
Cyclin D1 Serves as a Poor Prognostic Biomarker in Stage I Gastric Cancer

 , ,
, ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Patients and Specimens
2.2. Statistical Analysis
3. Results
3.1. Baseline Characteristics
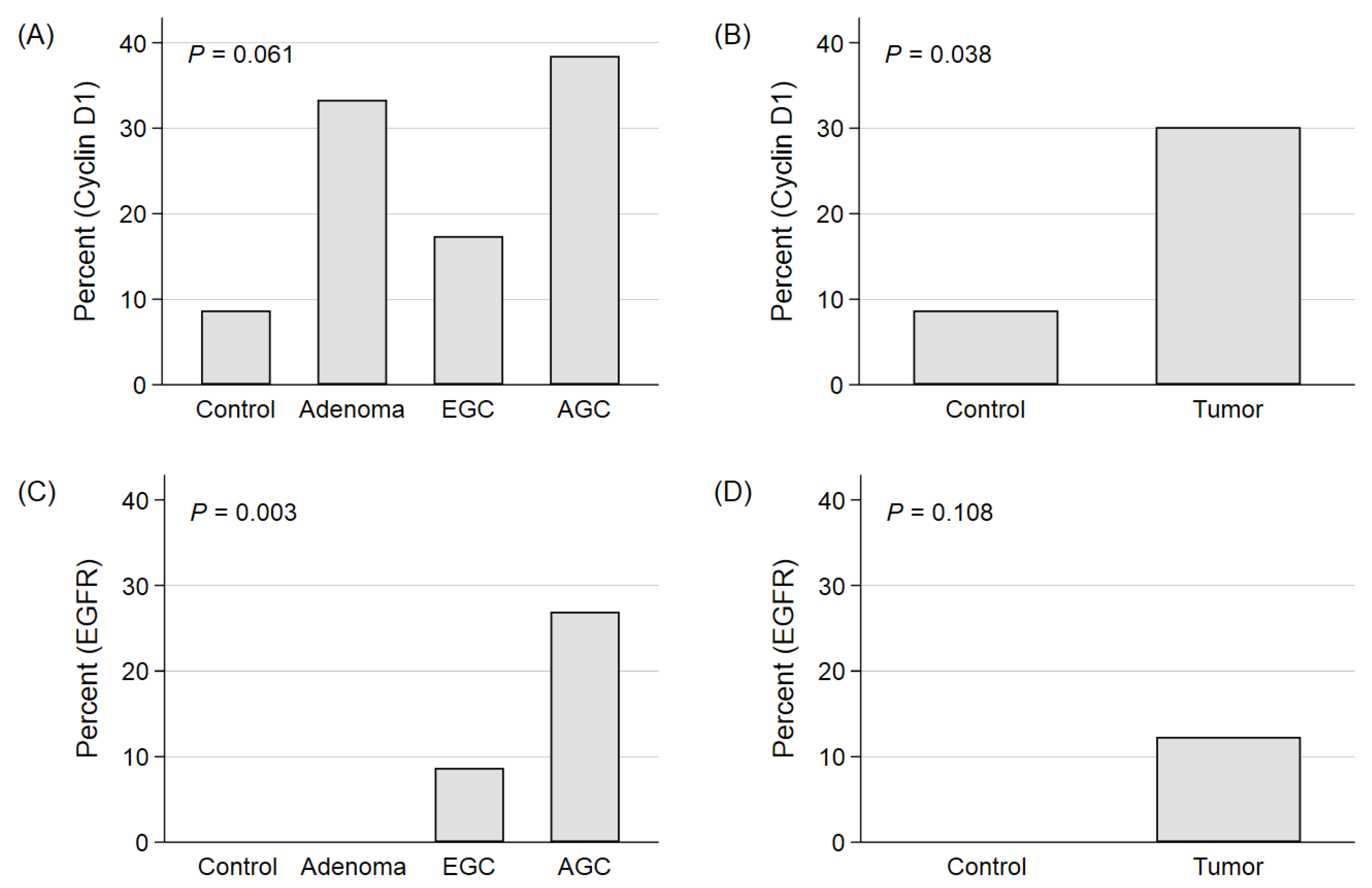
3.2. The Expression Patterns of Each Biomarker According to the Progression of Carcinogenesis and Advancement of Malignancy in GC
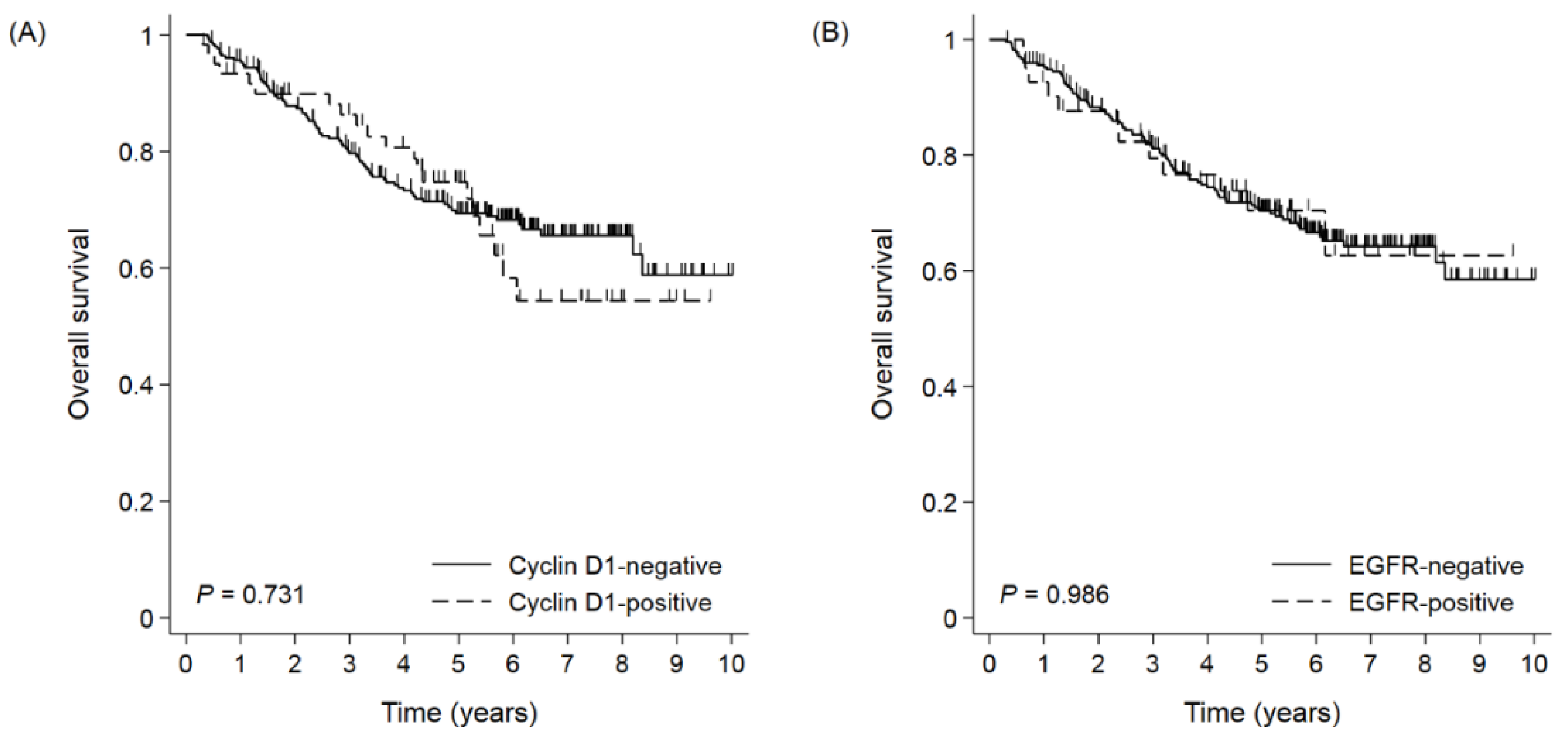
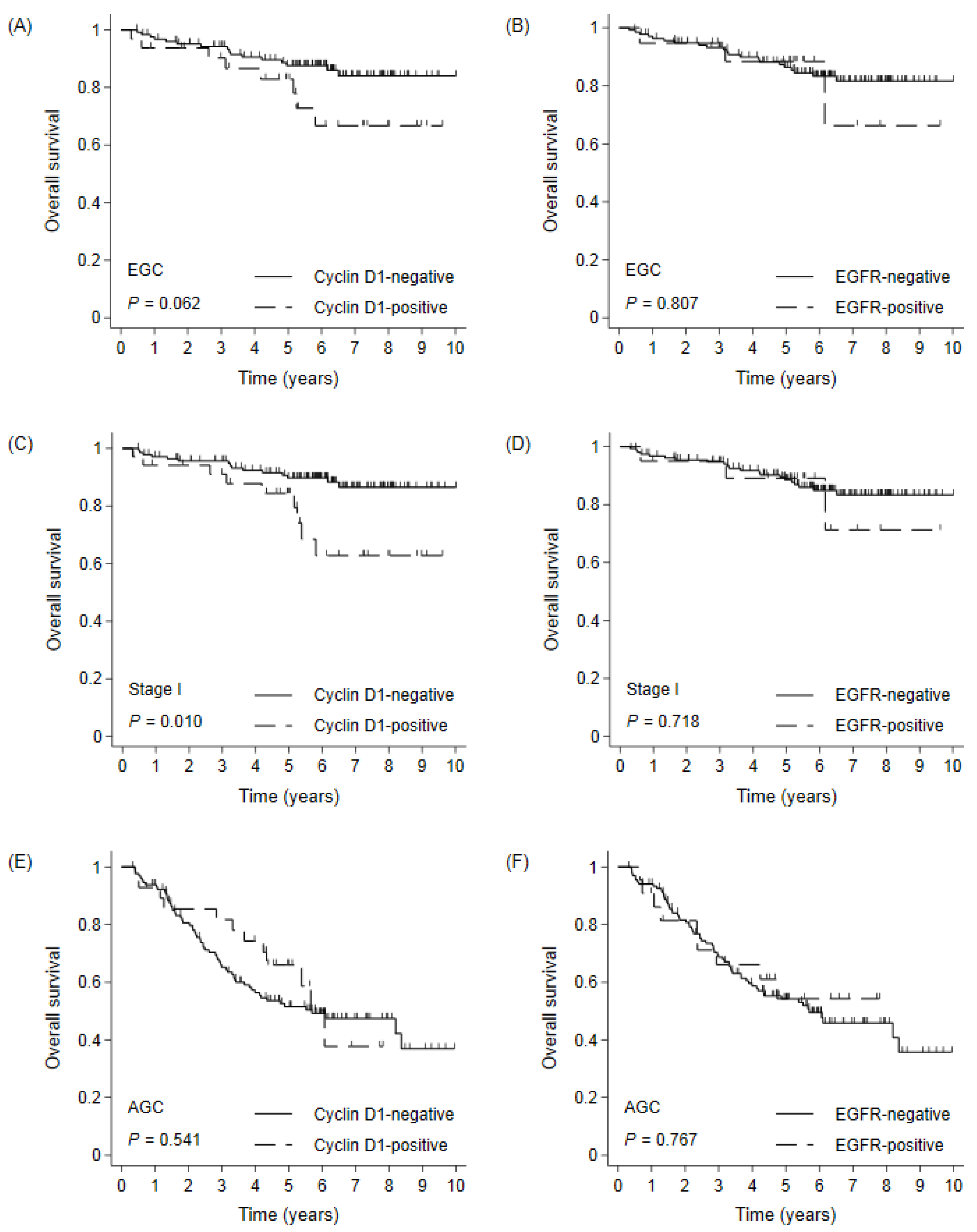
3.3. Overall Survival According to Cyclin D1 and EGFR Expression in Whole Cohort
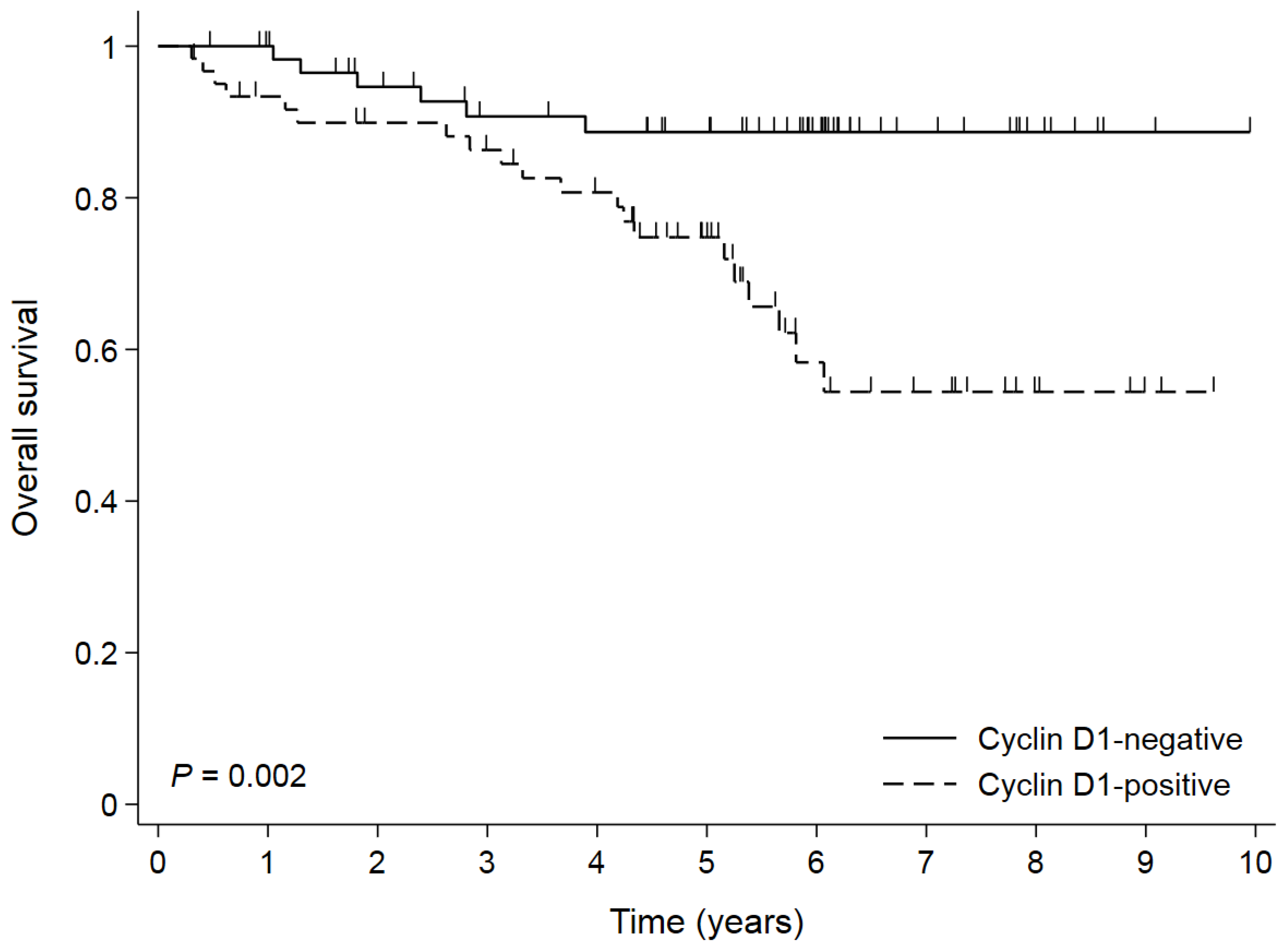
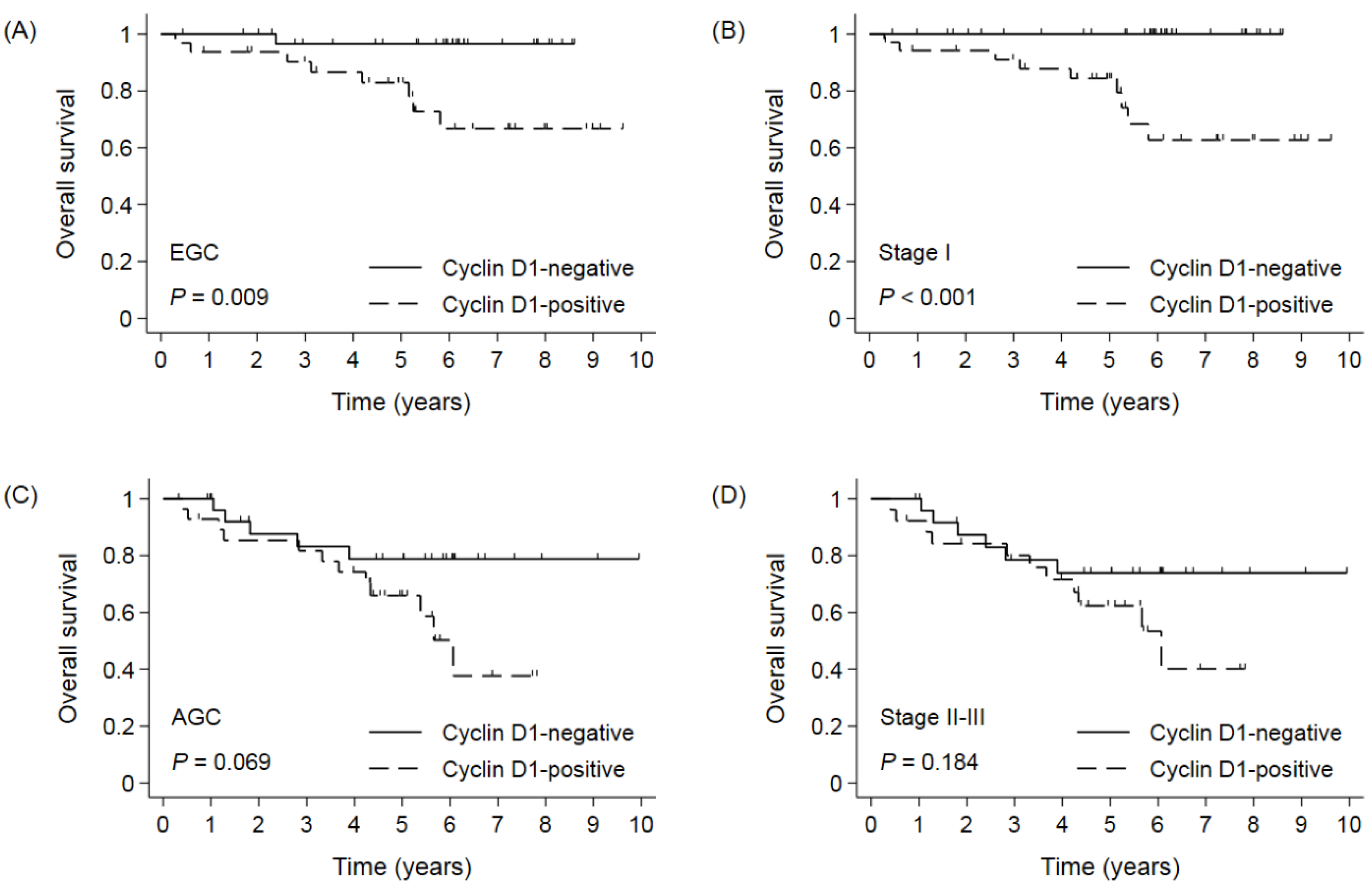
3.4. Survival According to Cyclin D1 Expression in Propensity Score-Matched Cohort
4. Discussion
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Bray, F.; Ferlay, J.; Soerjomataram, I.; Siegel, R.L.; Torre, L.A.; Jemal, A. Global cancer statistics 2018: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries. CA Cancer J. Clin. 2018, 68, 394–424. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hong, S.; Won, Y.J.; Lee, J.J.; Jung, K.W.; Kong, H.J.; Im, J.S.; Seo, H.G. Community of Population-Based Regional Cancer, R. Cancer Statistics in Korea: Incidence, Mortality, Survival, and Prevalence in 2018. Cancer Res. Treat. 2021, 53, 301–315. [Google Scholar] [CrossRef] [PubMed]
- Mo, H.; Li, P.; Jiang, S. A novel nomogram based on cardia invasion and chemotherapy to predict postoperative overall survival of gastric cancer patients. World J. Surg. Oncol. 2021, 19, 256. [Google Scholar] [CrossRef] [PubMed]
- Ko, G.H.; Go, S.I.; Lee, W.S.; Lee, J.H.; Jeong, S.H.; Lee, Y.J.; Hong, S.C.; Ha, W.S. Prognostic impact of Ki-67 in patients with gastric cancer-the importance of depth of invasion and histologic differentiation. Medicine 2017, 96, e7181. [Google Scholar] [CrossRef] [PubMed]
- Go, S.I.; Ko, G.H.; Lee, W.S.; Kim, R.B.; Lee, J.H.; Jeong, S.H.; Lee, Y.J.; Hong, S.C.; Ha, W.S. CD44 Variant 9 Serves as a Poor Prognostic Marker in Early Gastric Cancer, But Not in Advanced Gastric Cancer. Cancer Res. Treat. 2016, 48, 142–152. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zhang, Y.; Yu, C. Development and validation of a Surveillance, Epidemiology, and End Results (SEER)-based prognostic nomogram for predicting survival in elderly patients with gastric cancer after surgery. J. Gastrointest. Oncol. 2021, 12, 278–296. [Google Scholar] [CrossRef] [PubMed]
- Zhou, C.; Guo, Z.; Xu, L.; Jiang, H.; Sun, P.; Zhu, X.; Mu, X. PFND1 Predicts Poor Prognosis of Gastric Cancer and Promotes Cell Metastasis by Activating the Wnt/beta-Catenin Pathway. Onco Targets Ther. 2020, 13, 3177–3186. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Liu, H.; Zhang, Z.; Han, Y.; Fan, A.; Liu, H.; Zhang, X.; Liu, Y.; Zhang, R.; Liu, W.; Lu, Y.; et al. The FENDRR/FOXC2 Axis Contributes to Multidrug Resistance in Gastric Cancer and Correlates With Poor Prognosis. Front. Oncol. 2021, 11, 634579. [Google Scholar] [CrossRef] [PubMed]
- Guo, G.F.; Cai, Y.C.; Zhang, B.; Xu, R.H.; Qiu, H.J.; Xia, L.P.; Jiang, W.Q.; Hu, P.L.; Chen, X.X.; Zhou, F.F.; et al. Overexpression of SGLT1 and EGFR in colorectal cancer showing a correlation with the prognosis. Med. Oncol. 2011, 28 (Suppl. S1), S197–S203. [Google Scholar] [CrossRef] [PubMed]
- Park, S.J.; Gu, M.J.; Lee, D.S.; Yun, S.S.; Kim, H.J.; Choi, J.H. EGFR expression in pancreatic intraepithelial neoplasia and ductal adenocarcinoma. Int. J. Clin. Exp. Pathol. 2015, 8, 8298–8304. [Google Scholar]
- Fard, S.S.; Saliminejad, K.; Sotoudeh, M.; Soleimanifard, N.; Kouchaki, S.; Yazdanbod, M.; Mahmoodzadeh, H.; Ghavamzadeh, A.; Malekzadeh, R.; Chahardouli, B.; et al. The Correlation between EGFR and Androgen Receptor Pathways: A Novel Potential Prognostic Marker in Gastric Cancer. Anticancer Agents Med. Chem. 2019, 19, 2097–2107. [Google Scholar] [CrossRef] [PubMed]
- Al Zobair, A.A.; Al Obeidy, B.F.; Yang, L.; Yang, C.; Hui, Y.; Yu, H.; Zheng, F.; Yang, G.; Xie, C.; Zhou, F.; et al. Concomitant overexpression of EGFR and CXCR4 is associated with worse prognosis in a new molecular subtype of non-small cell lung cancer. Oncol. Rep. 2013, 29, 1524–1532. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Uribe, M.L.; Marrocco, I.; Yarden, Y. EGFR in Cancer: Signaling Mechanisms, Drugs, and Acquired Resistance. Cancers 2021, 13, 2748. [Google Scholar] [CrossRef] [PubMed]
- Yang, G.; Huang, L.; Jia, H.; Aikemu, B.; Zhang, S.; Shao, Y.; Hong, H.; Yesseyeva, G.; Wang, C.; Li, S.; et al. NDRG1 enhances the sensitivity of cetuximab by modulating EGFR trafficking in colorectal cancer. Oncogene 2021, 40, 5993–6006. [Google Scholar] [CrossRef] [PubMed]
- Wang, Y.K.; Gao, C.F.; Yun, T.; Chen, Z.; Zhang, X.W.; Lv, X.X.; Meng, N.L.; Zhao, W.Z. Assessment of ERBB2 and EGFR gene amplification and protein expression in gastric carcinoma by immunohistochemistry and fluorescence in situ hybridization. Mol. Cytogenet. 2011, 4, 14. [Google Scholar]
- Montalto, F.I.; De Amicis, F. Cyclin D1 in Cancer: A Molecular Connection for Cell Cycle Control, Adhesion and Invasion in Tumor and Stroma. Cells 2020, 9, 2648. [Google Scholar] [CrossRef] [PubMed]
- Tchakarska, G.; Sola, B. The double dealing of cyclin D1. Cell Cycle 2020, 19, 163–178. [Google Scholar] [CrossRef] [Green Version]
- Shan, Y.S.; Hsu, H.P.; Lai, M.D.; Hung, Y.H.; Wang, C.Y.; Yen, M.C.; Chen, Y.L. Cyclin D1 overexpression correlates with poor tumor differentiation and prognosis in gastric cancer. Oncol. Lett. 2017, 14, 4517–4526. [Google Scholar] [CrossRef] [Green Version]
- He, Q.; Wu, J.; Liu, X.L.; Ma, Y.H.; Wu, X.T.; Wang, W.Y.; An, H.X. Clinicopathological and prognostic significance of cyclin D1 amplification in patients with breast cancer: A meta-analysis. J. BUON 2017, 22, 1209–1216. [Google Scholar]
- Bachmann, K.; Neumann, A.; Hinsch, A.; Nentwich, M.F.; El Gammal, A.T.; Vashist, Y.; Perez, D.; Bockhorn, M.; Izbicki, J.R.; Mann, O. Cyclin D1 is a strong prognostic factor for survival in pancreatic cancer: Analysis of CD G870A polymorphism, FISH and immunohistochemistry. J. Surg. Oncol. 2015, 111, 316–323. [Google Scholar] [CrossRef]
- Luangdilok, S.; Wanchaijiraboon, P.; Chantranuwatana, P.; Teerapakpinyo, C.; Shuangshoti, S.; Sriuranpong, V. Cyclin D1 expression as a potential prognostic factor in advanced KRAS-mutant non-small cell lung cancer. Transl. Lung Cancer Res. 2019, 8, 959–966. [Google Scholar] [CrossRef] [PubMed]
- Gu, X.Y.; Jiang, Y.; Li, M.Q.; Han, P.; Liu, Y.L.; Cui, B.B. Over-expression of EGFR regulated by RARA contributes to 5-FU resistance in colon cancer. Aging 2020, 12, 156–177. [Google Scholar] [CrossRef] [PubMed]
- Li, W.; Liu, Z.; Li, C.; Li, N.; Fang, L.; Chang, J.; Tan, J. Radionuclide therapy using (1)(3)(1)I-labeled anti-epidermal growth factor receptor-targeted nanoparticles suppresses cancer cell growth caused by EGFR overexpression. J. Cancer Res. Clin. Oncol. 2016, 142, 619–632. [Google Scholar] [CrossRef] [PubMed]
- Ema, A.; Waraya, M.; Yamashita, K.; Kokubo, K.; Kobayashi, H.; Hoshi, K.; Shinkai, Y.; Kawamata, H.; Nakamura, K.; Nishimiya, H.; et al. Identification of EGFR expression status association with metastatic lymph node density (ND) by expression microarray analysis of advanced gastric cancer. Cancer Med. 2015, 4, 90–100. [Google Scholar] [CrossRef] [PubMed]
- Tang, C.; Yang, L.; Wang, N.; Li, L.; Xu, M.; Chen, G.G.; Liu, Z.M. High expression of GPER1, EGFR and CXCR1 is associated with lymph node metastasis in papillary thyroid carcinoma. Int. J. Clin. Exp. Pathol. 2014, 7, 3213–3223. [Google Scholar] [PubMed]
- Carlsson, J.; Shen, L.; Xiang, J.; Xu, J.; Wei, Q. Tendencies for higher co-expression of EGFR and HER2 and downregulation of HER3 in prostate cancer lymph node metastases compared with corresponding primary tumors. Oncol. Lett. 2013, 5, 208–214. [Google Scholar] [CrossRef] [PubMed]
- Hashmi, A.A.; Hussain, Z.F.; Aijaz, S.; Irfan, M.; Khan, E.Y.; Naz, S.; Faridi, N.; Khan, A.; Edhi, M.M. Immunohistochemical expression of epidermal growth factor receptor (EGFR) in South Asian head and neck squamous cell carcinoma: Association with various risk factors and clinico-pathologic and prognostic parameters. World J. Surg. Oncol. 2018, 16, 118. [Google Scholar] [CrossRef] [PubMed]
- Lerias, S.; Esteves, S.; Silva, F.; Cunha, M.; Cochicho, D.; Martins, L.; Felix, A. CD274 (PD-L1), CDKN2A (p16), TP53, and EGFR immunohistochemical profile in primary, recurrent and metastatic vulvar cancer. Mod. Pathol. 2020, 33, 893–904. [Google Scholar] [CrossRef] [PubMed]
- Ben Brahim, E.; Ayari, I.; Jouini, R.; Atafi, S.; Koubaa, W.; Elloumi, H.; Chadli, A. Expression of epidermal growth factor receptor (EGFR) in colorectal cancer: An immunohistochemical study. Arab. J. Gastroenterol. 2018, 19, 121–124. [Google Scholar] [CrossRef] [PubMed]
- Martins, W.P.; Zanardi, J.V. Subgroup analysis and statistical power. Eur. J. Obstet. Gynecol. Reprod. Biol. 2011, 159, 244–245. [Google Scholar] [CrossRef]
- Shevra, C.R.; Ghosh, A.; Kumar, M. Cyclin D1 and Ki-67 expression in normal, hyperplastic and neoplastic endometrium. J. Postgrad. Med. 2015, 61, 15–20. [Google Scholar]
- Kaufmann, C.; Kempf, W.; Mangana, J.; Cheng, P.; Emberger, M.; Lang, R.; Kaiser, A.K.; Lattmann, E.; Levesque, M.; Dummer, R.; et al. The role of cyclin D1 and Ki-67 in the development and prognostication of thin melanoma. Histopathology 2020, 77, 460–470. [Google Scholar] [CrossRef]
- Go, S.I.; Ko, G.H.; Lee, W.S.; Lee, J.H.; Jeong, S.H.; Lee, Y.J.; Hong, S.C.; Ha, W.S. The Use of CD44 Variant 9 and Ki-67 Combination Can Predicts Prognosis Better Than Their Single Use in Early Gastric Cancer. Cancer Res. Treat. 2019, 51, 1411–1419. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zinczuk, J.; Zareba, K.; Guzinska-Ustymowicz, K.; Kedra, B.; Kemona, A.; Pryczynicz, A. Expression of chosen cell cycle and proliferation markers in pancreatic intraepithelial neoplasia. Prz. Gastroenterol. 2018, 13, 118–126. [Google Scholar] [CrossRef] [PubMed]
- Gao, P.; Zhou, G.Y.; Liu, Y.; Li, J.S.; Zhen, J.H.; Yuan, Y.P. Alteration of cyclin D1 in gastric carcinoma and its clinicopathologic significance. World J. Gastroenterol. 2004, 10, 2936–2939. [Google Scholar] [CrossRef] [Green Version]
- Patel, S.B.; Manjunatha, B.S.; Shah, V.; Soni, N.; Sutariya, R. Immunohistochemical evaluation of p63 and cyclin D1 in oral squamous cell carcinoma and leukoplakia. J. Korean Assoc. Oral Maxillofac. Surg. 2017, 43, 324–330. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cho, E.Y.; Han, J.J.; Choi, Y.L.; Kim, K.M.; Oh, Y.L. Comparison of Her-2, EGFR and cyclin D1 in primary breast cancer and paired metastatic lymph nodes: An immunohistochemical and chromogenic in situ hybridization study. J. Korean Med. Sci. 2008, 23, 1053–1061. [Google Scholar] [CrossRef]








{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Cyclin D1-Negative (n = 255) | Cyclin D1-Positive (n = 61) | p | EGFR-Negative (n = 275) | EGFR-Positive (n = 41) | p | |
|---|---|---|---|---|---|---|
| Median (IQR) age, years | 65 (56–70) | 64 (54–70) | 0.890 | 65 (56–70) | 66 (56–69) | 0.958 |
| Sex | 0.504 | 0.544 | ||||
| Male | 164 (64.3) | 42 (68.9) | 181 (65.8) | 25 (61.0) | ||
| Female | 91 (35.7) | 19 (31.2) | 94 (34.2) | 16 (39.0) | ||
| Location | 0.117 | 0.997 | ||||
| Upper | 26 (10.2) | 12 (19.7) | 33 (12.0) | 5 (12.2) | ||
| Middle | 51 (20.0) | 12 (19.7) | 55 (20.0) | 8 (19.5) | ||
| Lower | 178 (69.8) | 37 (60.7) | 187 (68.0) | 28 (68.3) | ||
| Operation | 0.957 | 0.699 | ||||
| Subtotal gastrectomy | 180 (70.6) | 41 (67.2) | 190 (69.1) | 31 (75.6) | ||
| Total gastrectomy | 60 (23.5) | 16 (26.2) | 67 (24.4) | 9 (22.0) | ||
| Proximal gastrectomy | 12 (4.7) | 3 (4.9) | 14 (5.1) | 1 (2.4) | ||
| Wedge resection | 3 (1.2) | 1 (1.6) | 4 (1.5) | 0 | ||
| Depth of invasion | 0.669 | 0.616 | ||||
| EGC | 126 (49.4) | 32 (52.5) | 139 (50.6) | 19 (46.3) | ||
| AGC | 129 (50.6) | 29 (47.5) | 136 (49.5) | 22 (53.7) | ||
| Nodal status | 0.650 | 0.455 | ||||
| N0 | 155 (60.8) | 39 (63.9) | 171 (62.2) | 23 (56.1) | ||
| N+ | 100 (39.2) | 22 (36.1) | 104 (37.8) | 18 (43.9) | ||
| AJCC 8th edition staging | 0.088 | 0.577 | ||||
| I | 141 (55.3) | 35 (57.4) | 156 (56.7) | 20 (48.8) | ||
| II | 43 (16.9) | 16 (26.2) | 51 (18.6) | 8 (19.5) | ||
| III | 71 (27.8) | 10 (16.4) | 68 (24.7) | 13 (31.7) | ||
| Tumor size | 0.819 | 0.367 | ||||
| ≤4 cm | 117 (45.9) | 27 (44.3) | 128 (46.6) | 16 (39.0) | ||
| >4 cm | 138 (54.1) | 34 (55.7) | 147 (53.5) | 25 (61.0) | ||
| WHO classification | 0.597 | 0.389 | ||||
| Well-differentiated | 56 (22.0) | 10 (16.4) | 60 (21.8) | 6 (14.6) | ||
| Moderately differentiated | 77 (30.2) | 21 (34.4) | 82 (29.8) | 16 (39.0) | ||
| Poorly differentiated and others * | 122 (47.8) | 30 (49.2) | 133 (48.4) | 19 (46.3) | ||
| Lauren classification | 0.287 | 0.096 | ||||
| Intestinal | 179 (70.2) | 47 (77.1) | 192 (69.8) | 34 (82.9) | ||
| Diffuse or mixed | 76 (29.8) | 14 (23.0) | 83 (30.2) | 7 (17.1) |
| Univariate | Multivariate | ||||||
|---|---|---|---|---|---|---|---|
| HR | 95% CI | p | HR | 95% CI | p | p (Bootstrap) | |
| Age (≥65 vs. <65) | 2.623 | 1.087–6.328 | 0.032 | 2.679 | 1.110–6.466 | 0.028 | 0.042 |
| Sex (male vs. female) | 3.384 | 1.009–11.347 | 0.048 | 3.547 | 1.056–11.909 | 0.041 | 0.876 |
| Location (upper/middle vs. lower) | 1.086 | 0.465–2.538 | 0.849 | ||||
| Operation (total gastrectomy vs. others) | 1.894 | 0.752–4.774 | 0.176 | ||||
| Depth of invasion (AGC vs. EGC) | 0.651 | 0.153–2.770 | 0.561 | ||||
| Nodal status (positive vs. negative) | 2.035 | 0.477–8.685 | 0.337 | ||||
| Tumor size (>4 cm vs. ≤4 cm) | 0.687 | 0.273–1.730 | 0.425 | ||||
| WHO classification (others vs. well-differentiated) | 1.096 | 0.454–2.645 | 0.839 | ||||
| Lauren classification (diffuse/mixed vs. intestinal) | 1.055 | 0.419–2.658 | 0.910 | ||||
| Cyclin D1 (positive vs. negative) | 2.836 | 1.238–6.498 | 0.014 | 2.801 | 1.221–6.426 | 0.015 | 0.023 |
| EGFR (positive vs. negative) | 1.250 | 0.372–4.200 | 0.718 | ||||
| Univariate | Multivariate | ||||||
|---|---|---|---|---|---|---|---|
| HR | 95% CI | p | HR | 95% CI | p | p (Bootstrap) | |
| Age (≥65 vs. <65) | 0.833 | 0.385–1.803 | 0.643 | ||||
| Sex (male vs. female) | 1.881 | 0.755–4.688 | 0.175 | ||||
| Location (upper/middle vs. lower) | 1.266 | 0.575–2.791 | 0.558 | ||||
| Operation (total gastrectomy vs. others) | 1.940 | 0.863–4.362 | 0.109 | ||||
| Depth of invasion (AGC vs. EGC) | 2.564 | 1.139–5.769 | 0.023 | 1.033 | 0.328–3.255 | 0.956 | 0.960 |
| Nodal status (positive vs. negative) | 3.847 | 1.736–8.526 | 0.001 | 3.169 | 1.014–9.906 | 0.047 | 0.077 |
| Tumor size (>4 cm vs. ≤4 cm) | 2.102 | 0.913–4.838 | 0.081 | 1.403 | 0.576–3.414 | 0.456 | 0.479 |
| WHO classification (others vs. well-differentiated) | 0.931 | 0.351–2.469 | 0.885 | ||||
| Lauren classification (diffuse/mixed vs. intestinal) | 1.313 | 0.551–3.126 | 0.539 | ||||
| Cyclin D1 (positive vs. negative) | 3.831 | 1.532–9.578 | 0.004 | 3.630 | 1.450–9.086 | 0.006 | 0.030 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Go, S.-I.; Ko, G.H.; Lee, W.S.; Lee, J.-H.; Jeong, S.-H.; Lee, Y.-J.; Hong, S.C.; Ha, W.S. Cyclin D1 Serves as a Poor Prognostic Biomarker in Stage I Gastric Cancer. Curr. Issues Mol. Biol. 2022, 44, 1395-1406. https://doi.org/10.3390/cimb44030093
Go S-I, Ko GH, Lee WS, Lee J-H, Jeong S-H, Lee Y-J, Hong SC, Ha WS. Cyclin D1 Serves as a Poor Prognostic Biomarker in Stage I Gastric Cancer. Current Issues in Molecular Biology. 2022; 44(3):1395-1406. https://doi.org/10.3390/cimb44030093
Chicago/Turabian StyleGo, Se-Il, Gyung Hyuck Ko, Won Sup Lee, Jeong-Hee Lee, Sang-Ho Jeong, Young-Joon Lee, Soon Chan Hong, and Woo Song Ha. 2022. "Cyclin D1 Serves as a Poor Prognostic Biomarker in Stage I Gastric Cancer" Current Issues in Molecular Biology 44, no. 3: 1395-1406. https://doi.org/10.3390/cimb44030093