
Lobe-Specific Analysis of Sublobar Lung Resection for NSCLC Patients with Tumors ≤ 2 cm

 , ,
, ,
Abstract
:Simple Summary
Abstract
1. Introduction
2. Materials and Methods
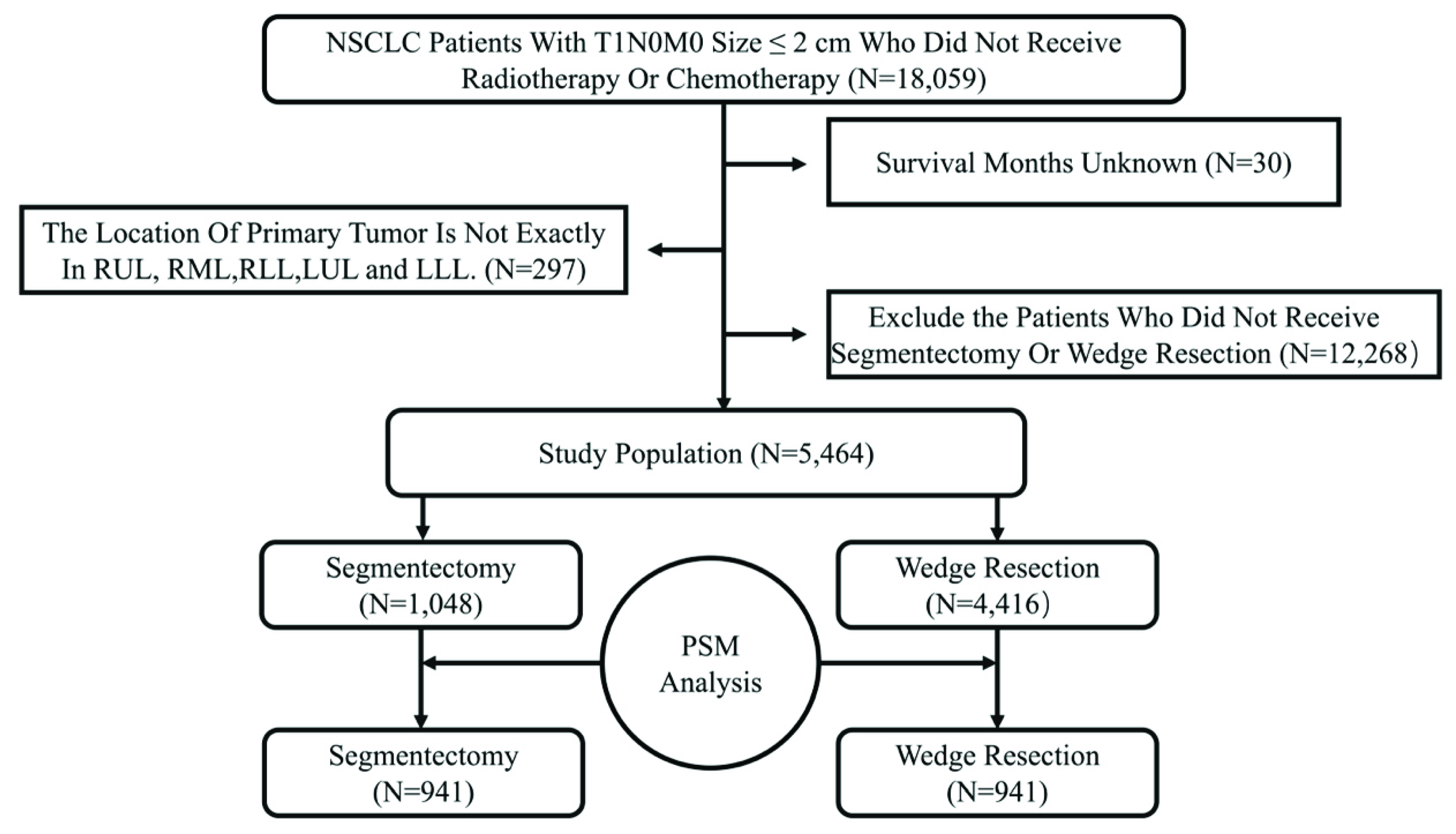
2.1. Patient Selection
2.2. Statistical Analysis
3. Results
3.1. Patient Characteristics
3.2. Surgical Outcome Analysis
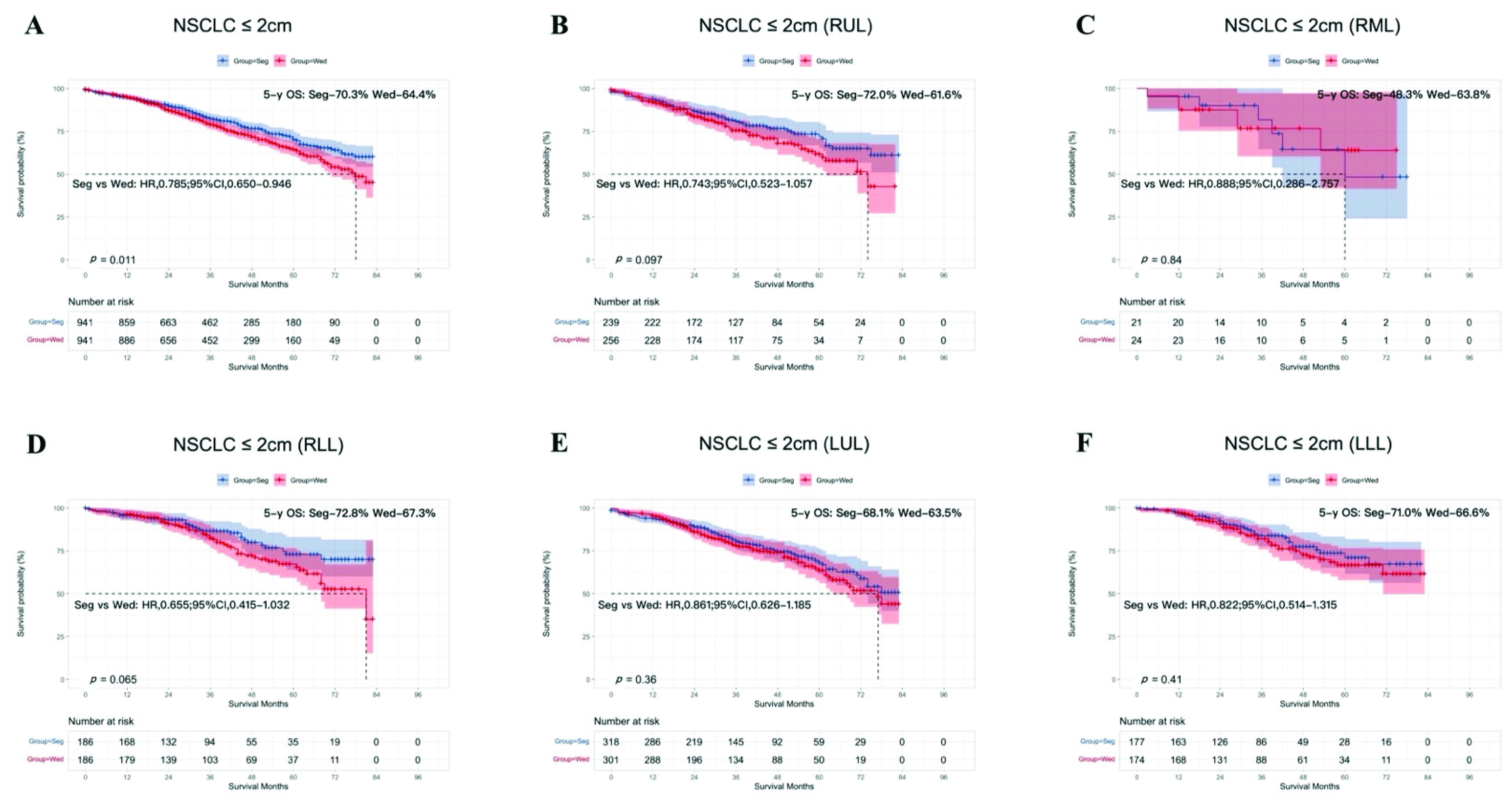
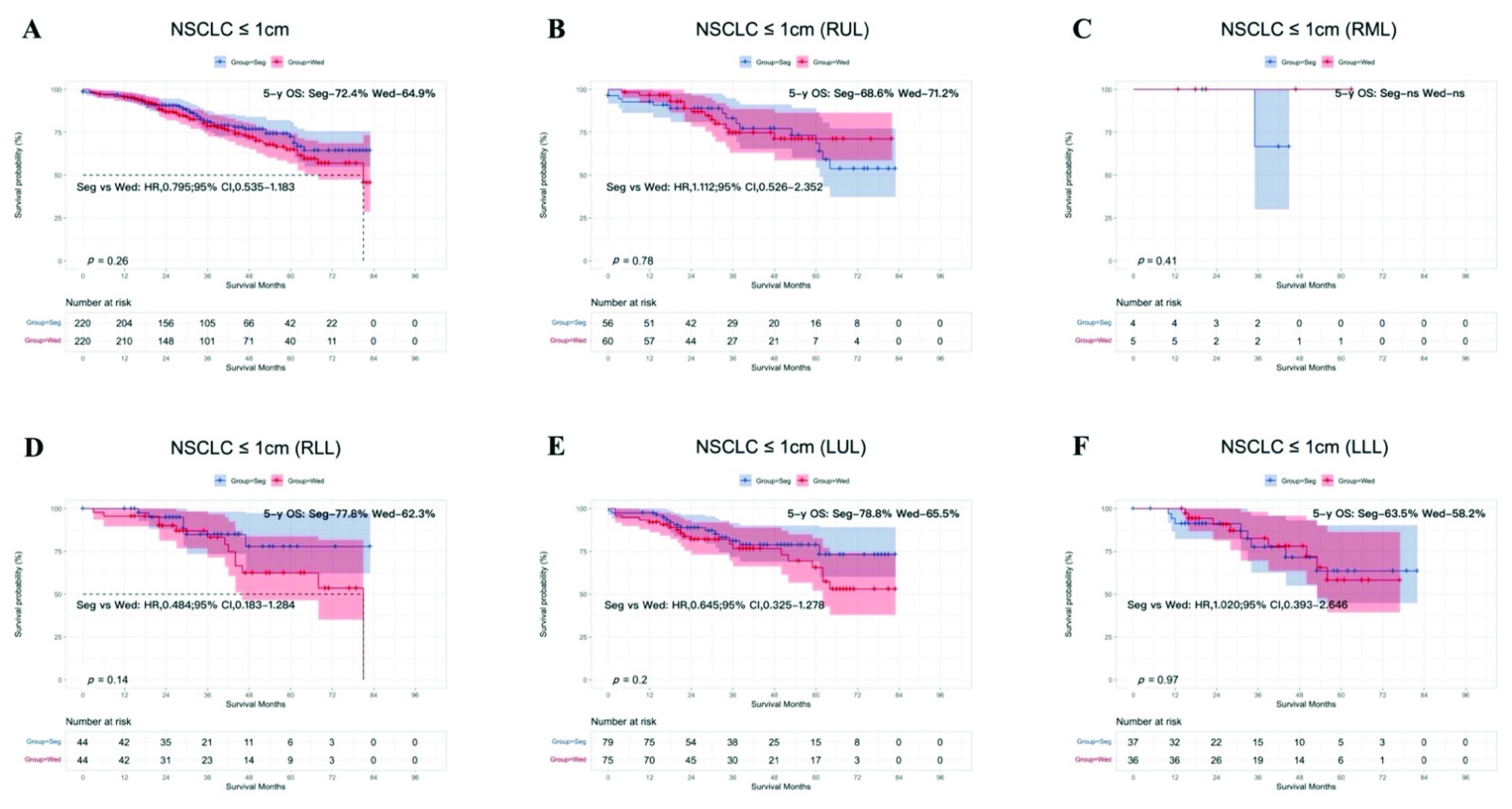
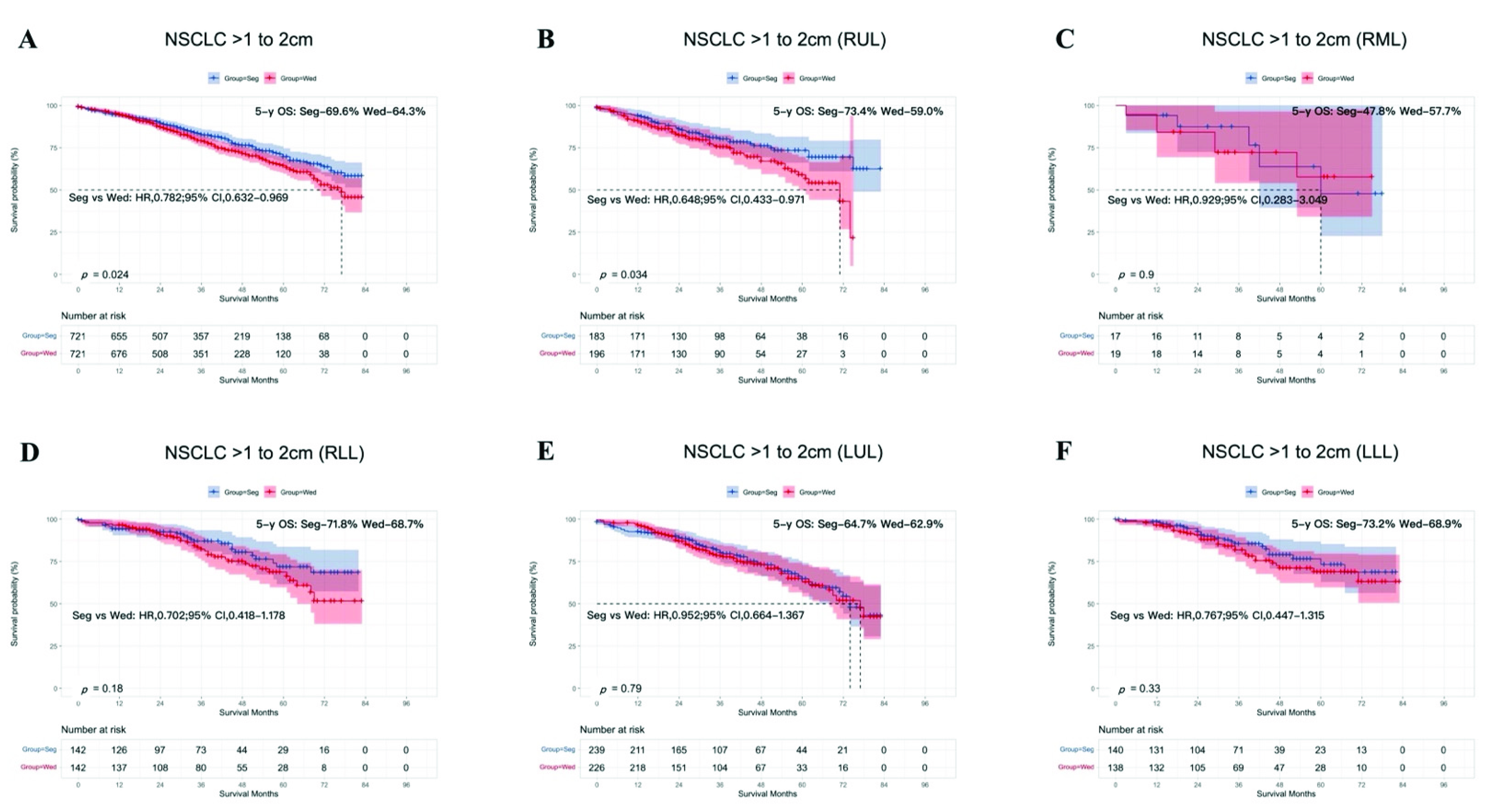
3.3. Subgroup Analysis According to Tumor Size
3.4. Subgroup Analysis According to Age after PSM
3.5. Subgroup Analysis According to Histological Type after PSM
3.6. Subgroup Analysis According to Sex after PSM
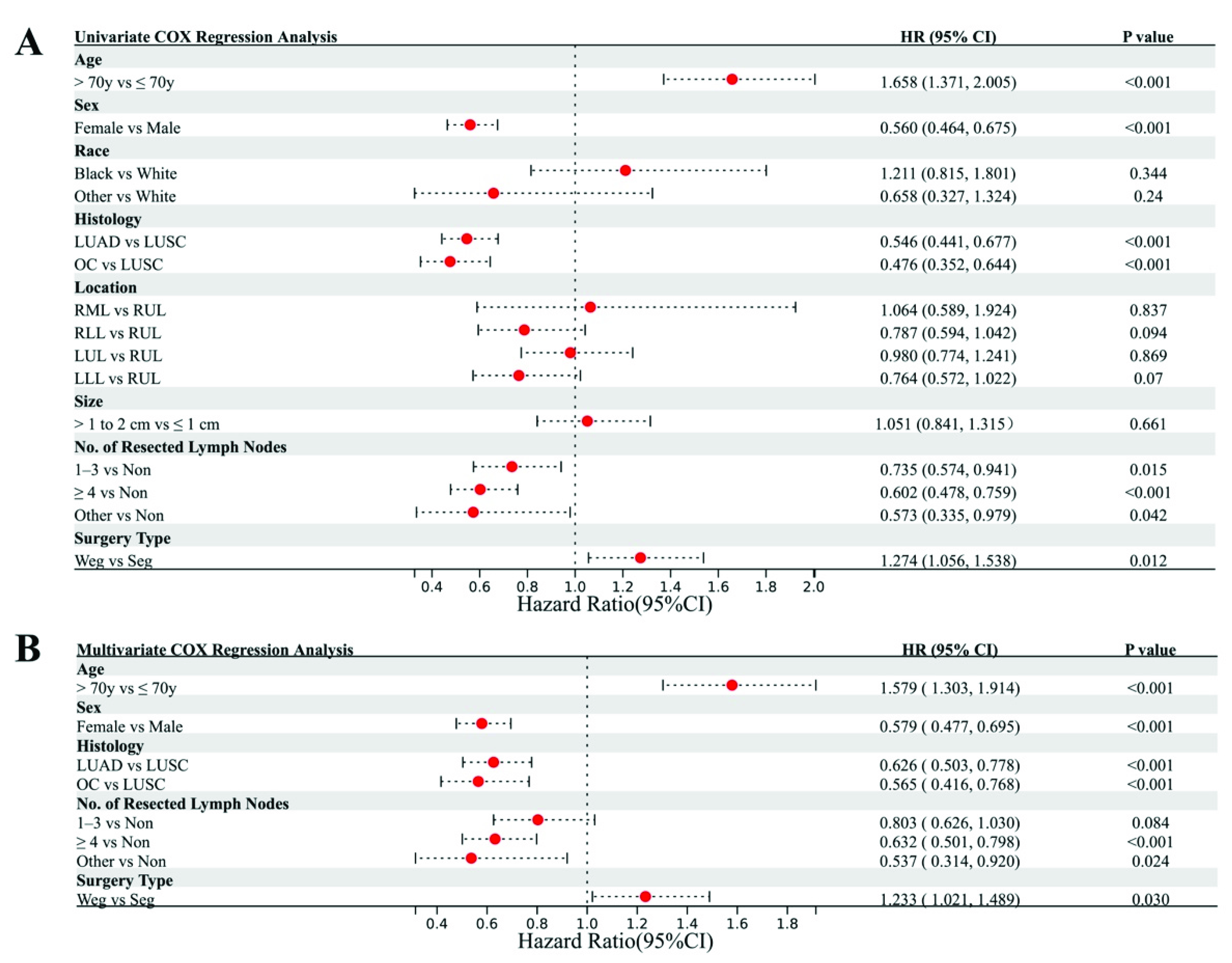
3.7. Cox Regression Analysis
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Cao, C.; D’Amico, T.; Demmy, T.; Dunning, J.; Gossot, D.; Hansen, H.; He, J.; Jheon, S.; Petersen, R.H.; Sihoe, A.; et al. Surgery versus SABR for resectable non-small-cell lung cancer. Lancet Oncol. 2015, 16, e370–e371. [Google Scholar] [CrossRef]
- Ginsberg, R.J.; Rubinstein, L.V. Randomized trial of lobectomy versus limited resection for T1 N0 non-small cell lung cancer. Lung Cancer Study Group. Ann. Thorac. Surg. 1995, 60, 615–622. [Google Scholar] [CrossRef]
- Stokes, W.A.; Bronsert, M.R.; Meguid, R.; Blum, M.G.; Jones, B.; Koshy, M.; Sher, D.J.; Louie, A.V.; Palma, D.A.; Senan, S.; et al. Post-Treatment Mortality After Surgery and Stereotactic Body Radiotherapy for Early-Stage Non-Small-Cell Lung Cancer. J. Clin. Oncol. 2018, 36, 642–651. [Google Scholar] [CrossRef] [PubMed]
- Keenan, R.J.; Landreneau, R.J.; Maley, R.H.; Singh, D.; Macherey, R.; Bartley, S.; Santucci, T. Segmental resection spares pulmonary function in patients with stage I lung cancer. Ann. Thorac. Surg. 2004, 78, 228–233. [Google Scholar] [CrossRef]
- Kates, M.; Swanson, S.; Wisnivesky, J.P. Survival following lobectomy and limited resection for the treatment of stage I non-small cell lung cancer ≤ 1 cm in size: A review of SEER data. Chest 2011, 139, 491–496. [Google Scholar] [CrossRef]
- Whitson, B.A.; Groth, S.S.; Andrade, R.S.; Mitiek, M.O.; Maddaus, M.A.; D’Cunha, J. Invasive adenocarcinoma with bronchoalveolar features: A population-based evaluation of the extent of resection in bronchoalveolar cell carcinoma. J. Thorac. Cardiovasc. Surg. 2012, 143, 591–600. [Google Scholar] [CrossRef] [Green Version]
- Yendamuri, S.; Sharma, R.; Demmy, M.; Groman, A.; Hennon, M.; Dexter, E.; Nwogu, C.; Miller, A.; Demmy, T. Temporal trends in outcomes following sublobar and lobar resections for small (≤2 cm) non-small cell lung cancers—A Surveillance Epidemiology End Results database analysis. J. Surg. Res. 2013, 183, 27–32. [Google Scholar] [CrossRef]
- Saji, H.; Okada, M.; Tsuboi, M.; Nakajima, R.; Suzuki, K.; Aokage, K.; Aoki, T.; Okami, J.; Yoshino, I.; Ito, H.; et al. Segmentectomy versus lobectomy in small-sized peripheral non-small-cell lung cancer (JCOG0802/WJOG4607L): A multicentre, open-label, phase 3, randomised, controlled, non-inferiority trial. Lancet 2022, 399, 1607–1617. [Google Scholar] [CrossRef]
- Sakurai, H.; Asamura, H. Sublobar resection for early-stage lung cancer. Transl. Lung Cancer Res. 2014, 3, 164–172. [Google Scholar]
- Tsutani, Y.; Handa, Y.; Shimada, Y.; Ito, H.; Ikeda, N.; Nakayama, H.; Yoshimura, K.; Okada, M. Comparison of cancer control between segmentectomy and wedge resection in patients with clinical stage IA non-small cell lung cancer. J. Thorac. Cardiovasc. Surg. 2021, 162, 1244–1252. [Google Scholar] [CrossRef]
- Wang, P.; Wang, S.; Liu, Z.; Sui, X.; Wang, X.; Li, X.; Qiu, M.; Yang, F. Segmentectomy and Wedge Resection for Elderly Patients with Stage I Non-Small Cell Lung Cancer: A Systematic Review and Meta-Analysis. J. Clin. Med. 2022, 11, 294. [Google Scholar] [CrossRef]
- Altorki, N.K.; Kamel, M.K.; Narula, N.; Ghaly, G.; Nasar, A.; Rahouma, M.; Lee, P.C.; Port, J.L.; Stiles, B.M. Anatomical Segmentectomy and Wedge Resections Are Associated with Comparable Outcomes for Patients with Small cT1N0 Non-Small Cell Lung Cancer. J. Thorac. Oncol. 2016, 11, 1984–1992. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mimae, T.; Saji, H.; Nakamura, H.; Okumura, N.; Tsuchida, M.; Sonobe, M.; Miyazaki, T.; Aokage, K.; Nakao, M.; Haruki, T.; et al. Survival of Octogenarians with Early-Stage Non-small Cell Lung Cancer is Comparable Between Wedge Resection and Lobectomy/Segmentectomy: JACS1303. Ann. Surg. Oncol. 2021, 28, 7219–7227. [Google Scholar] [CrossRef] [PubMed]
- Ueda, K.; Murakami, J.; Tanaka, T.; Nakamura, T.; Yoshimine, S.; Hamano, K. Postoperative Complications and Cancer Recurrence: Impact on Poor Prognosis of Lower Lobe Cancer. Ann. Thorac. Surg. 2020, 109, 1750–1756. [Google Scholar] [CrossRef] [PubMed]
- Ou, S.H.I.; Zell, J.A.; Ziogas, A.; Anton-Culver, H. Prognostic factors for survival of stage I nonsmall cell lung cancer patients: A population-based analysis of 19,702 stage I patients in the California Cancer Registry from 1989 to 2003. Cancer 2007, 110, 1532–1541. [Google Scholar] [CrossRef] [PubMed]
- Strand, T.E. Survival after resection for primary lung cancer: A population based study of 3211 resected patients. Thorax 2006, 61, 710–715. [Google Scholar] [CrossRef] [Green Version]
- Ichinose, Y.; Kato, H.; Koike, T.; Tsuchiya, R.; Fujisawa, T.; Shimizu, N.; Watanabe, Y.; Mitsudomi, T.; Yoshimura, M.; Tsuboi, M. Completely resected stage IIIA non-small cell lung cancer: The significance of primary tumor location and N2 station. J. Thorac. Cardiovasc. Surg. 2001, 122, 803–808. [Google Scholar] [CrossRef] [Green Version]
- Shaverdian, N.; Veruttipong, D.; Wang, J.; Kupelian, P.; Steinberg, M.; Lee, P. Location Matters: Stage I Non-Small-cell Carcinomas of the Lower Lobes Treated with Stereotactic Body Radiation Therapy Are Associated with Poor Outcomes. Clin Lung Cancer 2017, 18, e137–e142. [Google Scholar] [CrossRef]
- Dai, C.; Shen, J.; Ren, Y.; Zhong, S.; Zheng, H.; He, J.; Xie, D.; Fei, K.; Liang, W.; Jiang, G.; et al. Choice of Surgical Procedure for Patients with Non-Small-Cell Lung Cancer ≤ 1 cm or > 1 to 2 cm Among Lobectomy, Segmentectomy, and Wedge Resection: A Population-Based Study. J. Clin. Oncol. 2016, 34, 3175–3182. [Google Scholar] [CrossRef]
- Xue, W.; Duan, G.; Zhang, X.; Zhang, H.; Zhao, Q.; Xin, Z. Meta-analysis of segmentectomy versus wedge resection in stage IA non-small-cell lung cancer. Onco Targets Ther. 2018, 11, 3369–3375. [Google Scholar] [CrossRef] [Green Version]
- Ye, T.; Deng, L.; Wang, S.; Xiang, J.; Zhang, Y.; Hu, H.; Sun, Y.; Li, Y.; Shen, L.; Xie, L.; et al. Lung Adenocarcinomas Manifesting as Radiological Part-Solid Nodules Define a Special Clinical Subtype. J. Thorac. Oncol. 2019, 14, 617–627. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hattori, A.; Suzuki, K.; Takamochi, K.; Wakabayashi, M.; Aokage, K.; Saji, H.; Watanabe, S.-I.; Tsutani, Y.; Yoshioka, H.; Satoshi, S.; et al. Prognostic impact of a ground-glass opacity component in clinical stage IA non-small cell lung cancer. J. Thorac. Cardiovasc. Surg. 2021, 161, 1469–1480. [Google Scholar] [CrossRef] [PubMed]
- Hao, B.; Fan, T.; Xiong, J.; Zhang, L.; Lu, Z.; Liu, B.; Meng, H.; He, R.; Li, N.; Geng, Q. The Prognostic Significance of the Histological Types in Patients with Nonsmall Cell Lung Cancer ≤ 2 cm. Front. Surg. 2021, 8, 721567. [Google Scholar] [CrossRef] [PubMed]
- Yang, H.X.; Woo, K.M.; Sima, C.S.; Bains, M.S.; Adusumilli, P.S.; Huang, J.; Finley, D.J.; Rizk, N.P.; Rusch, V.W.; Jones, D.R.; et al. Long-term Survival Based on the Surgical Approach to Lobectomy for Clinical Stage I Nonsmall Cell Lung Cancer: Comparison of Robotic, Video-assisted Thoracic Surgery, and Thoracotomy Lobectomy. Ann. Surg. 2017, 265, 431–437. [Google Scholar] [CrossRef] [Green Version]
- Gu, Z.; Wang, H.; Mao, T.; Ji, C.; Xiang, Y.; Zhu, Y.; Xu, P.; Fang, W. Pulmonary function changes after different extent of pulmonary resection under video-assisted thoracic surgery. J. Thorac. Dis. 2018, 10, 2331–2337. [Google Scholar] [CrossRef] [Green Version]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Characteristics | Before PSM | After PSM | ||||||
|---|---|---|---|---|---|---|---|---|
| Estimate | Segmentectomy | Wedge Resection | p Value | Estimate | Segmentectomy | Wedge Resection | p Value | |
| 5464 (100%) | 1048 (19.18%) | 4416 (80.92%) | 1882 (100.00%) | 941 (50.00%) | 941 (50.00%) | |||
| Age | 0.871 | 0.356 | ||||||
| ≤70 | 2923 (53.50%) | 563 (10.30%) | 2360 (43.19%) | 986 (52.39%) | 503 (26.73%) | 483 (25.66%) | ||
| >70 | 2541 (46.5%) | 485 (8.88%) | 2056 (37.63%) | 896 (47.61%) | 438 (23.27%) | 458 (24.34%) | ||
| Sex | 0.240 | 0.337 | ||||||
| Male | 2115 (38.71%) | 389 (7.12%) | 1726 (31.59%) | 676 (35.92%) | 328 (17.43%) | 348 (18.49%) | ||
| Female | 3349 (61.29%) | 659 (12.06%) | 2690 (49.23%) | 1206 (64.08%) | 613 (32.57%) | 593 (31.51%) | ||
| Race | 0.869 | 1.000 | ||||||
| White | 4780 (87.48%) | 920 (16.84%) | 3860 (70.64%) | 1734 (92.14%) | 867 (46.07%) | 867 (46.07%) | ||
| Black | 411 (7.52%) | 79 (1.45%) | 332 (6.08%) | 88 (4.68%) | 44 (2.34%) | 44 (2.34%) | ||
| Other | 273 (5.00%) | 49 (0.90%) | 224 (4.10%) | 60 (3.19%) | 30 (1.59%) | 30 (1.59%) | ||
| Histologic Type | 0.163 | 0.320 | ||||||
| LUSC | 1045 (19.13%) | 183 (3.35%) | 862 (15.78%) | 332 (17.64%) | 156 (8.29%) | 176 (9.35%) | ||
| LUAD | 3118 (57.06%) | 624 (11.42%) | 2494 (45.64%) | 1178 (62.59%) | 589 (31.30%) | 589 (31.30%) | ||
| OC | 1301 (23.81%) | 241 (4.41%) | 1060 (19.40%) | 372 (19.77%) | 196 (10.41%) | 176 (9.35%) | ||
| Location | <0.001 | 0.865 | ||||||
| Right Upper Lobe | 1683 (30.80%) | 251 (4.59%) | 1432 (26.21%) | 495 (26.30%) | 239 (12.70%) | 256 (13.60%) | ||
| Right Middle Lobe | 303 (51.55%) | 26 (0.48%) | 277 (5.07%) | 45 (2.39%) | 21 (1.12%) | 24 (1.28%) | ||
| Right Lower Lobe | 974 (17.83%) | 209 (3.83%) | 765 (14.00%) | 372 (19.77%) | 186 (9.88%) | 186 (9.88%) | ||
| Left Upper Lobe | 1544 (28.26%) | 351 (6.42%) | 1193 (21.83%) | 619 (32.89%) | 318 (16.90%) | 301 (15.99%) | ||
| Left Lower Lobe | 960 (17.57%) | 211 (3.86%) | 749 (13.71%) | 351 (18.65%) | 177 (9.40%) | 174 (9.25%) | ||
| Tumor Size | <0.001 | 1.000 | ||||||
| ≤1 cm | 1730 (31.66%) | 256 (4.69%) | 1474 (26.98%) | 440 (23.38%) | 220 (11.69%) | 220 (11.69%) | ||
| >1 cm to 2 cm | 3734 (68.34%) | 792 (14.49%) | 2942 (53.84%) | 1442 (76.62%) | 721 (38.31%) | 721 (38.31%) | ||
| No. of Resected Lymph Nodes | <0.001 | 0.845 | ||||||
| 0 | 2338 (42.79%) | 208 (3.81%) | 2130 (38.98%) | 385 (20.46%) | 196 (10.41%) | 189 (10.04%) | ||
| >1 to 3 | 1343 (24.58%) | 269 (4.92%) | 1074 (19.66%) | 501 (26.62%) | 250 (13.28%) | 251 (13.34%) | ||
| ≥4 | 1574 (28.81%) | 523 (9.57%) | 1051 (19.23%) | 925 (49.15%) | 463 (24.60%) | 462 (24.55%) | ||
| Other | 209 (3.83%) | 48 (0.88%) | 161 (2.95%) | 71 (3.77%) | 32 (1.70%) | 39 (2.07%) | ||
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Lei, X.; Zhou, N.; Zhang, H.; Li, T.; Ren, F.; Zhang, B.; Li, X.; Zu, L.; Song, Z.; Xu, S. Lobe-Specific Analysis of Sublobar Lung Resection for NSCLC Patients with Tumors ≤ 2 cm. Cancers 2022, 14, 3265. https://doi.org/10.3390/cancers14133265
Lei X, Zhou N, Zhang H, Li T, Ren F, Zhang B, Li X, Zu L, Song Z, Xu S. Lobe-Specific Analysis of Sublobar Lung Resection for NSCLC Patients with Tumors ≤ 2 cm. Cancers. 2022; 14(13):3265. https://doi.org/10.3390/cancers14133265
Chicago/Turabian StyleLei, Xi, Ning Zhou, Hao Zhang, Tong Li, Fan Ren, Bo Zhang, Xiongfei Li, Lingling Zu, Zuoqing Song, and Song Xu. 2022. "Lobe-Specific Analysis of Sublobar Lung Resection for NSCLC Patients with Tumors ≤ 2 cm" Cancers 14, no. 13: 3265. https://doi.org/10.3390/cancers14133265