
Validating Methylated HOXA9 in Bronchial Lavage as a Diagnostic Tool in Patients Suspected of Lung Cancer

 ,
,  , , ,
, , ,  and
and
Abstract
:Simple Summary
Abstract
1. Introduction
2. Materials and Methods
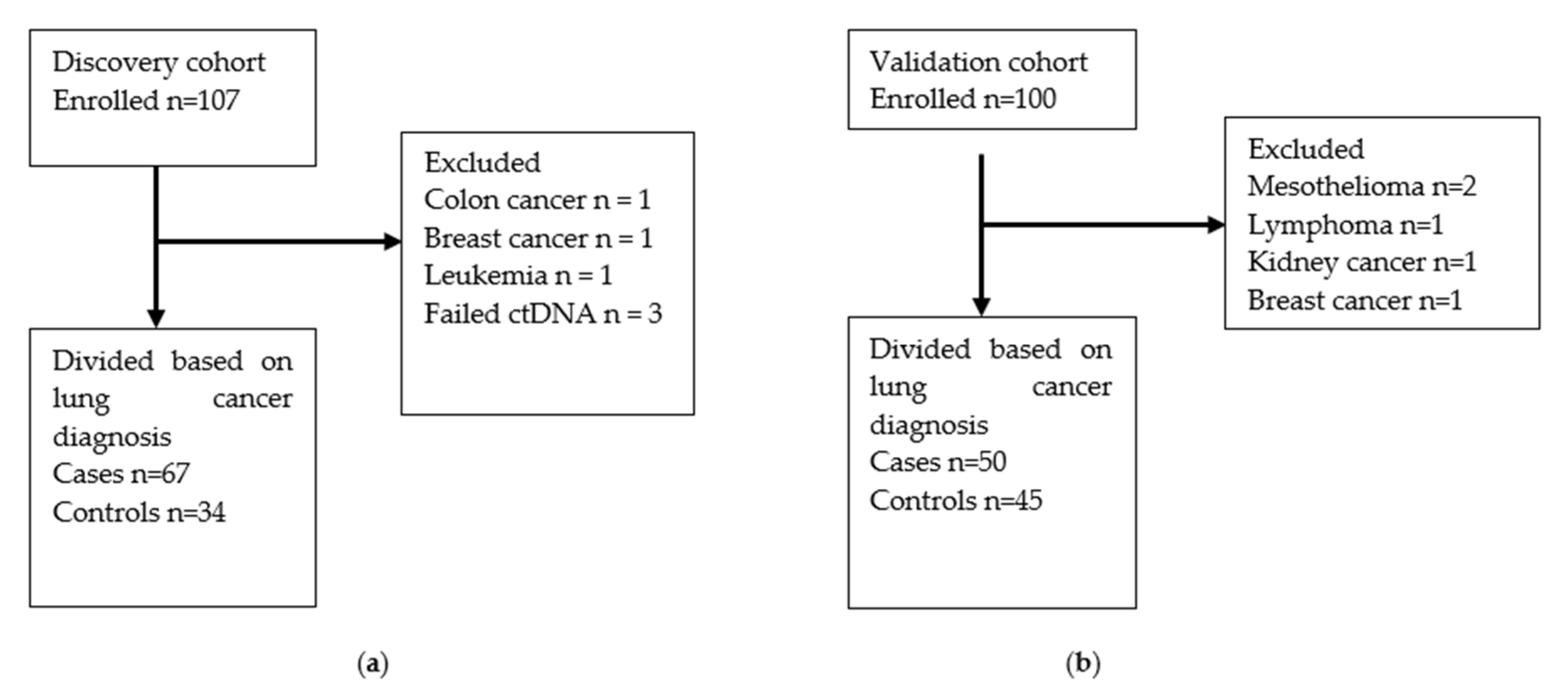
2.1. Participants and Study Design
2.2. Definition of Patient Characteristics
2.3. Diagnostic Work-Up
2.4. Bronchoscopy and Bronchial Lavage Sampling
2.5. Reference Test
2.6. Analysis of Methylated HOXA9
2.7. Determining the Optimal Cut-Off for Methylated HOXA9
2.8. Statistical Analysis
3. Results
3.1. Participant Characteristics
3.2. Methylated HOXA9 and Lung Cancer
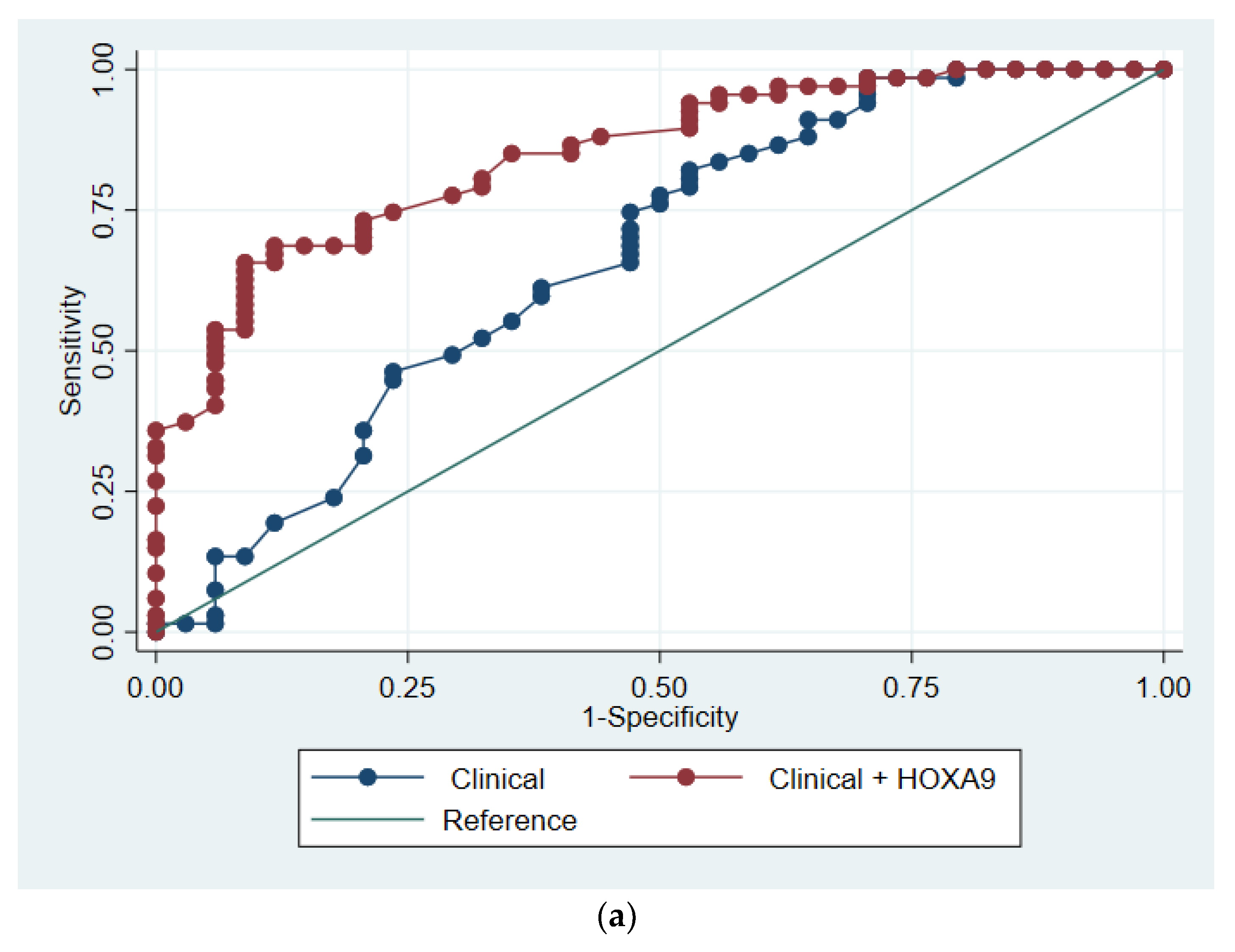
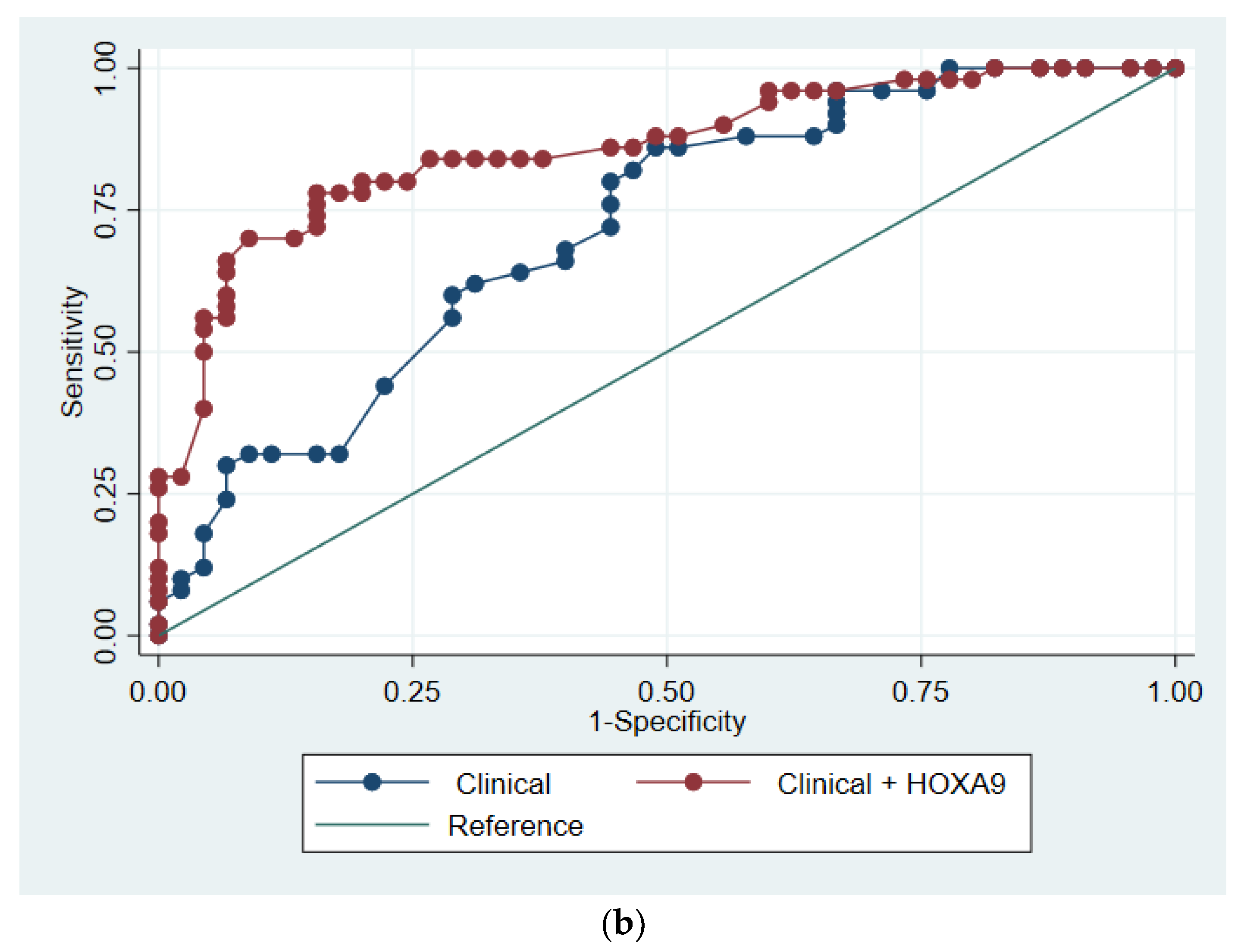
3.3. Predictive Modelling
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Bray, F.; Ferlay, J.; Soerjomataram, I.; Siegel, R.L.; Torre, L.A.; Jemal, A. Global cancer statistics 2018: Globocan estimates of incidence and mortality worldwide for 36 cancers in 185 countries. A Cancer J. Clin. 2018, 68, 394–424. [Google Scholar] [CrossRef] [Green Version]
- Jakobsen, E.; Rasmussen, T.R.; Green, A. Mortality and survival of lung cancer in Denmark: Results from the Danish Lung Cancer Group 2000–2012. Acta Oncologica. 2016, 55, 2–9. [Google Scholar] [CrossRef] [Green Version]
- Cancer Research UK. Lung Cancer Incidence Statistics. Available online: https://www.cancerresearchuk.org/health-professional/cancer-statistics/statistics-by-cancer-type/lung-cancer/incidence#heading-Three (accessed on 1 July 2020).
- Howlader, N.; Noone, A.M.; Krapcho, M.; Miller, D.; Brest, A.; Yu, M.; Ruhl, J.; Tatalovich, Z.; Mariotto, A.; Lewis, D.R.; et al. SEER Cancer Statistics Review, 1975–2016, National Cancer Institute. Bethesda, MD. Based on November 2018 SEER Data Submission, Posted to the SEER Web Site, April 2019. Available online: https://seer.cancer.gov/csr/1975_2016/results_merged/sect_15_lung_bronchus.pdf (accessed on 1 July 2020).
- The National Lung Screening Trial Research Team. Reduced Lung-Cancer Mortality with Low-Dose Computed Tomographic Screening. N. Engl. J. Med. 2011, 365, 395–409. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- de Koning, H.J.; van der Aalst, C.M.; de Jong, P.A.; Scholten, E.T.; Nackaerts, K.; Heuvelmans, M.A. Reduced Lung-Cancer Mortality with Volume CT Screening in a Randomized Trial. N. Engl. J. Med. 2020, 382, 503–513. [Google Scholar] [CrossRef]
- Wille, M.M.W.; Dirksen, A.; Ashraf, H.; Saghir, Z.; Bach, K.S.; Brodersen, J. Results of the Randomized Danish Lung Cancer Screening Trial with Focus on High-Risk Profiling. Am. J. Respir. Crit. Care Med. 2016, 193, 542–551. [Google Scholar] [CrossRef]
- American College of Radiology Committee on Lung-RADS®. Lung-RADS Assessment Categories Version 1.1. Available online: https://www.acr.org/-/media/ACR/Files/RADS/Lung-RADS/LungRADSAssessmentCategoriesv1-1.pdf (accessed on 1 November 2020).
- Cressman, S.; Peacock, S.J.; Tammemägi, M.C.; Evans, W.K.; Leighl, N.B.; Goffin, J.R. The Cost-Effectiveness of High-Risk Lung Cancer Screening and Drivers of Program Efficiency. J. Thorac. Oncol. 2017, 12, 1210–1222. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Snowsill, T.; Yang, H.; Griffin, E.; Long, L.; Varley-Campbell, J.; Coelho, H. Low-dose computed tomography for lung cancer screening in high-risk populations: A systematic review and economic evaluation. Health Technol. Assess. 2018, 22, 1–276. [Google Scholar] [CrossRef] [PubMed]
- Tammemägi, M.C.; Katki, H.A.; Hocking, W.G.; Church, T.R.; Caporaso, N.; Kvale, P.A. Selection Criteria for Lung-Cancer Screening. N. Engl. J. Med. 2013, 368, 728–736. [Google Scholar] [CrossRef] [Green Version]
- Oudkerk, M.; Liu, S.; Heuvelmans, M.A.; Walter, J.E.; Field, J.K. Lung cancer LDCT screening and mortality reduction—Evidence, pitfalls and future perspectives. Nat. Rev. Clin. Oncol. 2021, 18, 135–151. Available online: http://www.nature.com/articles/s41571-020-00432-6 (accessed on 17 November 2020). [CrossRef]
- Zhao, X.; Han, R.-B.; Zhao, J.; Wang, J.; Yang, F.; Zhong, W. Comparison of epidermal growth factor receptor mutation statuses in tissue and plasma in stage I-IV non-small cell lung cancer patients. Respiration 2013, 85, 119–125. [Google Scholar] [CrossRef]
- Cho, M.-S.; Park, C.H.; Lee, S.; Park, H.S. Clinicopathological parameters for circulating tumor DNA shedding in surgically resected non-small cell lung cancer with EGFR or KRAS mutation. PLoS ONE 2020, 15, e0230622. [Google Scholar] [CrossRef] [Green Version]
- Hulbert, A.; Jusue-Torres, I.; Stark, A.; Chen, C.; Rodgers, K.; Lee, B.; Griffin, C.; Yang, A.; Huang, P.; Wrangle, J.; et al. Early Detection of Lung Cancer Using DNA Promoter Hypermethylation in Plasma and Sputum. Clin. Cancer Res. 2016, 23, 1998–2005. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Belinsky, S.A.; Leng, S.; Wu, G.; Thomas, C.L.; Picchi, M.A.; Lee, S.J. Gene Methylation Biomarkers in Sputum and Plasma as Predictors for Lung Cancer Recurrence. Cancer Prev. Res. 2017, 10, 635–640. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Roncarati, R.; Lupini, L.; Miotto, E.; Saccenti, E.; Mascetti, S.; Morandi, L. Molecular testing on bronchial washings for the diagnosis and predictive assessment of lung cancer. Mol. Oncol. 2020, 14, 2163–2175. [Google Scholar] [CrossRef]
- Sharma, S.; Kelly, T.K.; Jones, P.A. Epigenetics in cancer. Carcinogenesis 2009, 31, 27–36. [Google Scholar] [CrossRef] [PubMed]
- HOXA9 Homeobox A9 [Homo Sapiens (Human)]. Gene ID 3205. Available online: https://www.ncbi.nlm.nih.gov/gene/3205 (accessed on 17 November 2020).
- Bhatlekar, S.; Fields, J.Z.; Boman, B.M. HOX genes and their role in the development of human cancers. J. Mol. Med. 2014, 92, 811–823. [Google Scholar] [CrossRef] [PubMed]
- Hwang, J.-A.; Lee, B.B.; Kim, Y.; Hong, S.-H.; Kim, Y.-H.; Han, J. HOXA9 inhibits migration of lung cancer cells and its hypermethylation is associated with recurrence in non-small cell lung cancer. Mol. Carcinog. 2015, 54, E72–E80. [Google Scholar] [CrossRef] [PubMed]
- Yu, S.-L.; Lee, D.C.; Sohn, H.A.; Lee, S.Y.; Jeon, H.S.; Lee, J.H. Homeobox A9 directly targeted by miR-196b regulates aggressiveness through nuclear Factor-kappa B activity in non-small cell lung cancer cells. Mol. Carcinog. 2016, 55, 1915–1926. [Google Scholar] [CrossRef]
- Liu, B.; Filho, J.R.; Mallisetty, A.; Villani, C.; Kottorou, A.E.; Rodgers, K.P.; Chen, C.; Ito, T.; Holmes, K.; Gastala, N.; et al. Detection of Promoter DNA Methylation in Urine and Plasma Aids the Detection of Non–Small Cell Lung Cancer. Clin. Cancer Res. 2020, 26, 4339–4348. [Google Scholar] [CrossRef]
- Wen, S.W.C.; Andersen, R.F.; Hansen, T.F.; Nyhus, C.H.; Hager, H.; Hilberg, O.; Jakobsen, A. The prognostic impact of circulating homeobox A9 methylated DNA in advanced non-small cell lung cancer. Transl. Lung Cancer Res. 2021, 10, 855–865. [Google Scholar] [CrossRef]
- Thomsen, C.B.; Andersen, R.F.; Steffensen, K.D.; Adimi, P.; Jakobsen, A. Delta tocotrienol in recurrent ovarian cancer. A phase II trial. Pharmacol. Res. 2019, 141, 392–396. [Google Scholar] [CrossRef] [PubMed]
- Rusan, M.; Andersen, R.F.; Jakobsen, A.; Steffensen, K.D. Circulating HOXA9-methylated tumour DNA: A novel biomarker of response to poly (ADP-ribose) polymerase inhibition in BRCA-mutated epithelial ovarian cancer. Eur. J. Cancer 2020, 125, 121–129. [Google Scholar] [CrossRef]
- Wen, S.W.C.; Andersen, R.F.; Petersen, L.M.S.; Hager, H.; Hilberg, O.; Jakobsen, A. Comparison of Mutated KRAS and Methylated HOXA9 Tumor-Specific DNA in Advanced Lung Adenocarcinoma. Cancers 2020, 12, 3728. [Google Scholar] [CrossRef] [PubMed]
- Pallisgaard, N.; Spindler, K.-L.G.; Andersen, R.F.; Brandslund, I.; Jakobsen, A. Controls to validate plasma samples for cell free DNA quantification. Clin. Chim. Acta 2015, 446, 141–146. [Google Scholar] [CrossRef]
- Roperch, J.-P.; Incitti, R.; Forbin, S.; Bard, F.; Mansour, H.; Mesli, F.; Baumgaertner, I.; Brunetti, F.; Sobhani, I. Aberrant methylation of NPY, PENK, and WIF1 as a promising marker for blood-based diagnosis of colorectal cancer. BMC Cancer 2013, 13, 566. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ooki, A.; Maleki, Z.; Tsay, J.-C.; Goparaju, C.; Brait, M.; Turaga, N.; Nam, H.-S.; Rom, W.; Pass, H.; Sidransky, D.; et al. A Panel of Novel Detection and Prognostic Methylated DNA Markers in Primary Non–Small Cell Lung Cancer and Serum DNA. Clin. Cancer Res. 2017, 23, 7141–7152. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Villalba, M.; Exposito, F.; Pajares, M.J.; Sainz, C.; Redrado, M.; Remirez, A.; Wistuba, I.; Behrens, C.; Jantus-Lewintre, E.; Camps, C.; et al. TMPRSS4: A Novel Tumor Prognostic Indicator for the Stratification of Stage IA Tumors and a Liquid Biopsy Biomarker for NSCLC Patients. J. Clin. Med. 2019, 8, 2134. [Google Scholar] [CrossRef] [Green Version]
- TMPRSS4 Transmembrane Serine Protease 4 [Homo Sapiens (Human)]. Gene ID: 56649. Available online: https://www.ncbi.nlm.nih.gov/gene/56649 (accessed on 17 November 2020).
- Wong Doo, N.; Makalic, E.; Joo, J.E.; Vajdic, C.M.; Schmidt, D.F.; Wong, E.M. Global measures of peripheral blood-derived DNA methylation as a risk factor in the development of mature B-cell neoplasms. Epigenomics 2016, 8, 55–66. [Google Scholar] [CrossRef] [PubMed]
- Trivedi, C.M.; Patel, R.C.; Patel, C.V. Homeobox gene HOXA9 inhibits nuclear factor-kappa B dependent activation of endothelium. Atherosclerosis 2007, 195, e50–e60. [Google Scholar] [CrossRef]
- Heerink, W.J.; de Bock, G.H.; de Jonge, G.J.; Groen, H.J.M.; Vliegenthart, R.; Oudkerk, M. Complication rates of CT-guided transthoracic lung biopsy: Meta-analysis. Eur. Radiol. 2017, 27, 138–148. [Google Scholar] [CrossRef] [Green Version]




{kind=link}
{kind=link}
{kind=link}
| Variable | Discovery Cohort Cases (n = 67) | Discovery Cohort Controls (n = 34) | Validation Cohort Cases (n = 50) | Validation Cohort Controls (n = 45) |
|---|---|---|---|---|
| Basic information | ||||
| Age, years | 73 (65–77) | 64 (54–73) | 69 (63–77) | 63 (56–72) |
| Sex, male | 39/67 (58%) | 19/34 (56%) | 24/50 (48%) | 26/45 (58%) |
| Employment status, employed | 5/65 (8%) | 11/29 (38%) | 10/47 (21%) | 21/39 (54%) |
| Smoking status: | ||||
| Never | 7/67 (10%) | 6/34 (18%) | 2/50 (4%) | 13/45 (29%) |
| Ever | 60/67 (90%) | 28/34 (82%) | 48/50 (96%) | 32/45 (71%) |
| Pack years | 40 (20–50) | 20 (12–40) | 35 (21–50) | 15 (0–45) |
| Performance status: | ||||
| 0 | 27/67 (40%) | 19/33 (58%) | 34/49 (69%) | 30/42 (71%) |
| 1 | 27/67 (40%) | 9/33 (27%) | 10/49 (20%) | 10/42 (24%) |
| ≥2 | 13/67 (19%) | 5/33 (15%) | 5/49 (10%) | 2/42 (5%) |
| FEV1, liter | 1.87 (1.24–2.44) | 2.33 (1.52–2.99) | 2.09 (1.54–2.44) | 2.54 (1.95–2.85) |
| Comorbidity | ||||
| Any comorbidity | 58/67 (87%) | 28/34 (82%) | 43/50 (86%) | 37/45 (82%) |
| Cancer within 5 years | 26/67 (39%) | 9/34 (26%) | 5/50 (10%) | 3/45 (7%) |
| Previous lung cancer | 24/67 (36%) | 6/34 (18%) | 0/50 (0%) | 0/45 (0%) |
| Discovery Cohort | Validation Cohort | |||
|---|---|---|---|---|
| Variable | Cases (n = 67) | Controls (n = 34) | Cases (n = 50) | Controls (n = 45) |
| Tumor on CT scan | 60 | 11 | 50 | 28 |
| Largest mean diameter, mm | 27 (19–47) | 19 (13–22) | 42 (23–70) | 22 (14–50) |
| Localization | - | - | - | - |
| Central | 19/60 (28%) | 3/11 (27%) | 12/50 (24%) | 6/28 (21%) |
| Intermediate | 15/60 (22%) | 2/11 (18%) | 22/50 (44%) | 11/28 (39%) |
| Peripheral | 26/60 (39%) | 6/11 (55%) | 16/50 (32%) | 11/28 (39%) |
| Confirmed lung cancer | ||||
| Stage | - | - | - | |
| 1 | 18/65 (28%) | - | 5/48 (10%) | - |
| 2 | 7/65 (11%) | - | 14/48 (29%) | - |
| 3 | 16/65 (25%) | - | 16/48 (33%) | - |
| 4 | 24/65 (37%) | - | 13/48 (27%) | - |
| Histology | - | - | ||
| Adenocarcinoma | 32/67 (48%) | - | 34/50 (68%) | - |
| Squamous cell carcinoma | 22/67 (33%) | - | 8/50 (16%) | - |
| Small cell carcinoma | 6/67 (9%) | - | 3/50 (6%) | - |
| Other non-small cell lung cancer | 7/67 (10%) | - | 5/50 (10%) | - |
| Discovery Cohort | Validation Cohort | |||||
|---|---|---|---|---|---|---|
| Diagnosis | HOXA9+ | HOXA9− | Total | HOXA9+ | HOXA9− | Total |
| Lung cancer | 49 | 18 | 67 | 40 | 10 | 50 |
| No lung cancer | 5 | 29 | 34 | 11 | 34 | 45 |
| Total | 54 | 47 | 101 | 51 | 44 | 95 |
| Sensitivity (95% CI) | 73.1% (60.9%–83.2%) | 80.0% (66.3%–90.0%) | ||||
| Specificity (95% CI) | 85.3% (68.9%–95.0%) | 75.6% (60.5%–87.1%) | ||||
| PPV (95% CI) | 90.7% (79.7%–96.9%) | 78.4% (64.7%–88.7%) | ||||
| NPV (95% CI) | 61.7% (46.4%–75.5%) | 77.3% (62.2%–88.5%) | ||||
| Discovery Cohort | Validation Cohort | |||||
|---|---|---|---|---|---|---|
| Cases (n = 67) | Controls (n = 34) | Cases (n = 50) | Controls (n = 45) | |||
| Variables | OR (95% CI) | OR (95% CI) | p-Value | OR (95% CI) | OR (95% CI) | p-Value |
| Age, years | - | - | - | - | - | - |
| Crude OR | 1 (ref) | 1.06 (1.02–1.11) | 0.002 * | 1 (ref) | 1.08 (1.03–1.13) | 0.001 * |
| Adjusted OR | 1 (ref) | 1.06 (1.01–1.11) | 0.023 * | 1 (ref) | 1.07 (1.01–1.14) | 0.020 * |
| Smoking status, ever | - | - | - | - | - | - |
| Percentage ever smoked | 89.6% | 82.4% | 0.307 | 96.0% | 71.1% | 0.001 * |
| Crude OR | 1 (ref) | 1.84 (0.56–5.97) | 0.312 | 1 (ref) | 9.75 (2.06–46.14) | 0.004 * |
| Adjusted OR | 1 (ref) | 1.07 (0.24–4.74) | 0.928 | 1 (ref) | 5.20 (0.82–32.95) | 0.080 |
| HOXA9 status | - | - | - | - | - | - |
| Percentage HOXA9+ | 68.7% | 11.8% | <0.001 * | 80.0% | 24.4% | <0.001 * |
| Crude OR | 1 (ref) | 15.80 (5.30–47.06) | <0.001 * | 1 (ref) | 12.36 (4.68–32.64) | <0.001 * |
| Adjusted OR | 1 (ref) | 14.27 (4.62–44.06) | <0.001 * | 1 (ref) | 11.95 (4.11–34.75) | <0.001 * |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Wen, S.W.C.; Andersen, R.F.; Rasmussen, K.; Thomsen, C.B.; Hansen, T.F.; Nederby, L.; Hager, H.; Jakobsen, A.; Hilberg, O. Validating Methylated HOXA9 in Bronchial Lavage as a Diagnostic Tool in Patients Suspected of Lung Cancer. Cancers 2021, 13, 4223. https://doi.org/10.3390/cancers13164223
Wen SWC, Andersen RF, Rasmussen K, Thomsen CB, Hansen TF, Nederby L, Hager H, Jakobsen A, Hilberg O. Validating Methylated HOXA9 in Bronchial Lavage as a Diagnostic Tool in Patients Suspected of Lung Cancer. Cancers. 2021; 13(16):4223. https://doi.org/10.3390/cancers13164223
Chicago/Turabian StyleWen, Sara W. C., Rikke F. Andersen, Kristian Rasmussen, Caroline Brenner Thomsen, Torben Frøstrup Hansen, Line Nederby, Henrik Hager, Anders Jakobsen, and Ole Hilberg. 2021. "Validating Methylated HOXA9 in Bronchial Lavage as a Diagnostic Tool in Patients Suspected of Lung Cancer" Cancers 13, no. 16: 4223. https://doi.org/10.3390/cancers13164223