 51.6 (25.7) | 0.781 0.130 0.021 |
| Physical Aspect | Hospitalization 30 days after ACS 180 days after ACS | 40.5 (41.7) 2.7 (9.4) 31.5 (32.9) | 41.9 (43.2) 6.0 (12.0) 47.2 (37.8) | 0.871 <0.001 <0.001 |
| Pain | Hospitalization 30 days after ACS 180 days after ACS | 45.8 (32.0) 36.4 (18.2) 58.4 (13.9) | 49.2 (28.3) 43.4 (19.4) 66.5 (14.4) | 0.074 <0.001 <0.001 |
| General Health Status | Hospitalization 30 days after ACS 180 days after ACS | 56.9 (23.1) 52.0 (18.9) 53.0 (17.1) | 57.6 (21.7) 53.7 (19.2) 56.2 (17.7) | 0.778 0.310 0.043 |
| Vitality | Hospitalization 30 days after ACS 180 days after ACS | 61.8 (24.6) 54.2 (6.4) 60.6 (12.4) | 58.5 (23.9) 54.0 (18.5) 63.8 (13.8) | 0.102 0.971 <0.001 |
| Social Aspect | Hospitalization 30 days after ACS 180 days after ACS | 70.1 (28.9) 56.9 (18.9) 78.5 (16.2) | 65.9 (29.0) 57.9 (20.6) 81.0 (17.5) | 0.062 0.362 0.022 |
| Emotional Aspect | Hospitalization 30 days after ACS 180 days after ACS | 53.5 (45.3) 60.0 (41.7) 80.4 (32.0) | 64.7 (42.6) 67.1 (39.6) 86.0 (28.3) | 0.003 0.064 0.027 |
| Mental Health | Hospitalization 30 days after ACS 180 days after ACS | 70.4 (22.5) 64.8 (17.0) 68.5 (13.2) | 66.6 (22.4) 64.6 (17.5) 71.0 (12.1) | 0.023 0.919 0.033 |
| Time of Evaluation | Variables | Type of Healthcare | p | |
|---|---|---|---|---|
| SUS (%) | PHCS (%) | |||
| Hospitalization | Much better | 37 (14.5) | 36 (11.1) | 0.111 |
| A little better | 50 (19.5) | 45 (13.8) | ||
| Almost the same | 67 (26.2) | 108 (33.2) | ||
| A little worse | 79 (30.9) | 112 (34.5) | ||
| Much worse | 23 (9.0) | 24 (7.4) | ||
| 30 Days after ACS | Much better | - | - | 0.014 |
| A little better | 3 (1.03) | 17 (5.9) | ||
| Almost the same | 106 (46.1) | 147 (50.9) | ||
| A little worse | 113 (49.1) | 118 (40.8) | ||
| Much worse | 8 (3.5) | 7 (2.4) | ||
| 180 Days after ACS | Much better | - | - | 0.008 |
| A little better | 19 (9.0) | 31 (11.2) | ||
| Almost the same | 92 (43.6) | 156 (56.3) | ||
| A little worse | 92 (43.6) | 85 (30.7) | ||
| Much worse | 8 (3.8) | 5 (1.8) | ||
| FUNCTIONAL CAPACITY (r2 = 0.50) | ||||
| Variables | β | CI (95%) | Standard Error | p |
| Hospitalization time in days (Log) | −2.31 | −4.55; −0.07 | 1.14 | 0.043 |
| Age (years) | −0.57 | −0.73; −0.41 | 0.08 | <0.001 |
| Male Sex | 15.97 | 12.35; 19.59 | 1.84 | <0.001 |
| Schooling (years) | 0.22 | −0.20; 0.65 | 0.22 | 0.301 |
| Private Health Care System | 7.22 | 2.95; 11.50 | 2.17 | 0.001 |
| Systemic Arterial Hypertension | −7.01 | −11.41; −2.61 | 2.24 | 0.002 |
| Diabetes Mellitus | −2.71 | −6.37; 0.94 | 1.86 | 0.146 |
| Dyslipidemia | −0.04 | −3.60; 3.52 | 1.81 | 0.983 |
| Overweight | 0.97 | −3.79; 5.72 | 2.42 | 0.690 |
| Abdominal Obesity | −0.25 | −5.37; 4.86 | 2.60 | 0.922 |
| Cardiovascular Event | −9.30 | −14.65; −3.95 | 2.72 | 0.001 |
| Adherence to Physical Activity | 19.68 | 16.20; 23.17 | 1.78 | <0.001 |
| Adherence to Diet | 0.91 | −2.45; 4.27 | 1.71 | 0.595 |
| Adherence to Medication | 0.64 | −3.00; 4.29 | 1.85 | 0.729 |
| Smoking | 1.85 | −5.75; 9.45 | 3.87 | 0.633 |
| PHYSICAL ASPECT (r2 = 0.34) | ||||
| Variables | β | CI (95%) | Standard Error | p |
| Hospitalization time in days (Log) | −5.71 | −9.41; −2.01 | 1.88 | 0.003 |
| Age (years) | −0.21 | −0.47; 0.06 | 0.14 | 0.124 |
| Male Sex | 14.36 | 8.37; 20.34 | 3.05 | <0.001 |
| Schooling (years) | 1.25 | 0.55; 1.96 | 0.36 | 0.001 |
| Private Health Care System | 10.10 | 3.04; 17.16 | 3.59 | 0.005 |
| Systemic Arterial Hypertension | −8.67 | −15.94; −1.39 | 3.70 | 0.020 |
| Diabetes Mellitus | −3.24 | −9.28; 2.81 | 3.08 | 0.293 |
| Dyslipidemia | −0.38 | −6.26; 5.51 | 3.00 | 0.900 |
| Overweight | −1.19 | −9.05; 6.66 | 4.00 | 0.765 |
| Abdominal Obesity | −2.41 | −10.85; 6.04 | 4.30 | 0.576 |
| Cardiovascular Event | −11.98 | −20.82; −3.13 | 4.50 | 0.008 |
| Adherence to Physical Activity | 26.64 | 20.88; 32.40 | 2.93 | <0.001 |
| Adherence to Diet | 3.66 | −1.89; 9.21 | 2.82 | 0.195 |
| Adherence to Medication | −0.08 | −6.10; 5.95 | 3.06 | 0.980 |
| Smoking | 15.32 | 2.76; 27.88 | 6.39 | 0.087 |
| PAIN (r2 = 0.15) | ||||
| Variables | β | CI (95%) | Standard Error | p |
| Hospitalization time in days (Log) | −1.65 | −3.34; 0.03 | 0.86 | 0.055 |
| Age (years) | −0.16 | −0.28; −0.04 | 0.06 | 0.011 |
| Male Sex | 2.82 | 0.09; 5.54 | 1.39 | 0.043 |
| Schooling (years) | −0.06 | −0.38; 0.26 | 0.16 | 0.716 |
| Private Health Care System | 8.54 | 5.33; 11.76 | 1.64 | <0.001 |
| Systemic Arterial Hypertension | −2.36 | −5.67; 0.96 | 1.69 | 0.163 |
| Diabetes Mellitus | 2.54 | −0.22; 5.29 | 1.40 | 0.071 |
| Dyslipidemia | −0.54 | −3.22; 2.14 | 1.36 | 0.691 |
| Overweight | 2.26 | −1.32; 5.84 | 1.82 | 0.216 |
| Abdominal Obesity | 2.03 | −1.81; 5.88 | 1.96 | 0.300 |
| Cardiovascular Event | −1.43 | −5.46; 2.60 | 2.05 | 0.486 |
| Adherence to Physical Activity | 5.83 | 3.21; 8.46 | 1.34 | <0.001 |
| Adherence to Diet | 0.54 | −1.99; 3.07 | 1.29 | 0.674 |
| Adherence to Medication | −0.22 | −2.96; 2.53 | 1.40 | 0.877 |
| Smoking | 2.09 | −3.64; 7.81 | 2.91 | 0.474 |
| GENERAL HEALTH STATUS (r2 = 0.19) | ||||
| Variables | β | CI (95%) | Standard Error | p |
| Hospitalization time in days (Log) | −4.31 | −6.28; −2.34 | 1.00 | <0.001 |
| Age (years) | −0.01 | −0.15; 0.13 | 0.07 | 0.875 |
| Male Sex | 5.30 | 2.11; 8.48 | 1.62 | 0.001 |
| Schooling (years) | 0.48 | 0.11; 0.86 | 0.19 | 0.011 |
| Private Health Care System | 1.24 | −2.52; 4.99 | 1.91 | 0.517 |
| Systemic Arterial Hypertension | −5.79 | −9.66; −1.92 | 1.97 | 0.003 |
| Diabetes Mellitus | −0.15 | −3.36; 3.07 | 1.64 | 0.928 |
| Dyslipidemia | −3.58 | −6.71; −0.45 | 1.59 | 0.025 |
| Overweight | 3.68 | −0.50; 7.86 | 2.13 | 0.084 |
| Abdominal Obesity | 3.96 | −0.53; 8.46 | 2.29 | 0.084 |
| Cardiovascular Event | −4.37 | −9.08; 0.34 | 2.40 | 0.069 |
| Adherence to Physical Activity | 6.04 | 2.97; 9.11 | 1.56 | <0.001 |
| Adherence to Diet | 0.22 | −2.73; 3.17 | 1.50 | 0.883 |
| Adherence to Medication | 0.34 | −2.87; 3.54 | 1.63 | 0.837 |
| Smoking | −3.96 | −10.64; 2.73 | 3.40 | 0.245 |
| VITALITY (r2 = 0.14) | ||||
| Variables | β | CI (95%) | Standard Error | p |
| Hospitalization time in days (Log) | −1.30 | −2.84; 0.25 | 0.79 | 0.101 |
| Age (years) | 0.00 | −0.11; 0.11 | 0.06 | 0.964 |
| Male Sex | 4.31 | 1.81; 6.82 | 1.27 | 0.001 |
| Schooling (years) | 0.15 | −0.15; 0.44 | 0.15 | 0.320 |
| Private Health Care System | 2.03 | −0.92; 4.98 | 1.50 | 0.178 |
| Systemic Arterial Hypertension | −1.47 | −4.51; 1.57 | 1.55 | 0.343 |
| Diabetes Mellitus | 0.63 | −1.90; 3.15 | 1.29 | 0.627 |
| Dyslipidemia | −1.21 | −3.67; 1.25 | 1.25 | 0.333 |
| Overweight | 2.13 | −1.15; 5.42 | 1.67 | 0.202 |
| Abdominal Obesity | −0.67 | −4.21; 2.86 | 1.80 | 0.708 |
| Cardiovascular Event | −5.10 | −8.79; −1.40 | 1.88 | 0.007 |
| Adherence to Physical Activity | 5.53 | 3.12; 7.94 | 1.23 | <0.001 |
| Adherence to Diet | −0.55 | −2.87; 1.77 | 1.18 | 0.642 |
| Adherence to Medication | 2.72 | 0.20; 5.24 | 1.28 | 0.034 |
| Smoking | −0.29 | −5.54; 4.96 | 2.67 | 0.913 |
| SOCIAL ASPECT (r2 = 0.13) | ||||
| Variables | β | CI (95%) | Standard Error | p |
| Hospitalization time in days (Log) | −1.97 | −3.94; 0.01 | 1.01 | 0.051 |
| Age (years) | −0.12 | −0.26; 0.02 | 0.07 | 0.092 |
| Male Sex | 5.73 | 2.52; 8.93 | 1.63 | <0.001 |
| Schooling (years) | 0.39 | 0.76; 0.01 | 0.19 | 0.044 |
| Private Health Care System | 4.57 | 0.79; 8.34 | 1.92 | 0.018 |
| Systemic Arterial Hypertension | −2.79 | −6.68; 1.10 | 1.98 | 0.159 |
| Diabetes Mellitus | −0.14 | −3.37; 3.09 | 1.65 | 0.932 |
| Dyslipidemia | −1.00 | −4.15; 2.15 | 1.60 | 0.534 |
| Overweight | −0.70 | −4.90; 3.50 | 2.14 | 0.744 |
| Abdominal Obesity | −3.69 | −8.21; 0.82 | 2.30 | 0.109 |
| Cardiovascular Event | −8.14 | −12.87; −3.41 | 2.41 | 0.001 |
| Adherence to Physical Activity | 6.49 | 3.41; 9.57 | 1.57 | <.001 |
| Adherence to Diet | 0.70 | −2.27; 3.66 | 1.51 | 0.644 |
| Adherence to Medication | 0.58 | −2.65; 3.80 | 1.64 | 0.726 |
| Smoking | −1.13 | −7.84; 5.59 | 3.42 | 0.742 |
| EMOTIONAL ASPECT (r2 = 0.15) | ||||
| Variables | β | CI (95%) | Standard Error | p |
| Hospitalization time in days (Log) | −2.98 | −6.42; 0.45 | 1.75 | 0.089 |
| Age (years) | −0.10 | −0.34; 0.15 | 0.13 | 0.447 |
| Male Sex | 8.83 | 3.27; 14.39 | 2.83 | 0.002 |
| Schooling (years) | −0.18 | −0.84; 0.47 | 0.33 | 0.580 |
| Private Health Care System | 5.73 | −0.83; 12.28 | 3.34 | 0.087 |
| Systemic Arterial Hypertension | −2.37 | −9.13; 4.39 | 3.44 | 0.491 |
| Diabetes Mellitus | −3.20 | −8.82; 2.42 | 2.86 | 0.263 |
| Dyslipidemia | 0.02 | −5.45; 5.48 | 2.78 | 0.995 |
| Overweight | 3.67 | −3.63; 10.97 | 3.71 | 0.324 |
| Abdominal Obesity | 1.46 | −6.39; 9.31 | 3.99 | 0.715 |
| Cardiovascular Event | −16.84 | −25.06; −8.62 | 4.18 | <0.001 |
| Adherence to Physical Activity | 13.76 | 8.40; 19.11 | 2.72 | <0.001 |
| Adherence to Diet | 2.57 | −2.59; 7.72 | 2.62 | 0.329 |
| Adherence to Medication | 4.78 | −0.81; 10.37 | 2.85 | 0.094 |
| Smoking | 3.83 | −7.84; 15.49 | 5.94 | 0.520 |
| MENTAL HEALTH (r2 = 0.10) | ||||
| Variables | β | CI (95%) | Standard Error | p |
| Hospitalization time in days (Log) | −0.29 | −1.81; 1.23 | 0.77 | 0.706 |
| Age (years) | 0.07 | −0.04; 0.17 | 0.06 | 0.246 |
| Male Sex | 4.10 | 1.64; 6.55 | 1.25 | 0.001 |
| Schooling (years) | 0.00 | −0.29; 0.29 | 0.15 | 0.983 |
| Private Health Care System | 2.63 | −0.27; 5.52 | 1.48 | 0.075 |
| Systemic Arterial Hypertension | −1.24 | −4.22; 1.75 | 1.52 | 0.416 |
| Diabetes Mellitus | −0.22 | −2.70; 2.27 | 1.26 | 0.865 |
| Dyslipidemia | −1.98 | −4.40; 0.43 | 1.23 | 0.107 |
| Overweight | −0.22 | −3.45; 3.00 | 1.64 | 0.891 |
| Abdominal Obesity | −1.23 | −4.7; 2.24 | 1.76 | 0.487 |
| Cardiovascular Event | −5.87 | −9.50; −2.24 | 1.85 | 0.002 |
| Adherence to Physical Activity | 3.56 | 1.19; 5.92 | 1.20 | 0.003 |
| Adherence to Diet | −0.87 | −3.15; 1.40 | 1.16 | 0.452 |
| Adherence to Medication | 2.02 | −0.46; 4.49 | 1.26 | 0.110 |
| Smoking | −3.57 | −8.72; 1.59 | 2.62 | 0.175 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
de Carvalho Costa, I.M.N.B.; da Silva, D.G.; Oliveira, J.L.M.; Silva, J.R.S.; de Andrade, F.A.; de Góes Jorge, J.; de Oliveira, L.M.S.M.; de Almeida, R.R.; Oliveira, V.B.; Martins, L.S.; et al. Quality of Life among Patients with Acute Coronary Syndromes Receiving Care from Public and Private Health Care Systems in Brazil. Clin. Pract. 2022, 12, 513-526. https://doi.org/10.3390/clinpract12040055
de Carvalho Costa IMNB, da Silva DG, Oliveira JLM, Silva JRS, de Andrade FA, de Góes Jorge J, de Oliveira LMSM, de Almeida RR, Oliveira VB, Martins LS, et al. Quality of Life among Patients with Acute Coronary Syndromes Receiving Care from Public and Private Health Care Systems in Brazil. Clinics and Practice. 2022; 12(4):513-526. https://doi.org/10.3390/clinpract12040055
Chicago/Turabian Stylede Carvalho Costa, Ingrid Maria Novais Barros, Danielle Góes da Silva, Joselina Luzia Meneses Oliveira, José Rodrigo Santos Silva, Fabrício Anjos de Andrade, Juliana de Góes Jorge, Larissa Marina Santana Mendonça de Oliveira, Rebeca Rocha de Almeida, Victor Batista Oliveira, Larissa Santos Martins, and et al. 2022. "Quality of Life among Patients with Acute Coronary Syndromes Receiving Care from Public and Private Health Care Systems in Brazil" Clinics and Practice 12, no. 4: 513-526. https://doi.org/10.3390/clinpract12040055