
Clonal Hematopoiesis after Autologous Stem Cell Transplantation Does Not Confer Adverse Prognosis in Patients with AML

 and
and
Abstract
:Simple Summary
Abstract
1. Introduction
2. Materials and Methods
2.1. Study Design and Patients
2.2. Treatment
2.3. Risk and Response Assessment
2.4. Survival
2.5. Molecular Analyses
2.6. Assessment and Definition of Clonal Hematopoiesis
2.7. Statistical Analyses
3. Results
3.1. Patients
3.2. Treatment
3.3. Clonal Hematopoiesis
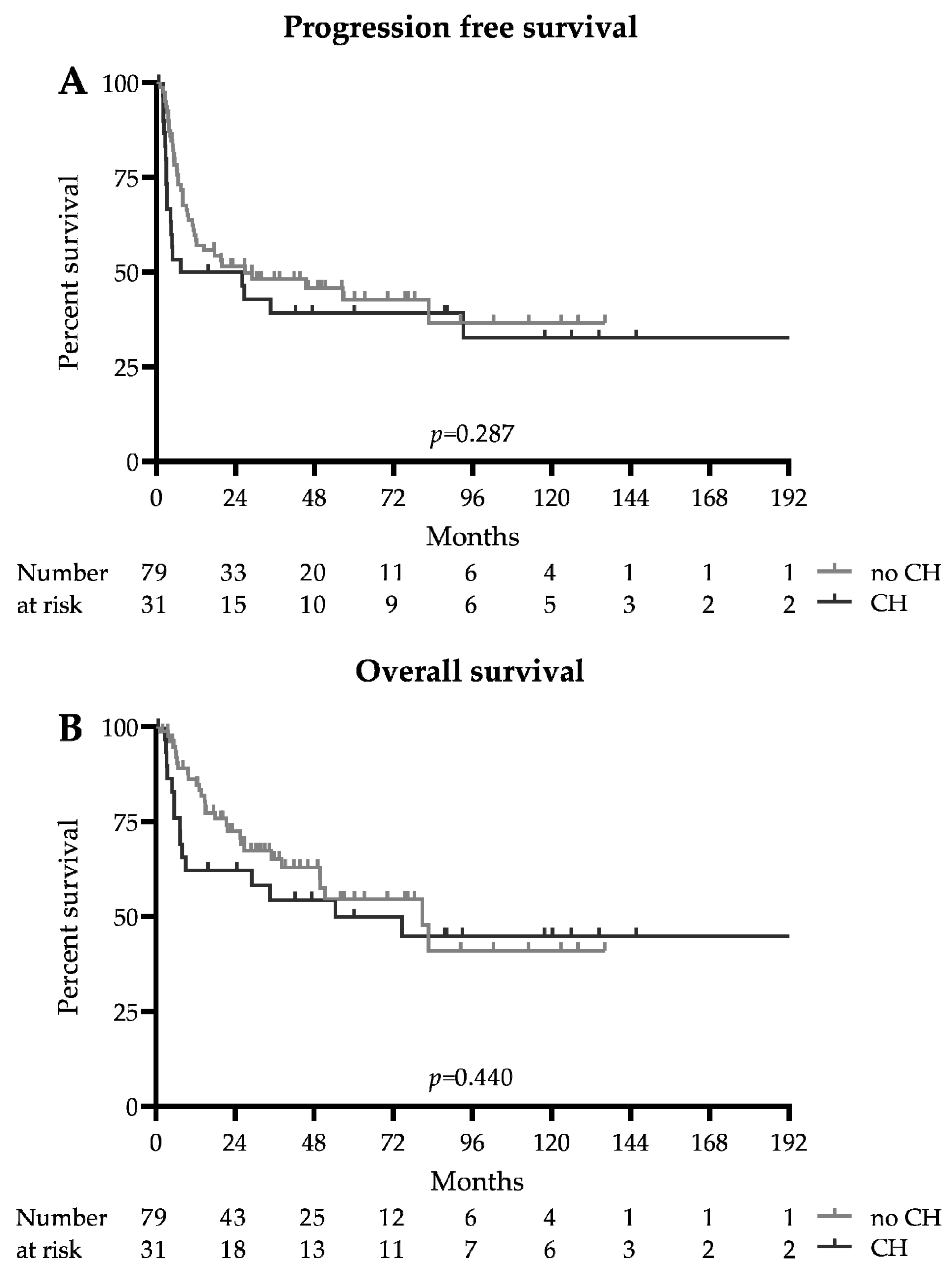
3.4. Survival Analysis
3.5. Survival of DTA Subgroups
3.6. Secondary Malignancies
3.7. Different VAF Cutoffs
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Döhner, H.; Estey, E.; Grimwade, D.; Amadori, S.; Appelbaum, F.R.; Büchner, T.; Dombret, H.; Ebert, B.L.; Fenaux, P.; Larson, R.A.; et al. Diagnosis and management of AML in adults: 2017 ELN recommendations from an international expert panel. Blood 2017, 129, 424–447. [Google Scholar] [CrossRef] [Green Version]
- Wetzel, D.; Mueller, B.U.; Mansouri Taleghani, B.; Baerlocher, G.M.; Seipel, K.; Leibundgut, K.; Pabst, T. Delayed Haematological recovery after autologous stem cell transplantation is associated with favourable outcome in acute myeloid leukaemia. Br. J. Haematol. 2015, 168, 268–273. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- de Benito, A.S.; Jeker, B.; Gfeller, E.; Porret, N.; Banz, Y.; Novak, U.; Bacher, U.; Pabst, T. Molecular minimal residual disease negativity and decreased stem cell mobilization potential predict excellent outcome after autologous transplant in NPM1 mutant acute myeloid leukemia. Haematologica 2020, 105, e9–e12. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Jongen-Lavrencic, M.; Grob, T.; Hanekamp, D.; Kavelaars, F.G.; Al Hinai, A.; Zeilemaker, A.; Erpelinck-Verschueren, C.A.J.; Gradowska, P.L.; Meijer, R.; Cloos, J.; et al. Molecular Minimal Residual Disease in Acute Myeloid Leukemia. N. Engl. J. Med. 2018, 378, 1189–1199. [Google Scholar] [CrossRef]
- Flach, J.; Shumilov, E.; Joncourt, R.; Porret, N.; Tchinda, J.; Legros, M.; Scarpelli, I.; Hewer, E.; Novak, U.; Schoumans, J.; et al. Detection of rare reciprocal RUNX1 rearrangements by next-generation sequencing in acute myeloid leukemia. Genes Chromosom. Cancer 2020, 59, 268–274. [Google Scholar] [CrossRef] [PubMed]
- Flach, J.; Shumilov, E.; Wiedemann, G.; Porret, N.; Shakhanova, I.; Bürki, S.; Legros, M.; Joncourt, R.; Pabst, T.; Bacher, U. Clinical potential of introducing next-generation sequencing in patients at relapse of acute myeloid leukemia. Hematol. Oncol. 2020, 38, 425–431. [Google Scholar] [CrossRef] [PubMed]
- Shumilov, E.; Flach, J.; Kohlmann, A.; Banz, Y.; Bonadies, N.; Fiedler, M.; Pabst, T.; Bacher, U. Current status and trends in the diagnostics of AML and MDS. Blood Rev. 2018, 32, 508–519. [Google Scholar] [CrossRef] [PubMed]
- Shlush, L.I. Age-related clonal hematopoiesis. Blood 2018, 131, 496–504. [Google Scholar] [CrossRef] [Green Version]
- Bacher, U.; Shumilov, E.; Flach, J.; Porret, N.; Joncourt, R.; Wiedemann, G.; Fiedler, M.; Novak, U.; Amstutz, U.; Pabst, T. Challenges in the introduction of next-generation sequencing (NGS) for diagnostics of myeloid malignancies into clinical routine use. Blood Cancer J. 2018, 8, 113. [Google Scholar] [CrossRef] [Green Version]
- Steensma, D.P.; Bejar, R.; Jaiswal, S.; Lindsley, R.C.; Sekeres, M.A.; Hasserjian, R.P.; Ebert, B.L. Clonal hematopoiesis of indeterminate potential and its distinction from myelodysplastic syndromes. Blood 2015, 126, 9–16. [Google Scholar] [CrossRef] [Green Version]
- Genovese, G.; Kähler, A.K.; Handsaker, R.E.; Lindberg, J.; Rose, S.A.; Bakhoum, S.F.; Chambert, K.; Mick, E.; Neale, B.M.; Fromer, M. Clonal hematopoiesis and blood-cancer risk inferred from blood DNA sequence. N. Engl. J. Med. 2014, 371, 2477–2487. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Jaiswal, S.; Fontaninallas, P.; Flannick, J.; Manning, A.; Grauman, P.V.; Mar, B.G.; Lindsley, R.C.; Mermel, C.H.; Burtt, N.; Chavez, A.; et al. Age-related clonal hematopoiesis associated with adverse outcomes. N. Engl. J. Med. 2014, 371, 2488–2498. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mueller, B.U.; Seipel, K.; Bacher, U.; Pabst, T. Autologous transplantation for older adults with AML. Cancers 2018, 10, 340. [Google Scholar] [CrossRef] [Green Version]
- Sula, M.; Bacher, U.; Oppliger-Leibundgut, E.; Mansouri Taleghani, B.; Novak, U.; Pabst, T. Excellent outcome after consolidation with autologous transplantation in patients with core binding factor acute myeloid leukemia. Bone Marrow Transplant. 2020, 55, 1690–1693. [Google Scholar] [CrossRef]
- von Grünigen, I.; Raschle, J.; Rüsges-Wolter, I.; Taleghani Behrouz, M.; Mueller, B.U.; Pabst, T. The relapse risk of AML patients undergoing autologous transplantation correlates with the stem cell mobilizing potential. Leuk. Res. 2012, 36, 1325–1329. [Google Scholar] [CrossRef]
- Cheson, B.D.; Bennett, J.M.; Kopecky, K.J.; Büchner, T.; Willman, C.L.; Estey, E.H.; Schiffer, C.A.; Doehner, H.; Tallman, M.S.; Lister, T.A.; et al. Revised Recommendations of the International Working Group for diagnosis, standardization of response criteria, treatment outcomes, and reporting standards for therapeutic trials in acute myeloid leukemia. J. Clin. Oncol. 2003, 21, 4642–4649. [Google Scholar] [CrossRef] [PubMed]
- Serratì, S.; de Summa, S.; Pilato, B.; Petriella, D.; Lacalamita, R.; Tommasi, S.; Pinto, R. Next-generation sequencing: Advances and applications in cancer diagnosis. Onco Targets. Ther. 2016, 9, 7355–7365. [Google Scholar] [CrossRef] [Green Version]
- Young, A.L.; Spencer Tong, R.; Birmann, B.M.; Druley, T.E. Clonal hematopoiesis and risk of acute myeloid leukemia. Haematologica 2019, 104, 2410–2417. [Google Scholar] [CrossRef] [Green Version]
- Abelson, S.; Collord, G.; Ng, S.W.K.; Weissbrod, O.; Mendelson Cohen, N.; Niemeyer, E.; Barda, N.; Zuzarte, P.C.; Heisler, L.; Sundaravadanam, Y.; et al. Prediction of acute myeloid leukaemia risk in healthy individuals. Nature 2018, 559, 400–404. [Google Scholar] [CrossRef]
- Desai, P.; Mencia-Trinchant, N.; Savenkov, O.; Simon, M.S.; Cheang, G.; Lee, S.; Samuel, M.; Ritchie, E.K.; Guzman, M.L.; Ballman, K.V.; et al. Somatic mutations precede acute myeloid leukemia years before diagnosis. Nat. Med. 2018, 24, 1015–1023. [Google Scholar] [CrossRef]
- Grimm, J.; Bill, M.; Jentzsch, M.; Beinicke, S.; Häntschel, J.; Goldmann, K.; Schulz, J.; Cross, M.; Franke, G.N.; Behre, G.; et al. Clinical impact of clonal hematopoiesis in acute myeloid leukemia patients receiving allogeneic transplantation. Bone Marrow Transplant. 2019, 54, 1189–1197. [Google Scholar] [CrossRef]
- Mouhieddine, T.H.; Sperling, A.S.; Redd, R.; Park, J.; Leventhal, M.; Gibson, C.J.; Manier, S.; Nassar, A.H.; Capelletti, M.; Huynh, D.; et al. Clonal hematopoiesis is associated with adverse outcomes in multiple myeloma patients undergoing transplant. Nat. Commun. 2020, 11, 2996. [Google Scholar] [CrossRef] [PubMed]
- Gibson, C.J.; Lindsley, R.C.; Tchekmedyian, V.; Mar, B.G.; Shi, J.; Jaiswal, S.; Bosworth, A.; Francisco, L.; He, J.; Bansal, A.; et al. Clonal hematopoiesis associated with adverse outcomes after autologous stem-cell transplantation for lymphoma. J. Clin. Oncol. 2017, 35, 1598–1605. [Google Scholar] [CrossRef] [PubMed]
- Gibson, C.J.; Kim, H.T.; Murdock, H.M.; Hambley, B.; Zhao, L.; Green, L.; Fleharty, M.; Blumenstiel, B.; Cibulskis, C.; Gocke, C.D.; et al. DNMT3A clonal hematopoiesis in older donors is associated with improved survival in recipients after allogeneic hematopoietic cell transplant. Blood 2020, 136, 26. [Google Scholar] [CrossRef]
- Shlush, L.I.; Zandi, S.; Mitchell, A.; Chen, W.C.; Brandwein, J.M.; Gupta, V.; Kennedy, J.A.; Schimmer, A.D.; Schuh, A.C.; Yee, K.W.; et al. Identification of pre-leukaemic haematopoietic stem cells in acute leukaemia. Nature 2014, 506, 328–333. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| Parameter | DTA-CH (n = 31) | No CH (n = 79) | Total (n = 110) | p |
|---|---|---|---|---|
| Demographics | ||||
| Female sex—no. (%) | 17 (55) | 45 (44) | 52 (47) | 0.397 |
| Median age—years (IQR) | 54 (41–63) | 54 (40–61) | 54 (40–61) | 0.415 |
| Parameters at Diagnosis, Median (Range) | ||||
| Leukocytes (G/L) | 16.2 (1.2–303) | 7.0 (0.6–240) | 8.6 (0.6–303) | 0.262 |
| Neutrophils (G/L) | 1.7 (0.2–50.2) | 1.1 (0.0–19.4) | 1.4 (0.0–50.2) | 0.035 |
| Platelets (G/L) | 80 (9–268) | 63 (7–714) | 69 (7–714) | 0.586 |
| Hemoglobin (g/L) | 99 (61–137) | 89 (37–151) | 95 (37–151) | 0.163 |
| Peripheral blasts (%) | 44 (0–94) | 41 (0–97) | 44 (0–97) | 0.924 |
| Bone marrow blasts (%) | 75 (30–95) | 80 (0–95) | 80 (0–95) | 0.646 |
| ELN Risk Groups—no. (%) | ||||
| Favorable | 14 (45) | 40 (51) | 54 (49) | 0.674 |
| t(8;21)/RUNX1-RUNX1T1 | 2 (7) | 9 (11) | 11 (10) | 0.725 |
| inv(16)/CBFB-MYH11 | 2 (7) | 8 (10) | 10 (9) | 0.722 |
| Mut. CEBPA | 1 (3) | 4 (5) | 5 (5) | >0.999 |
| Mut. NPM1 w/o FLT3-ITD/FLT3-ITD (low allelic ratio) | 9 (29) | 19 (24) | 28 (26) | 0.630 |
| Intermediate | 15 (48) | 33 (42) | 52 (43) | 0.670 |
| Mut. NPM1 and FLT3-ITD (high allelic ratio) | 6 (19) | 4 (5) | 10 (9) | 0.029 |
| NOS | 9 (29) | 29 (37) | 38 (35) | 0.509 |
| Adverse | 2 (7) | 6 (8) | 8 (7) | >0.999 |
| Wild-type NPM1 and FLT3-ITD (high allelic ratio) | 2 (7) | 1 (1) | 3 (3) | 0.191 |
| Monosomal or complex karyotype | 0 | 2 (3) | 2 (2) | >0.999 |
| t(v;11)/KMT2A rearranged | 0 | 1 (1) | 1 (1) | >0.999 |
| Mut. RUNX1 | 0 | 1 (1) | 1 (1) | >0.999 |
| Mut. TP53 | 0 | 1 (1) | 1 (1) | >0.999 |
| High-Dose Chemotherapy and Autologous Stem Cell Transplantation | ||||
| Conditioning regimen—no. (%) | ||||
| Busulfan/Cyclophosphamide | 25 (80) | 63 (80) | 88 (80) | >0.999 |
| Busulfan/Melphalan | 4 (13) | 9 (11) | 13 (12) | >0.999 |
| Treosulfan/Melphalan | 2 (7) | 7 (9) | 9 (8) | >0.999 |
| Median time to ASCT (IQR)—months | 3.4 (3.2–3.8) | 3.7 (3.2–4.5) | 3.7 (3.2–4.3) | 0.153 |
| Median CD34+ transfused—106/kg BW | 3.81 (3.1–5.2) | 4.20 (3.3–5.2) | 4.17 (3.2–5.2) | 0.448 |
| Parameter | CH (n = 31) | No CH (n = 79) | p |
|---|---|---|---|
| Survival | |||
| Median follow up for OS—months | 93.0 | 46.1 | - |
| Median progression free survival—months | 16.7 | 26.9 | 0.287 |
| Median overall survival—months | 54.4 | 80.9 | 0.440 |
| 2-year progression free survival probability (95% CI) | 0.39 (0.34–0.57) | 0.46 (0.22–0.56) | 0.391 |
| 2-year overall survival probability (95%CI) | 0.54 (0.35–0.71) | 0.63 (0.49–0.73) | 0.251 |
| 30-day mortality—no. (%) | 0 | 0 | >0.999 |
| Allogeneic transplantation in CR2—no. (%) | 6 (19) | 19 (24) | 0.801 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Heini, A.D.; Porret, N.; Zenhaeusern, R.; Winkler, A.; Bacher, U.; Pabst, T. Clonal Hematopoiesis after Autologous Stem Cell Transplantation Does Not Confer Adverse Prognosis in Patients with AML. Cancers 2021, 13, 3190. https://doi.org/10.3390/cancers13133190
Heini AD, Porret N, Zenhaeusern R, Winkler A, Bacher U, Pabst T. Clonal Hematopoiesis after Autologous Stem Cell Transplantation Does Not Confer Adverse Prognosis in Patients with AML. Cancers. 2021; 13(13):3190. https://doi.org/10.3390/cancers13133190
Chicago/Turabian StyleHeini, Alexander D., Naomi Porret, Reinhard Zenhaeusern, Annette Winkler, Ulrike Bacher, and Thomas Pabst. 2021. "Clonal Hematopoiesis after Autologous Stem Cell Transplantation Does Not Confer Adverse Prognosis in Patients with AML" Cancers 13, no. 13: 3190. https://doi.org/10.3390/cancers13133190