
Multi-Institutional Retrospective Analysis of Carbon-Ion Radiotherapy for Patients with Locally Advanced Adenocarcinoma of the Uterine Cervix

 , , , , and
, , , , and
Abstract
:Simple Summary
Abstract
1. Introduction
2. Results
2.1. Patients and Tumor Characteristics
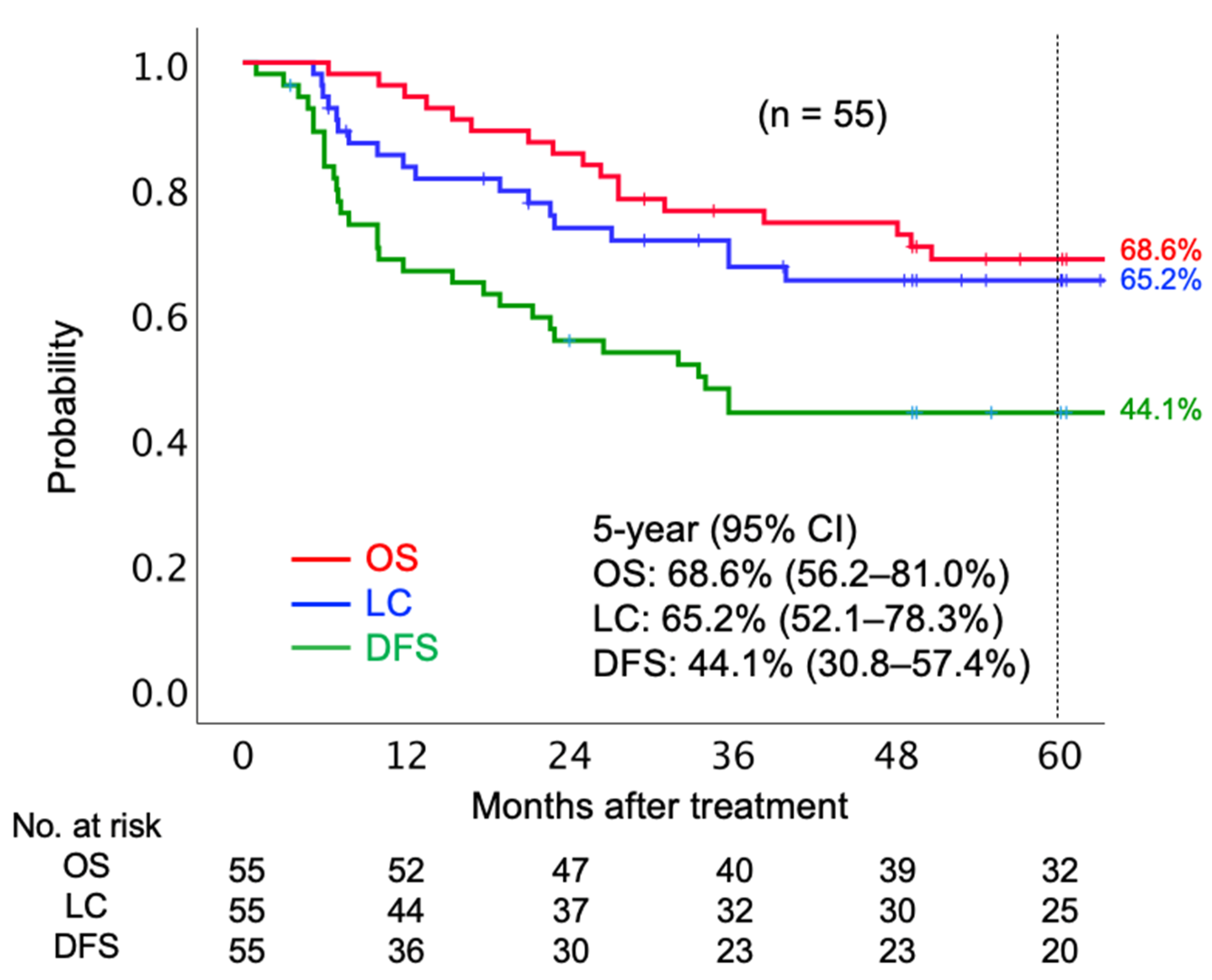
2.2. Treatment Efficacy and Prognostic Factors
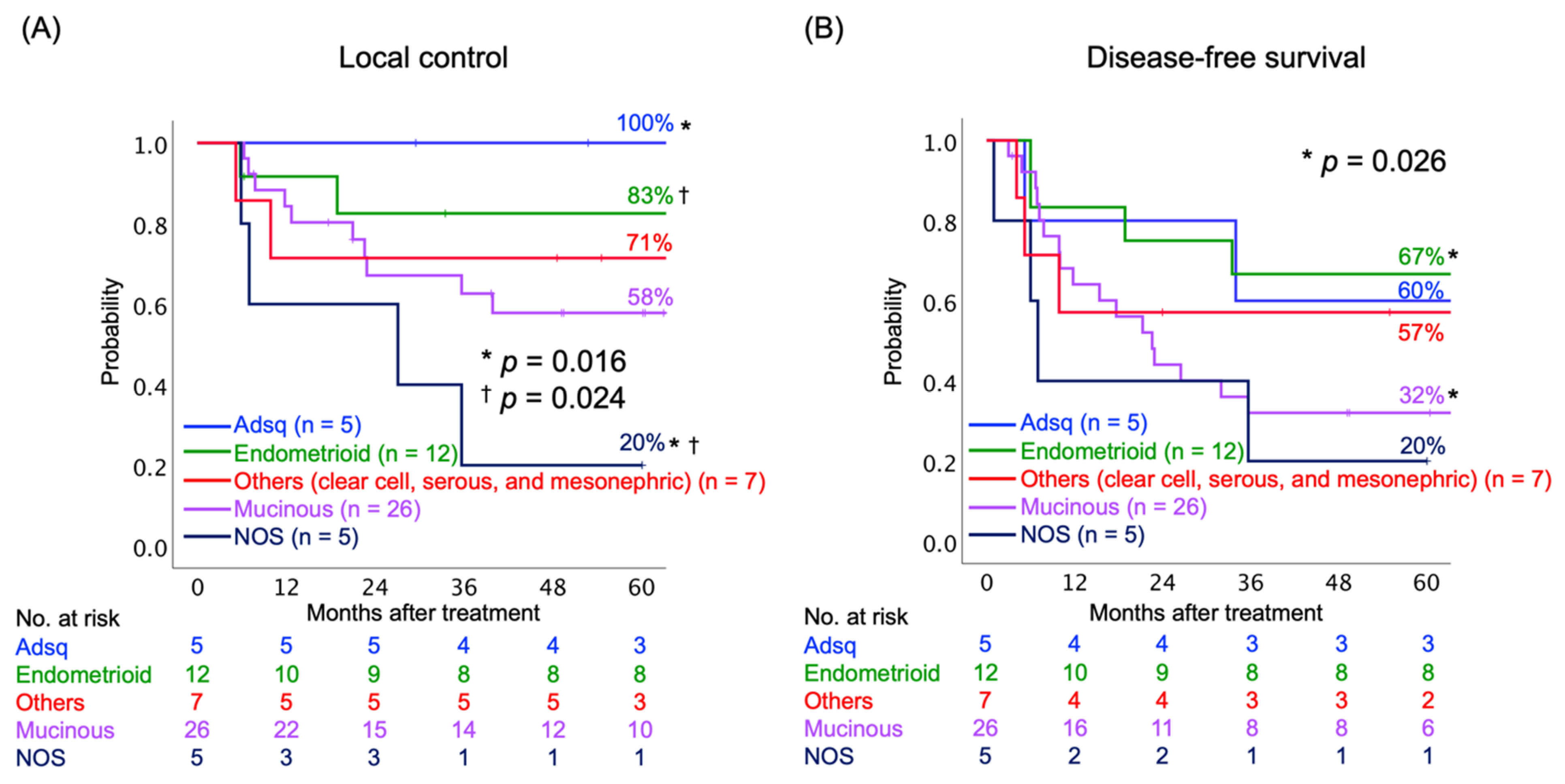
2.3. Relationship between Clinical Outcomes and Histological Subtypes
2.4. Acute and Late Toxicities
3. Discussion
4. Materials and Methods
4.1. Eligibility
4.2. Carbon-Ion Radiotherapy
4.3. Chemotherapy
4.4. Evaluation and Statistical Analyses
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Mathew, A.; George, P.S. Trends in Incidence and Mortality Rates of Squamous Cell Carcinoma and Adenocarcinoma of Cervix--Worldwide. Asian Pac. J. Cancer Prev. 2009, 10, 645–650. [Google Scholar]
- NCCN Guidelines version 1.2021 Cervical Cancer. Available online: https://www.nccn.org/professionals/physician_gls/pdf/cervical_blocks.pdf (accessed on 21 May 2021).
- Wang, S.S.; Sherman, M.E.; Hildesheim, A.; Lacey, J.V., Jr.; Devesa, S. Cervical Adenocarcinoma and Squamous Cell Carcinoma Incidence Trends Among White Women and Black Women in the United States for 1976–2000. Cancer 2004, 100, 1035–1044. [Google Scholar] [CrossRef]
- Bray, F.; Carstensen, B.; Møller, H.; Zappa, M.; Zakelj, M.P.; Lawrence, G.; Hakama, M.; Weiderpass, E. Incidence Trends of Adenocarcinoma of the Cervix in 13 European Countries. Cancer Epidemiol. Biomarkers Prev. 2005, 14, 2191–2199. [Google Scholar] [CrossRef] [Green Version]
- Rose, P.G.; Bundy, B.N.; Watkins, E.B.; Thigpen, J.T.; Deppe, G.; Maiman, M.A.; Clarke-Pearson, D.L.; Insalaco, S. Concurrent Cisplatin-Based Radiotherapy and Chemotherapy for Locally Advanced Cervical Cancer. N. Engl. J. Med. 1999, 340, 1144–1153. [Google Scholar] [CrossRef] [PubMed]
- Green, J.A.; Kirwan, J.M.; Tierney, J.F.; Symonds, P.; Fresco, L.; Collingwood, M.; Williams, C.J. Survival and Recurrence After Concomitant Chemotherapy and Radiotherapy for Cancer of the Uterine Cervix: A Systematic Review and Meta-Analysis. Lancet 2001, 358, 781–786. [Google Scholar] [CrossRef]
- Eifel, P.J.; Winter, K.; Morris, M.; Levenback, C.; Grigsby, P.W.; Cooper, J.; Rotman, M.; Gershenson, D.; Mutch, D.G. Pelvic Irradiation with Concurrent Chemotherapy Versus Pelvic and Para-Aortic Irradiation for High-Risk Cervical Cancer: An Update of Radiation Therapy Oncology Group Trial (RTOG) 90-01. J. Clin. Oncol. 2004, 22, 872–880. [Google Scholar] [CrossRef]
- Vale, C.; Tierney, J.; Stewart, L. Concomitant Chemoradiotherapy for Cervical Cancer: A Systematic Review and Meta-Analysis of Individual Patient Data. Gynecol. Oncol. 2006, 100, 442–443. [Google Scholar] [CrossRef] [PubMed]
- Chemoradiotherapy for Cervical Cancer Meta-Analysis Collaboration. Reducing Uncertainties About the Effects of Chemoradiotherapy for Cervical Cancer: A Systematic Review and Meta-Analysis of Individual Patient Data From 18 Randomized Trials. J. Clin. Oncol. 2008, 26, 5802–5812. [Google Scholar] [CrossRef] [Green Version]
- Eifel, P.J.; Morris, M.; Oswald, M.J.; Wharton, J.T.; Delclos, L. Adenocarcinoma of the Uterine Cervix. Prognosis and Patterns of Failure in 367 Cases. Cancer 1990, 65, 2507–2514. [Google Scholar] [CrossRef]
- Farley, J.H.; Hickey, K.W.; Carlson, J.W.; Rose, G.S.; Kost, E.R.; Harrison, T.A. Adenosquamous Histology Predicts a Poor Outcome for Patients with Advanced-Stage, but Not Early-Stage, Cervical Carcinoma. Cancer 2003, 97, 2196–2202. [Google Scholar] [CrossRef] [PubMed]
- Niibe, Y.; Kenjo, M.; Onishi, H.; Ogawa, Y.; Kazumoto, T.; Ogino, I.; Tsujino, K.; Harima, Y.; Takahashi, T.; Anbai, A.; et al. High-Dose-Rate Intracavitary Brachytherapy Combined with External Beam Radiotherapy for stage IIIb Adenocarcinoma of the Uterine Cervix in Japan: A Multi-Institutional Study of Japanese Society of Therapeutic Radiology and Oncology 2006–2007 (Study of JASTRO 2006–2007). Jpn. J. Clin. Oncol. 2010, 40, 795–799. [Google Scholar] [PubMed]
- Huang, Y.T.; Wang, C.C.; Tsai, C.S.; Lai, C.H.; Chang, T.C.; Chou, H.H.; Hsueh, S.; Chen, C.K.; Lee, S.P.; Hong, J.H. Long-Term Outcome and Prognostic Factors for Adenocarcinoma/Adenosquamous Carcinoma of Cervix After Definitive Radiotherapy. Int. J. Radiat. Oncol. Biol. Phys. 2011, 80, 429–436. [Google Scholar] [CrossRef]
- Pötter, R.; Haie-Meder, C.; Van Limbergen, E.; Barillot, I.; De Brabandere, M.; Dimopoulos, J.; Dumas, I.; Erickson, B.; Lang, S.; Nulens, A.; et al. Recommendations from Gynaecological (GYN) GEC ESTRO Working Group (II): Concepts and Terms in 3D Image-Based Treatment Planning in Cervix Cancer brachytherapy-3D Dose Volume Parameters and Aspects of 3D Image-Based Anatomy, Radiation Physics, Radiobiology. Radiother. Oncol. 2006, 78, 67–77. [Google Scholar] [CrossRef]
- Pötter, R.; Georg, P.; Dimopoulos, J.C.; Grimm, M.; Berger, D.; Nesvacil, N.; Georg, D.; Schmid, M.P.; Reinthaller, A.; Sturdza, A.; et al. Clinical Outcome of Protocol Based Image (MRI) Guided Adaptive Brachytherapy Combined With 3D Conformal Radiotherapy with or Without Chemotherapy in Patients with Locally Advanced Cervical Cancer. Radiother. Oncol. 2011, 100, 116–123. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sturdza, A.; Pötter, R.; Fokdal, L.U.; Haie-Meder, C.; Tan, L.T.; Mazeron, R.; Petric, P.; Šegedin, B.; Jurgenliemk-Schulz, I.M.; Nomden, C.; et al. Image Guided Brachytherapy in Locally Advanced Cervical Cancer: Improved Pelvic Control and Survival in RetroEMBRACE, a Multicenter Cohort Study. Radiother. Oncol. 2016, 120, 428–433. [Google Scholar] [CrossRef] [PubMed]
- Minkoff, D.; Gill, B.S.; Kang, J.; Beriwal, S. Cervical Cancer Outcome Prediction to High-Dose Rate Brachytherapy Using Quantitative Magnetic Resonance Imaging Analysis of Tumor Response to External Beam Radiotherapy. Radiother. Oncol. 2015, 115, 78–83. [Google Scholar] [CrossRef]
- Kusada, T.; Toita, T.; Ariga, T.; Maemoto, H.; Hashimoto, S.; Shiina, H.; Kakinohana, Y.; Heianna, J.; Nagai, Y.; Kudaka, W.; et al. Computed Tomography-Based Image-Guided Brachytherapy for Cervical Cancer: Correlations Between Dose-Volume Parameters and Clinical Outcomes. J. Radiat. Res. 2018, 59, 67–76. [Google Scholar] [CrossRef] [Green Version]
- Kanai, T.; Furusawa, Y.; Fukutsu, K.; Itsukaichi, H.; Eguchi-Kasai, K.; Ohara, H. Irradiation of Mixed Beam and Design of Spread-Out Bragg Peak for Heavy-Ion Radiotherapy. Radiat. Res. 1997, 147, 78–85. [Google Scholar] [CrossRef]
- Kanai, T.; Endo, M.; Minohara, S.; Miyahara, N.; Koyama-ito, H.; Tomura, H.; Matsufuji, N.; Futami, Y.; Fukumura, A.; Hiraoka, T.; et al. Biophysical Characteristics of HIMAC Clinical Irradiation System for Heavy-Ion Radiation Therapy. Int. J. Radiat. Oncol. Biol. Phys. 1999, 44, 201–210. [Google Scholar] [CrossRef]
- Kamada, T.; Tsujii, H.; Blakely, E.A.; Debus, J.; De Neve, W.; Durante, M.; Jäkel, O.; Mayer, R.; Orecchia, R.; Pötter, R.; et al. Carbon Ion Radiotherapy in Japan: An Assessment of 20 Years of Clinical Experience. Lancet Oncol. 2015, 16, e93–e100. [Google Scholar] [CrossRef] [Green Version]
- Wakatsuki, M.; Kato, S.; Ohno, T.; Karasawa, K.; Kiyohara, H.; Tamaki, T.; Ando, K.; Tsujii, H.; Nakano, T.; Kamada, T.; et al. Clinical Outcomes of Carbon Ion Radiotherapy for Locally Advanced Adenocarcinoma of the Uterine Cervix in phase 1/2 Clinical Trial (Protocol 9704). Cancer 2014, 120, 1663–1669. [Google Scholar] [CrossRef]
- Ohno, T.; Noda, S.E.; Murata, K.; Yoshimoto, Y.; Okonogi, N.; Ando, K.; Tamaki, T.; Kato, S.; Hirakawa, T.; Kanuma, T.; et al. Phase I Study of Carbon Ion Radiotherapy and Image-Guided Brachytherapy for Locally Advanced Cervical Cancer. Cancers 2018, 10, 338. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Okonogi, N.; Wakatsuki, M.; Kato, S.; Karasawa, K.; Kiyohara, H.; Shiba, S.; Kobayashi, D.; Nakano, T.; Kamada, T.; Shozu, M.; et al. Clinical Outcomes of Carbon Ion Radiotherapy with Concurrent Chemotherapy for Locally Advanced Uterine Cervical Adenocarcinoma in a phase 1/2 Clinical Trial (Protocol 1001). Cancer Med. 2018, 7, 351–359. [Google Scholar] [CrossRef] [Green Version]
- Okonogi, N.; Wakatsuki, M.; Kato, S.; Karasawa, K.; Miyasaka, Y.; Murata, H.; Nakano, T.; Kamada, T.; Shozu, M.; Working Group of Gynecological Tumors. A Phase 1/2 Study of Carbon Ion Radiation Therapy with Concurrent Chemotherapy for Locally Advanced Uterine Cervical Squamous Cell Carcinoma (Protocol 1302). Int. J. Radiat. Oncol. Biol. Phys. 2019, 104, 631–639. [Google Scholar] [CrossRef]
- Wang, L.; Wang, X.; Zhang, Q.; Ran, J.; Geng, Y.; Feng, S.; Li, C.; Zhao, X. Is There a Role for Carbon Therapy in the Treatment of Gynecological Carcinomas? A Systematic Review. Future Oncol. 2019, 15, 3081–3095. [Google Scholar] [CrossRef]
- Yokoi, E.; Mabuchi, S.; Takahashi, R.; Matsumoto, Y.; Kuroda, H.; Kozasa, K.; Kimura, T. Impact of Histological Subtype on Survival in Patients with Locally Advanced Cervical Cancer That Were Treated With Definitive Radiotherapy: Adenocarcinoma/Adenosquamous Carcinoma Versus Squamous Cell Carcinoma. J. Gynecol. Oncol. 2017, 28, e19. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Miyasaka, Y.; Yoshimoto, Y.; Murata, K.; Noda, S.E.; Ando, K.; Ebara, T.; Okonogi, N.; Kaminuma, T.; Yamada, S.; Ikota, H.; et al. Treatment Outcomes of Patients with Adenocarcinoma of the Uterine Cervix After Definitive Radiotherapy and the Prognostic Impact of Tumor-Infiltrating CD8+ Lymphocytes in Pre-Treatment Biopsy Specimens: A Multi-Institutional Retrospective Study. J. Radiat. Res. 2020, 61, 275–284. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zhang, J.; Qin, L.; Chen, H.M.; Hsu, H.C.; Chuang, C.C.; Chen, D.; Wu, S.Y. Overall Survival, Locoregional Recurrence, and Distant Metastasis of Definitive Concurrent Chemoradiotherapy for Cervical Squamous Cell Carcinoma and Adenocarcinoma: Before and After Propensity Score Matching Analysis of a Cohort Study. Am. J. Cancer Res. 2020, 10, 1808–1820. [Google Scholar]
- Zhou, J.; Wu, S.G.; Sun, J.Y.; Li, F.Y.; Lin, H.X.; Chen, Q.H.; He, Z.Y. Comparison of Clinical Outcomes of Squamous Cell Carcinoma, Adenocarcinoma, and Adenosquamous Carcinoma of the Uterine Cervix After Definitive Radiotherapy: A Population-Based Analysis. J. Cancer Res. Clin. Oncol. 2017, 143, 115–122. [Google Scholar] [CrossRef]
- Wright, A.A.; Howitt, B.E.; Myers, A.P.; Dahlberg, S.E.; Palescandolo, E.; Van Hummelen, P.; MacConaill, L.E.; Shoni, M.; Wagle, N.; Jones, R.T.; et al. Oncogenic Mutations in Cervical Cancer: Genomic Differences Between Adenocarcinomas and Squamous Cell Carcinomas of the Cervix. Cancer 2013, 119, 3776–3783. [Google Scholar] [CrossRef]
- Ojesina, A.I.; Lichtenstein, L.; Freeman, S.S.; Pedamallu, C.S.; Imaz-Rosshandler, I.; Pugh, T.J.; Cherniack, A.D.; Ambrogio, L.; Cibulskis, K.; Bertelsen, B.; et al. Landscape of Genomic Alterations in Cervical Carcinomas. Nature 2014, 506, 371–375. [Google Scholar] [CrossRef]
- Kirwan, J.M.; Symonds, P.; Green, J.A.; Tierney, J.; Collingwood, M.; Williams, C.J. A Systematic Review of Acute and Late Toxicity of Concomitant Chemoradiation for Cervical Cancer. Radiother. Oncol. 2003, 68, 217–226. [Google Scholar] [CrossRef]
- Inaniwa, T.; Kanematsu, N.; Matsufuji, N.; Kanai, T.; Shirai, T.; Noda, K.; Tsuji, H.; Kamada, T.; Tsujii, H. Reformulation of a Clinical-Dose System for Carbon-Ion Radiotherapy Treatment Planning at the National Institute of Radiological Sciences, Japan. Phys. Med. Biol. 2015, 60, 3271–3286. [Google Scholar] [CrossRef] [Green Version]
- Authorized Treatment Policy of Carbon-Ion Radiotherapy for Locally Advanced Cervical Cancer, Japanese Society for Radiation Oncology (Written in Japanese). Available online: https://www.jastro.or.jp/medicalpersonnel/particle_beam/pdf/2018/S-J-5-1.pdf (accessed on 21 May 2021).
- Kubota, Y.; Ohno, T.; Kawashima, M.; Murata, K.; Okonogi, N.; Noda, S.E.; Tsuda, K.; Sakai, M.; Tashiro, M.; Nakano, T. Development of a Vaginal Immobilization Device: A Treatment-Planning Study of Carbon-Ion Radiotherapy and Intensity-Modulated Radiation Therapy for Uterine Cervical Cancer. Anticancer Res. 2019, 39, 1915–1921. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Histopathology of the Uterine Cervix, WHO 2014. Available online: https://screening.iarc.fr/atlasclassifwho.php (accessed on 1 May 2021).
- Cox, J.D.; Stetz, J.; Pajak, T.F. Toxicity Criteria of the Radiation Therapy Oncology Group (RTOG) and the European Organization for Research and Treatment of Cancer (EORTC). Int. J. Radiat. Oncol. Biol. Phys. 1995, 31, 1341–1346. [Google Scholar] [CrossRef]
- Eisenhauer, E.A.; Therasse, P.; Bogaerts, J.; Schwartz, L.H.; Sargent, D.; Ford, R.; Dancey, J.; Arbuck, S.; Gwyther, S.; Mooney, M.; et al. New Response Evaluation Criteria in Solid Tumours: Revised RECIST Guideline (Version 1.1). Eur. J. Cancer 2009, 45, 228–247. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| Characteristics | n = 55 |
|---|---|
| Age (median), years | 26–81 (55) |
| Follow-up period (median), months | 6.3–109.6 (67.5) |
| FIGO stage (2008) | |
| IIB | 37 |
| IIIB | 15 |
| IVA | 3 |
| Histological subtypes | |
| Endocervical adenocarcinoma, usual type | 14 |
| Mucinous adenocarcinoma | 10 |
| Mucinous carcinoma, gastric type | 1 |
| Mucinous carcinoma, signet-ring cell type | 1 |
| Endometrioid adenocarcinoma | 12 |
| Clear cell adenocarcinoma | 3 |
| Serous adenocarcinoma | 3 |
| Mesonephric adenocarcinoma | 1 |
| Adenocarcinoma, NOS | 5 |
| Adenosquamous carcinoma | 5 |
| Pelvic LN metastasis | |
| No | 33 |
| Yes | 22 |
| Tumor size (median), cm | 2.8–12.0 (5.3) |
| Weekly CDDP administrations | |
| No | 19 |
| Yes | 36 |
| 1 course | 1 |
| 2 courses | 0 |
| 3 courses | 3 |
| 4 courses | 6 |
| 5 courses | 26 |
| (A) | |||||||
| Factor | No. of Patients | LC | DFS | OS | |||
| 5-Year (%) | p Value | 5-Year (%) | p Value | 5-Year (%) | p Value | ||
| FIGO stage (2008) | 0.243 | 0.684 | 0.019 | ||||
| IIB | 37 | 71.8 | 48.6 | 75.4 | |||
| IIIB-IVA | 18 | 50.8 | 33.2 | 54.3 | |||
| Pelvic LN metastasis | 0.221 | 0.274 | 0.572 | ||||
| No | 33 | 60.5 | 48.9 | 72.2 | |||
| Yes | 22 | 73.5 | 40.5 | 63.3 | |||
| Tumor size | 0.896 | 0.392 | 0.741 | ||||
| ≤5.3 cm | 27 | 68.9 | 38.3 | 67.6 | |||
| >5.3 cm | 28 | 61.6 | 50.2 | 70.2 | |||
| Concurrent CDDP | 0.827 | 0.805 | 0.102 | ||||
| No | 19 | 65.4 | 46.3 | 57.4 | |||
| Yes | 36 | 65.4 | 42.9 | 71.2 | |||
| Initial tumor response | <0.001 | 0.001 | <0.001 | ||||
| CR | 41 | 76.8 | 53.2 | 82.6 | |||
| Non-CR | 15 | 28.9 | 15.5 | 28.6 | |||
| (B) | |||||||
| Factor | LC | DFS | OS | ||||
| p Value | HR (95% CI) | p Value | HR (95% CI) | p Value | HR (95% CI) | ||
| FIGO stage (2008) | 0.672 | - | 0.767 | - | 0.075 | - | |
| Pelvic LN metastasis | 0.286 | - | 0.664 | - | 0.611 | - | |
| Tumor size (≤5.3 cm) | 0.972 | - | 0.261 | - | 0.336 | - | |
| Concurrent CDDP | 0.838 | - | 0.826 | - | 0.181 | - | |
| Initial tumor response | 0.003 | 0.227 (0.086–0.598) | 0.002 | 0.264 (0.115–0.610) | 0.002 | 0.253 (0.104–0.615) | |
| (A) | |||||||
| Treatment Regimen | Number of Patients | Neutrophil Decrease Grade | Hemoglobin Decrease Grade | Platelet Decrease Grade | |||
| 0–2 | 3–4 | 0–2 | 3–4 | 0–2 | 3–4 | ||
| CIRT alone | 19 | 18 | 1 | 18 | 1 | 19 | 0 |
| Chemo-CIRT | 36 | 34 | 2 | 36 | 0 | 36 | 0 |
| p-value | 0.929 | 0.168 | N/A | ||||
| (B) | |||||||
| Treatment Regimen | Number of Patients | Nausea/Vomiting Grade | Lower Gastrointestinal Grade | Genitourinary Grade | |||
| 0–2 | 3–4 | 0–2 | 3–4 | 0–2 | 3–4 | ||
| CIRT alone | 19 | 19 | 0 | 19 | 0 | 19 | 0 |
| Chemo-CIRT | 36 | 35 | 1 | 36 | 0 | 36 | 0 |
| p-value | 0.463 | N/A | N/A | ||||
| (C) | |||||||
| Treatment Regimen | Number of Patients | Rectum/Sigmoid Grade | Small Intestine Grade | Genitourinary Grade | |||
| 0–2 | 3–4 | 0–2 | 3–4 | 0–2 | 3–4 | ||
| CIRT alone | 19 | 18 | 1 | 19 | 0 | 19 | 0 |
| Chemo-CIRT | 36 | 32 | 4 * | 36 | 0 | 33 | 3 † |
| p-value | 0.473 | N/A | 0.195 | ||||
| Author (Year), References | Stage | Number | Treatment | 5y LC | 5y OS |
|---|---|---|---|---|---|
| (%) | (%) | ||||
| Eifel PJ (1990) [10] | III–IV | 48 | RT | 52% | 31% |
| Farley JH (2003) [11] | III | 13 | RT/CCRT | N/R | 32% |
| Niibe Y (2010) [12] | IIIB | 61 | RT/CCRT | 36% | 20% |
| Huang YT (2011) [13] | III | 38 | RT/CCRT | 58% | N/R |
| IVA | 3 | 0% | |||
| Yokoi E (2017) [27] | IIB–IVA | 24 | CCRT (IGBT) | N/R | 27% |
| Miyasaka Y (2020) [28] | III–IVA | 35 | RT/CCRT (IGBT) | 62% (IB–IVA) | 26% |
| Zhang J (2020) [29] | II | 149 | CCRT | N/R | 33% |
| III | 65 | 33% | |||
| IVA | 49 | 9% | |||
| Present study (2021) | IIB–IVA (Good responders *) | 55 | CIRT/ chemo-CIRT | 65% | 69% |
| 41 | (77%) | (83%) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Okonogi, N.; Ando, K.; Murata, K.; Wakatsuki, M.; Noda, S.-e.; Irie, D.; Tsuji, H.; Shozu, M.; Ohno, T. Multi-Institutional Retrospective Analysis of Carbon-Ion Radiotherapy for Patients with Locally Advanced Adenocarcinoma of the Uterine Cervix. Cancers 2021, 13, 2713. https://doi.org/10.3390/cancers13112713
Okonogi N, Ando K, Murata K, Wakatsuki M, Noda S-e, Irie D, Tsuji H, Shozu M, Ohno T. Multi-Institutional Retrospective Analysis of Carbon-Ion Radiotherapy for Patients with Locally Advanced Adenocarcinoma of the Uterine Cervix. Cancers. 2021; 13(11):2713. https://doi.org/10.3390/cancers13112713
Chicago/Turabian StyleOkonogi, Noriyuki, Ken Ando, Kazutoshi Murata, Masaru Wakatsuki, Shin-ei Noda, Daisuke Irie, Hiroshi Tsuji, Makio Shozu, and Tatsuya Ohno. 2021. "Multi-Institutional Retrospective Analysis of Carbon-Ion Radiotherapy for Patients with Locally Advanced Adenocarcinoma of the Uterine Cervix" Cancers 13, no. 11: 2713. https://doi.org/10.3390/cancers13112713