
Folinic Acid Potentiates the Liver Regeneration Process after Selective Portal Vein Ligation in Rats

 , , and
, , and 
Abstract
:Simple Summary
Abstract
1. Introduction
2. Materials and Methods
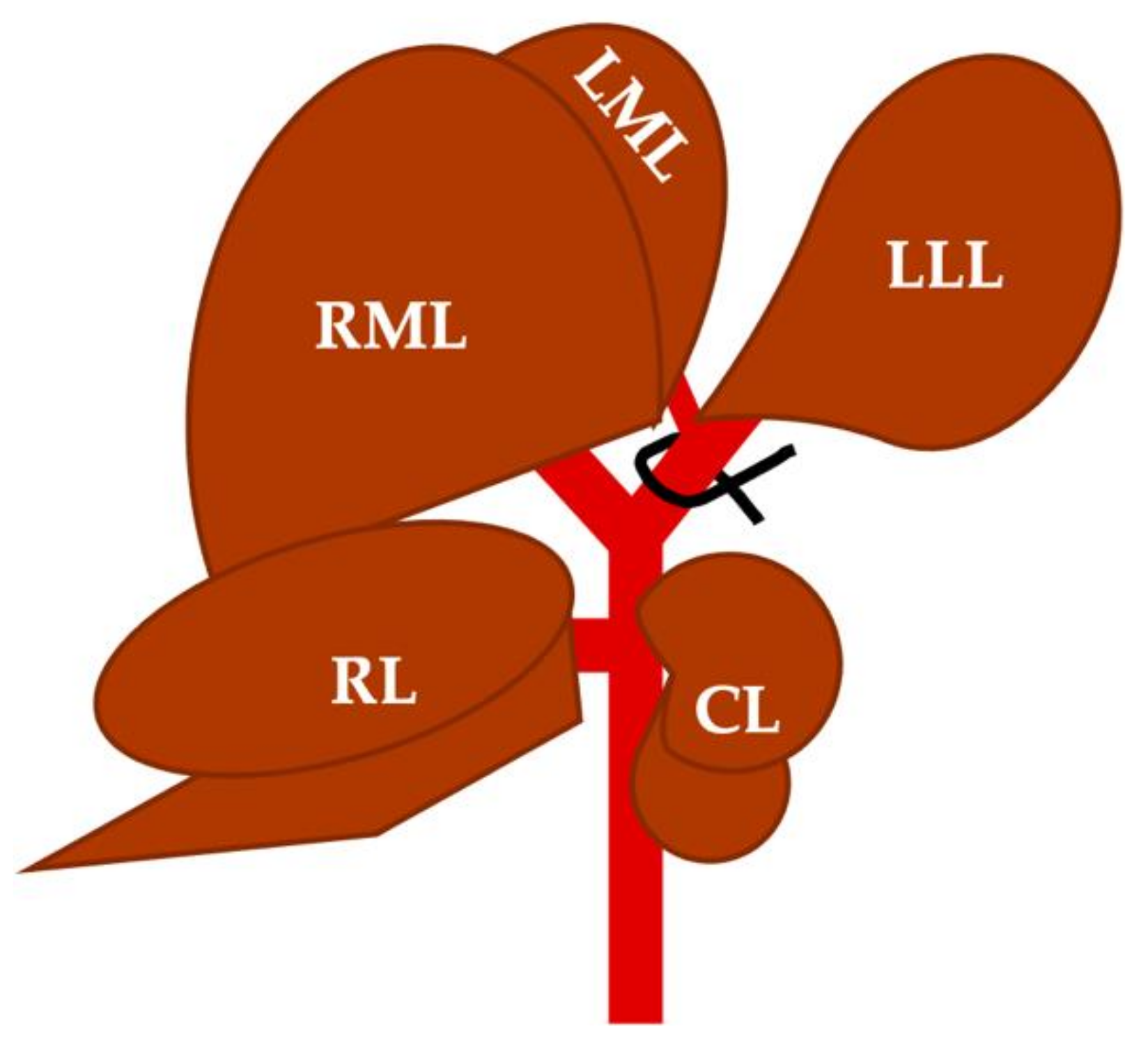
2.1. Selective Portal Vein Ligation
2.2. Folinic Acid or Saline Administration
2.3. Blood Collection and Histological Samples Obtention
2.4. Serum Samples and Histological Sections Analysis
2.5. Statistical Analysis
3. Results
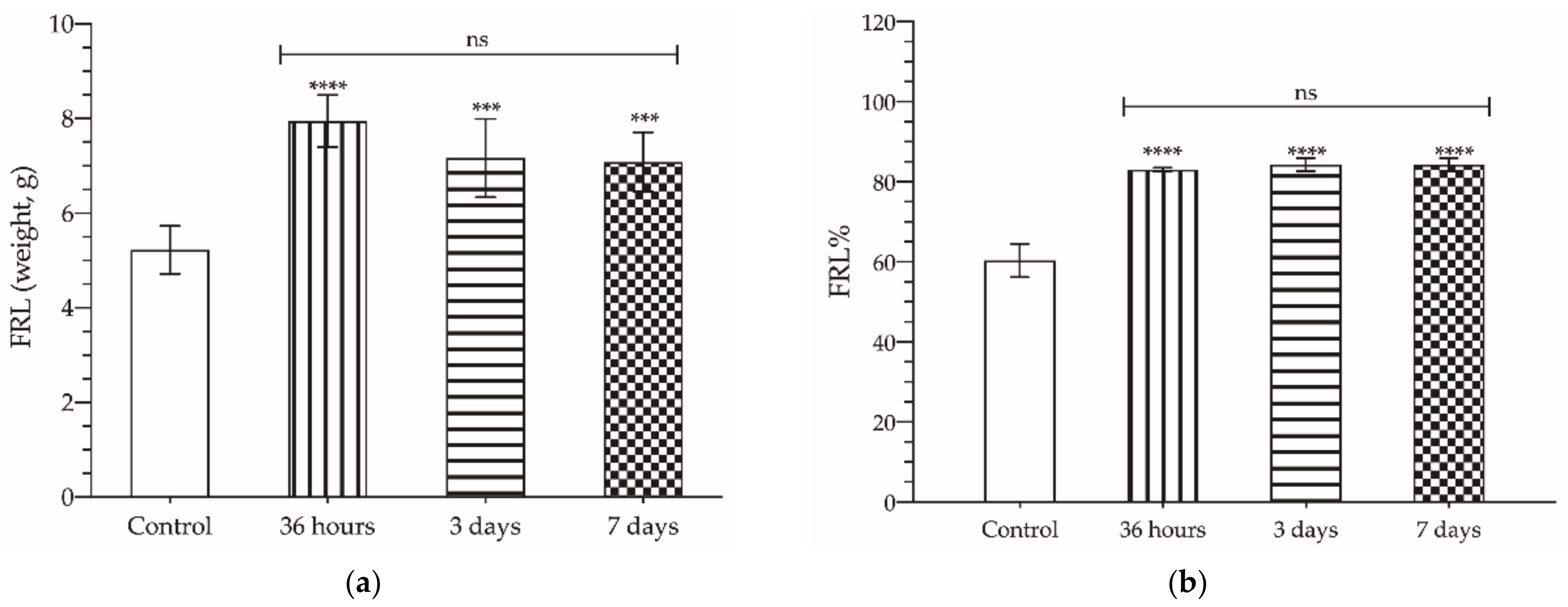
3.1. Regenerative Response of the Liver after Selective PVL
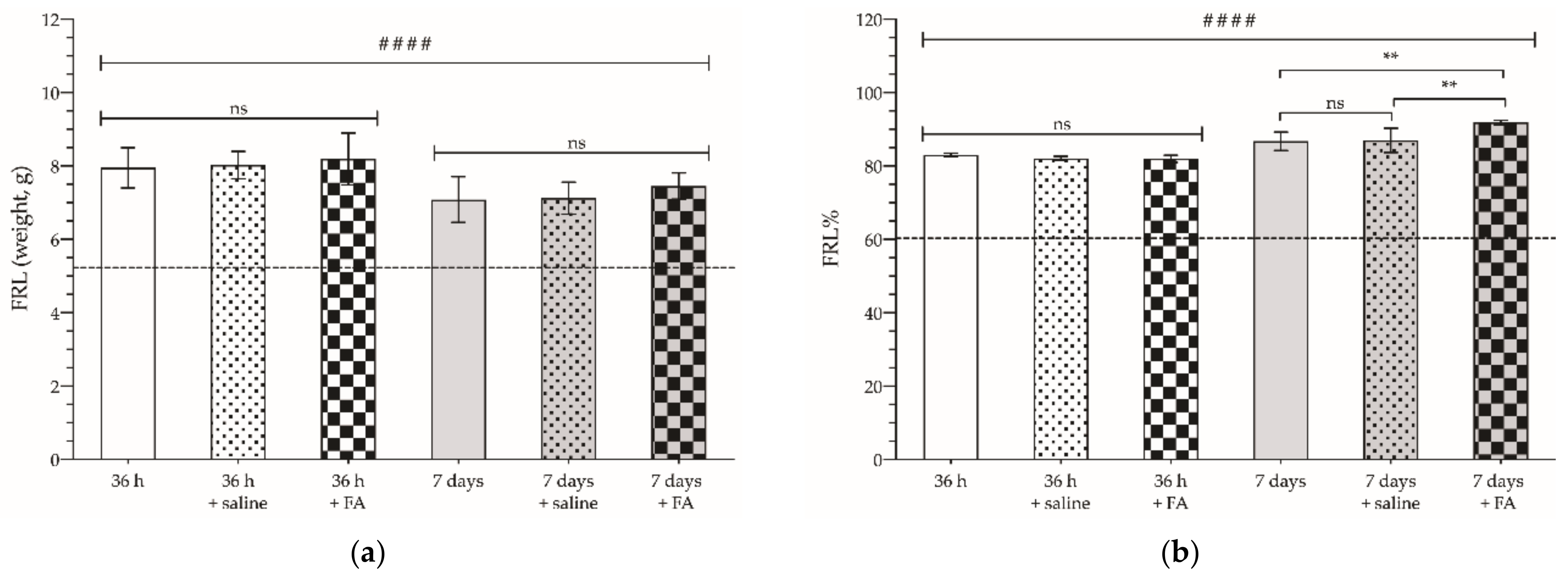
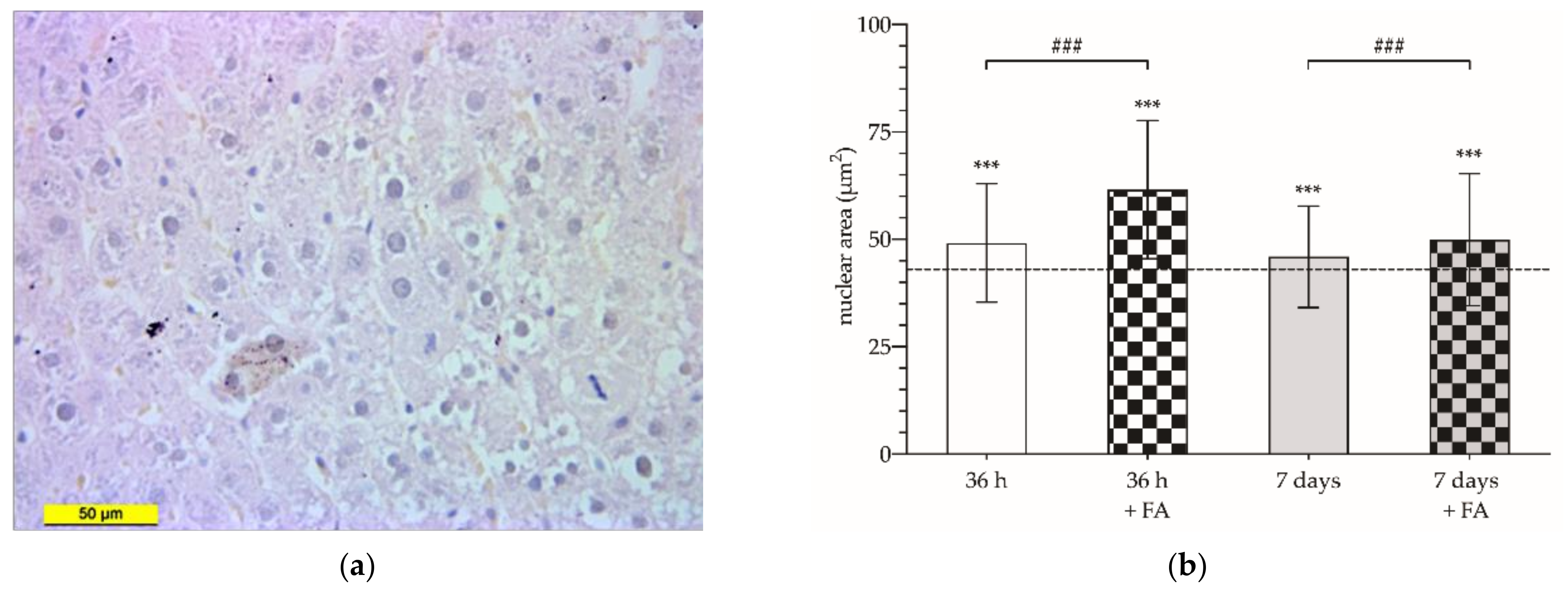
3.2. Enhancing Effect of FA on Hepatic Hypertrophy after Selective PVL
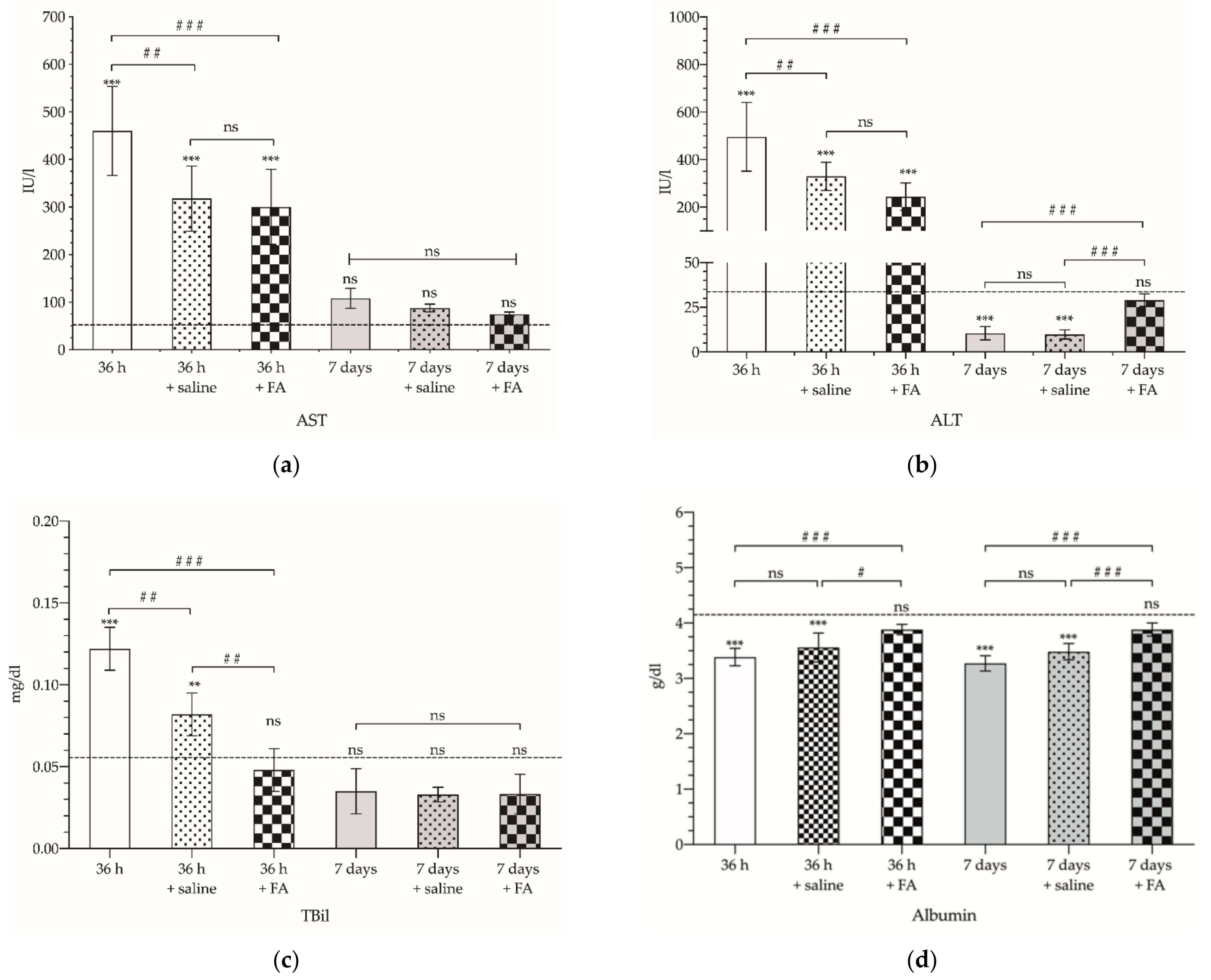
3.3. Liver Functional Status after Selective PVL
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Mohamed, F.; Kallioinen, M.; Braun, M.; Fenwick, S.; Shackcloth, M.; Davies, R.J.; Committee, G. Management of colorectal cancer metastases to the liver, lung or peritoneum suitable for curative intent: Summary of NICE guidance. Br. J. Surg. 2020, 107, 943–945. [Google Scholar] [CrossRef] [PubMed]
- Cugat, E.; Mir-Labrador, J.; Cortese, S.; Pareja, E.; Fuster, J.; Santoyo, J. Cirugía hepática. In Cirugía Hepática; Robles Campos, R., Parrilla Paricio, P., Eds.; Arán Ediciones: Madrid, Spain, 2018; pp. 34–44. ISBN 978-84-17554-12-5. [Google Scholar]
- García Pérez, R. Estudio Comparativo de Regeneración Hepática Inducida por Técnica ALPPS Versus Ligadura Portal en un Modelo Experimental en Rata. Ph.D. Thesis, University of Murcia, Murcia, Spain, 2005. [Google Scholar]
- Soares Kevin, C.; Jarnagin, W.R. Liver & Portal Venous System. In Current Diagnosis and Treatment Surgery; Doherty, G.M., Ed.; McGraw Hill: New York, NY, USA, 2020; ISBN 978-1-260-12221-3. [Google Scholar]
- Bingham, G.; Shetye, A.; Suresh, R.; Mirnezami, R. Impact of primary tumour location on colorectal liver metastases: A systematic review. World J. Clin. Oncol. 2020, 11, 294–307. [Google Scholar] [CrossRef] [PubMed]
- Moris, D.; Ronnekleiv-Kelly, S.; Kostakis, I.D.; Tsilimigras, D.I.; Beal, E.W.; Papalampros, A.; Dimitroulis, D.; Felekouras, E.; Pawlik, T.M. Operative Results and Oncologic Outcomes of Associating Liver Partition and Portal Vein Ligation for Staged Hepatectomy (ALPPS) Versus Two-Stage Hepatectomy (TSH) in Patients with Unresectable Colorectal Liver Metastases: A Systematic Review and Meta-Anal. World J. Surg. 2018, 42, 806–815. [Google Scholar] [CrossRef] [PubMed]
- Lang, H.; Baumgart, J.; Mittler, J. Associating Liver Partition and Portal Vein Ligation for Staged Hepatectomy in the Treatment of Colorectal Liver Metastases: Current Scenario. Dig. Surg. 2018, 35, 294–302. [Google Scholar] [CrossRef] [PubMed]
- Hernandez-Alejandro, R.; Sharma, H. Small-for-size syndrome in liver transplantation: New horizons to cover with a good launchpad. Liver Transplant. 2016, 22, 33–36. [Google Scholar] [CrossRef]
- González Arribas, M. Efecto de la Hepatectomía Parcial Sobre el Desarrollo de Metástasis Hepáticas: Revisión Bibliográfica y Estudio Experimental en un Modelo Murino; Final Degree Project; University of The Basque Country: Biscay, Spain, 2019. [Google Scholar]
- Zhang, G.Q.; Zhang, Z.W.; Lau, W.Y.; Chen, X.P. Associating liver partition and portal vein ligation for staged hepatectomy (ALPPS): A new strategy to increase resectability in liver surgery. Int. J. Surg. 2014, 12, 437–441. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Schnitzbauer, A.A.; Lang, S.A.; Goessmann, H.; Nadalin, S.; Baumgart, J.; Farkas, S.A.; Fichtner-Feigl, S.; Lorf, T.; Goralcyk, A.; Hörbelt, R.; et al. Right Portal Vein Ligation Combined With In Situ Splitting Induces Rapid Left Lateral Liver Lobe Hypertrophy Enabling 2-Staged Extended Right Hepatic Resection in Small-for-Size Settings. Ann. Surg. 2012, 255, 405–414. [Google Scholar] [CrossRef] [PubMed]
- Truant, S.; Scatton, O.; Dokmak, S.; Regimbeau, J.-M.; Lucidi, V.; Laurent, A.; Gauzolino, R.; Castro Benitez, C.; Pequignot, A.; Donckier, V.; et al. Associating liver partition and portal vein ligation for staged hepatectomy (ALPPS): Impact of the inter-stages course on morbi-mortality and implications for management. Eur. J. Surg. Oncol. 2015, 41, 674–682. [Google Scholar] [CrossRef] [PubMed]
- Khuu, D.N.; Nyabi, O.; Maerckx, C.; Sokal, E.; Najimi, M. Adult Human Liver Mesenchymal Stem/Progenitor Cells Participate in Mouse Liver Regeneration after Hepatectomy. Cell Transplant. 2013, 22, 1369–1380. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wabitsch, S.; Benzing, C.; Krenzien, F.; Splith, K.; Haber, P.K.; Arnold, A.; Nösser, M.; Kamali, C.; Hermann, F.; Günther, C.; et al. Human Stem Cells Promote Liver Regeneration After Partial Hepatectomy in BALB/C Nude Mice. J. Surg. Res. 2019, 239, 191–200. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Li, D.-L.; He, X.-H.; Zhang, S.-A.; Fang, J.; Chen, F.-S.; Fan, J.-J. Bone Marrow-Derived Mesenchymal Stem Cells Promote Hepatic Regeneration after Partial Hepatectomy in Rats. Pathobiology 2013, 80, 228–234. [Google Scholar] [CrossRef] [PubMed]
- Schadde, E.; Tsatsaris, C.; Swiderska-Syn, M.; Breitenstein, S.; Urner, M.; Schimmer, R.; Booy, C.; Z’graggen, B.R.; Wenger, R.H.; Spahn, D.R.; et al. Hypoxia of the growing liver accelerates regeneration. Surgery 2017, 161, 666–679. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Maeno, H.; Ono, T.; Dhar, D.K.; Sato, T.; Yamanoi, A.; Nagasue, N. Expression of hypoxia inducible factor-1α during liver regeneration induced by partial hepatectomy in rats. Liver Int. 2005, 25, 1002–1009. [Google Scholar] [CrossRef] [PubMed]
- Schmeding, M.; Rademacher, S.; Boas-Knoop, S.; Roecken, C.; Lendeckel, U.; Neuhaus, P.; Neumann, U.P. rHuEPo Reduces Ischemia-Reperfusion Injury and Improves Survival After Transplantation of Fatty Livers in Rats. Transplantation 2010, 89, 161–168. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ohtake, M.; Aono, T.; Sakaguchi, T. Liver regeneration is enhanced by omeprazole in rats following partial hepatectomy. Br. J. Surg. 1994, 81, 1179–1180. [Google Scholar] [CrossRef]
- Portugal, V.; García-Alonso, I.; Méndez, J. Hepatotrophic effect of folinic acid in rats. J. Surg. Res. 1996, 61, 527–530. [Google Scholar] [CrossRef]
- Reddy, S.K.; Barbas, A.S.; Turley, R.S.; Steel, J.L.; Tsung, A.; Marsh, J.W.; Geller, D.A.; Clary, B.M. A standard definition of major hepatectomy: Resection of four or more liver segments. HPB 2011, 13, 494–502. [Google Scholar] [CrossRef] [Green Version]
- Khan, A.S.; Garcia-Aroz, S.; Ansari, M.A.; Atiq, S.M.; Senter-Zapata, M.; Fowler, K.; Doyle, M.B.; Chapman, W.C. Assessment and optimization of liver volume before major hepatic resection: Current guidelines and a narrative review. Int. J. Surg. 2018, 52, 74–81. [Google Scholar] [CrossRef] [PubMed]
- Schroeder, R.A.; Marroquin, C.E.; Bute, B.P.; Khuri, S.; Henderson, W.G.; Kuo, P.C. Predictive indices of morbidity and mortality after liver resection. Ann. Surg. 2006, 243, 373–379. [Google Scholar] [CrossRef] [PubMed]
- Horiguchi, N.; Ishac, E.J.N.; Gao, B. Liver regeneration is suppressed in alcoholic cirrhosis: Correlation with decreased STAT3 activation. Alcohol 2007, 41, 271–280. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Koteish, A.; Yang, S.; Lin, H.; Huang, J.; Diehl, A.M. Ethanol Induces Redox-Sensitive Cell-Cycle Inhibitors and Inhibits Liver Regeneration After Partial Hepatectomy. Alcohol. Clin. Exp. Res. 2002, 26, 1710–1718. [Google Scholar] [CrossRef] [PubMed]
- Cardin, R.; D’errico, A.; Fiorentino, M.; Cecchetto, A.; Naccarato, R.; Farinati, F. Hepatocyte proliferation and apoptosis in relation to oxidative damage in alcohol-related liver disease. Alcohol Alcohol. 2002, 37, 43–48. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- De Santibañes, M.; Boccalatte, L.; de Santibañes, E. A literature review of associating liver partition and portal vein ligation for staged hepatectomy (ALPPS): So far, so good. Updates Surg. 2017, 69, 9–19. [Google Scholar] [CrossRef] [PubMed]
- Fischer, C.; Melstrom, L.G.; Arnaoutakis, D.; Jarnagin, W.; Brown, K.; D’Angelica, M.; Covey, A.; DeMatteo, R.; Allen, P.; Kingham, T.P.; et al. Chemotherapy after portal vein embolization to protect against tumor growth during liver hypertrophy before hepatectomy. JAMA Surg. 2013, 148, 1103–1108. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zhao, J.; Xu, H.; Li, Y.; Gong, L.; Zheng, G.; Wang, X.; Luan, W.; Li, S.; Ma, F.; Ni, L.; et al. NAFLD Induction Delays Postoperative Liver Regeneration of ALPPS in Rats. Dig. Dis. Sci. 2019, 64, 456–468. [Google Scholar] [CrossRef]
- Almau Trenard, H.M.; Moulin, L.E.; Padin, J.M.; Gondolesi, G.E.; Barros Schelotto, P. Desarrollo de un modelo experimental de ligadura portal asociada a transección parenquimatosa (ALPPS) en ratas. Cirugía Española 2014, 92, 676–681. [Google Scholar] [CrossRef] [PubMed]
- Yang, X.; Yang, C.; Qiu, Y.; Shen, S.; Kong, J.; Wang, W. A preliminary study of associating liver partition and portal vein ligation for staged hepatectomy in a rat model of liver cirrhosis. Exp. Ther. Med. 2019, 18, 1203–1211. [Google Scholar] [CrossRef] [PubMed]
- Shi, J.H.; Hammarström, C.; Grzyb, K.; Line, P.D. Experimental evaluation of liver regeneration patterns and liver function following ALPPS. BJS Open 2017, 1, 84–96. [Google Scholar] [CrossRef]
- García-Pérez, R.; Revilla-Nuin, B.; Martínez, C.M.; Bernabé-García, A.; Baroja Mazo, A.; Parrilla Paricio, P. Associated Liver Partition and Portal Vein Ligation (ALPPS) vs selective Portal Vein Ligation (PVL) for staged hepatectomy in a rat model. Similar regenerative response? PLoS ONE 2015, 10, e0144096. [Google Scholar] [CrossRef]
- Liao, M.; Zhang, T.; Wang, H.; Liu, Y.; Lu, M.; Huang, J.; Zeng, Y. Rabbit model provides new insights in liver regeneration after transection with portal vein ligation. J. Surg. Res. 2017, 209, 242–251. [Google Scholar] [CrossRef] [Green Version]
- Croome, K.P.; Mao, S.A.; Glorioso, J.M.; Krishna, M.; Nyberg, S.L.; Nagorney, D.M. Characterization of a porcine model for associating liver partition and portal vein ligation for a staged hepatectomy. HPB 2015, 17, 1130–1136. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Yifan, T.; Ming, X.; Yifan, W.; Hanning, Y.; Guangyi, J.; Peijian, Y.; Ke, W.; Xiujun, C. Hepatic regeneration by associating liver partition and portal vein ligation for staged hepatectomy (ALPPS) is feasible but attenuated in rat liver with thioacetamide-induced fibrosis. Surgery 2019, 165, 345–352. [Google Scholar] [CrossRef]
- Dili, A.; Lebrun, V.; Bertrand, C.; Leclercq, I.A. Associating liver partition and portal vein ligation for staged hepatectomy: Establishment of an animal model with insufficient liver remnant. Lab. Investig. 2019, 99, 698–707. [Google Scholar] [CrossRef] [PubMed]
- Higgins, G.M.; Anderson, R.M. Experimental pathology of the liver. Restoration of the liver of the white rat following partial surgical removal. AMA Arch. Pathol. 1931, 12, 186–202. [Google Scholar]
- Veith, N.T.; Histing, T.; Menger, M.D.; Pohlemann, T.; Tschernig, T. Helping prometheus: Liver protection in acute hemorrhagic shock. Ann. Transl. Med. 2017, 5, 206. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Correa-Gallego, C.; Tan, K.S.; Arslan-Carlon, V.; Gonen, M.; Denis, S.C.; Langdon-Embry, L.; Grant, F.; Kingham, T.P.; DeMatteo, R.P.; Allen, P.J.; et al. Goal-Directed Fluid Therapy Using Stroke Volume Variation for Resuscitation after Low Central Venous Pressure-Assisted Liver Resection: A Randomized Clinical Trial. J. Am. Coll. Surg. 2015, 221, 591–601. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sheng, R.F.; Yang, L.; Jin, K.P.; Wang, H.Q.; Liu, H.; Ji, Y.; Fu, C.X.; Zeng, M.S. Assessment of liver regeneration after associating liver partition and portal vein ligation for staged hepatectomy: A comparative study with portal vein ligation. HPB 2018, 20, 305–312. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Linecker, M.; Stavrou, G.A.; Oldhafer, K.J.; Jenner, R.M.; Seifert, B.; Lurje, G.; Bednarsch, J.; Neumann, U.; Capobianco, I.; Nadalin, S.; et al. The ALPPS Risk Score: Avoiding Futile Use of ALPPS. Ann. Surg. 2016, 264, 763–771. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Olthof, P.B.; Tomassini, F.; Huespe, P.E.; Truant, S.; Pruvot, F.-R.; Troisi, R.I.; Castro, C.; Schadde, E.; Axelsson, R.; Sparrelid, E.; et al. Hepatobiliary scintigraphy to evaluate liver function in associating liver partition and portal vein ligation for staged hepatectomy: Liver volume overestimates liver function. Surgery 2017, 162, 775–783. [Google Scholar] [CrossRef] [PubMed]
- Kang, D.; Schadde, E. Hypertrophy and Liver Function in ALPPS: Correlation with Morbidity and Mortality. Visc. Med. 2017, 33, 426–433. [Google Scholar] [CrossRef]
- Wang, M.J.; Chen, F.; Lau, J.T.Y.; Hu, Y.P. Hepatocyte polyploidization and its association with pathophysiological processes. Cell Death Dis. 2017, 8, e2805. [Google Scholar] [CrossRef] [PubMed]
- Fausto, N.; Campbell, J.S. The role of hepatocytes and oval cells in liver regeneration and repopulation. Mech. Dev. 2003, 120, 117–130. [Google Scholar] [CrossRef]
- Hwang, S.Y.; Kang, Y.J.; Sung, B.; Jang, J.Y.; Hwang, N.L.; Oh, H.J.; Ahn, Y.R.; Kim, H.J.; Shin, J.H.; Yoo, M.; et al. Folic acid is necessary for proliferation and differentiation of C2C12 myoblasts. J. Cell. Physiol. 2018, 233, 736–747. [Google Scholar] [CrossRef] [PubMed]
- Bayer, A.L.; Fraker, C.A. The Folate Cycle As a Cause of Natural Killer Cell Dysfunction and Viral Etiology in Type 1 Diabetes. Front. Endocrinol. Lausanne 2017, 8, 315. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Williams, P.J.; Bulmer, J.N.; Innes, B.A.; Broughton Pipkin, F. Possible Roles for Folic Acid in the Regulation of Trophoblast Invasion and Placental Development in Normal Early Human Pregnancy. Biol. Reprod. 2011, 84, 1148–1153. [Google Scholar] [CrossRef]
- Portugal, V. Estudio de la Regeneración Hepatocitaria en el Hígado Sometido a Isquemia Normotérmica. Ph.D. Thesis, University of The Basque Country, Biscay, Spain, 1992. [Google Scholar]
- Blomgren, H.; Edler, D.; Hallström, M.; Ragnhammar, P. Dual effects of folinic acid in 5-fluorouracil induced killing of human tumor cell lines in vitro. Anticancer Res. 1996, 16, 2713–2717. [Google Scholar] [PubMed]
- Roncalés, M.; Achón, M.; Manzarbeitia, F.; Maestro de las Casas, C.; Ramírez, C.; Varela-Moreiras, G.; Pérez-Miguelsanz, J. Folic Acid Supplementation for 4 Weeks Affects Liver Morphology in Aged Rats. J. Nutr. 2004, 134, 1130–1133. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Marsillach, J.; Ferré, N.; Camps, J.; Riu, F.; Rull, A.; Joven, J. Moderately High Folic Acid Supplementation Exacerbates Experimentally Induced Liver Fibrosis in Rats. Exp. Biol. Med. 2008, 233, 38–47. [Google Scholar] [CrossRef] [PubMed]








{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Group No. | Group Name | PVL | Treatment | Sample Collection Time after PVL | No. of Animals |
|---|---|---|---|---|---|
| 1 | Control | no | no | – | 8 |
| 2 | 36 h | yes | no | 36 h | 8 |
| 3 | 3 d | yes | no | 3 days | 8 |
| 4 | 7 d | yes | no | 7 days | 8 |
| 5 | 36 h + FA | yes | FA (2.5 mg/kg) | 36 h | 8 |
| 6 | 36 h + saline | yes | saline | 36 h | 8 |
| 7 | 7 d + FA | yes | FA (2.5 mg/kg) | 7 days | 8 |
| 8 | 7 d + saline | yes | saline | 7 days | 8 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Gutiérrez Sáenz de Santa María, J.; Herrero de la Parte, B.; Gutiérrez-Sánchez, G.; Ruiz Montesinos, I.; Iturrizaga Correcher, S.; Mar Medina, C.; García-Alonso, I. Folinic Acid Potentiates the Liver Regeneration Process after Selective Portal Vein Ligation in Rats. Cancers 2022, 14, 371. https://doi.org/10.3390/cancers14020371
Gutiérrez Sáenz de Santa María J, Herrero de la Parte B, Gutiérrez-Sánchez G, Ruiz Montesinos I, Iturrizaga Correcher S, Mar Medina C, García-Alonso I. Folinic Acid Potentiates the Liver Regeneration Process after Selective Portal Vein Ligation in Rats. Cancers. 2022; 14(2):371. https://doi.org/10.3390/cancers14020371
Chicago/Turabian StyleGutiérrez Sáenz de Santa María, Jorge, Borja Herrero de la Parte, Gaizka Gutiérrez-Sánchez, Inmaculada Ruiz Montesinos, Sira Iturrizaga Correcher, Carmen Mar Medina, and Ignacio García-Alonso. 2022. "Folinic Acid Potentiates the Liver Regeneration Process after Selective Portal Vein Ligation in Rats" Cancers 14, no. 2: 371. https://doi.org/10.3390/cancers14020371