
Response to First-Line Treatment with Immune-Checkpoint Inhibitors in Patients with Advanced Cutaneous Squamous Cell Carcinoma: A Multicenter, Retrospective Analysis from the German ADOReg Registry
 , , , , , , , ,
, , , , , , , ,  , and
, and
Abstract
:Simple Summary
Abstract
1. Introduction
2. Materials and Methods
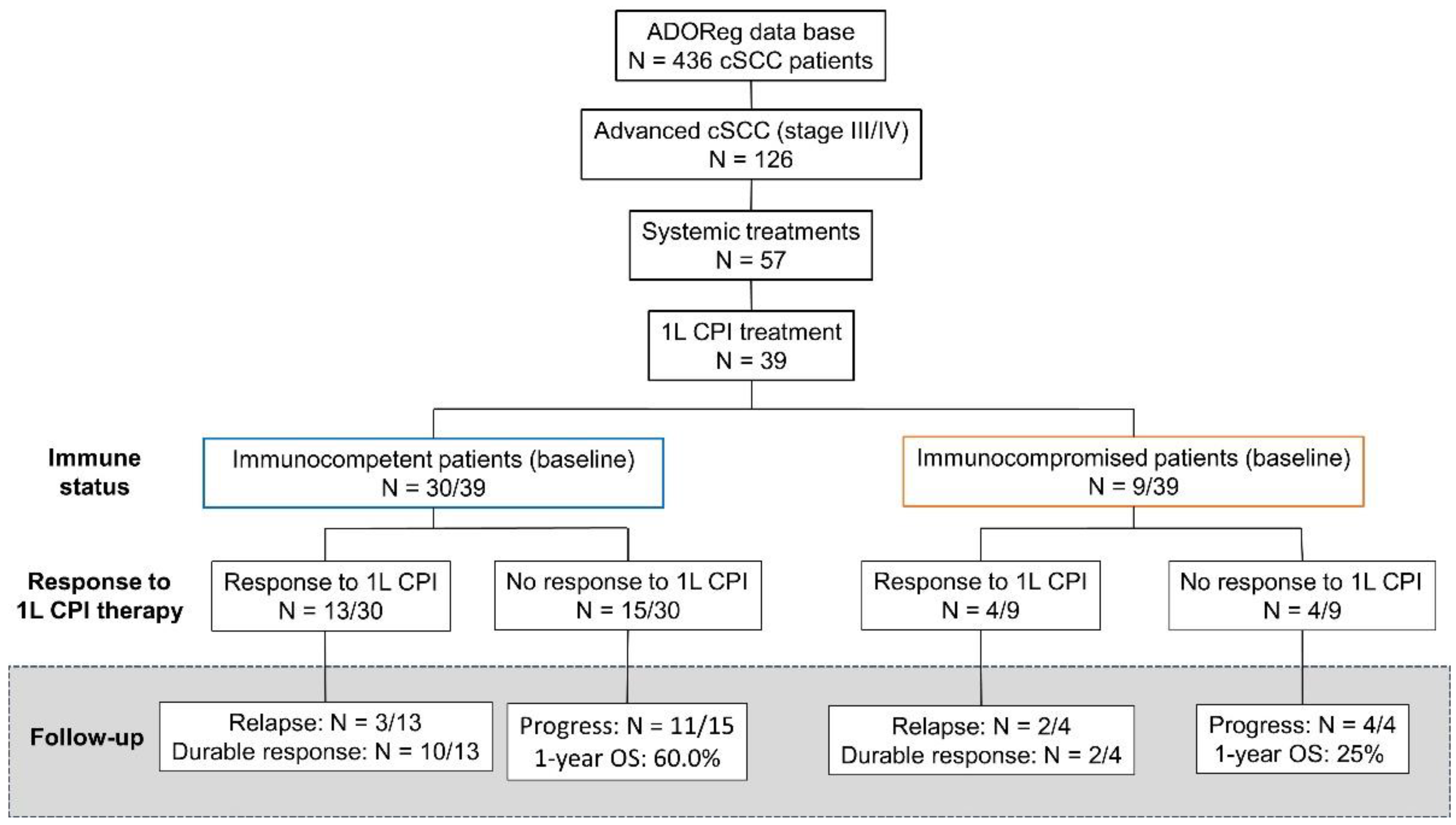
2.1. Study Design and Data Source
2.2. Patient Cohort
2.3. Statistical Analysis
3. Results
3.1. Baseline Patient Characteristics
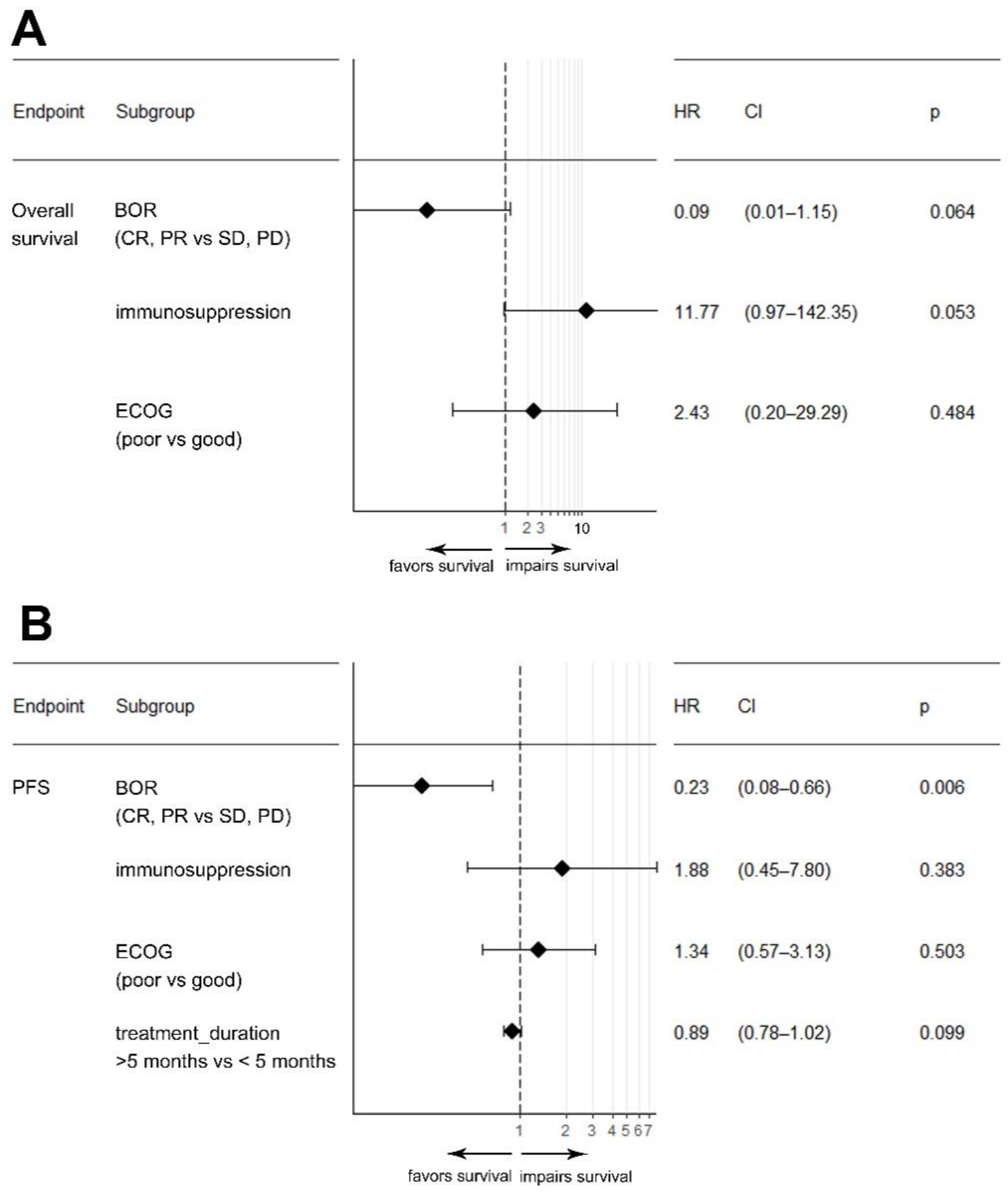
3.2. Clinical and Pathological Factors Associated with Response and Survival upon CPI Therapy
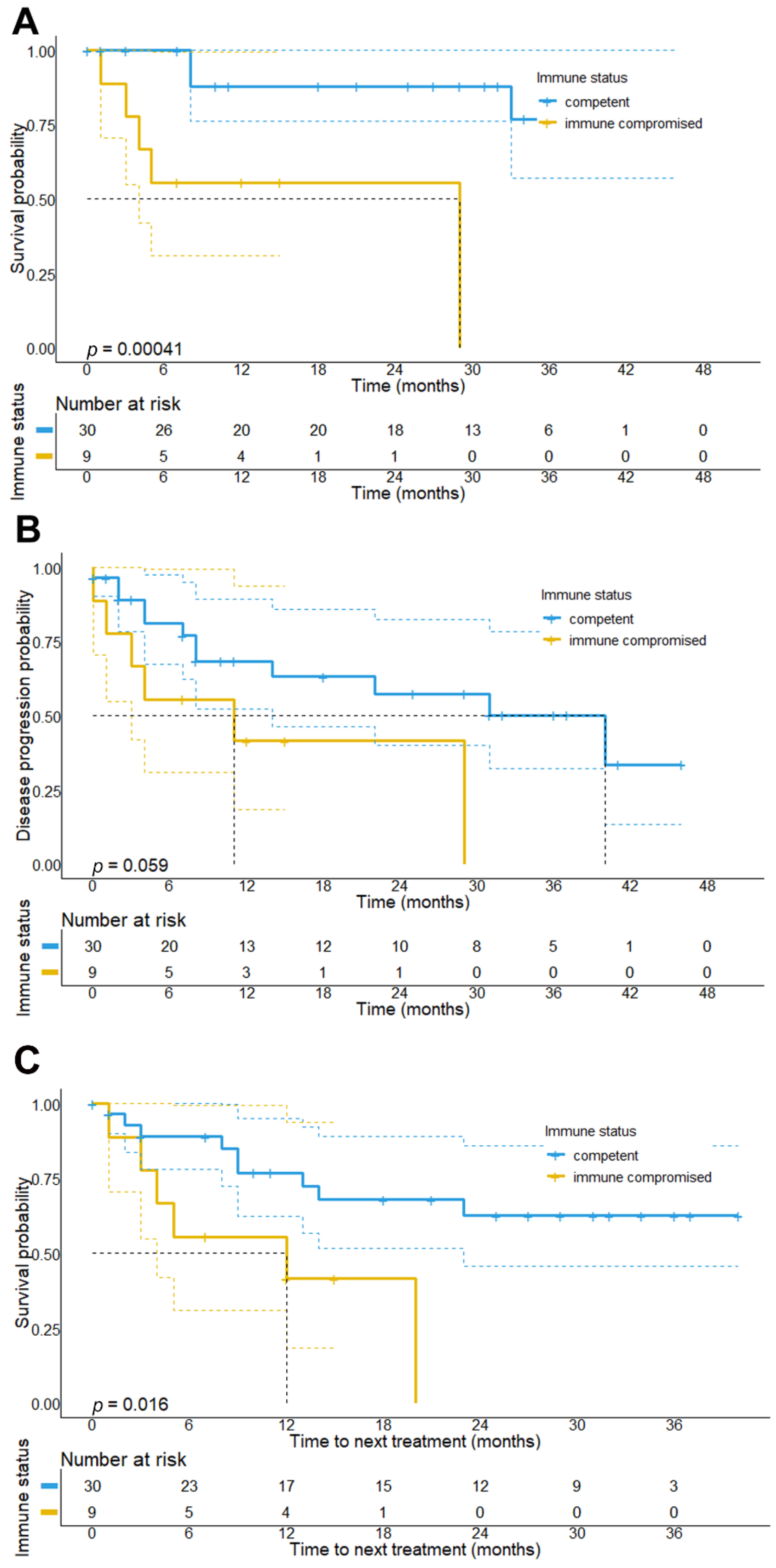
3.3. Response and Survival upon CPI Therapy in Immunocompromised Patients
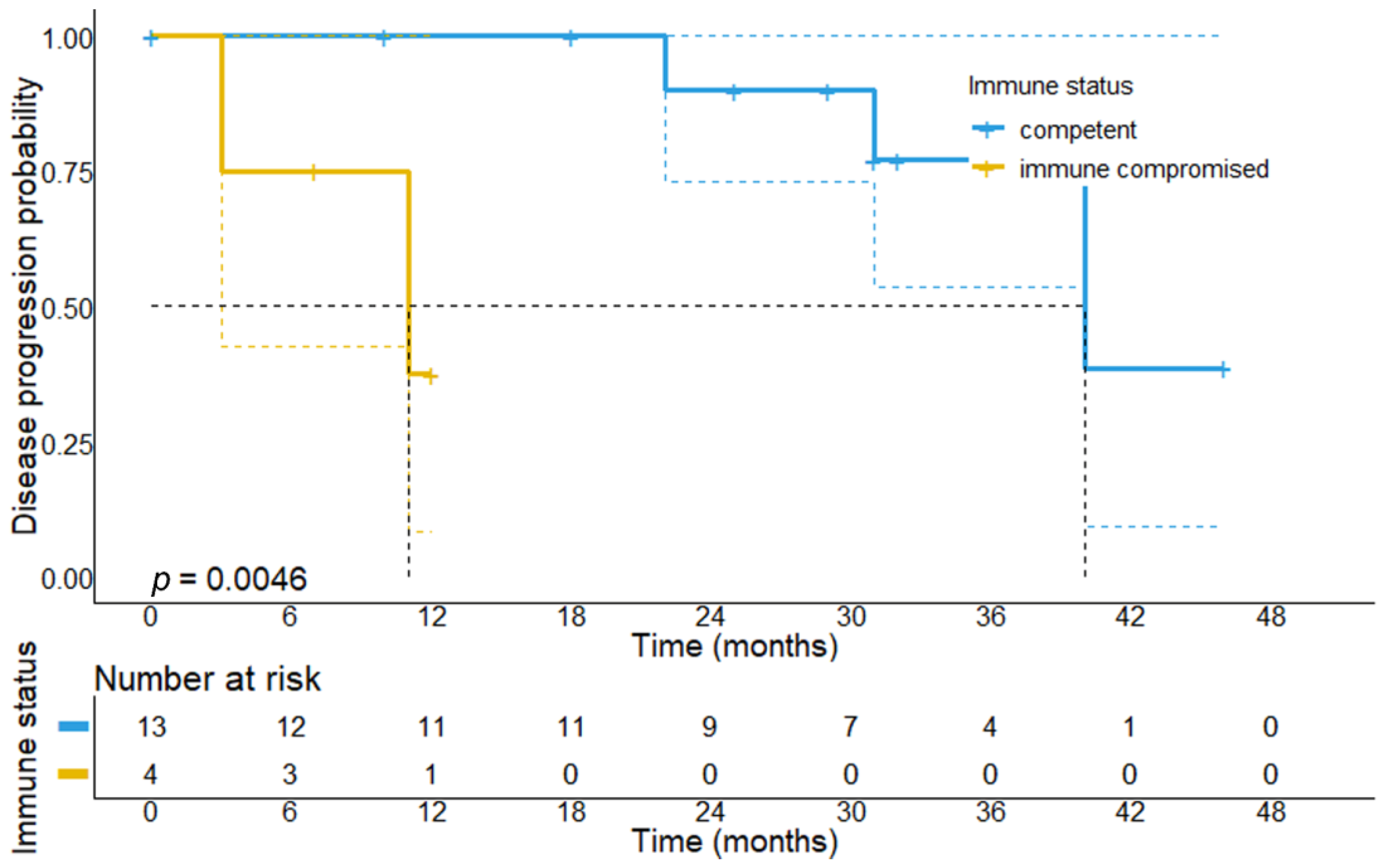
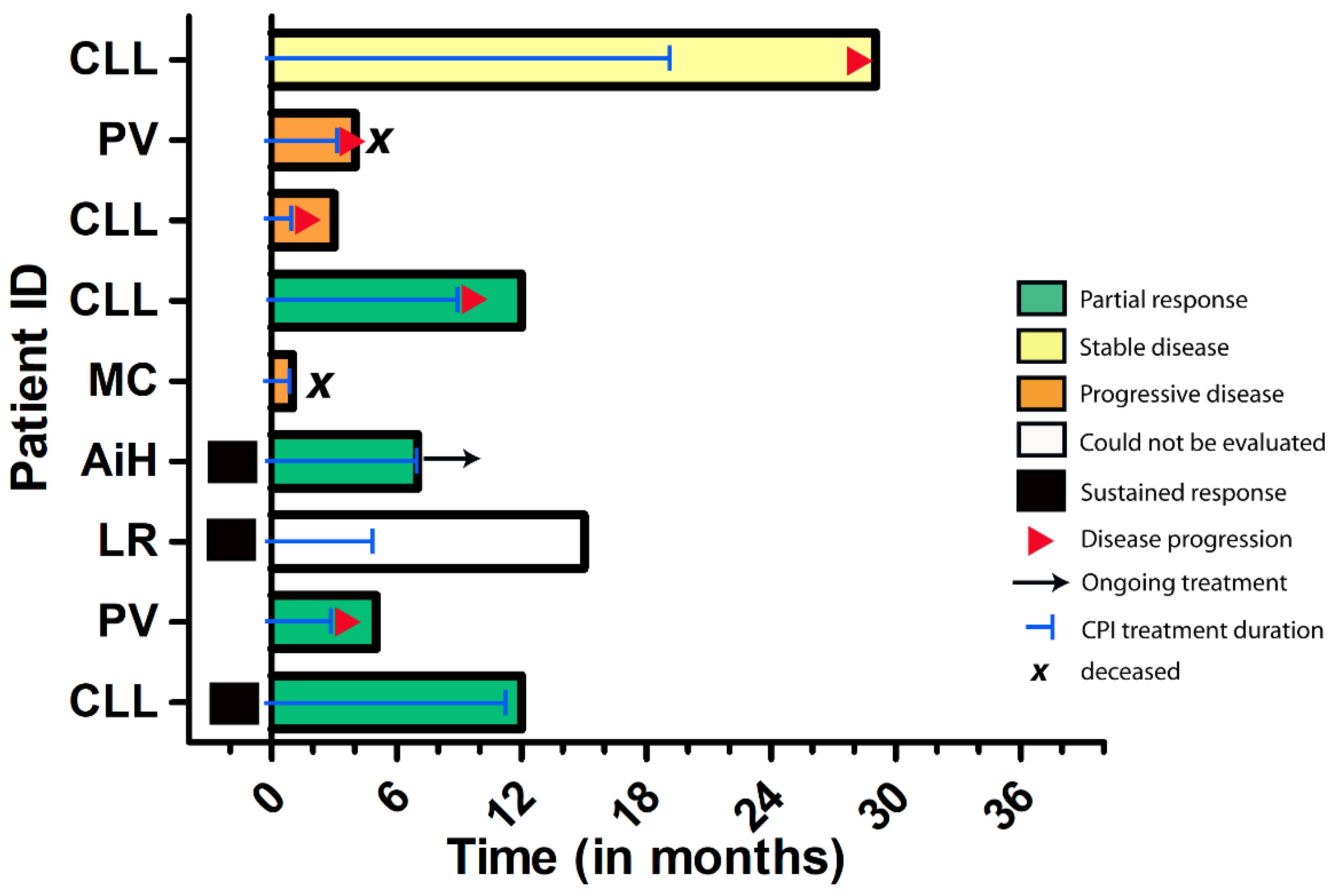
3.4. Duration of CPI Treatment Response in Immunocompromised Patients
3.5. Durable Response upon CPI Cessation and Efficacy of CPI Re-Challenge
3.6. Treatment-Related Adverse Events during CPI Therapy
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Abbreviations
| AE | Adverse events |
| AID | Autoimmune disease |
| AiH | Autoimmune hepatitis |
| CI | Confidence interval |
| CPI | Immune-checkpoint inhibitors |
| CR | Complete response |
| ECOG | Eastern Cooperative Oncology Group |
| 1 L | First-line |
| HR | Hazard ratio |
| trAE | Treatment-related adverse events |
| NED | No evidence of disease |
| OS | Overall survival |
| PD | Progressive disease |
| PD-1 | Programmed death protein 1 |
| PD-L1 | Programmed death protein ligand 1 |
| PFS | Progression-free survival |
| PR | Partial response |
| rwTCR | Real-world tumor control rate |
| rwTR | Real-world tumor response |
| rwTRR | Real-world tumor response rate |
| SD | Stable disease |
References
- Rogers, H.W.; Weinstock, M.A.; Feldman, S.R.; Coldiron, B.M. Incidence Estimate of Nonmelanoma Skin Cancer (Keratinocyte Carcinomas) in the U.S. Population, 2012. JAMA Dermatol. 2015, 151, 1081–1086. [Google Scholar] [CrossRef] [PubMed]
- Leiter, U.; Keim, U.; Eigentler, T.; Katalinic, A.; Holleczek, B.; Martus, P.; Garbe, C. Incidence, Mortality, and Trends of Nonmelanoma Skin Cancer in Germany. J. Investig. Dermatol. 2017, 137, 1860–1867. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- In, G.K.; Vaidya, P.; Filkins, A.; Hermel, D.J.; King, K.G.; Ragab, O.; Tseng, W.W.; Swanson, M.; Kokot, N.; Lang, J.E.; et al. PD-1 inhibition therapy for advanced cutaneous squamous cell carcinoma: A retrospective analysis from the University of Southern California. J. Cancer Res. Clin. Oncol. 2021, 147, 1803–1811. [Google Scholar] [CrossRef] [PubMed]
- Hillen, U.; Leiter, U.; Haase, S.; Kaufmann, R.; Becker, J.; Gutzmer, R.; Terheyden, P.; Krause-Bergmann, A.; Schulze, H.J.; Hassel, J.; et al. Advanced cutaneous squamous cell carcinoma: A retrospective analysis of patient profiles and treatment patterns-Results of a non-interventional study of the DeCOG. Eur. J. Cancer 2018, 96, 34–43. [Google Scholar] [CrossRef] [PubMed]
- Petzold, A.; Steeb, T.; Wessely, A.; Schatton, T.; Berking, C.; Heppt, M.V. Comparative efficacy analysis identifies immune checkpoint blockade as a new survival benchmark in advanced cutaneous squamous cell carcinoma. Eur. J. Cancer 2022, 170, 42–53. [Google Scholar] [CrossRef] [PubMed]
- Salzmann, M.; Leiter, U.; Loquai, C.; Zimmer, L.; Ugurel, S.; Gutzmer, R.; Thoms, K.M.; Enk, A.H.; Hassel, J.C. Programmed cell death protein 1 inhibitors in advanced cutaneous squamous cell carcinoma: Real-world data of a retrospective, multicenter study. Eur. J. Cancer 2020, 138, 125–132. [Google Scholar] [CrossRef]
- Migden, M.R.; Khushalani, N.I.; Chang, A.L.S.; Lewis, K.D.; Schmults, C.D.; Hernandez-Aya, L.; Meier, F.; Schadendorf, D.; Guminski, A.; Hauschild, A.; et al. Cemiplimab in locally advanced cutaneous squamous cell carcinoma: Results from an open-label, phase 2, single-arm trial. Lancet Oncol. 2020, 21, 294–305. [Google Scholar] [CrossRef]
- Migden, M.R.; Rischin, D.; Schmults, C.D.; Guminski, A.; Hauschild, A.; Lewis, K.D.; Chung, C.H.; Hernandez-Aya, L.; Lim, A.M.; Chang, A.L.S.; et al. PD-1 Blockade with Cemiplimab in Advanced Cutaneous Squamous-Cell Carcinoma. N. Engl. J. Med. 2018, 379, 341–351. [Google Scholar] [CrossRef] [Green Version]
- Hughes, B.G.M.; Munoz-Couselo, E.; Mortier, L.; Bratland, Å.; Gutzmer, R.; Roshdy, O.; González Mendoza, R.; Schachter, J.; Arance, A.; Grange, F.; et al. Pembrolizumab for locally advanced and recurrent/metastatic cutaneous squamous cell carcinoma (KEYNOTE-629 study): An open-label, nonrandomized, multicenter, phase II trial. Ann. Oncol. 2021, 32, 1276–1285. [Google Scholar] [CrossRef]
- Maubec, E.; Boubaya, M.; Petrow, P.; Beylot-Barry, M.; Basset-Seguin, N.; Deschamps, L.; Grob, J.J.; Dréno, B.; Scheer-Senyarich, I.; Bloch-Queyrat, C.; et al. Phase II Study of Pembrolizumab As First-Line, Single-Drug Therapy for Patients with Unresectable Cutaneous Squamous Cell Carcinomas. J. Clin. Oncol. 2020, 38, 3051–3061. [Google Scholar] [CrossRef]
- Amaral, T.; Osewold, M.; Presser, D.; Meiwes, A.; Garbe, C.; Leiter, U. Advanced cutaneous squamous cell carcinoma: Real world data of patient profiles and treatment patterns. J. Eur. Acad. Dermatol. Venereol. 2019, 33 (Suppl. S8), 44–51. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Baggi, A.; Quaglino, P.; Rubatto, M.; Depenni, R.; Guida, M.; Ascierto, P.A.; Trojaniello, C.; Queirolo, P.; Saponara, M.; Peris, K.; et al. Real world data of cemiplimab in locally advanced and metastatic cutaneous squamous cell carcinoma. Eur. J. Cancer 2021, 157, 250–258. [Google Scholar] [CrossRef] [PubMed]
- Hober, C.; Fredeau, L.; Ledard, A.P.; Boubaya, M.; Herms, F.; Aubin, F.; Benetton, N.; Dinulescu, M.; Jannic, A.; Cesaire, L.; et al. 1086P Cemiplimab for advanced cutaneous squamous cell carcinoma: Real life experience. Ann. Oncol. 2020, 31, S737. [Google Scholar] [CrossRef]
- Migden, M.R.; Chandra, S.; Rabinowits, G.; Chen, C.I.; Desai, J.; Seluzhytsky, A.; Sasane, M.; Campanelli, B.; Chen, Z.; Freeman, M.L.; et al. CASE (CemiplimAb-rwlc Survivorship and Epidemiology) study in advanced cutaneous squamous cell carcinoma. Future Oncol. 2020, 16, 11–19. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Leiter, U.; Weichenthal, M. ADOReg–wissenschaftliches Register der Arbeitsgemeinschaft Dermatologische Onkologie. JDDG J. Dtsch. Dermatol. Ges. 2014, 12, 1156–1157. [Google Scholar]
- Mohr, P.; Scherrer, E.; Assaf, C.; Bender, M.; Berking, C.; Chandwani, S.; Eigentler, T.; Grimmelmann, I.; Gutzmer, R.; Haferkamp, S.; et al. Real-World Therapy with Pembrolizumab: Outcomes and Surrogate Endpoints for Predicting Survival in Advanced Melanoma Patients in Germany. Cancers 2022, 14, 1804. [Google Scholar] [CrossRef]
- Rischin, D.; Khushalani, N.I.; Schmults, C.D.; Guminski, A.D.; Chang, A.L.S.; Lewis, K.D.; Lim, A.M.L.; Hernandez-Aya, L.F.; Hughes, B.G.M.; Schadendorf, D.; et al. Phase II study of cemiplimab in patients (pts) with advanced cutaneous squamous cell carcinoma (CSCC): Longer follow-up. J. Clin. Oncol. 2020, 38, 10018. [Google Scholar] [CrossRef]
- Hodi, F.S.; Chiarion-Sileni, V.; Gonzalez, R.; Grob, J.J.; Rutkowski, P.; Cowey, C.L.; Lao, C.D.; Schadendorf, D.; Wagstaff, J.; Dummer, R.; et al. Nivolumab plus ipilimumab or nivolumab alone versus ipilimumab alone in advanced melanoma (CheckMate 067): 4-year outcomes of a multicentre, randomised, phase 3 trial. Lancet Oncol. 2018, 19, 1480–1492. [Google Scholar] [CrossRef]
- Cheng, J.Y.; Li, F.Y.; Ko, C.J.; Colegio, O.R. Cutaneous Squamous Cell Carcinomas in Solid Organ Transplant Recipients Compared With Immunocompetent Patients. JAMA Dermatol. 2018, 154, 60–66. [Google Scholar] [CrossRef]
- Leiter, U.; Loquai, C.; Reinhardt, L.; Rafei-Shamsabadi, D.; Gutzmer, R.; Kaehler, K.; Heinzerling, L.; Hassel, J.C.; Glutsch, V.; Sirokay, J.; et al. Immune checkpoint inhibition therapy for advanced skin cancer in patients with concomitant hematological malignancy: A retrospective multicenter DeCOG study of 84 patients. J. Immunother. Cancer 2020, 8, e000897. [Google Scholar] [CrossRef]
- Fisher, J.; Zeitouni, N.; Fan, W.; Samie, F.H. Immune checkpoint inhibitor therapy in solid organ transplant recipients: A patient-centered systematic review. J. Am. Acad. Dermatol. 2020, 82, 1490–1500. [Google Scholar] [CrossRef] [PubMed]
- Gutzmer, R.; Koop, A.; Meier, F.; Hassel, J.C.; Terheyden, P.; Zimmer, L.; Heinzerling, L.; Ugurel, S.; Pfohler, C.; Gesierich, A.; et al. Programmed cell death protein-1 (PD-1) inhibitor therapy in patients with advanced melanoma and preexisting autoimmunity or ipilimumab-triggered autoimmunity. Eur. J. Cancer 2017, 75, 24–32. [Google Scholar] [CrossRef] [PubMed]
- Kahler, K.C.; Eigentler, T.K.; Gesierich, A.; Heinzerling, L.; Loquai, C.; Meier, F.; Meiss, F.; Pfohler, C.; Schlaak, M.; Terheyden, P.; et al. Ipilimumab in metastatic melanoma patients with pre-existing autoimmune disorders. Cancer Immunol. Immunother. 2018, 67, 825–834. [Google Scholar] [CrossRef] [PubMed]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Clinicopathological Characteristics | Overall Patient Cohort | Immunocompetent Patients | Immunocompromised Patients | p Value |
|---|---|---|---|---|
| Number of patients | 39 | 30 | 9 | |
| A Demographics | ||||
| Age at CPI initiation (median, range) | 79 years (55–96) | 79.5 years (55–96) | 79.0 years (61–87) | 0.812 |
| Gender | 0.607 | |||
| Female | 6 (15.4%) | 4 (13.3%) | 2 (22.2%) | |
| Male | 33 (84.6%) | 26 (86.7%) | 7 (77.8%) | |
| Median ECOG performance status1 | 0.062 | |||
| Good performance status (ECOG ≤ 1) | 17 (60.7%) | 16 (69.6%) | 1 (20%) | |
| Poor performance status (ECOG > 1) | 11 (39.2%) | 7 (30.4%) | 4 (80%) | |
| Primary site of disease | 0.604 | |||
| Head and neck | 25 (64.1%) | 19 (63.3%) | 6 (66.7%) | |
| Limb | 8 (20.5%) | 6 (20.0%) | 2 (22.2%) | |
| Trunk | 4 (10.3%) | 4 (13.3%) | 0 | |
| Genitoanal area | 2 (5.1%) | 1 (3.3%) | 1 (11.1%) | |
| Immunosuppression | NA | |||
| None | 30 (76.9%) | 30 | 0 | |
| Autoimmune disease | 2 (5.1%) | 0 | 2 (22.2%) | |
| Hematological disease | 6 (15.4%) | 0 | 6 (66.7%) | |
| Other (immunosuppressive medication) | 1 (2.6%) | 0 | 1 (11.1%) | |
| Initial stage at diagnosis2 | 0.451 | |||
| Stages I and II | 17 (43.6%) | 15 (50.0%) | 2 (22.2%) | |
| Stages III and IV | 20 (51.3%) | 14 (46.7%) | 6 (66.7%) | |
| Unknown | 2 (5.1%) | 1 (3.3%) | 1 (11.1%) | |
| High-risk features | 0.168 | |||
| Diameter > 2 cm 3 | 8 (20.5%) | 4 (13.3%) | 4 (44.4%) | |
| Vertical thickness > 6 mm 4 | 8 (20.5%) | 5 (16.7%) | 3 (33.3%) | |
| Poorly differentiated histology 5 | 12 (30.8%) | 11 (36.7%) | 1 (11.1%) | |
| Other pathological risk factors 6 | 5 (12.8%) | 5 (16.7%) | 0 | |
| Time to metastasis (median, range) | 8 months (0–72) | 12 months (0–72) | 1.0 month (0–19) | 0.023 |
| Extent of disease7 | 0.518 | |||
| Locally advanced | 7 (17.9%) | 7 (23.3%) | 0 | |
| Regional metastasis | 21 (53.8%) | 15 (50.0%) | 6 (66.7%) | |
| Distant metastases | 9 (23.1%) | 7 (23.3%) | 2 (22.2%) | |
| NA | 2 (5.2%) | 1 (3.3%) | 1 (11.1%) | |
| Anatomic sites of metastasis | 0.399 | |||
| Lymphatic tissue | 23 (59.0%) | 17 (56.7%) | 6 (66.7%) | |
| Soft tissue/skin | 12 (30.8%) | 8 (26.7%) | 4 (44.4%) | |
| Bone | 4 (10.3%) | 3 (10.0%) | 1 (11.1%) | |
| Lung | 4 (10.3%) | 2 (6.7%) | 2 (22.2%) | |
| (Lepto-)meningeal | 3 (7.7%) | 3 (10.0%) | 0 | |
| Other (mucosal, intraorbital) | 3 (7.7%) | 3 (10.0%) | 0 | |
| Baseline LDH levels8 | 1.0 | |||
| Normal (<245 U/l) | 19 (48.7%) | 15 (50.0%) | 4 (44.4%) | |
| Elevated (>245 U/l) | 15 (38.5%) | 12 (40.0%) | 3 (33.3%) | |
| B Treatments | ||||
| Initial treatment regimen for advanced disease | 0.06 | |||
| Surgery alone | 9 (23.1%) | 9 (30.0%) | 0 | |
| Definitive RTx | 9 (23.1%) | 8 (26.7%) | 1 (11.1%) | |
| Surgery + RTx | 20 (51.3%) | 12 (40.0%) | 8 (88.9%) | |
| None | 1 (2.6%) | 1 (3.3%) | 0 | |
| CPI regimens | 0.387 | |||
| Nivolumab | 10 (25.6%) | 8 (26.7%) | 2 (22.2%) | |
| Pembrolizumab | 9 (23.1%) | 7 (23.3%) | 2 (22.2%) | |
| Avelumab | 1 (2.6%) | 0 | 1 (11.1%) | |
| Cemiplimab | 19 (48.7%) | 15 (50.0%) | 4 (44.4%) | |
| Real-world tumor responses | 0.093 | |||
| Progressive disease, PD | 7 (20.0%) | 4 (14.8%) | 3 (37.5%) | |
| Stable disease, SD | 11 (28.9%) | 10 (37.0%) | 1 (12.5%) | |
| Partial response, PR | 10 (28.5%) | 6 (22.2%) | 4 (50%) | |
| Complete response, CR | 7 (20.0%) | 7 (25.9%) | 0 | |
| Not assessed 9 | 4 | 3 | 1 | |
| Median duration of CPI treatment | 5 months (0–29) | 4.5 months (0–29) | 5.0 months (0–19) | 0.98 |
| Treatment-related adverse events | 12 (34.3%) | 9 (30.0%) | 4 (44.4%) | 0.689 |
| Serious adverse events | 7 (17.9%) | 4 (13.3%) | 3 (33.3%) | 0.319 |
| Discontinuation due to trAE | 7 (15.4%) | 4 (13.3%) | 2 (22.2%) | 0.653 |
| Subsequent treatments | 1.0 | |||
| Re-induction of CPI therapy | 8 (20.5%) | 7 (23.3%) | 1 (11.1%) | |
| EGFR-inhibitor | 2 | 0 | 2 | |
| Chemotherapy | 1 | 1 | 0 | |
| C Survival outcomes | ||||
| Median overall survival (95% CI) | Not reached | Not reached | 29.0 months | <0.001 |
| 1-year OS | 32 (82.1%) | 27 (90%) | 5 (55.5%) | |
| Deceased | 9 (23.1%) | 4 (13.3%) | 5 (55.6%) | 0.018 |
| Median progression-free survival (95% CI) | 29.0 months (8.6–49.4) | 40.0 months (16.9–63.1) | 11.0 months (0–28.1) | 0.059 |
| Disease progression or relapse | 18 (46.2%) | 12 (40%) | 6 (66.7%) | 0.255 |
| Median follow-up period (95% CI) | 27.0 months (21.7–32.2) | 29.0 months (24.0–34.0) | 12.0 months (6.6–17.4) | 0.242 |
| AID | AID-Status at CPI Start | Concomitant Medication 30 d Prior to CPI Initiation | Steroids during CPI | AE during CPI Therapy | AE Resolved? | Permanent CPI Cessation? | BOR to CPI |
|---|---|---|---|---|---|---|---|
| Crohn´s disease | Acute relapse | Mesalazine 2 g/d Prednisolone > 10 mg/d | No | Anaphylactic shock | Yes | Yes | PD |
| AiH | Active | Prednisolone 10 mg/d Azathioprine 1 mg/kg bw | Yes | Pancytopenia grade 3 | Yes | No | PR |
| Lichen planus mucosae | Active | Prednisolone >10 mg/d Acitretin 0.5 mg/kg bw Topical Betamethasone | No | Pneumonitis grade 2 | Yes | Yes | PR |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Haist, M.; Stege, H.; Lang, B.M.; Tsochataridou, A.; Salzmann, M.; Mohr, P.; Schadendorf, D.; Ugurel, S.; Placke, J.-M.; Weichenthal, M.; et al. Response to First-Line Treatment with Immune-Checkpoint Inhibitors in Patients with Advanced Cutaneous Squamous Cell Carcinoma: A Multicenter, Retrospective Analysis from the German ADOReg Registry. Cancers 2022, 14, 5543. https://doi.org/10.3390/cancers14225543
Haist M, Stege H, Lang BM, Tsochataridou A, Salzmann M, Mohr P, Schadendorf D, Ugurel S, Placke J-M, Weichenthal M, et al. Response to First-Line Treatment with Immune-Checkpoint Inhibitors in Patients with Advanced Cutaneous Squamous Cell Carcinoma: A Multicenter, Retrospective Analysis from the German ADOReg Registry. Cancers. 2022; 14(22):5543. https://doi.org/10.3390/cancers14225543
Chicago/Turabian StyleHaist, Maximilian, Henner Stege, Berenice Mareen Lang, Aikaterini Tsochataridou, Martin Salzmann, Peter Mohr, Dirk Schadendorf, Selma Ugurel, Jan-Malte Placke, Michael Weichenthal, and et al. 2022. "Response to First-Line Treatment with Immune-Checkpoint Inhibitors in Patients with Advanced Cutaneous Squamous Cell Carcinoma: A Multicenter, Retrospective Analysis from the German ADOReg Registry" Cancers 14, no. 22: 5543. https://doi.org/10.3390/cancers14225543