
The Role of Emotion Regulation and Executive Functioning in the Intervention Outcome of Children with Emotional and Behavioural Problems †

Abstract
:1. Introduction
2. Method
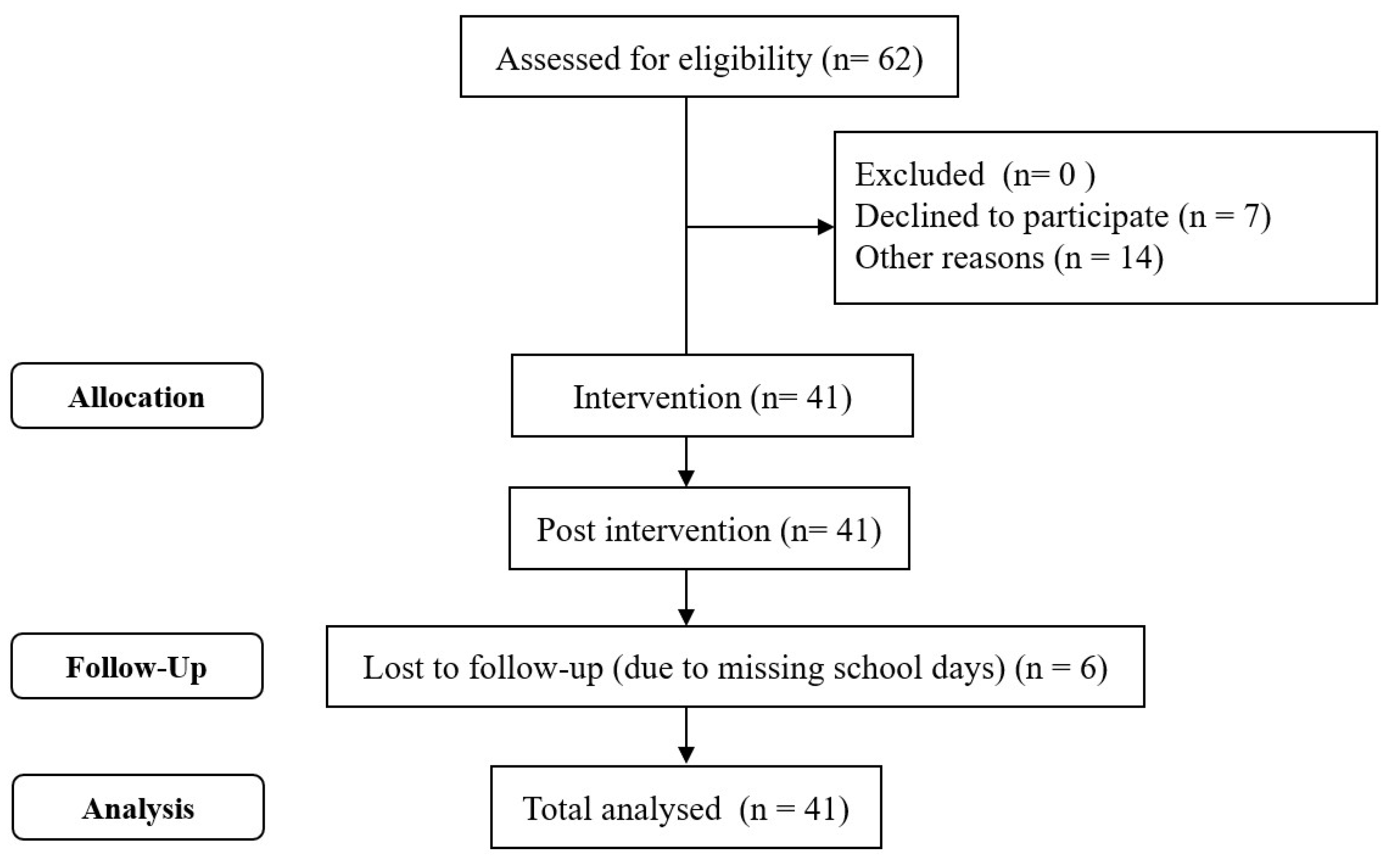
2.1. Participants
2.2. Procedure
2.3. Super Skills for Life Programme
2.4. Implementation of SSL
2.5. Measures
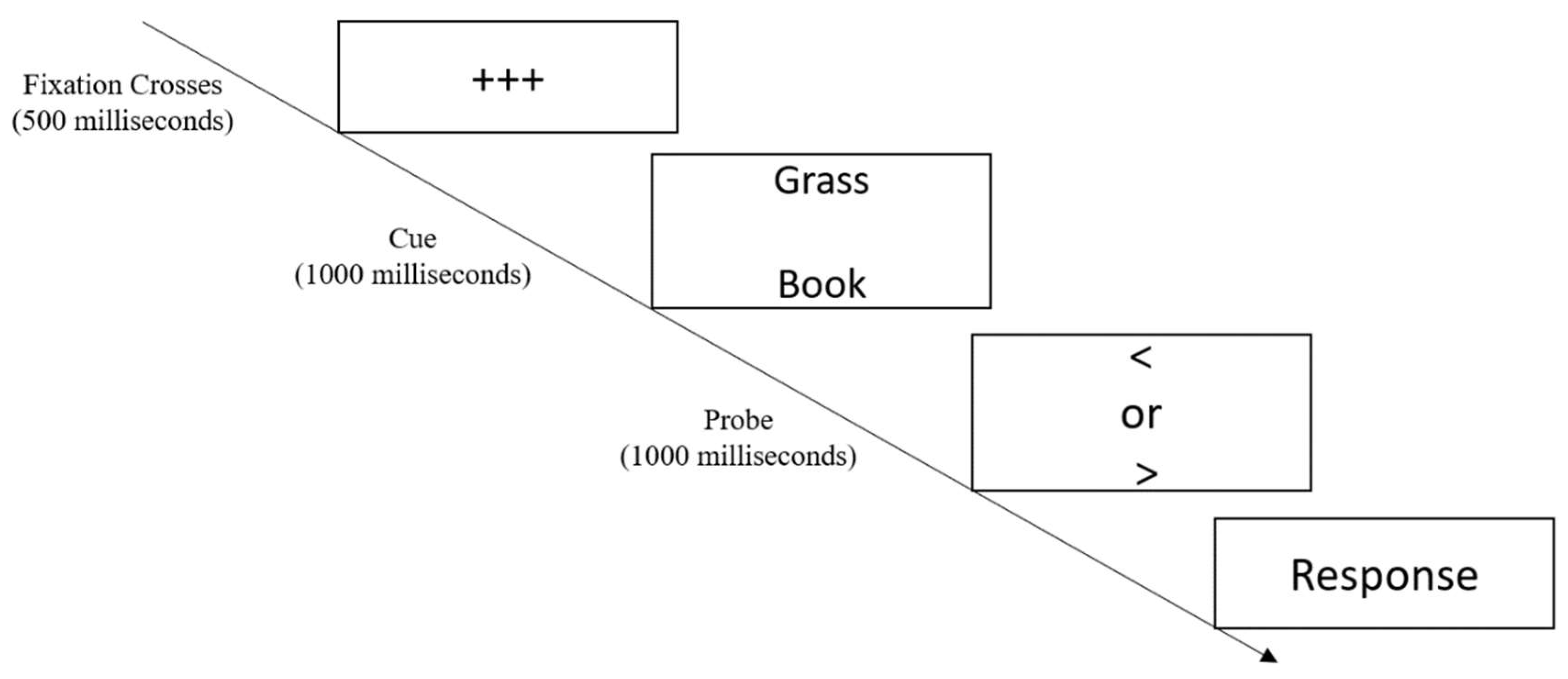
2.6. EF Tasks
2.7. Questionnaires
3. Results
3.1. Preliminary Analysis
3.2. Predictors and Mediators of Treatment Outcomes
4. Discussion
5. Strengths and Limitations
6. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Deighton, J.; Lereya, T.; Casey, P.; Patalay, P.; Humphrey, N.; Wolpert, M. Prevalence of mental health problems in schools: Poverty and other risk factors among 28,000 adolescents in England. Br. J. Psychiatry 2019, 215, 565–567. [Google Scholar] [CrossRef] [Green Version]
- Furniss, T.; Beyer, T.; Guggenmos, J. Prevalence of behavioural and emotional problems among six-years-old preschool children. Soc. Psychiatry Psychiatr. Epidemiol. 2006, 41, 394–399. [Google Scholar] [CrossRef] [PubMed]
- Aldao, A.; Gee, D.G.; De Los Reyes, A.; Seager, I. Emotion regulation as a transdiagnostic factor in the development of internalizing and externalizing psychopathology: Current and future directions. Dev. Psychopathol. 2016, 28, 927–946. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Campbell-Sills, L.; Barlow, D.H. Incorporating Emotion Regulation into Conceptualizations and Treatments of Anxiety and Mood Disorders; American Psychological Association: Washington, DC, USA, 2007. [Google Scholar]
- Kristin, D.; Thomas, H.; Hannesdottir, D.K.; Ollendick, T.H. The role of emotion regulation in the treatment of child anxiety disorders. Clin. Child Fam. Psychol. Rev. 2007, 10, 275–293. [Google Scholar]
- Zeman, J.; Shipman, K.; Suveg, C. Anger and sadness regulation: Predictions to internalizing and externalizing symptoms in children. J. Clin. Child Adolesc. Psychol. 2002, 31, 393–398. [Google Scholar] [CrossRef]
- Warren, S.L.; Heller, W.; Miller, G.A. The Structure of Executive Dysfunction in Depression and Anxiety. J. Affect. Disord. 2021, 279, 208–216. [Google Scholar] [CrossRef] [PubMed]
- Miyake, A.; Friedman, N.P.; Emerson, M.J.; Witzki, A.H.; Howerter, A.; Wager, T.D. The unity and diversity of executive functions and their contributions to complex “Frontal Lobe” tasks: A latent variable analysis. Cogn. Psychol. 2000, 41, 49–100. [Google Scholar] [CrossRef] [Green Version]
- Toren, P.; Sadeh, M.; Wolmer, L.; Eldar, S.; Koren, S.; Weizman, R.; Laor, N. Neurocognitive correlates of anxiety disorders in children: A preliminary report. J. Anxiety Disord. 2000, 14, 239–247. [Google Scholar] [CrossRef]
- Ajilchi, B.; Nejati, V. Executive Functions in Students With Depression, Anxiety, and Stress Symptoms. Basic Clin. Neurosci. 2017, 8, 223. [Google Scholar]
- O’Rourke, E.J.; Halpern, L.F.; Vaysman, R. Examining the relations among emerging adult coping, executive function, and anxiety. Emerg. Adulthood 2018, 8, 209–225. [Google Scholar] [CrossRef]
- Barch, D.M.; Harms, M.P.; Tillman, R.; Hawkey, E.; Luby, J.L. Early childhood depression, emotion regulation, episodic memory, and hippocampal development. J. Abnorm. Psychol. 2019, 128, 81–95. [Google Scholar] [CrossRef] [PubMed]
- Pruessner, L.; Barnow, S.; Holt, D.V.; Joormann, J.; Schulze, K. A cognitive control framework for understanding emotion regulation flexibility. Emotion 2020, 20, 21–29. [Google Scholar] [CrossRef] [PubMed]
- Garnefski, N.; Kraaij, V.; Spinhoven, P. Negative life events, cognitive emotion regulation and emotional problems. Pers. Individ. Dif. 2001, 30, 1311–1327. [Google Scholar] [CrossRef]
- Young, K.S.; Sandman, C.F.; Craske, M.G. Positive and Negative Emotion Regulation in Adolescence: Links to Anxiety and Depression. Brain Sci. 2019, 9, 76. [Google Scholar] [CrossRef] [Green Version]
- Golombek, K.; Lidle, L.; Tuschen-Caffier, B.; Schmitz, J.; Vierrath, V. The role of emotion regulation in socially anxious children and adolescents: A systematic review. Eur. Child Adolesc. Psychiatry 2019, 29, 1479–1501. [Google Scholar] [CrossRef] [PubMed]
- Platje, E.; Huijbregts, S.C.J.; van Goozen, S.H.M.; Popma, A.; Cima, M.; Swaab, H.J.T. Executive Functioning, Reward/Punishment Sensitivity, and Conduct Problems in Boys With Callous-Unemotional Traits. Int. J. Offender Ther. Comp. Criminol. 2018, 62, 4008–4023. [Google Scholar] [CrossRef]
- Graziano, P.A.; Landis, T.; Maharaj, A.; Ros-Demarize, R.; Hart, K.C.; Garcia, A. Differentiating Preschool Children with Conduct Problems and Callous-Unemotional Behaviors through Emotion Regulation and Executive Functioning. J. Clin. Child Adolesc. Psychol. 2019, 51, 170–182. [Google Scholar] [CrossRef]
- Tajik-Parvinchi, D.; Farmus, L.; Modica, P.T.; Cribbie, R.A.; Weiss, J.A. The role of cognitive control and emotion regulation in predicting mental health problems in children with neurodevelopmental disorders. Child. Care. Health Dev. 2021, 47, 608–617. [Google Scholar] [CrossRef]
- Emerson, C.; Mollet, G.; Harrison, D. Anxious-depression in boys: An evaluation of executive functioning. Arch. Clin. Neuropsychol. 2005, 20, 539–546. [Google Scholar] [CrossRef] [Green Version]
- Micco, J.A.; Henin, A.; Biederman, J.; Rosenbaum, J.F.; Petty, C.; Rindlaub, L.A.; Murphy, M.; Hirshfeld-Becker, D.R. Executive functioning in offspring at risk for depression and anxiety. Depress. Anxiety 2009, 26, 780–790. [Google Scholar] [CrossRef]
- Mohlman, J. More Power to the Executive? A Preliminary Test of CBT Plus Executive Skills Training for Treatment of Late-Life GAD. Cogn. Behav. Pract. 2008, 15, 306–316. [Google Scholar] [CrossRef]
- Huang, F.Y.; Hsu, A.-L.; Hsu, L.-M.; Tsai, J.-S.; Huang, C.-M.; Chao, Y.-P.; Hwang, T.-J.; Wu, C.W. Mindfulness Improves Emotion Regulation and Executive Control on Bereaved Individuals: An fMRI Study. Front. Hum. Neurosci. 2019, 12, 541. [Google Scholar] [CrossRef] [PubMed]
- Essau, C.A.; Olaya, B.; Sasagawa, S.; Pithia, J.; Bray, D.; Ollendick, T.H. Integrating video-feedback and cognitive preparation, social skills training and behavioural activation in a cognitive behavioural therapy in the treatment of childhood anxiety. J. Affect. Disord. 2014, 167, 261–267. [Google Scholar] [CrossRef] [PubMed]
- Higa-McMillan, C.K.; Francis, S.E.; Rith-Najarian, L.; Chorpita, B.F. Evidence Base Update: 50 Years of Research on Treatment for Child and Adolescent Anxiety. J. Clin. Child Adolesc. Psychol. 2015, 45, 91–113. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kodal, A.; Fjermestad, K.; Bjelland, I.; Gjestad, R.; Öst, L.-G.; Bjaastad, J.F.; Haugland, B.S.; Havik, O.E.; Heiervang, E.; Wergeland, G.J. Long-term effectiveness of cognitive behavioral therapy for youth with anxiety disorders. J. Anxiety Disord. 2018, 53, 58–67. [Google Scholar] [CrossRef]
- Essau, C.A.; Sasagawa, S.; Jones, G.; Fernandes, B.; Ollendick, T.H. Evaluating the real-world effectiveness of a cognitive behavior therapy-based transdiagnostic program for emotional problems in children in a regular school setting. J. Affect. Disord. 2019, 253, 357–365. [Google Scholar] [CrossRef]
- Goodkind, M.S.; Gallagher-Thompson, D.; Thompson, L.W.; Kesler, S.R.; Anker, L.; Flournoy, J.; Berman, M.P.; Holland, J.M.; O'Hara, R.M. The impact of executive function on response to cognitive behavioral therapy in late-life depression. Int. J. Geriatr. Psychiatry 2016, 31, 334–339. [Google Scholar] [CrossRef]
- Asnaani, A.; Tyler, J.; McCann, J.; Brown, L.; Zang, Y. Anxiety sensitivity and emotion regulation as mechanisms of successful CBT outcome for anxiety-related disorders in a naturalistic treatment setting. J. Affect. Disord. 2020, 267, 86–95. [Google Scholar] [CrossRef]
- Derella, O.J.; Johnston, O.G.; Loeber, R.; Burke, J.D. CBT-Enhanced Emotion Regulation as a Mechanism of Improvement for Childhood Irritability. J. Clin. Child Adolesc. Psychol. 2019, 48, 146–154. [Google Scholar] [CrossRef]
- Suveg, C.; Sood, E.; Comer, J.S.; Kendall, P.C. Changes in Emotion Regulation Following Cognitive-Behavioral Therapy for Anxious Youth. J. Clin. Child Adolesc. Psychol. 2009, 38, 390–401. [Google Scholar] [CrossRef]
- Ramdhonee-Dowlot, K.; Balloo, K.; Essau, C.A. Effectiveness of the Super Skills for Life programme in enhancing the emotional wellbeing of children and adolescents in residential care institutions in a low- and middle-income country: A randomised waitlist-controlled trial. J. Affect. Disord. 2021, 278, 327–338. [Google Scholar] [CrossRef]
- Fernández-Martínez, I.; Orgilés, M.; Morales, A.; Espada, J.P.; Essau, C.A. One-Year follow-up effects of a cognitive behavior therapy-based transdiagnostic program for emotional problems in young children: A school-based cluster-randomized controlled trial. J. Affect. Disord. 2020, 262, 258–266. [Google Scholar] [CrossRef] [PubMed]
- de la Torre-Luque, A.; Fiol-Veny, A.; Essau, C.A.; Balle, M.; Bornas, X. Effects of a transdiagnostic cognitive behaviour therapy-based programme on the natural course of anxiety symptoms in adolescence. J. Affect. Disord. 2020, 264, 474–482. [Google Scholar] [CrossRef]
- Melero, S.; Orgilés, M.; Espada, J.P.; Morales, A. Spanish version of Super Skills for Life in individual modality: Improvement of children’s emotional well-being from a transdiagnostic approach. J. Clin. Psychol. 2021, 77, 2187–2202. [Google Scholar] [CrossRef] [PubMed]
- Suveg, C.; Jones, A.; Davis, M.; Jacob, M.L.; Morelen, D.; Thomassin, K.; Whitehead, M. Emotion-Focused Cognitive-Behavioral Therapy for Youth with Anxiety Disorders: A Randomized Trial. J. Abnorm. Child Psychol. 2017, 46, 569–580. [Google Scholar] [CrossRef] [PubMed]
- Kamphaus, R.W.; Thorpe, J.S.; Winsor, A.P.; Kroncke, A.P.; Dowdy, E.T.; VanDeventer, M.C. Development and Predictive Validity of a Teacher Screener for Child Behavioral and Emotional Problems at School. Educ. Psychol. Meas. 2007, 67, 342–356. [Google Scholar] [CrossRef]
- Jensen, P.S.; Goldman, E.; Offord, D.; Costello, E.J.; Friedman, R.; Huff, B.; Crowe, M.; Amsel, L.; Bennett, K.; Bird, H.; et al. Overlooked and Underserved: ‘Action Signs’ for Identifying Children With Unmet Mental Health Needs. Pediatrics 2011, 128, 970–979. [Google Scholar] [CrossRef] [Green Version]
- MacLeod, C.; Mathews, A.; Tata, P. Attentional bias in emotional disorders. J. Abnorm. Psychol. 1986, 95, 15–20. [Google Scholar] [CrossRef]
- Davidson, M.C.; Amso, D.; Anderson, L.C.; Diamond, A. Development of cognitive control and executive functions from 4 to 13 years: Evidence from manipulations of memory, inhibition, and task switching. Neuropsychologia 2006, 44, 2037–2078. [Google Scholar] [CrossRef] [Green Version]
- Goodman, R. The Strengths and Difficulties Questionnaire: A Research Note. J. Child Psychol. Psychiatry 1997, 38, 581–586. [Google Scholar] [CrossRef]
- Birmaher, B.; Khetarpal, S.; Brent, D.; Cully, M.; Balach, L.; Kaufman, J.; Neer, S.M. The Screen for Child Anxiety Related Emotional Disorders (SCARED): Scale Construction and Psychometric Characteristics. J. Am. Acad. Child Adolesc. Psychiatry 1997, 36, 545–553. [Google Scholar] [CrossRef]
- Orgilés, M.; Melero, S.; Fernández-Martínez, I.; Espada, J.P.; Morales, A. Effectiveness of video-feedback with cognitive preparation in improving social performance and anxiety through super skills for life programme implemented in a school setting. Int. J. Environ. Res. Public Health 2020, 17, 2805. [Google Scholar] [CrossRef] [PubMed]
- Garnefski, N.; Rieffe, C.; Jellesma, F.; Terwogt, M.M.; Kraaij, V. Cognitive emotion regulation strategies and emotional problems in 9–11-year-old children: The development of an instrument. Eur. Child Adolesc. Psychiatry 2007, 16, 1–9. [Google Scholar] [CrossRef]
- Moltrecht, B.; Deighton, J.; Patalay, P.; Edbrooke-Childs, J. Effectiveness of current psychological interventions to improve emotion regulation in youth: A meta-analysis. Eur. Child Adolesc. Psychiatry 2021, 30, 829–848. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Healy, K.L.; Oei, T.P.; Shaw, S. Effectiveness of a Questionnaire Measure of Executive Function in Predicting Treatment Outcomes for Anxiety and Depression Following CBT. Sci. J. Depress. Anxiety 2018, 2, 1. [Google Scholar]
- Friedman, N.P.; Robbins, T.W. The role of prefrontal cortex in cognitive control and executive function. Neuropsychopharmacology 2021, 47, 72–89. [Google Scholar] [CrossRef] [PubMed]
- Abend, R.; Gold, A.L.; Britton, J.C.; Michalska, K.J.; Shechner, T.; Sachs, J.F.; Winkler, A.M.; Leibenluft, E.; Averbeck, B.B.; Pine, D.S. Anticipatory Threat Responding: Associations With Anxiety, Development, and Brain Structure. Biol. Psychiatry 2020, 87, 916–925. [Google Scholar] [CrossRef]
- Chavira, D.A.; Bantados, B.; Rapp, A.; Firpo-Perretti, Y.M.; Escovar, E.; Dixon, L.; Drahota, A.; Palinkas, L.A. Parent-reported stigma and child anxiety: A mixed methods research study. Child. Youth Serv. Rev. 2017, 76, 237–242. [Google Scholar] [CrossRef] [Green Version]
- Fujisawa, D.; Nakagawa, A.; Tajima, M.; Sado, M.; Kikuchi, T.; Hanaoka, M.; Ono, Y. Cognitive behavioral therapy for depression among adults in Japanese clinical settings: A single-group study. BMC Res. Notes 2010, 3, 160. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Dowdy, E.; Doane, K.; Eklund, K.; Dever, B.V. A comparison of teacher nomination and screening to identify behavioral and emotional risk within a sample of underrepresented students. J. Emot. Behav. Disord. 2011, 21, 127–137. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| Pre-Intervention Mean (SD) | Post-Intervention Mean (SD) | 3-Month Follow Up Mean (SD) | F | Ƞ2 | |
|---|---|---|---|---|---|
| SDQ | |||||
| Emotional problems | 4.24 (2.37) | 3.08 (2.77) | 3.10 (2.16) | 2.45 | 0.08 |
| Conduct problems | 3.37 (2.68) | 3.11 (2.20) | 2.90 (1.81) | 0.30 | 0.01 |
| Hyperactivity | 4.48 (2.32) | 4.14 (2.14) | 4.48 (2.13) | 0.77 | 0.01 |
| Peer problems | 3.25 (2.37) | 2.80 (1.94) | 2.67 (1.65) | 0.74 | 0.01 |
| SCARED | |||||
| Panic disorder | 6.56 (4.72) | 6.14 (5.99) | 4.40 (4.46) | 1.02 | 0.03 |
| Generalised anxiety disorder | 5.92 (3.50) | 5.51 (4.56) | 5.25 (4.01) | 0.21 | 0.01 |
| Social Anxiety | 6.04 (3.63) | 5.64 (3.85) | 5.10 (3.80) | 0.83 | 0.02 |
| Separation anxiety | 6.44 (3.70) | 5.68 (4.32) | 5.00 (4.10) | 0.64 | 0.01 |
| School avoidance | 1.53 (1.46) | 1.81 (1.77) | 1.45 (1.35) | 0.44 | 0.01 |
| CERQ | |||||
| Self-blame | 5.37 (1.80) | 4.52 (1.95) | 5.57 (2.11) | 2.62 | 0.05 |
| Rumination | 5.97 (2.21) | 5.18 (2.65) | 4.86 (1.93) | 1.91 | 0.04 |
| Catastrophising | 5.84 (2.23) | 5.66 (2.62) | 3.95 (1.69) | 4.10 ** | 0.08 |
| Other blame | 5.05 (2.36) | 4.31 (1.98) | 3.76 (1.37) | 2.96 * | 0.06 |
| Acceptance | 5.65 (2.32) | 5.09 (1.80) | 5.67 (2.08) | 0.81 | 0.02 |
| Positive refocusing | 5.38 (2.42) | 4.85 (2.30) | 4.23 (2.02) | 1.74 | 0.04 |
| Planning | 4.86 (2.22) | 4.42 (2.26) | 4.61 (2.15) | 0.72 | 0.01 |
| Putting into perspective | 5.84 (2.23) | 5.65 (2.62) | 3.95 (1.68) | 5.08 ** | 0.10 |
| Positive reappraisal | 5.81 (1.90) | 5.02 (2.33) | 5.19 (2.16) | 0.26 | 0.01 |
| Pre-Intervention Mean (SD) | Post-Intervention Mean (SD) | 3-Month Follow Up Mean (SD) | F | Ƞ2 | |
|---|---|---|---|---|---|
| Forward digit span | 8.85 (2.50) | 9.17 (1.98) | 9.88 (2.14) | 6.28 ** | 0.21 |
| Backward digit span | 3.47 (1.43) | 4.10 (2.19) | 4.12 (1.88) | 2.78 | 0.11 |
| Dot probe task | 66.30 (22.24) | 69.78 (18.53) | 95.53 (97.52) | 1.45 | 0.07 |
| Inhibition (Dot Probe) | Working Memory (Digit Span) | |||||
|---|---|---|---|---|---|---|
| Variable | b | SE | t | b | SE | t |
| Catastrophising | −0.39 | 0.21 | −1.80 | −0.49 | 0.19 | −2.53 * |
| Other blame | 0.63 | 0.19 | 3.21 * | 0.64 | 0.17 | 3.73 ** |
| Rumination | 0.15 | 0.19 | 0.81 | 0.15 | 0.17 | 0.89 |
| Self-blame | 0.23 | 0.23 | 1.01 | 0.19 | 0.20 | 0.93 |
| R2 | 0.34 | 0.44 | ||||
| F | 2.70 * | 3.98 * | ||||
| Inhibition (Dot Probe) | Working Memory (Digit Span) | |||||
|---|---|---|---|---|---|---|
| Variable | b | SE | t | b | SE | t |
| Catastrophising | 0.11 | 0.20 | 0.52 | 0.26 | 0.19 | −1.34 |
| Other blame | 0.42 | 0.18 | 2.41 * | 0.38 | 0.17 | 2.17 * |
| Rumination | −0.25 | 0.19 | −1.28 | −0.26 | 0.19 | −1.34 |
| Self-blame | −0.12 | 23 | −0.50 | −0.14 | 0.28 | 2.14 |
| R2 | 0.58 | 0.63 | ||||
| F | 2.89 * | 3.45 * | ||||
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Fernandes, B.; Wright, M.; Essau, C.A. The Role of Emotion Regulation and Executive Functioning in the Intervention Outcome of Children with Emotional and Behavioural Problems. Children 2023, 10, 139. https://doi.org/10.3390/children10010139
Fernandes B, Wright M, Essau CA. The Role of Emotion Regulation and Executive Functioning in the Intervention Outcome of Children with Emotional and Behavioural Problems. Children. 2023; 10(1):139. https://doi.org/10.3390/children10010139
Chicago/Turabian StyleFernandes, Blossom, Mark Wright, and Cecilia A. Essau. 2023. "The Role of Emotion Regulation and Executive Functioning in the Intervention Outcome of Children with Emotional and Behavioural Problems" Children 10, no. 1: 139. https://doi.org/10.3390/children10010139