
A Randomized Trial of Precision Prevention Materials to Improve Primary and Secondary Melanoma Prevention Activities among Individuals with Limited Melanoma Risk Phenotypes

 , , ,
, , ,
Abstract
:Simple Summary
Abstract

1. Introduction
2. Materials and Methods
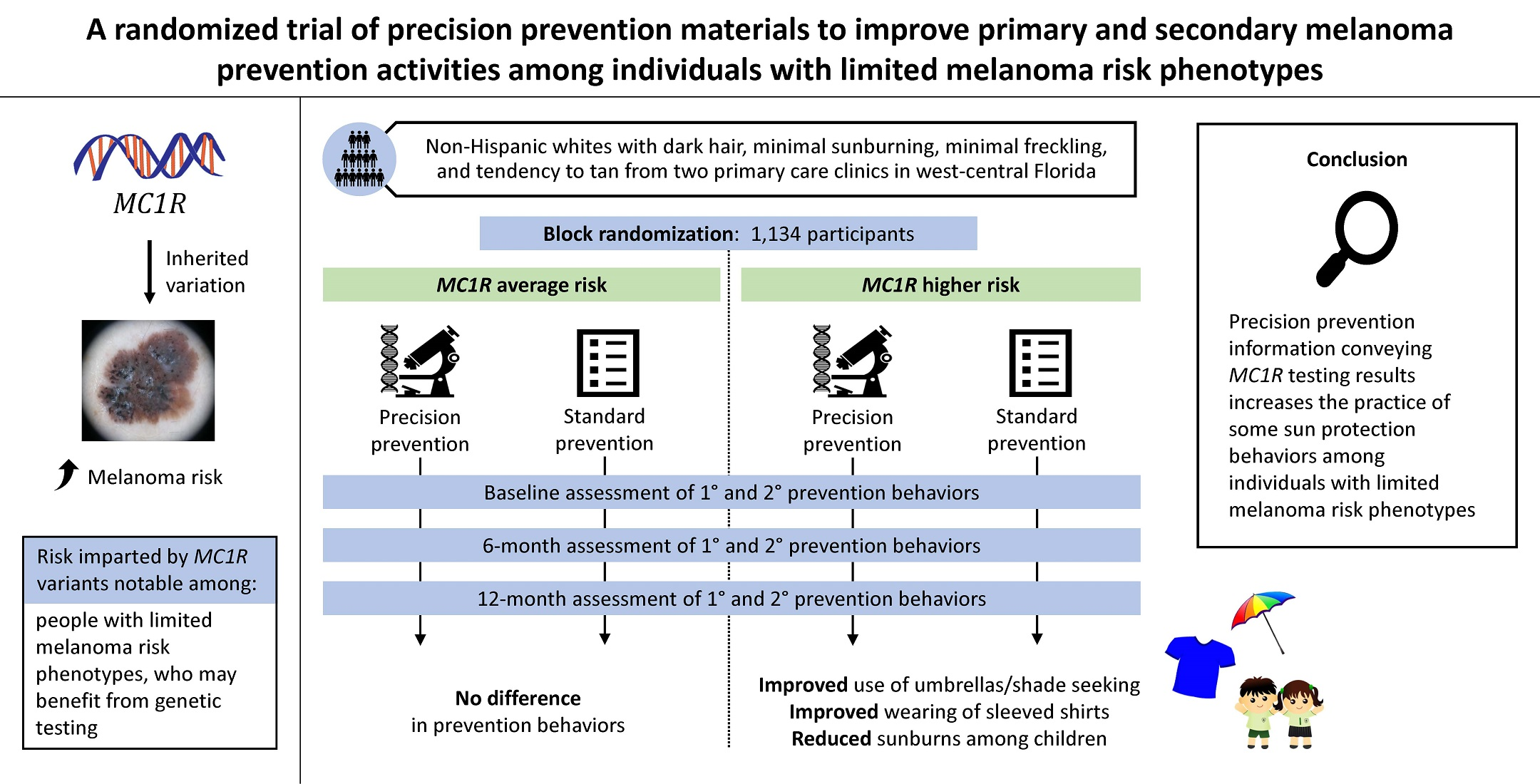
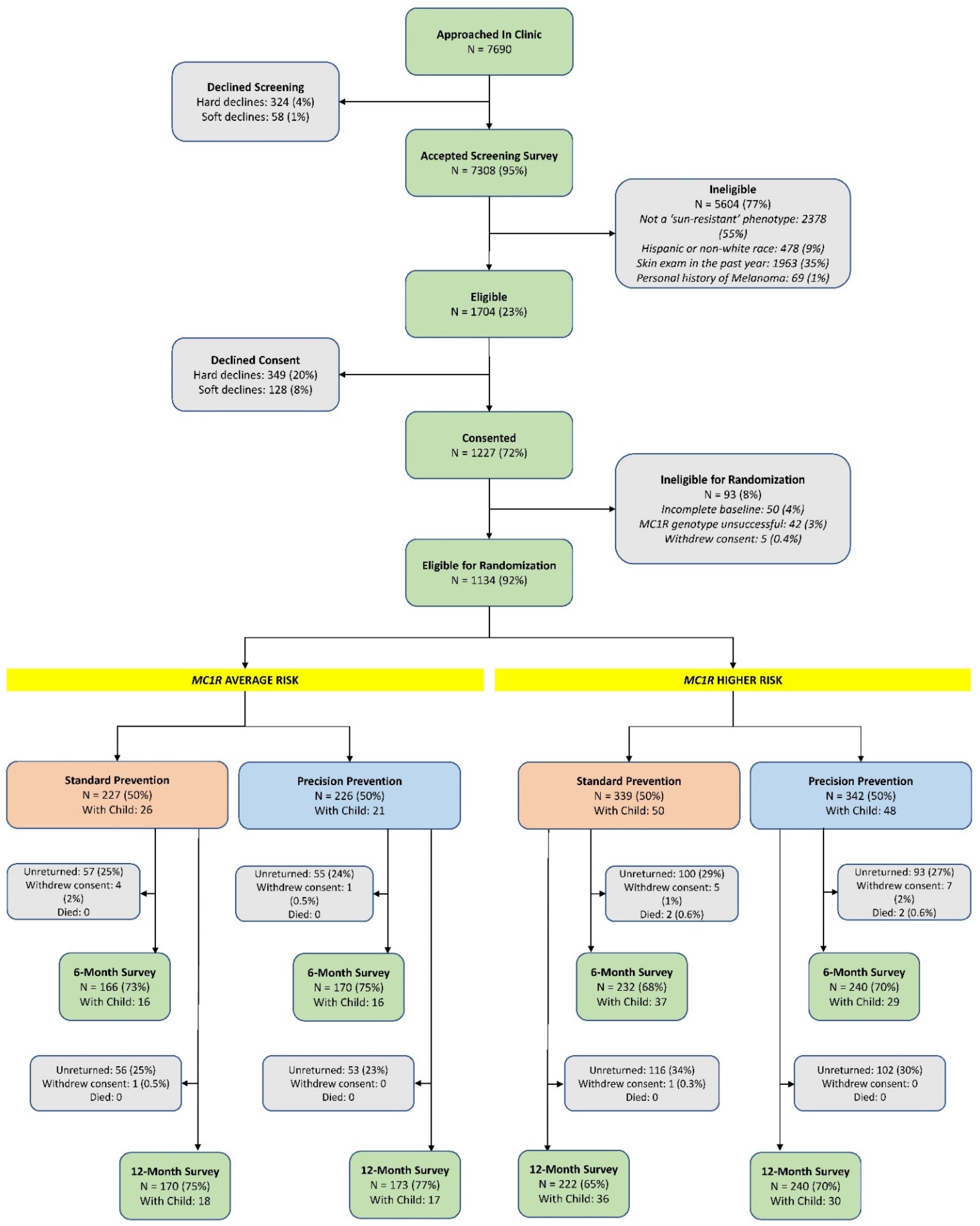
2.1. Setting and Participants
2.2. Biospecimens and Genotyping
2.3. Randomization and Mailed Prevention Materials
2.4. Study Assessments
2.5. Statistical Analysis
3. Results
3.1. MC1R Average-Risk Participants
3.2. MC1R Higher-Risk Participants
3.3. Children of Participants
3.4. Per Protocol Analyses
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Erdmann, F.; Lortet-Tieulent, J.; Schuz, J.; Zeeb, H.; Greinert, R.; Breitbart, E.W.; Bray, F. International trends in the incidence of malignant melanoma 1953–2008—Are recent generations at higher or lower risk? Int. J. Cancer 2013, 132, 385–400. [Google Scholar] [CrossRef] [PubMed]
- Olsen, C.M.; Green, A.C.; Pandeya, N.; Whiteman, D.C. Trends in Melanoma Incidence Rates in Eight Susceptible Populations through 2015. J. Investig. Dermatol. 2019, 139, 1392–1395. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gandini, S.; Sera, F.; Cattaruzza, M.S.; Pasquini, P.; Picconi, O.; Boyle, P.; Melchi, C.F. Meta-analysis of risk factors for cutaneous melanoma: II. Sun exposure. Eur. J. Cancer 2005, 41, 45–60. [Google Scholar] [CrossRef] [PubMed]
- Wu, Y.P.; Aspinwall, L.G.; Conn, B.M.; Stump, T.; Grahmann, B.; Leachman, S.A. A systematic review of interventions to improve adherence to melanoma preventive behaviors for individuals at elevated risk. Prev. Med. 2016, 88, 153–167. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mulliken, J.S.; Russak, J.E.; Rigel, D.S. The effect of sunscreen on melanoma risk. Dermatol. Clin. 2012, 30, 369–376. [Google Scholar] [CrossRef]
- Henrikson, N.B.; Morrison, C.C.; Blasi, P.R.; Nguyen, M.; Shibuya, K.C.; Patnode, C.D. Behavioral Counseling for Skin Cancer Prevention: Evidence Report and Systematic Review for the US Preventive Services Task Force. JAMA 2018, 319, 1143–1157. [Google Scholar] [CrossRef]
- Forsea, A.M. Melanoma Epidemiology and Early Detection in Europe: Diversity and Disparities. Dermatol. Pract. Concept. 2020, 10, e2020033. [Google Scholar] [CrossRef]
- Chiaravalloti, A.J.; Laduca, J.R. Melanoma screening by means of complete skin exams for all patients in a dermatology practice reduces the thickness of primary melanomas at diagnosis. J. Clin. Aesthet. Dermatol. 2014, 7, 18–22. [Google Scholar]
- Coups, E.J.; Manne, S.L.; Heckman, C.J. Multiple skin cancer risk behaviors in the U.S. population. Am. J. Prev. Med. 2008, 34, 87–93. [Google Scholar] [CrossRef]
- Hay, J.; Coups, E.J.; Ford, J.; DiBonaventura, M. Exposure to mass media health information, skin cancer beliefs, and sun protection behaviors in a United States probability sample. J. Am. Acad. Dermatol. 2009, 61, 783–792. [Google Scholar] [CrossRef] [Green Version]
- Gerstenblith, M.R.; Shi, J.; Landi, M.T. Genome-wide association studies of pigmentation and skin cancer: A review and meta-analysis. Pigment. Cell Melanoma Res. 2010, 23, 587–606. [Google Scholar] [CrossRef]
- Pasquali, E.; Garcia-Borron, J.C.; Fargnoli, M.C.; Gandini, S.; Maisonneuve, P.; Bagnardi, V.; Specchia, C.; Liu, F.; Kayser, M.; Nijsten, T.; et al. MC1R variants increased the risk of sporadic cutaneous melanoma in darker-pigmented Caucasians: A pooled-analysis from the M-SKIP project. Int. J. Cancer 2015, 136, 618–631. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kanetsky, P.A.; Panossian, S.; Elder, D.E.; Guerry, D.; Ming, M.E.; Schuchter, L.; Rebbeck, T.R. Does MC1R genotype convey information about melanoma risk beyond risk phenotypes? Cancer 2010, 116, 2416–2428. [Google Scholar] [CrossRef] [Green Version]
- Raimondi, S.; European Institute of Oncology (IEO), IRCCS, Milan, Italy. Personal communication, 2020.
- Rogers, R.; Cacioppo, J.; Petty, R. Cognitive and physiological processes in fear-based attitude change: A revised theory of protection motivation. In Social Psychophysiology: A Sourcebook; Guilford Press: New York, NY, USA, 1983; pp. 153–176. [Google Scholar]
- Fitzpatrick, T.B. The validity and practicality of sun-reactive skin types I through VI. Arch. Dermatol 1988, 124, 869–871. [Google Scholar] [CrossRef] [PubMed]
- Sunyaev, S.; Ramensky, V.; Bork, P. Towards a structural basis of human non-synonymous single nucleotide polymorphisms. Trends Genet. 2000, 16, 198–200. [Google Scholar] [CrossRef]
- Hay, J.L.; Berwick, M.; Zielaskowski, K.; White, K.A.; Rodriguez, V.M.; Robers, E.; Guest, D.D.; Sussman, A.; Talamantes, Y.; Schwartz, M.R.; et al. Implementing an Internet-Delivered Skin Cancer Genetic Testing Intervention to Improve Sun Protection Behavior in a Diverse Population: Protocol for a Randomized Controlled Trial. JMIR Res. Protoc 2017, 6, e52. [Google Scholar] [CrossRef] [Green Version]
- Rodriguez, V.M.; Robers, E.; Zielaskowski, K.; Javier Gonzalez, C.; Hunley, K.; Kaphingst, K.A.; Guest, D.D.; Sussman, A.; Meyer White, K.A.; Schwartz, M.R.; et al. Translation and adaptation of skin cancer genomic risk education materials for implementation in primary care. J. Community Genet. 2017, 8, 53–63. [Google Scholar] [CrossRef] [Green Version]
- Chew, L.D.; Bradley, K.A.; Boyko, E.J. Brief questions to identify patients with inadequate health literacy. Fam. Med. 2004, 36, 588–594. [Google Scholar] [PubMed]
- Figueroa, J.D.; Garcia-Closas, M.; Humphreys, M.; Platte, R.; Hopper, J.L.; Southey, M.C.; Apicella, C.; Hammet, F.; Schmidt, M.K.; Broeks, A.; et al. Associations of common variants at 1p11.2 and 14q24.1 (RAD51L1) with breast cancer risk and heterogeneity by tumor subtype: Findings from the Breast Cancer Association Consortium. Hum. Mol. Genet. 2011, 20, 4693–4706. [Google Scholar] [CrossRef] [Green Version]
- Glanz, K.; Yaroch, A.L.; Dancel, M.; Saraiya, M.; Crane, L.A.; Buller, D.B.; Manne, S.; O’Riordan, D.L.; Heckman, C.J.; Hay, J.; et al. Measures of sun exposure and sun protection practices for behavioral and epidemiologic research. Arch. Dermatol. 2008, 144, 217–222. [Google Scholar] [CrossRef] [Green Version]
- Aspinwall, L.G.; Taber, J.M.; Leaf, S.L.; Kohlmann, W.; Leachman, S.A. Genetic testing for hereditary melanoma and pancreatic cancer: A longitudinal study of psychological outcome. Psychooncology 2013, 22, 276–289. [Google Scholar] [CrossRef]
- Lerman, C.; Daly, M.; Masny, A.; Balshem, A. Attitudes about genetic testing for breast-ovarian cancer susceptibility. J. Clin. Oncol. 1994, 12, 843–850. [Google Scholar] [CrossRef]
- Hock, K.T.; Christensen, K.D.; Yashar, B.M.; Roberts, J.S.; Gollust, S.E.; Uhlmann, W.R. Direct-to-consumer genetic testing: An assessment of genetic counselors’ knowledge and beliefs. Genet. Med. 2011, 13, 325–332. [Google Scholar] [CrossRef] [Green Version]
- Glanz, K.; Volpicelli, K.; Kanetsky, P.A.; Ming, M.E.; Schuchter, L.M.; Jepson, C.; Domchek, S.M.; Armstrong, K. Melanoma genetic testing, counseling, and adherence to skin cancer prevention and detection behaviors. Cancer Epidemiol. Biomark. Prev. 2013, 22, 607–614. [Google Scholar] [CrossRef] [Green Version]
- Stump, T.K.; Aspinwall, L.G.; Drummond, D.M.; Taber, J.M.; Kohlmann, W.; Champine, M.; Cassidy, P.B.; Petrie, T.; Liley, B.; Leachman, S.A. CDKN2A testing and genetic counseling promote reductions in objectively measured sun exposure one year later. Genet. Med. 2020, 22, 26–34. [Google Scholar] [CrossRef] [PubMed]
- Aspinwall, L.G.; Taber, J.M.; Kohlmann, W.; Leaf, S.L.; Leachman, S.A. Unaffected family members report improvements in daily routine sun protection 2 years following melanoma genetic testing. Genet. Med. 2014, 16, 846–853. [Google Scholar] [CrossRef] [Green Version]
- Frieser, M.J.; Wilson, S.; Vrieze, S. Behavioral impact of return of genetic test results for complex disease: Systematic review and meta-analysis. Health Psychol. 2018, 37, 1134–1144. [Google Scholar] [CrossRef]
- McCambridge, J.; Witton, J.; Elbourne, D.R. Systematic review of the Hawthorne effect: New concepts are needed to study research participation effects. J. Clin. Epidemiol. 2014, 67, 267–277. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Behrens, C.L.; Thorgaard, C.; Philip, A.; Bentzen, J. Sunburn in children and adolescents: Associations with parents’ behaviour and attitudes. Scand. J. Public Health 2013, 41, 302–310. [Google Scholar] [CrossRef]
- Holman, D.M.; Watson, M. Correlates of Intentional Tanning Among Adolescents in the United States: A Systematic Review of the Literature. J. Adolesc. Health 2013, 52, S52–S59. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hoerster, K.D.; Mayer, J.A.; Woodruff, S.I.; Malcarne, V.; Roesch, S.C.; Clapp, E. The influence of parents and peers on adolescent indoor tanning behavior: Findings from a multi-city sample. J. Am. Acad. Dermatol. 2007, 57, 990–997. [Google Scholar] [CrossRef] [Green Version]
- Cokkinides, V.E.; Bandi, P.; Weinstock, M.A.; Ward, E. Use of sunless tanning products among US adolescents aged 11 to 18 years. Arch. Dermatol. 2010, 146, 987–992. [Google Scholar] [CrossRef]
- Whiteman, D.C.; Whiteman, C.A.; Green, A.C. Childhood sun exposure as a risk factor for melanoma: A systematic review of epidemiologic studies. Cancer Causes Control 2001, 12, 69–82. [Google Scholar] [CrossRef]
- Green, A.C.; Wallingford, S.C.; McBride, P. Childhood exposure to ultraviolet radiation and harmful skin effects: Epidemiological evidence. Prog. Biophys. Mol. Biol. 2011, 107, 349–355. [Google Scholar] [CrossRef] [Green Version]
- Koch, S.; Pettigrew, S.; Hollier, L.P.; Slevin, T.; Strickland, M.; Minto, C.; Jalleh, G.; Lin, C. Trends in Australian adolescents’ sun-protection behaviours: Implications for health campaigns. Aust. N. Z. J. Public Health 2016, 40, 468–473. [Google Scholar] [CrossRef] [Green Version]
- Gorig, T.; Diehl, K.; Greinert, R.; Breitbart, E.W.; Schneider, S. Prevalence of sun-protective behaviour and intentional sun tanning in German adolescents and adults: Results of a nationwide telephone survey. J. Eur. Acad. Dermatol. Venereol. 2018, 32, 225–235. [Google Scholar] [CrossRef]
- Shuk, E.; Burkhalter, J.E.; Baguer, C.F.; Holland, S.M.; Pinkhasik, A.; Brady, M.S.; Coit, D.G.; Ariyan, C.E.; Hay, J.L. Factors associated with inconsistent sun protection in first-degree relatives of melanoma survivors. Qual. Health Res. 2012, 22, 934–945. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Diao, D.Y.; Lee, T.K. Sun-protective behaviors in populations at high risk for skin cancer. Psychol. Res. Behav. Manag. 2013, 7, 9–18. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Glenn, B.A.; Lin, T.; Chang, L.C.; Okada, A.; Wong, W.K.; Glanz, K.; Bastani, R. Sun protection practices and sun exposure among children with a parental history of melanoma. Cancer Epidemiol. Biomark. Prev. 2015, 24, 169–177. [Google Scholar] [CrossRef] [Green Version]
- Wu, Y.P.; Parsons, B.G.; Mooney, R.; Aspinwall, L.G.; Cloyes, K.; Hay, J.L.; Kohlmann, W.; Grossman, D.; Leachman, S.A. Barriers and Facilitators to Melanoma Prevention and Control Behaviors Among At-Risk Children. J. Community Health 2018, 43, 993–1001. [Google Scholar] [CrossRef] [PubMed]
- Benjamini, Y.; Hochberg, Y. Controlling the False Discovery Rate—A Practical and Powerful Approach to Multiple Testing. J. R. Stat. Soc. B 1995, 57, 289–300. [Google Scholar] [CrossRef]


{kind=link}
{kind=link}
| MC1R Average-Risk, n (%) | MC1R Higher-Risk, n (%) | |||||
|---|---|---|---|---|---|---|
| Variable | Standard Arm (n = 227) | Precision Prevention Arm (n = 226) | p-Value * | Standard Arm (n = 339) | Precision Prevention Arm (n = 342) | p-Value * |
| Participant Characteristics | ||||||
| Age (mean, SD) | 48.1 (16.0) | 46.6 (16.8) | 0.34 | 48.5 (15.9) | 47.7 (14.9) | 0.55 |
| Female | 112 (49.3) | 116 (51.3) | 0.67 | 175 (51.6) | 168 (49.1) | 0.51 |
| Marital status | 0.79 | 0.06 | ||||
| Single or never married | 59 (26.0) | 60 (26.5) | 67 (19.8) | 79 (23.1) | ||
| Married, domestic partnership, or civil union | 138 (60.8) | 134 (59.3) | 228 (67.3) | 201 (58.8) | ||
| Divorced, separated, or widowed | 27 (11.9) | 32 (14.2) | 42 (12.4) | 59 (17.3) | ||
| Education | 0.80 | 0.13 | ||||
| Graduate degree or higher | 70 (30.8) | 66 (29.2) | 102 (30.1) | 108 (31.6) | ||
| Four-year college degree | 55 (24.2) | 61 (27.0) | 109 (32.2) | 122 (35.7) | ||
| Some college † | 47 (20.6) | 49 (21.6) | 62 (18.3) | 53 (15.5) | ||
| High school or GED | 45 (19.8) | 41 (18.1) | 53 (15.6) | 45 (13.2) | ||
| Less than high school or GED | 7 (3.1) | 9 (4.0) | 11 (3.2) | 10 (2.9) | ||
| Season at baseline | 0.92 | 0.84 | ||||
| Spring | 71 (31.3) | 66 (29.2) | 89 (26.3) | 93 (27.2) | ||
| Summer | 39 (17.2) | 38 (16.8) | 60 (17.7) | 63 (18.4) | ||
| Fall | 61 (26.9) | 60 (26.5) | 106 (31.3) | 96 (28.1) | ||
| Winter | 56 (24.7) | 62 (27.4) | 84 (24.8) | 90 (26.3) | ||
| Health literacy | 0.94 | 0.91 | ||||
| Extremely confident | 151 (66.5) | 153 (67.7) | 233 (68.7) | 230 (67.3) | ||
| Quite a bit confident | 57 (25.1) | 47 (20.8) | 75 (22.1) | 85 (24.9) | ||
| Not at all, a little bit, or somewhat confident | 17 (7.5) | 25 (11.1) | 31 (9.1) | 25 (7.3) | ||
| Health numeracy | 0.004 | 0.26 | ||||
| Very easy | 121 (53.3) | 92 (40.7) | 157 (46.3) | 142 (41.5) | ||
| Easy | 91 (40.1) | 110 (48.7) | 163 (48.1) | 178 (52.0) | ||
| Hard | 12 (5.3) | 22 (9.7) | 18 (5.3) | 18 (5.3) | ||
| Very hard | 1 (0.4) | 1 (0.4) | 0 | 1 (0.3) | ||
| Family history of melanoma | 38 (16.7) | 47 (20.8) | 0.28 | 74 (21.8) | 74 (21.6) | 0.94 |
| Family history of skin cancer | 68 (30.0) | 61 (27.0) | 0.52 | 97 (28.6) | 99 (28.9) | 0.92 |
| Burnability | 0.75 | 0.63 | ||||
| Burner | 49 (21.6) | 46 (20.4) | 112 (33.0) | 119 (34.8) | ||
| Non-burner | 178 (78.4) | 180 (79.7) | 227 (67.0) | 223 (65.2) | ||
| Outcomes | ||||||
| Sun exposure (hours) (mean, SD) | ||||||
| Weekday | 1.4 (1.3) | 1.4 (1.0) | 0.97 | 1.3 (1.1) | 1.4 (1.3) | 0.15 |
| Weekend | 2.3 (1.5) | 2.4 (1.4) | 0.58 | 2.1 (1.4) | 2.4 (1.6) | 0.05 |
| Sunburns (mean, SD) | 0.6 (1.0) | 0.7 (1.0) | 0.43 | 0.7 (1.0) | 0.8 (1.1) | 0.23 |
| Outdoor intentional tanning (mean, SD) | 1.9 (1.0) | 2.0 (0.9) | 0.48 | 2.0 (1.0) | 2.0 (1.0) | 0.58 |
| Indoor tanning | 10 (0.04) | 12 (0.05) | 0.63 | 18 (0.05) | 7 (0.02) | 0.03 |
| Wearing a hat often or always | 62 (27.6) | 56 (25.2) | 0.58 | 92 (27.2) | 95 (28.0) | 0.81 |
| Seeking shade or using umbrella often or always | 86 (38.2) | 71 (31.8) | 0.16 | 103 (30.5) | 106 (31.2) | 0.84 |
| Wearing a shirt with sleeves often or always | 158 (69.9) | 154 (69.1) | 0.84 | 220 (65.1) | 228 (66.9) | 0.63 |
| Wearing sunglasses often or always | 161 (71.6) | 153 (68.6) | 0.50 | 217 (64.4) | 233 (68.5) | 0.25 |
| Wearing sunscreen often or always | 82 (36.3) | 66 (29.6) | 0.13 | 111 (32.8) | 127 (37.2) | 0.23 |
| Standard Arm | Precision Prevention Arm | Intervention Effect * | ||||||
|---|---|---|---|---|---|---|---|---|
| Outcomes | Baseline | Post-Intervention † | p ‡ | Baseline | Post-Intervention † | p ‡ | Beta/Odds Ratio | p |
| MC1R Average-Risk | ||||||||
| n = 227 | n = 226 | |||||||
| Continuous Outcomes § | ||||||||
| Weekday hours | 1.27 | 1.09 | 0.009 | 1.30 | 1.18 | 0.069 | 0.12 | 0.16 |
| Weekend hours | 2.17 | 2.00 | 0.067 | 2.25 | 2.08 | 0.031 | 0.11 | 0.18 |
| Sunburns | 0.60 | 0.29 | <0.0001 | 0.66 | 0.20 | <0.0001 | -0.07 | 0.35 |
| Outdoor intentional tanning | 2.01 | 1.79 | <0.0001 | 2.03 | 1.85 | <0.0001 | 0.06 | 0.48 |
| Binary Outcomes ¶ | ||||||||
| Wearing a hat often or always | 0.20 | 0.24 | 0.09 | 0.17 | 0.29 | <0.0001 | 1.36 | 0.25 |
| Seeking shade or using umbrella often or always | 0.35 | 0.34 | 0.89 | 0.27 | 0.35 | 0.02 | 1.24 | 0.32 |
| Wearing a shirt with sleeves often or always | 0.72 | 0.71 | 0.79 | 0.70 | 0.72 | 0.59 | 1.08 | 0.72 |
| Wearing sunglasses often or always | 0.76 | 0.77 | 0.61 | 0.75 | 0.76 | 0.57 | 0.91 | 0.72 |
| Wearing sunscreen often or always | 0.36 | 0.37 | 0.98 | 0.28 | 0.30 | 0.53 | 0.85 | 0.51 |
| Indoor intentional tanning | 0.05 | 0.01 | -- | 0.06 | 0.03 | -- | -- | -- |
| MC1R Higher-Risk | ||||||||
| n = 339 | n = 342 | |||||||
| Continuous Outcomes § | ||||||||
| Weekday hours | 1.26 | 1.09 | 0.001 | 1.29 | 1.05 | <0.0001 | 0.01 | 0.74 |
| Weekend hours | 2.25 | 1.89 | 0.002 | 2.30 | 1.89 | 0.001 | -0.01 | 0.76 |
| Sunburns | 0.83 | 0.27 | <0.0001 | 0.85 | 0.28 | <0.0001 | 0.03 | 0.97 |
| Outdoor intentional tanning | 1.96 | 1.70 | <0.0001 | 1.95 | 1.71 | <0.0001 | 0.004 | 0.98 |
| Binary Outcomes ¶ | ||||||||
| Wearing a hat often or always | 0.25 | 0.33 | 0.001 | 0.27 | 0.32 | 0.03 | 0.87 | 0.53 |
| Seeking shade or using umbrella often or always | 0.33 | 0.35 | 0.48 | 0.34 | 0.43 | 0.006 | 1.42 | 0.046 |
| Wearing a shirt with sleeves often or always | 0.68 | 0.67 | 0.83 | 0.70 | 0.75 | 0.08 | 1.49 | 0.033 |
| Wearing sunglasses often or always | 0.66 | 0.70 | 0.16 | 0.70 | 0.73 | 0.23 | 1.13 | 0.61 |
| Wearing sunscreen often or always | 0.36 | 0.42 | 0.10 | 0.40 | 0.38 | 0.44 | 0.83 | 0.39 |
| Indoor intentional tanning | 0.06 | 0.03 | -- | 0.02 | 0.01 | -- | -- | -- |
| Skin Exam Type | Standard Arm | Precision Prevention Arm | Intervention Effect * | |||||
|---|---|---|---|---|---|---|---|---|
| n † | Post- Intervention ‡ | n † | Post- Intervention ‡ | Odds Ratio | 95% Confidence Interval | p | ||
| MC1R Average-Risk | ||||||||
| Health professional | 166 | 0.18 | 169 | 0.17 | 0.90 | 0.51 | 1.60 | 0.72 |
| Self/partner | 153 | 0.17 | 148 | 0.19 | 1.17 | 0.64 | 2.11 | 0.61 |
| Either | 151 | 0.33 | 144 | 0.34 | 1.02 | 0.62 | 1.69 | 0.94 |
| MC1R Higher-Risk | ||||||||
| Health professional | 216 | 0.21 | 229 | 0.21 | 0.96 | 0.60 | 1.52 | 0.86 |
| Self/partner | 202 | 0.28 | 211 | 0.23 | 0.76 | 0.49 | 1.20 | 0.24 |
| Either | 199 | 0.37 | 202 | 0.38 | 1.01 | 0.66 | 1.53 | 0.98 |
| Outcome | Moderator | Intervention Effect | Intervention Effect P | Moderation P |
|---|---|---|---|---|
| MC1R Average-Risk | ||||
| Weekend Hours | Marital status | 0.019 | ||
| Single, separated, divorced, or widowed | −0.15 | 0.34 | ||
| Married, domestic partnership, or civil union | 0.32 | 0.01 | ||
| Sunburns | Family history of non-melanoma skin cancer | 0.049 | ||
| No | −0.10 | 0.07 | ||
| Yes | 0.09 | 0.23 | ||
| Wearing a hat often or always | Family history of melanoma | 0.030 | ||
| No | 1.05 * | 0.87 | ||
| Yes | 5.23 * | 0.01 | ||
| Seeking shade or using umbrella often or always | Family history of melanoma | 0.023 | ||
| No | 0.98 * | 0.93 | ||
| Yes | 3.67 * | 0.01 | ||
| MC1R Higher-Risk | ||||
| Sunburns | Tendency to burn | 0.032 | ||
| Burners | −0.14 | 0.09 | ||
| Non-burners | 0.07 | 0.16 | ||
| Standard Arm | Precision Prevention Arm | Intervention Effect * | ||||||
|---|---|---|---|---|---|---|---|---|
| Outcomes | Baseline | Post-Intervention † | p ‡ | Baseline | Post-Intervention † | p ‡ | Beta | p |
| MC1R Average-Risk | ||||||||
| n = 25 | n = 21 | |||||||
| Continuous Outcomes § | ||||||||
| Weekday hours | 1.31 | 1.29 | 0.91 | 1.50 | 1.23 | 0.21 | −0.06 | 0.87 |
| Weekend hours | 2.23 | 2.36 | 0.42 | 2.29 | 2.10 | 0.35 | −0.24 | 0.41 |
| Sunburns | 0.31 | 0.25 | 0.33 | 0.48 | 0.16 | 0.12 | −0.20 | 0.77 |
| Outdoor intentional tanning | 1.09 | 1.06 | 0.77 | 1.13 | 0.99 | 0.27 | 0.09 | 0.42 |
| Binary Outcomes ¶ | ||||||||
| Wearing a hat often or always ** | 0.24 | 0.08 | 0.26 | 0.11 | 0.02 | 0.19 | 0.17 | 0.08 |
| Seeking shade or using umbrella often or always | 0.12 | 0.49 | 0.15 | 0.19 | 0.17 | 0.87 | 0.60 | 0.78 |
| Wearing a shirt with sleeves often or always †† | 0.85 | 0.88 | -- | 0.69 | 1.00 | -- | -- | -- |
| Wearing sunglasses often or always ** | 0.04 | 0.02 | 0.34 | 0.04 | 0.04 | 0.93 | 1.59 | 0.81 |
| Wearing sunscreen often or always | 0.71 | 0.70 | 0.78 | 0.66 | 0.44 | 0.43 | 0.29 | 0.24 |
| MC1R Higher-Risk | ||||||||
| n = 49 | n = 46 | |||||||
| Continuous Outcomes § | ||||||||
| Weekday hours | 1.42 | 1.34 | 0.59 | 1.40 | 1.47 | 0.61 | 0.03 | 0.38 |
| Weekend hours | 2.33 | 2.28 | 0.77 | 2.26 | 2.24 | 0.89 | 0.10 | 0.76 |
| Sunburns | 0.32 | 0.26 | 0.33 | 0.37 | 0.10 | 0.01 | −0.13 | 0.03 |
| Outdoor intentional tanning | 1.16 | 1.03 | 0.02 | 1.10 | 1.06 | 0.20 | 0.01 | 0.78 |
| Binary Outcomes ¶ | ||||||||
| Wearing a hat often or always ** | 0.07 | 0.07 | 0.93 | 0.09 | 0.05 | 0.41 | 0.88 | 0.87 |
| Seeking shade or using umbrella often or always | 0.14 | 0.07 | 0.24 | 0.15 | 0.18 | 0.99 | 2.53 | 0.10 |
| Wearing a shirt with sleeves often or always | 0.91 | 0.84 | 0.41 | 0.84 | 0.96 | 0.05 | 2.45 | 0.13 |
| Wearing sunglasses often or always †† | 0.07 | 0.06 | -- | 0.11 | 0.12 | -- | -- | -- |
| Wearing sunscreen often or always | 0.83 | 0.69 | 0.21 | 0.88 | 0.86 | 0.79 | 2.65 | 0.06 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Lacson, J.C.A.; Doyle, S.H.; Qian, L.; Del Rio, J.; Forgas, S.M.; Valavanis, S.; Carvajal, R.; Gonzalez-Calderon, G.; Kim, Y.; Roetzheim, R.G.; et al. A Randomized Trial of Precision Prevention Materials to Improve Primary and Secondary Melanoma Prevention Activities among Individuals with Limited Melanoma Risk Phenotypes. Cancers 2021, 13, 3143. https://doi.org/10.3390/cancers13133143
Lacson JCA, Doyle SH, Qian L, Del Rio J, Forgas SM, Valavanis S, Carvajal R, Gonzalez-Calderon G, Kim Y, Roetzheim RG, et al. A Randomized Trial of Precision Prevention Materials to Improve Primary and Secondary Melanoma Prevention Activities among Individuals with Limited Melanoma Risk Phenotypes. Cancers. 2021; 13(13):3143. https://doi.org/10.3390/cancers13133143
Chicago/Turabian StyleLacson, John Charles A., Scarlet H. Doyle, Lu Qian, Jocelyn Del Rio, Stephanie M. Forgas, Stella Valavanis, Rodrigo Carvajal, Guillermo Gonzalez-Calderon, Youngchul Kim, Richard G. Roetzheim, and et al. 2021. "A Randomized Trial of Precision Prevention Materials to Improve Primary and Secondary Melanoma Prevention Activities among Individuals with Limited Melanoma Risk Phenotypes" Cancers 13, no. 13: 3143. https://doi.org/10.3390/cancers13133143