
Simulated Adaptive Radiotherapy for Shrinking Glioblastoma Resection Cavities on a Hybrid MRI–Linear Accelerator
 ,
,
Abstract
:Simple Summary
Abstract
1. Introduction
2. Materials and Methods
2.1. Daily Set up Images
2.2. Patient Data Base and Analysis
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Stupp, R.; Mason, W.P.; van den Bent, M.J.; Weller, M.; Fisher, B.; Taphoorn, M.J.B.; Belanger, K.; Brandes, A.A.; Marosi, C.; Bogdahn, U.; et al. Radiotherapy plus concomitant and adjuvant temozolomide for glioblastoma. N. Engl. J. Med. 2005, 352, 987–996. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cramer, C.K.; Cummings, T.L.; Andrews, R.N.; Strowd, R.; Rapp, S.R.; Shaw, E.G.; Chan, M.D.; Lesser, G.J. Treatment of Radiation-Induced Cognitive Decline in Adult Brain Tumor Patients. Curr. Treat. Options Oncol. 2019, 20, 42. [Google Scholar] [CrossRef] [PubMed]
- Brown, P.D.; Parsons, M.W.; Rusthoven, C.G.; Gondi, V. Hippocampal Avoidance Prophylactic Cranial Irradiation: A New Standard of Care? J. Clin. Oncol. 2021, 39, 3093–3096. [Google Scholar] [CrossRef] [PubMed]
- Mutic, S.; Dempsey, J.F. The ViewRay system: Magnetic resonance-guided and controlled radiotherapy. Semin. Radiat. Oncol. 2014, 24, 196–199. [Google Scholar] [CrossRef] [PubMed]
- Noel, C.E.; Parikh, P.J.; Spencer, C.R.; Green, O.L.; Hu, Y.; Mutic, S.; Olsen, J.R. Comparison of onboard low-field magnetic resonance imaging versus onboard computed tomography for anatomy visualization in radiotherapy. Acta Oncol. 2015, 54, 1474–1482. [Google Scholar] [CrossRef]
- Spieler, B.O.; Portelance, L.; Mellon, E.A. Stereotactic ablative radiation therapy in the treatment of liver tumors. Appl. Radiat. Oncol. 2018, 7, 17–23. [Google Scholar]
- Mehta, S.; Gajjar, S.R.; Padgett, K.R.; Asher, D.; Stoyanova, R.; Ford, J.C.; Mellon, E.A. Daily Tracking of Glioblastoma Resection Cavity, Cerebral Edema, and Tumor Volume with MRI-Guided Radiation Therapy. Cureus 2018, 10, e2346. [Google Scholar] [CrossRef] [Green Version]
- Cabrera, A.R.; Kirkpatrick, J.P.; Fiveash, J.B.; Shih, H.A.; Koay, E.J.; Lutz, S.; Petit, J.; Chao, S.T.; Brown, P.D.; Vogelbaum, M.; et al. Radiation therapy for glioblastoma: Executive summary of an American Society for Radiation Oncology Evidence-Based Clinical Practice Guideline. Pract. Radiat Oncol. 2016, 6, 217–225. [Google Scholar] [CrossRef] [Green Version]
- Stewart, J.; Sahgal, A.; Lee, Y.; Soliman, H.; Tseng, C.-L.; Detsky, J.; Husain, Z.; Ho, L.; Das, S.; Maralani, P.J.; et al. Quantitating Interfraction Target Dynamics During Concurrent Chemoradiation for Glioblastoma: A Prospective Serial Imaging Study. Int. J. Radiat. Oncol. Biol. Phys. 2021, 109, 736–746. [Google Scholar] [CrossRef]
- Cullison, K.; Maziero, D.; Azzam, G.; Ford, J.; Meshman, J.J.; Prieto, P.; De La Fuente, M.; Mellon, E.A. Interfractional Dynamics of Glioblastoma Treated on MRI-Linac. Int. J. Radiat. Oncol. Biol. Phys. 2022, 114, S79. [Google Scholar] [CrossRef]
- Emami, B.; Lyman, J.; Brown, A.; Cola, L.; Goitein, M.; Munzenrider, J.E.; Shank, B.; Solin, L.J.; Wesson, M. Tolerance of normal tissue to therapeutic irradiation. Int. J. Radiat. Oncol. Biol. Phys. 1991, 21, 109–122. [Google Scholar] [CrossRef] [PubMed]
- Mayo, C.; Yorke, E.; Merchant, T.E. Radiation associated brainstem injury. Int. J. Radiat. Oncol. Biol. Phys. 2010, 76 (Suppl. S3), S36–S41. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mayo, C.; Martel, M.K.; Marks, L.B.; Flickinger, J.; Nam, J.; Kirkpatrick, J. Radiation dose-volume effects of optic nerves and chiasm. Int. J. Radiat. Oncol. Biol. Phys. 2010, 76 (Suppl. S3), S28–S35. [Google Scholar] [CrossRef] [PubMed]
- Brown, P.D.; Gondi, V.; Pugh, S.; Tome, W.A.; Wefel, J.S.; Armstrong, T.S.; Bovi, J.A.; Robinson, C.; Konski, A.; Khuntia, D.; et al. Hippocampal Avoidance During Whole-Brain Radiotherapy Plus Memantine for Patients with Brain Metastases: Phase III Trial NRG Oncology CC001. J. Clin. Oncol. 2020, 38, 1019–1029. [Google Scholar] [CrossRef]
- Batth, S.S.; Sreeraman, R.; Dienes, E.; Beckett, L.A.; Daly, M.E.; Cui, J.; Mathai, M.; Purdy, J.A.; Chen, A.M. Clinical-dosimetric relationship between lacrimal gland dose and ocular toxicity after intensity-modulated radiotherapy for sinonasal tumours. Br. J. Radiol. 2013, 86, 20130459. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- El-Bared, N.; Portelance, L.; Spieler, B.O.; Kwon, D.; Padgett, K.R.; Brown, K.M.; Mellon, E.A. Dosimetric Benefits and Practical Pitfalls of Daily Online Adaptive MRI-Guided Stereotactic Radiation Therapy for Pancreatic Cancer. Pract. Radiat Oncol. 2019, 9, e46–e54. [Google Scholar] [CrossRef]
- Gondi, V.; Hermann, B.P.; Mehta, M.P.; Tomé, W.A. Hippocampal dosimetry predicts neurocognitive function impairment after fractionated stereotactic radiotherapy for benign or low-grade adult brain tumors. Int. J. Radiat. Oncol. Biol. Phys. 2013, 85, 348–354. [Google Scholar] [CrossRef] [Green Version]
- Okoukoni, C.; McTyre, E.R.; Peacock, D.N.A.; Peiffer, A.M.; Strowd, R.; Cramer, C.; Hinson, W.H.; Rapp, S.; Metheny-Barlow, L.; Shaw, E.G.; et al. Hippocampal dose volume histogram predicts Hopkins Verbal Learning Test scores after brain irradiation. Adv. Radiat. Oncol. 2017, 2, 624–629. [Google Scholar] [CrossRef] [Green Version]
- Karunamuni, R.; Bartsch, H.; White, N.S.; Moiseenko, V.; Carmona, R.; Marshall, D.C.; Seibert, T.M.; McDonald, C.R.; Farid, N.; Krishnan, A.; et al. Dose-Dependent Cortical Thinning After Partial Brain Irradiation in High-Grade Glioma. Int. J. Radiat. Oncol. Biol. Phys. 2016, 94, 297–304. [Google Scholar] [CrossRef] [Green Version]
- Connor, M.; Karunamuni, R.; McDonald, C.; White, N.; Pettersson, N.; Moiseenko, V.; Seibert, T.; Marshall, D.; Cervino, L.; Bartsch, H.; et al. Dose-dependent white matter damage after brain radiotherapy. Radiother Oncol. 2016, 121, 209–216. [Google Scholar] [CrossRef] [Green Version]
- Weber, D.C.; Lim, P.S.; Tran, S.; Walser, M.; Bolsi, A.; Kliebsch, U.; Beer, J.; Bachtiary, B.; Lomax, T.; Pica, A. Proton therapy for brain tumours in the area of evidence-based medicine. Br. J. Radiol. 2020, 93, 20190237. [Google Scholar] [CrossRef] [PubMed]
- Brown, P.D.; Chung, C.; Liu, D.D.; McAvoy, S.; Grosshans, D.; Al Feghali, K.; Mahajan, A.; Li, J.; McGovern, S.L.; McAleer, M.-F.; et al. A prospective phase II randomized trial of proton radiotherapy vs intensity-modulated radiotherapy for patients with newly diagnosed glioblastoma. Neuro Oncol. 2021, 23, 1337–1347. [Google Scholar] [CrossRef] [PubMed]
- Mohan, R.; Liu, A.Y.; Brown, P.D.; Mahajan, A.; Dinh, J.; Chung, C.; McAvoy, S.; McAleer, M.F.; Lin, S.H.; Li, J.; et al. Proton therapy reduces the likelihood of high-grade radiation-induced lymphopenia in glioblastoma patients: Phase II randomized study of protons vs photons. Neuro Oncol. 2021, 23, 284–294. [Google Scholar] [CrossRef] [PubMed]
- Senkesen, O.; Tezcanlı, E.; Abacıoğlu, M.U.; Özen, Z.; Çöne, D.; Küçücük, H.; Göksel, E.O.; Arifoğlu, A.; Şengöz, M. Limited field adaptive radiotherapy for glioblastoma: Changes in target volume and organ at risk doses. Radiat. Oncol. J. 2022, 40, 9–19. [Google Scholar] [CrossRef]
- Matsuyama, T.; Fukugawa, Y.; Kuroda, J.; Toya, R.; Watakabe, T.; Matsumoto, T.; Oya, N. A prospective comparison of adaptive and fixed boost plans in radiotherapy for glioblastoma. Radiat. Oncol 2022, 17, 40. [Google Scholar] [CrossRef]
- Végváry, Z.; Darázs, B.; Paczona, V.; Dobi, Á.; Reisz, Z.; Varga, Z.; Fodor, E.; Cserháti, A.; Oláh, J.; Kis, D.; et al. Adaptive Radiotherapy for Glioblastoma Multiforme-The Impact on Disease Outcome. Anticancer Res. 2020, 40, 4237–4244. [Google Scholar] [CrossRef]
- Maziero, D.; Straza, M.W.; Ford, J.C.; Bovi, J.A.; Diwanji, T.; Stoyanova, R.; Paulson, E.S.; Mellon, E.A. MR-Guided Radiotherapy for Brain and Spine Tumors. Front. Oncol. 2021, 11, 626100. [Google Scholar] [CrossRef]
- FDA Drug Safety Communication: FDA Warns That Gadolinium-Based Contrast Agents (GBCAs) Are Retained in the Body; Requires New Class Warnings. Available online: https://www.fda.gov/drugs/drug-safety-and-availability/fda-drug-safety-communication-fda-warns-gadolinium-based-contrast-agents-gbcas-are-retained-body (accessed on 8 December 2022).





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| PATIENT # | SUM HIPPOCAMPUS | BRAIN | UNINVOLVED HIPPOCAMPUS | ||||
|---|---|---|---|---|---|---|---|
| Static Plan | Adaptive Plan | Static Plan | Adaptive Plan | ||||
| mean | max | mean | max | mean | mean | ||
| 1 | 23.8 | 44.4 | 11.8 | 19.9 | 23.0 | 18.5 | both |
| 2 | 12.2 | 16.8 | 8.9 | 11.2 | 14.3 | 9.7 | left |
| 3 | 2.4 | 3.7 | 2.0 | 2.9 | 13.0 | 11.2 | both |
| 4 | 11.0 | 13.7 | 7.6 | 12.1 | 26.4 | 26.0 | left |
| 5 | 4.6 | 9.6 | 3.9 | 6.9 | 19.5 | 17.9 | both |
| 6 | 10.4 | 17.0 | 7.2 | 15.6 | 19.4 | 15.9 | right |
| 7 | 22.8 | 29.2 | 16.4 | 21.5 | 22.7 | 22.4 | both |
| 8 | 13.1 | 43.6 | 9.5 | 32.4 | 21.3 | 19.2 | both |
| 9 | 12.3 | 16.2 | 8.7 | 15.1 | 14.3 | 13.7 | both |
| 10 | 12.9 | 15.9 | 8.4 | 14.5 | 32.5 | 32.1 | right |
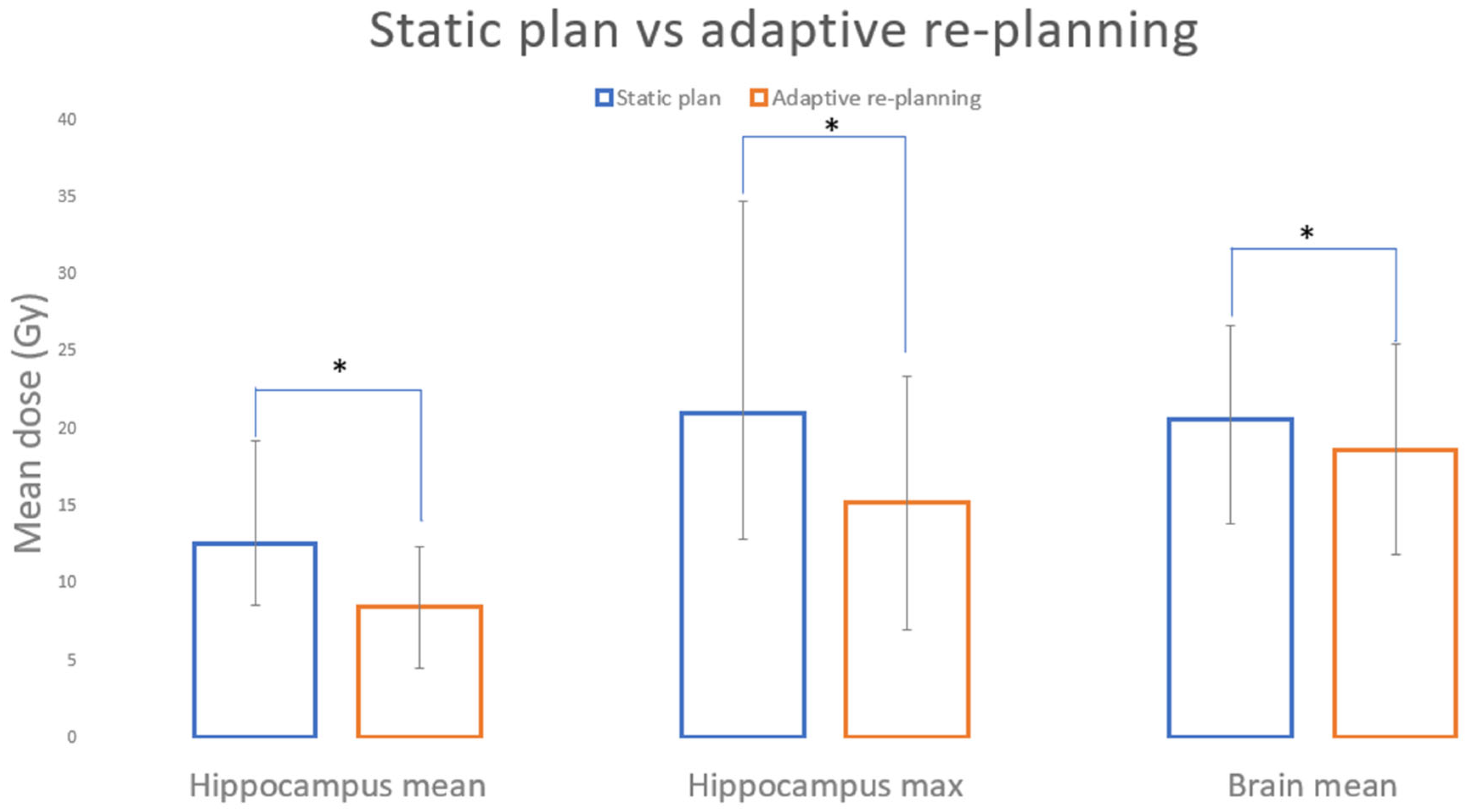
| STATIC PLAN (SP) | ADAPTIVE RE-PLANNING | STDEV SP | STDEV AP | p-VALUES | |
|---|---|---|---|---|---|
| Hippocampus mean | 12.5 | 8.4 | 6.7 | 3.96 | 0.003 |
| Hippocampus max | 21 | 15.2 | 13.7 | 8.19 | 0.036 |
| Brain mean | 20.6 | 18.7 | 6.0 | 6.81 | 0.005 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Guevara, B.; Cullison, K.; Maziero, D.; Azzam, G.A.; De La Fuente, M.I.; Brown, K.; Valderrama, A.; Meshman, J.; Breto, A.; Ford, J.C.; et al. Simulated Adaptive Radiotherapy for Shrinking Glioblastoma Resection Cavities on a Hybrid MRI–Linear Accelerator. Cancers 2023, 15, 1555. https://doi.org/10.3390/cancers15051555
Guevara B, Cullison K, Maziero D, Azzam GA, De La Fuente MI, Brown K, Valderrama A, Meshman J, Breto A, Ford JC, et al. Simulated Adaptive Radiotherapy for Shrinking Glioblastoma Resection Cavities on a Hybrid MRI–Linear Accelerator. Cancers. 2023; 15(5):1555. https://doi.org/10.3390/cancers15051555
Chicago/Turabian StyleGuevara, Beatriz, Kaylie Cullison, Danilo Maziero, Gregory A. Azzam, Macarena I. De La Fuente, Karen Brown, Alessandro Valderrama, Jessica Meshman, Adrian Breto, John Chetley Ford, and et al. 2023. "Simulated Adaptive Radiotherapy for Shrinking Glioblastoma Resection Cavities on a Hybrid MRI–Linear Accelerator" Cancers 15, no. 5: 1555. https://doi.org/10.3390/cancers15051555