
SARS-CoV-2-Induced Gut Microbiome Dysbiosis: Implications for Colorectal Cancer
by

Mark C. Howell
1,2, 
Ryan Green
1,2,
Andrew R. McGill
1,2,
Rinku Dutta
3,
Subhra Mohapatra
1,3,* and 
Shyam S. Mohapatra
1,2,*
1
Department of Veterans Affairs, James A. Haley Veterans Hospital, Tampa, FL 33612, USA
2
Department of Internal Medicine, Morsani College of Medicine, University of South Florida, Tampa, FL 33612, USA
3
Department of Molecular Medicine, Morsani College of Medicine, University of South Florida, Tampa, FL 33612, USA
*
Authors to whom correspondence should be addressed.
Cancers 2021, 13(11), 2676; https://doi.org/10.3390/cancers13112676
Submission received: 5 April 2021
/
Revised: 22 May 2021
/
Accepted: 24 May 2021
/
Published: 28 May 2021
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Abstract
:Simple Summary
Specific guidance regarding cancer treatment in coronavirus disease-19 (COVID-19) patients is lacking due to minimal knowledge. It has been observed that patients with severe COVID-19 develop a dysbiotic microbiota of the gut. This impact may be long-lasting, resulting in a greater possibility of a future diagnosis of colorectal cancer (CRC) or aggravating the condition in those already afflicted. Given that CRC is the third most common and third deadliest type of cancer, we must understand how infection with SARS-CoV-2 will impact CRC biology and treatment strategies.
Abstract
The emergence of a novel coronavirus, severe acute respiratory syndrome coronavirus-2 (SARS-CoV-2), in December 2019 led to a worldwide pandemic with over 170 million confirmed infections and over 3.5 million deaths (as of May 2021). Early studies have shown higher mortality rates from SARS-CoV-2 infection in cancer patients than individuals without cancer. Herein, we review the evidence that the gut microbiota plays a crucial role in health and has been linked to the development of colorectal cancer (CRC). Investigations have shown that SARS-CoV-2 infection causes changes to the gut microbiota, including an overall decline in microbial diversity, enrichment of opportunistic pathogens such as Fusobacterium nucleatum bacteremia, and depletion of beneficial commensals, such as the butyrate-producing bacteria. Further, these changes lead to increased colonic inflammation, which leads to gut barrier disruption, expression of genes governing CRC tumorigenesis, and tumor immunosuppression, thus further exacerbating CRC progression. Additionally, a long-lasting impact of SARS-CoV-2 on gut dysbiosis might result in a greater possibility of new CRC diagnosis or aggravating the condition in those already afflicted. Herein, we review the evidence relating to the current understanding of how infection with SARS-CoV-2 impacts the gut microbiota and the effects this will have on CRC carcinogenesis and progression.
1. Introduction
A novel coronavirus, severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2), emerged late in 2019 in Wuhan, China, which led to a global pandemic resulting in over 170 million confirmed cases and over 3.5 million deaths attributed to this virus as of May 2021 [1]. SARS-CoV-2 is a positive-sense single-stranded RNA virus thought to be transmissible mainly by respiratory aerosol droplets and direct contact, which causes coronavirus disease 2019 (COVID-19) in humans [2]. The SARS-CoV-2 spike glycoprotein (S) protein S1 domain recognizes and binds the angiotensin-converting enzyme-2 (ACE2) receptor expressed on target cells, which facilitates attachment of the virus to the host cell [3]. Host protease TMPRSS2 subsequently cleaves S, revealing the S2 fusion domain, thus facilitating infection of the host cell [4]. It has been demonstrated that the ACE2 receptor and TMPRSS2 protease are required for viral binding to the cell and subsequent entry. However, other tissues have been shown to express differential receptors and proteases that can also interact with the spike protein, which could help explain the multi-tissue affinity of SARS-CoV-2 [5,6,7]. Upon infection, disease pathology involves multiple organs, including lung, gut, and brain. The symptoms range from mildly symptomatic with fatigue, headache, diarrhea, cough, and shortness of breath to acute respiratory distress syndrome and cytokine storm with multi-organ failure requiring mechanical ventilation. Immune dysregulation is a hallmark of COVID-19, paired with increased IL-6 and IL-13, which are potently prognostic [8]. The severity of the illness varies with co-existing comorbidities, biological sex, and age [9]. The potent inflammatory effects from this virus due to their immune system subverting non-structural proteins result in systemic pathologies in the severely ill. SARS-CoV-2 infections have unknown long-term consequences in patients with comorbidities, such as cancer [10].
Cancer patients are traditionally considered at high risk for respiratory viral infections due to their underlying immunosuppression [11]. Respiratory infections have a particularly lethal burden in cancer patients, given their reduced competency to fight infections due to altered immune responsiveness [11]. Infection with a respiratory syncytial virus (RSV), along with other family members of Coronaviridae, has been shown to inhibit and degrade p53, a tumor suppressor that can inhibit carcinogenesis [12,13]. This leads to the question, are cancer patients more likely to develop lethal complications after being infected by SARS-CoV-2? Early studies investigating the relationship between SARS-CoV-2 and cancer have shown higher mortality rates from SARS-CoV-2 infection in cancer patients than individuals without cancer [14]. While a massive effort to collect data on COVID-19 and cancer has been performed over the last year, the reported findings should be interpreted with caution. Specifically, patients with ongoing or recent treatment for hematologic, lung, or metastatic cancers are at higher risk of developing severe COVID-19 [14,15]. It is unclear how much of the increase in mortality rates is due to delayed diagnosis and suboptimal cancer management due to the pandemic [15].
SARS-CoV-2-caused immune dysregulation itself could provide even more significant complications for this already vulnerable subpopulation. Mechanistically, the interaction between the host immune environment and cancer or SARS-CoV-2 infections uses similar pathways, such as hypercoagulability, dysregulated immune response, elevated cytokine levels, altered expression ACE-2 and TMPRSS2, and prothrombotic status, which bring the human body into severe disequilibrium and may aggravate the effects of SARS-CoV-2 in some cancer patients [15]. Specific guidance regarding cancer treatment in COVID-19 patients is lacking due to minimal knowledge, particularly regarding differential immune responses.
SARS-CoV-2 infection begins with attachment to the host ACE2 receptor, with the primary site of infection being in the upper airway and lungs. However, the highest expression of ACE2 in the human body occurs in the intestinal enterocytes’ brush border [16]. A pan-cancer analysis found that ACE2 and TMPRSS2 are generally expressed less in tumors relative to normal tissue and that digestive organs (both tumor and normal samples) have the highest expression [17,18]. It has also been shown that colon epithelial cells express high levels of ACE2 and can support viral replication of SARS-CoV-2, resulting in gut barrier dysfunction [19]. Furthermore, the accessory host proteases required for spike processing and S2 domain exposure are present, including TMPRSS2 and TMPRSS4 [5]. The resulting local inflammation in the gut epithelia in conjunction with the systemic inflammation from the respiratory infection from SARS-CoV-2 can significantly impact the resident gut microbiota.
Influenza infection has been previously shown to significantly alter the composition of the intestinal microbiota [20]. Interferons produced in the lungs lead to the depletion of obligate anaerobic bacteria and proteobacteria enrichment in the gut, leading to dysbiosis. The action of these interferons was shown to inhibit the antimicrobial and inflammatory responses in the gut during Salmonella-induced colitis, which was shown to further enhance Salmonella intestinal colonization and dissemination, a risk factor for colon cancer [21]. Furthermore, patients with irritable bowel syndrome (IBD) had an increased risk for influenza, and IBD inflammation impacted the resolution of flu-like symptoms [22]. This is significant given that IBD is a prominent risk factor for CRC, and it is also known that the gut microbiota within this population is typically highly dysbiotic. It is known that dysbiosis of the gut can influence carcinogenesis and the progression of CRC [23,24]. A dysbiotic gut microbiota is incapable of properly signaling to distal tissues though bacterial metabolic by-products. This is further augmented alongside viral infections, which increase systemic inflammation, resulting in further dysbiosis to the symbiotic microbiome within the host [25]. In contrast to the dysbiosis leading to CRC, individuals with metastatic cancer were reported to regress, in response to viral infection, known as oncolytic therapy [26]. Additionally, another study reported transient remission of refractory NK/T-cell lymphoma during COVID-19 infection and the relapse after COVID-19 resolution in a single patient [27]. These reports together suggest SARS-CoV-2 immune responses have been shown to suppress NK cells cytotoxicity [28]. It has also been hypothesized that the antiviral CD8+ T cell immunity induced by SARS-CoV-2 infections could be used to enhance cancer immunotherapies [29]. While these studies provide the foundational premise for the impact of SARS-CoV-2, further understanding of how respiratory viral infections, particularly SARS-CoV-2, affect CRC progression represents a knowledge gap and critical unmet need.
Currently, little is known about the effect SARS-CoV-2 will have on the host microbiome, let alone on niche environments, such as the gut microbiota and its relation to CRC. According to the American Cancer Society, CRC is estimated to have caused over 140,000 new cases and 50,000 deaths in the United States in 2020 alone. A detailed understanding of how SARS-CoV-2 infection impacts the gut microbiota and CRC progression is of utmost importance [30].
2. The Gut Microbiome and CRC
CRC death remains one of the leading cancer-related mortalities in the United States, but the molecular mechanism of its development is not fully understood. Studies have found that in the United States, CRC incidence rates have increased by 2% annually among adults younger than age 55 from 2007 to 2016 [30] that has led to the recommendation to lower the age for starting colonoscopic screening for CRC. In the past decade, the Human Microbiome Project’s initiative by the National Institutes of Health has highlighted the importance of the gut microbiota to human health. The gut microbiota plays a crucial role in health through its protective, trophic, and metabolic activities. The gut microbiota has been recently linked to CRC development, as microbiota-derived metabolites have been shown to influence carcinogenesis directly [31].
The anaerobic microbes ferment undigested dietary components that reach the large intestine to produce a wide range of metabolites, with the significant fermentation products in healthy adults being gases and organic acids: short-chain fatty acids (SCFAs), such as acetic acid, propionic acid, and butyric acid and medium-chain fatty acids (MCFAs), such as linoleic acid, lauric acid, and oleic acid [32]. They are then released into the colonic lumen and function as signaling molecules between the bacteria and the host [31]. SCFAs have also been shown to maintain the gut barrier and produce an anti-inflammatory effect by introducing Treg cell differentiation and the expression of anti-inflammatory cytokines [33]. Importantly, these activities in the gut form a multi-organ axes, such as the “gut–lung axis” and the “gut–brain axis”, which are dependent on the metabolic products of the gut in maintaining the healthy homeostatic status of these organ systems [34,35].
Gut dysbiosis allows bacterial metabolomes and products to enter the circulatory system, leading to systemic inflammation [36]. The fecal analysis identifies marked dysbiosis in CRC patients from healthy cohorts [23]. Dysbiosis of the gut microbiota can influence immune status, carcinogenesis, and tumor progression in CRC [37,38]. CRC studies have demonstrated continual alterations in the gut microbiota during tumor development, and these alterations are directly responsible for tumor progression [39]. In one study, the colonization of germ-free mice with microbiota from tumor-bearing mice significantly increased tumorigenesis [40].
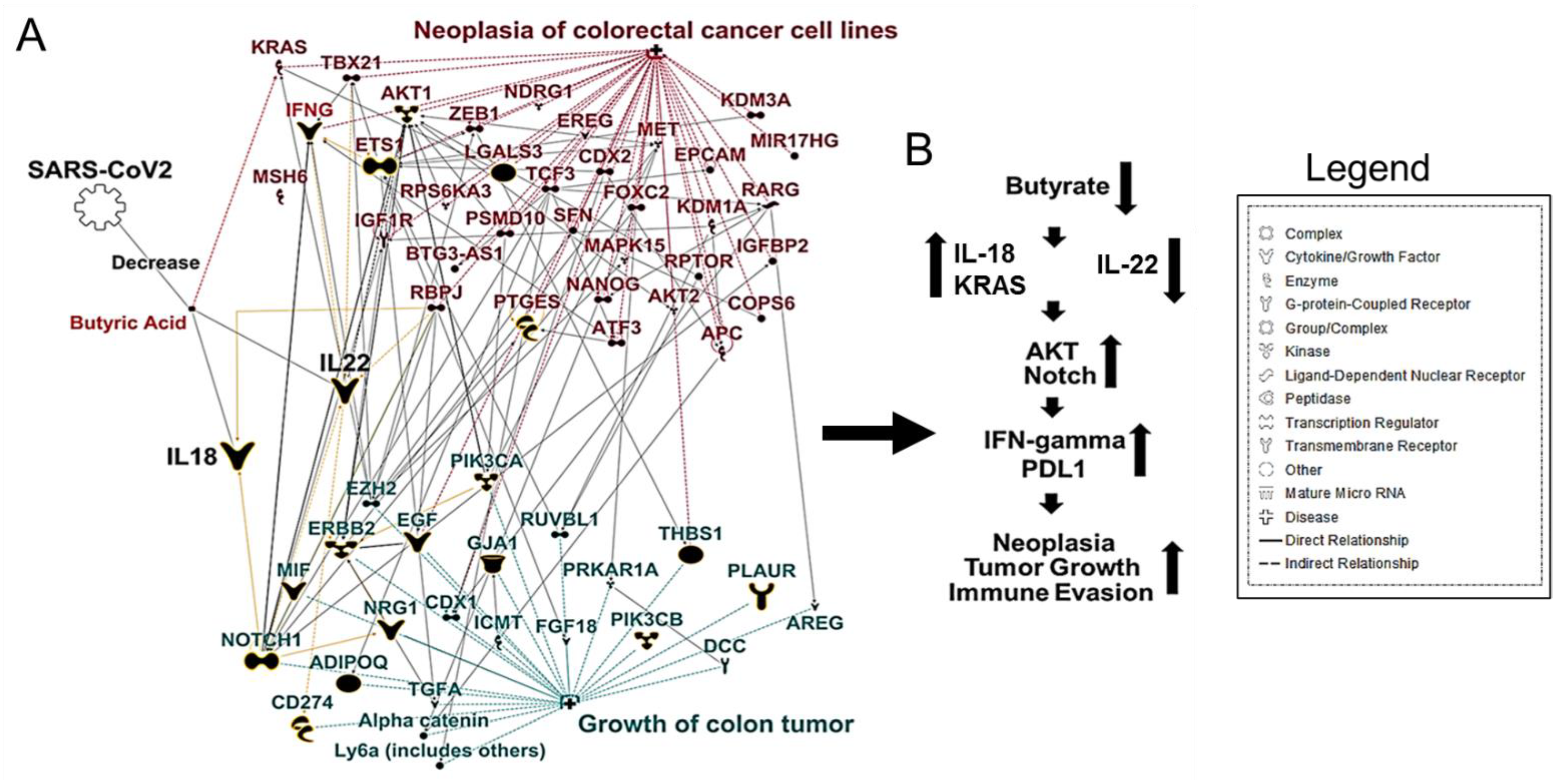
Typical findings in CRC patients are a marked decrease in Firmicutes, Bacteroides, and Actinobacteria, paired with increases in Fusobacterium and Porphyromonas populations [41]. Actinobacteria are one of the four major phyla of the gut microbiota. Although they represent only a small percentage of the bacterial community, Actinobacteria are pivotal in maintaining gut homeostasis and immune tolerance [42]. Unbalanced populations of Actinobacteria have been evidenced in several pathological conditions [43]. Specifically for CRC, the reduction in metabolites associated with the Actinobacteria phylum paired with a proinflammatory, cellular-mediated, cytotoxic T-helper cell-1 (Th1) immune response induced by this group lends itself to a poor prognosis of CRC [44]. A decrease in butyrate-producing bacteria (especially the Actinobacteria and Firmicutes phyla) also decreases the primary energy source for colonocytes. It increases intra-colonic pH, creating a hostile environment for colonocytes and contributing to tumorigenesis [41]. To further explore the relationship between butyrate and CRC, we used Ingenuity Pathway Analysis (IPA) [45] that uses a database of prior biological knowledge derived from analyzing and annotating the peer-reviewed scientific literature. We used the My Pathway/Path Designer tools in IPA to plot known interactions between butyrate and CRC. We found that gut dysbiosis could cause a decrease in butyrate-producing bacteria. A subsequent lack of IL-22 production allows bacterial metabolites to enter the circulatory system, leading to increased inflammatory cell infiltration, thus increasing colitis associated with colon cancer (Figure 1A,B).
Consumption of a high-fat and -protein diet has been linked to increased secretion of bile acids. Certain microbes convert into primary and secondary bile acids, which are toxic and promote tumorigenesis [46]. Bile acids are key signaling molecules that regulate digestive functions and physiological functions such as glucose and lipid metabolism and immune homeostasis [47]. Bile acids are synthesized from cholesterol and conjugated to glycine or taurine in hepatocytes. Most bile acids are secreted into the small intestine. However, bile acids that reach the large intestine will interact with gut microbes. Bile acids are toxic for many gut bacteria. Thus, high levels will put selective growth pressure on our gut microbiota, favoring certain bacteria in our gut to act enzymatically on the bile acids [47]. For example, excess taurine is excreted as a conjugated bile acid called taurocholic acid and converted into deoxycholic acid, which studies have shown to be genotoxic and promote tumor formation [48]. In studies, deoxycholic acid can activate cellular signaling pathways associated with cell proliferation and apoptosis [46]. A major enzyme in the production of deoxycholic acid, 7α-dehydroxylation, has been characterized in species belonging to the genera Eubacterium and Clostridium, including the species Clostridium scindens and Clostridium hylemonae [47].
It has been shown in mice that increasing the proportion of Lactobacillus and Bifidobacterium in the gut microbiota through probiotic supplementation (oral gavage daily of 0.6 billion CFU (colony forming units) each of Lactobacillus acidophilus, Lactobacillus rhamnosus, and Bifidobacterium bifidum, diluted in 200 μL of drinking water) reduced inflammatory cell infiltration, lowered chemokine expression, and reduced colitis-associated CRC [49]. Other studies have suggested that an expansion of Proteobacteria, usually a minor constituent of the gut microbiota, is a potential microbial signature of epithelial dysfunction observed in patients with CRC [39,50,51]. A complete understanding of the complex factors that lead to dysbiosis has not yet materialized, and the effect of this on CRC remains unclear.
3. SARS-CoV-2 Induced Gut Microbiome Dysbiosis and CRC
Although the most common COVID-19 symptoms are respiratory, SARS-CoV-2 infections also target the gastrointestinal tract, culminating in inflammation and intestinal cramps to diarrhea [52]. One hypothesis is that ACE2 downregulation, caused by SARS-CoV-2 infection, decreases activation of the mechanistic target of rapamycin (mTOR) and increases autophagy, leading to intestinal dysbiosis and diarrhea [52]. ACE2 expression in lungs is downregulated in wild-type mice infected with SARS-CoV and mice injected with recombinant SARS spike protein. This downregulation may play a role in SARS pathogenesis and disease progression to ARDS [53,54,55]. Another hypothesis is that the small bowel is likely a key site of amplification of the systemic inflammatory response, where blockage of ACE2 causes increased levels of angiotensinogen and hyperactivation of the renin–angiotensin system, leading to a shutdown of the amino acid transporter BA0T1 and a subsequent lack of cellular tryptophan, which leads to decreased secretion of antimicrobial peptides and gut dysbiosis [56].
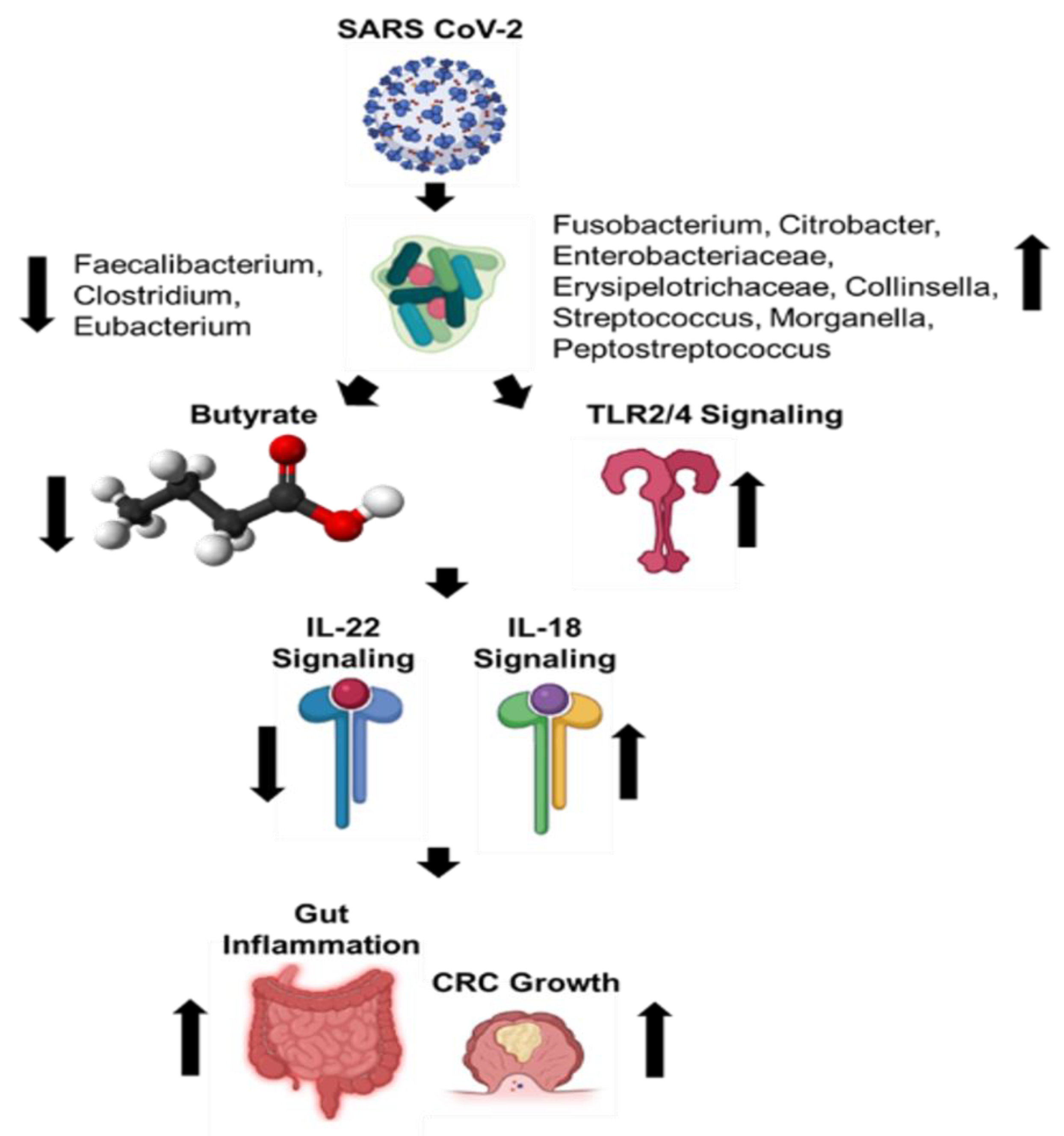
Recent studies have observed that patients with COVID-19 develop a dysbiotic microbiota of the gut [24,57,58,59,60,61] (Figure 2). One study investigated changes in fecal microbiomes of patients with SARS-CoV-2 infection during hospitalization and associations with severity and fecal shedding of the virus [24]. Patients with COVID-19 had significant alterations in their fecal microbiomes, characterized by enrichment of opportunistic pathogens and depletion of beneficial commensals at the time of hospitalization and at all time points during hospitalization. Depleted symbionts and gut dysbiosis persisted throughout hospitalization, even after clearance of SARS-CoV-2 and resolution of respiratory symptoms. Throughout hospitalization, Bacteroides dorei, Bacteroides taiotaomicron, Bacteroides massiliensis, and Bacteroides ovatus, which downregulate the expression of ACE2 in the murine gut, correlated inversely with SARS-CoV-2 load in fecal samples from patients. Interestingly, the baseline abundance of specific microbes in the gut, such as Coprobacillus, Clostridium ramosum, and Clostridium hathewayi, correlated with COVID-19 severity. There was an inverse correlation between the abundance of Faecalibacterium prausnitzii, an anti-inflammatory bacterium, and disease severity.
Another study investigated the changes in abundance of ten predominant intestinal bacterial groups in COVID-19 patients to establish a correlation between these bacterial groups and clinical indicators of pneumonia [58]. The results indicate that dysbiosis occurred in COVID-19 patients, and changes in the gut microbial community were associated with disease severity and hematological parameters. The number of common opportunistic pathogens, Enterococcus (Ec) and Enterobacteriaceae (E), were shown to be increased in COVID-19 patients, especially in the critically ill. Observations suggest that these bacterial groups can serve as diagnostic biomarkers for COVID-19 and that the Ec/E ratio can be used to predict death in critically ill patients.
The next study investigated the transcriptional activity of SARS-CoV-2 and its association with fecal microbiome alterations in COVID-19 patients [61]. Even in the absence of gastrointestinal (GI) symptoms, some patients continued to display an active viral infection signature up to 6 days after clearance of SARS-CoV-2 from respiratory samples. Fecal samples with a high SARS-CoV-2 signature had higher abundances of the bacterial species Collinsella aerofaciens, Collinsella tanakaei, Streptococcus infantis, and Morganella morganii. The gut microbiota of patients with active SARS-CoV-2 GI infection was characterized by enrichment of opportunistic pathogens, loss of salutary bacteria, increased functional capacity for nucleotide and amino acid biosynthesis, and carbohydrate metabolism. This study provides evidence for a dormant, prolonged GI infection by SARS-CoV-2, even in the absence of GI symptoms and after recovery from respiratory infection of SARS-CoV-2.
COVID-19 patients have also been shown to have significantly reduced bacterial diversity, a higher relative abundance of opportunistic pathogens, such as Streptococcus, Rothia, Veillonella, and Actinomyces, and a lower relative abundance of beneficial symbionts [57,59]. Levels of Fusicatenibacter, Romboutsia, Intestinibacter, Actinomyces, and Erysipelatoclostridium showed high accuracy for distinguishing COVID-19 patients, which suggests the potential value of the gut microbiota as a diagnostic biomarker and therapeutic target for COVID-19. Reduced bacterial diversity in the gut has been associated with acute and long-term metabolic effects and disease propensities.
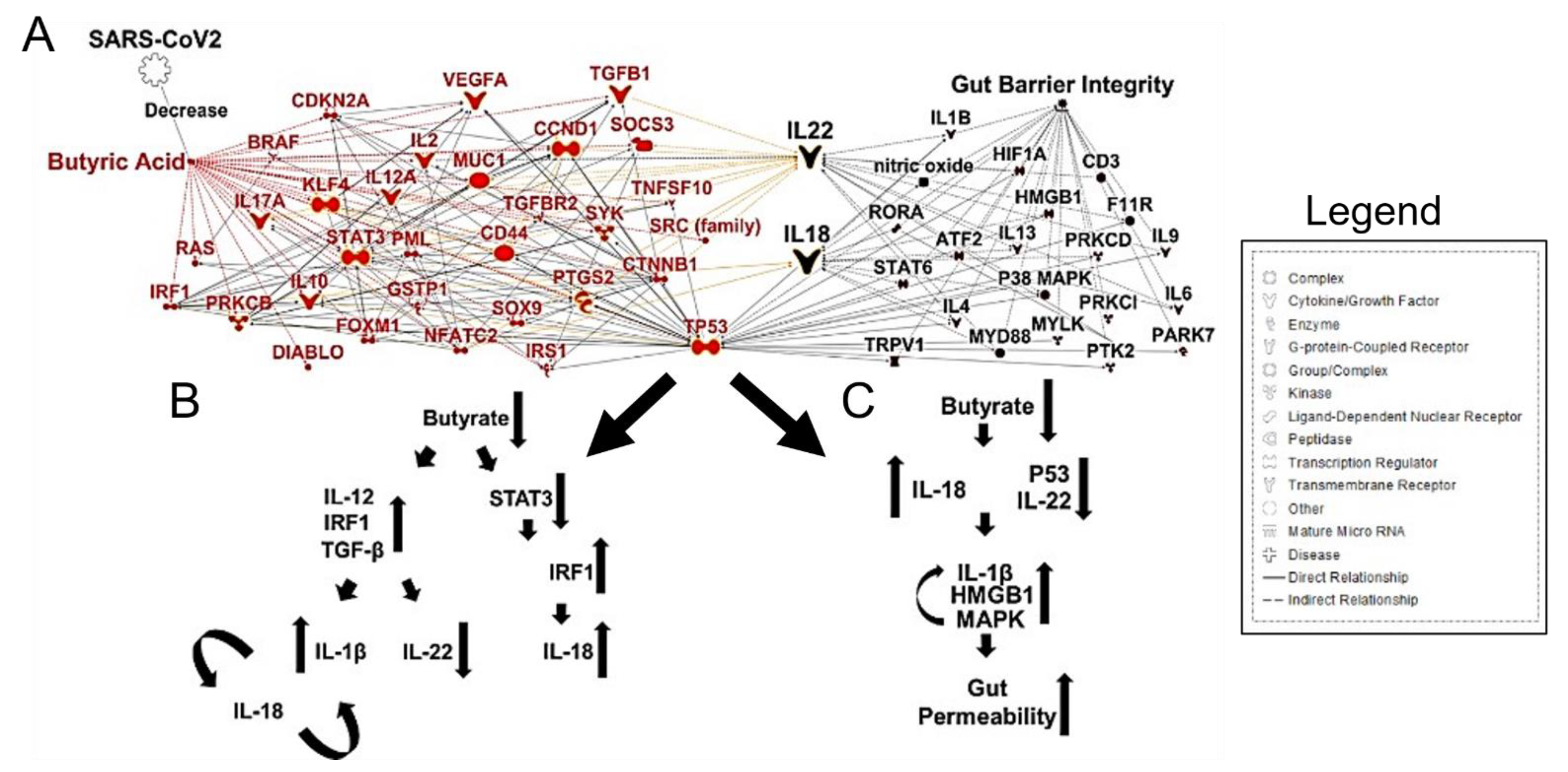
In patients with COVID-19, the abundance of butyrate-producing bacteria, such as Faecalibacterium prausnitzii, Clostridium butyricum, Clostridium leptum, and Eubacterium rectale, decreased significantly, and this shift in the bacterial community may help discriminate critically ill patients from patients that have a more moderate disease state [58]. Fecal samples from patients with low-to-no SARS-CoV-2 infectivity had higher abundances of SCFA-producing bacteria, Parabacteroides merdae, Bacteroides stercoris, Alistipes onderdonkii, and Lachnospiraceae bacterium 1_1_57FAA [61]. Importantly, butyrate-producing bacteria are of critical importance in maintaining gut barrier integrality. SCFAs have been implicated in signaling for IL-22, which maintains gut and lung epithelial barrier integrity [62]. Butyrate and other SCFAs regulate inflammation by macrophages in the intestine and promote the Warburg effect, which metabolically constrains the neoplastic cells [63]. CRC has a metabolic dependence on anaerobic glycolysis; thus, fatty acid oxidation is limited. Given this metabolic state, butyrate begins to accumulate in the cytoplasm of cancerous colonocytes, allowing this SCFA to act as an HDAC inhibitor, sensitizing the cancerous colonocytes to apoptotic pathways [64,65]. Specifically, a reduction in butyrate-producing bacteria and gut dysbiosis contributed to less IL-22 production, which is integral to maintain both gut and lung epithelial barrier integrity [66] (Figure 3A,B).
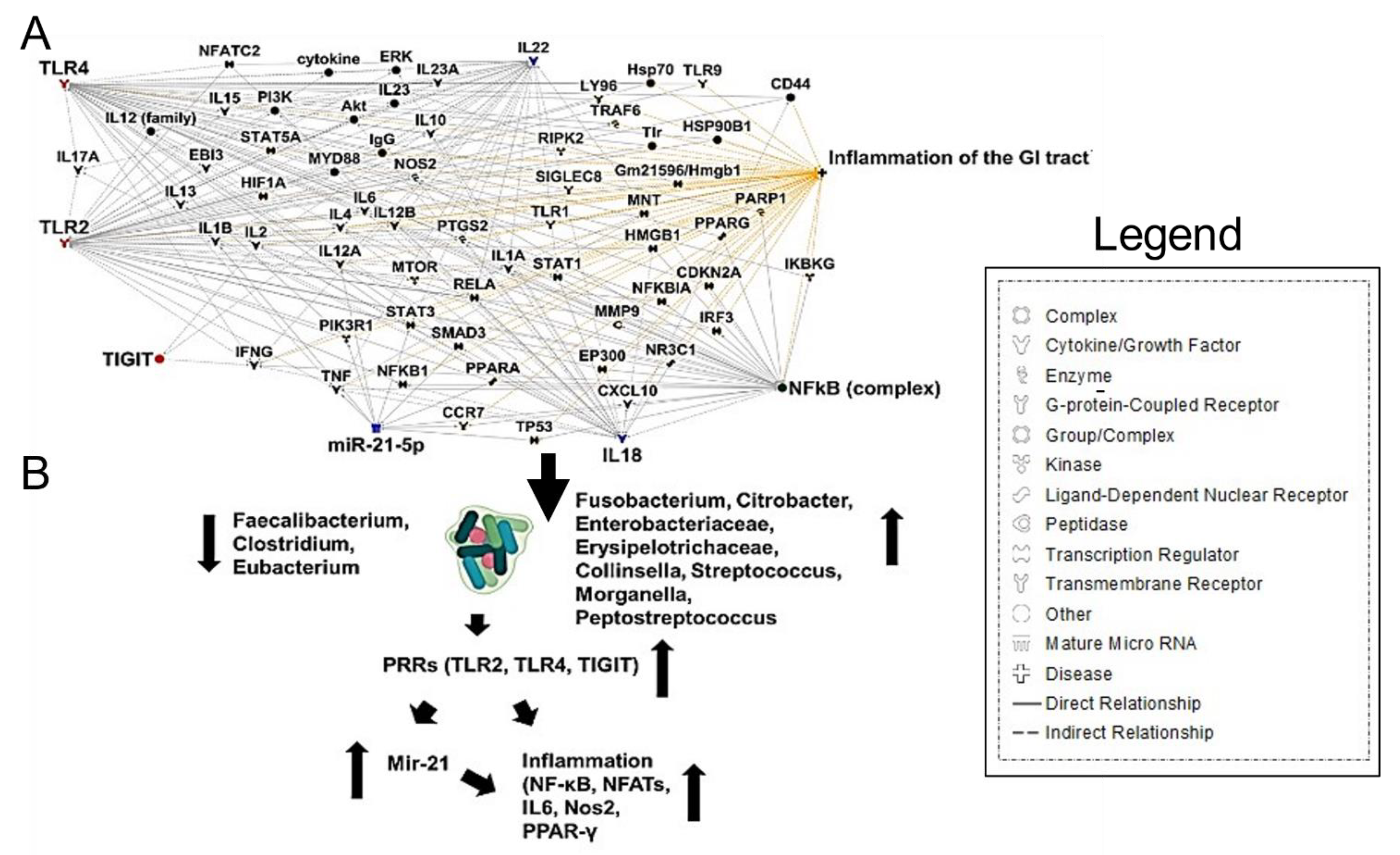
Fusobacterium nucleatum bacteremia has also been observed in severe COVID-19 cases and shown to colonize colon mucus with associated mucosal inflammation [67]. Along with the immune dysfunction seen in COVID-19, F. nucleatum causes immunosuppression by the action of one of its surface proteins, Fap2, which has been recognized as a galactose-binding lectin that can interact with the T cell ITIM domain (TIGIT) inhibitory receptor [68]. Furthermore, F. nucleatum was shown to interact with Toll-like receptors 2 and 4 signaling, resulting in increased microRNA-21 (miRNA21) expression, which promotes NF-kB induction, contributing to inflammation and cell proliferation [68] (Figure 4A,B). The intestinal inflammatory cytokine IL-18 was also shown to be elevated in the serum of COVID-19 patients [59]. These results indicate that gut microbiota composition changes contribute to the SARS-CoV-2-induced inflammatory cytokines production in the intestine.
Interestingly, one study also investigated changes in the fecal fungal microbiomes (mycobiome) of COVID-19 patients [69]. Patients with COVID-19 had significant alterations in their fecal mycobiomes, characterized by increased proportions of opportunistic fungal pathogens, Candida albicans, Candida auris, and Aspergillus flavus. Two respiratory-associated fungal pathogens, A. flavus and Aspergillus niger, were detected in fecal samples from a subset of patients with COVID-19, even after clearance of SARS-CoV-2 from nasopharyngeal samples and resolution of respiratory symptoms. These results are striking and re-enforce the commensal nature of all microbes, which may encompass bacteria, fungi, protists, and viruses alike.
There are increasing reports of persistent and prolonged effects after COVID-19, now termed “long haulers”, a syndrome characterized by persistent symptoms and delayed or long-term complications beyond 4–6 weeks from the onset of symptoms [70,71]. This may be caused by the observed post-acute COVID-19 syndrome seen in some cases, where immune dysregulation and gastrointestinal symptoms are still ongoing even after clearance of SARS-CoV-2, thus impacting the status of the patient’s microbiome [72,73]. Due to the recent nature of the COVID-19 pandemic, the time of restoration of normal gut microbiota has yet to be thoroughly investigated, so the timeline and long-term effects of dysbiosis are unknown and require further studies.
A well-known respiratory infection phenomenon is gut-barrier dysfunction, which is correlated with a more severe clinical course of the disease [74]. Clinically, it has been shown that modulating the gut microbiota can slow early influenza virus replication in lung epithelia, resulting in reduced enteritis and ventilator-associated pneumonia [74]. Expansion of Bifidobacterium species upon and after influenza infection, for example, has been shown to be protective from the inflammation that could cause dysbiotic events [75,76]. Currently, there is no direct clinical evidence that the modulation of the gut microbiota plays a therapeutic role in the treatment of COVID-19. However, clinical trials of probiotics against COVID-19 are underway [77]. Probiotics can help patients maintain immune homeostasis in the gut and avoid overactivation of the immune response by decreasing proinflammatory signaling and maintaining gut barrier integrity.
The human immune system has evolved to cope with the presence of microorganisms both inside our body and out [78]. This fact means that most infectious diseases caused by viruses or bacteria are self-limiting [79,80]. This could be one possible reason for the asymptomatic or mild nature of most COVID-19 cases [81]. These microorganisms can serve as a source of metabolites, such as essential amino acids and fatty acids, for the human body [82]. In a state of gut dysbiosis, a transient nutritional supply excess may occur, as both the microorganisms and the damaged host tissue will be degraded and become a possible source of nutrition. This may promote hyper inflammation during acute infection [83] and possibly lead to chronic diseases, such as cancer [84]. For example, some of the excess nutrition from damaged tissue, together with the excess nutrition from a dysbiotic gut microbiome, could be turned into lipid intermediates, causing lipotoxicity and further tissue damage [85]. This highlights how the nutritional state can impact a person’s health and disease outcome. As such, food intake restriction could offer a promising way to control chronic inflammation [86].
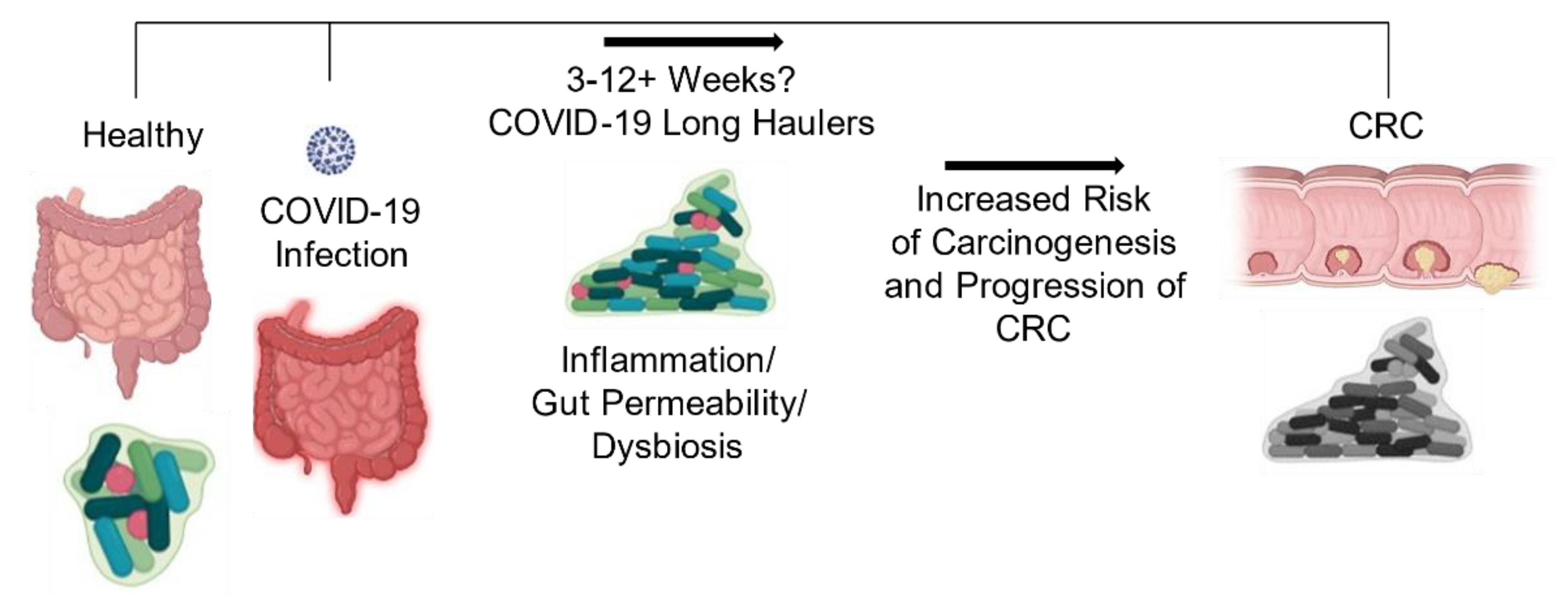
Together, these collective observations warrant greater investigation into the relationship between changes in the gut microbiota that encompass all microorganisms due to COVID-19 infection and associations with increased risk for CRC development or progression (Figure 5). Given the widespread incidence of this virus and that CRC is the third most common cancer diagnosed in the United States in both men and women, studies investigating the associated effects of these two diseases are in great need. Upon elucidating answers to these questions, it may be possible to develop effective probiotic therapies that maintain a more homeostatic gut environment during the disease, which could help improve CRC survival rates.
4. Conclusions and Future Directions
The SARS-CoV-2 pandemic has left many unanswered questions on the long-term impacts of this virus post-infection. This question is of particular importance to those with underlying comorbidities before the onset of COVID-19. Cancer is just one of many of said comorbidities. Still, the multifaceted nature of this disease and immunosuppressive treatments make understanding the role of COVID-19 in relation to cancer to be of the utmost importance. Once age is considered, those born in 1990 have about double the risk of colon cancer than people born around 1950 [30]. Factors such as dietary changes, greater preservatives in foods, and changes in hygiene practices may contribute to this observable phenomenon. The gut microbiota plays a crucial role in health and has been linked to CRC development [31]. Early investigations have shown that the gut microbiota and mycobiota are significantly altered in patients with COVID-19. Changes to the gut microbiota caused by SARS-CoV-2 infection include enrichment of opportunistic pathogens and depletion of beneficial commensals, an overall decline in microbial diversity, a loss of butyrate-producing bacteria, and F. nucleatum bacteremia. In both CRC and SARS-CoV-2 infection, the increased expression of genes involved in the inflammatory response leads to a worsening in gut barrier dysfunction. Changes caused by SARS-CoV-2 infection may further exacerbate CRC progression through increased expression of CRC tumorigenesis markers, tumor immunosuppression, and the induction of inflammation, leading to gut barrier disruption and worsening CRC progression (Figure 6).
A complete understanding of the complex factors leading to dysbiosis has not yet materialized. It is critically important that we understand how infection with SARS-CoV-2 will impact the gut microbiota and CRC progression. The impact of SARS-CoV-2 on gut dysbiosis and the gut microbiota may be long-lasting, thus underscoring the importance of restoring a competent microbiome to resist the development of GI diseases, such as irritable bowel syndrome, allergic colitis, recurrent Clostridioides difficile infection, and CRC [87,88].
Author Contributions
Literature gathering and analysis: M.C.H., R.G., A.R.M., R.D., S.M., and S.S.M. Ingenuity Pathway Analysis: M.C.H. and R.G. Wrote the manuscript: M.C.H., R.G., A.R.M., R.D., S.M., and S.S.M. Figure illustration: M.C.H., R.G., A.R.M., S.M., and S.S.M. All authors have read and agreed to the published version of the manuscript.
Funding
This work is supported by the Research Career Scientist Awards to Subhra Mohapatra (IK6BX004212) and Shyam S Mohapatra (IK6 BX003778), and the Veterans Affairs Merit Review grants, BX005490 and BX003413 to Subhra Mohapatra and BX003685 to Shyam S Mohapatra. Though this report is based upon work supported, in part, by the Department of Veterans Affairs, Veterans Health Administration, Office of Research and Development, the contents of this report do not represent the views of the Department of Veterans Affairs or the United States Government.
Conflicts of Interest
The authors declare no potential conflict of interest.
References
- WHO. WHO Coronavirus Disease (COVID-19) Dashboard. Available online: https://covid19.who.int (accessed on 5 April 2021).
- Rothan, H.A.; Byrareddy, S.N. The epidemiology and pathogenesis of coronavirus disease (COVID-19) outbreak. J. Autoimmun. 2020, 109, 102433. [Google Scholar] [CrossRef] [PubMed]
- Shang, J.; Wan, Y.; Luo, C.; Ye, G.; Geng, Q.; Auerbach, A.; Li, F. Cell entry mechanisms of SARS-CoV-2. Proc. Natl. Acad. Sci. USA 2020, 117, 11727–11734. [Google Scholar] [CrossRef] [PubMed]
- Huang, Y.; Yang, C.; Xu, X.F.; Xu, W.; Liu, S.W. Structural and functional properties of SARS-CoV-2 spike protein: Potential antivirus drug development for COVID-19. Acta Pharm. Sin. 2020, 41, 1141–1149. [Google Scholar] [CrossRef]
- Zang, R.; Gomez Castro, M.F.; McCune, B.T.; Zeng, Q.; Rothlauf, P.W.; Sonnek, N.M.; Liu, Z.; Brulois, K.F.; Wang, X.; Greenberg, H.B.; et al. TMPRSS2 and TMPRSS4 promote SARS-CoV-2 infection of human small intestinal enterocytes. Sci. Immunol. 2020, 5. [Google Scholar] [CrossRef] [PubMed]
- Cantuti-Castelvetri, L.; Ojha, R.; Pedro, L.D.; Djannatian, M.; Franz, J.; Kuivanen, S.; van der Meer, F.; Kallio, K.; Kaya, T.; Anastasina, M.; et al. Neuropilin-1 facilitates SARS-CoV-2 cell entry and infectivity. Science 2020, 370, 856–860. [Google Scholar] [CrossRef]
- Helal, M.A.; Shouman, S.; Abdelwaly, A.; Elmehrath, A.O.; Essawy, M.; Sayed, S.M.; Saleh, A.H.; El-Badri, N. Molecular basis of the potential interaction of SARS-CoV-2 spike protein to CD147 in COVID-19 associated-lymphopenia. J. Biomol. Struct. Dyn. 2020, 1–11. [Google Scholar] [CrossRef] [PubMed]
- Costela-Ruiz, V.J.; Illescas-Montes, R.; Puerta-Puerta, J.M.; Ruiz, C.; Melguizo-Rodríguez, L. SARS-CoV-2 infection: The role of cytokines in COVID-19 disease. Cytokine Growth Factor Rev. 2020, 54, 62–75. [Google Scholar] [CrossRef]
- Wang, B.; Li, R.; Lu, Z.; Huang, Y. Does comorbidity increase the risk of patients with COVID-19: Evidence from meta-analysis. Aging 2020, 12, 6049–6057. [Google Scholar] [CrossRef]
- McGill, A.R.; Kahlil, R.; Dutta, R.; Green, R.; Howell, M.; Mohapatra, S.; Mohapatra, S.S. SARS-CoV-2 Immuno-Pathogenesis and Potential for Diverse Vaccines and Therapies: Opportunities and Challenges. Infect. Dis. Rep. 2021, 13, 102–125. [Google Scholar] [CrossRef] [PubMed]
- Chamilos, G.; Lionakis, M.S.; Kontoyiannis, D.P. Are All Patients with Cancer at Heightened Risk for Severe Coronavirus Disease 2019 (COVID-19)? Clin. Infect. Dis. 2021, 72, 351–356. [Google Scholar] [CrossRef]
- Machado, D.; Pizzorno, A.; Hoffmann, J.; Traversier, A.; Endtz, H.; Lina, B.; Rosa-Calatrava, M.; Paranhos-Baccala, G.; Terrier, O. Role of p53/NF-kappaB functional balance in respiratory syncytial virus-induced inflammation response. J. Gen. Virol. 2018, 99, 489–500. [Google Scholar] [CrossRef] [PubMed]
- Yuan, L.; Chen, Z.; Song, S.; Wang, S.; Tian, C.; Xing, G.; Chen, X.; Xiao, Z.X.; He, F.; Zhang, L. p53 degradation by a coronavirus papain-like protease suppresses type I interferon signaling. J. Biol. Chem. 2015, 290, 3172–3182. [Google Scholar] [CrossRef] [Green Version]
- Dai, M.; Liu, D.; Liu, M.; Zhou, F.; Li, G.; Chen, Z.; Zhang, Z.; You, H.; Wu, M.; Zheng, Q.; et al. Patients with Cancer Appear More Vulnerable to SARS-CoV-2: A Multicenter Study during the COVID-19 Outbreak. Cancer Discov. 2020, 10, 783–791. [Google Scholar] [CrossRef] [PubMed]
- van Dam, P.A.; Huizing, M.; Mestach, G.; Dierckxsens, S.; Tjalma, W.; Trinh, X.B.; Papadimitriou, K.; Altintas, S.; Vermorken, J.; Vulsteke, C.; et al. SARS-CoV-2 and cancer: Are they really partners in crime? Cancer Treat Rev. 2020, 89, 102068. [Google Scholar] [CrossRef]
- Zhang, H.; Li, H.B.; Lyu, J.R.; Lei, X.M.; Li, W.; Wu, G.; Lyu, J.; Dai, Z.M. Specific ACE2 expression in small intestinal enterocytes may cause gastrointestinal symptoms and injury after 2019-nCoV infection. Int. J. Infect. Dis. 2020, 96, 19–24. [Google Scholar] [CrossRef] [PubMed]
- Bao, R.; Hernandez, K.; Huang, L.; Luke, J.J. ACE2 and TMPRSS2 expression by clinical, HLA, immune, and microbial correlates across 34 human cancers and matched normal tissues: Implications for SARS-CoV-2 COVID-19. J. Immunother Cancer 2020, 8. [Google Scholar] [CrossRef]
- Liu, C.; Wang, K.; Zhang, M.; Hu, X.; Hu, T.; Liu, Y.; Hu, Q.; Wu, S.; Yue, J. High expression of ACE2 and TMPRSS2 and clinical characteristics of COVID-19 in colorectal cancer patients. NPJ Precis Oncol. 2021, 5, 1–7. [Google Scholar] [CrossRef]
- Lamers, M.M.; Beumer, J.; van der Vaart, J.; Knoops, K.; Puschhof, J.; Breugem, T.I.; Ravelli, R.B.G.; Paul van Schayck, J.; Mykytyn, A.Z.; Duimel, H.Q.; et al. SARS-CoV-2 productively infects human gut enterocytes. Science 2020, 369, 50. [Google Scholar] [CrossRef] [PubMed]
- Deriu, E.; Boxx, G.M.; He, X.; Pan, C.; Benavidez, S.D.; Cen, L.; Rozengurt, N.; Shi, W.; Cheng, G. Influenza Virus Affects Intestinal Microbiota and Secondary Salmonella Infection in the Gut through Type I Interferons. Plos Pathog. 2016, 12, e1005572. [Google Scholar] [CrossRef]
- Zha, L.; Garrett, S.; Sun, J. Salmonella Infection in Chronic Inflammation and Gastrointestinal Cancer. Diseases 2019, 7, 28. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Tinsley, A.; Navabi, S.; Williams, E.D.; Liu, G.; Kong, L.; Coates, M.D.; Clarke, K. Increased Risk of Influenza and Influenza-Related Complications Among 140,480 Patients With Inflammatory Bowel Disease. Inflamm Bowel. Dis. 2019, 25, 369–376. [Google Scholar] [CrossRef]
- Sanchez-Alcoholado, L.; Ramos-Molina, B.; Otero, A.; Laborda-Illanes, A.; Ordonez, R.; Medina, J.A.; Gomez-Millan, J.; Queipo-Ortuno, M.I. The Role of the Gut Microbiome in Colorectal Cancer Development and Therapy Response. Cancers 2020, 12, 1406. [Google Scholar] [CrossRef]
- Zuo, T.; Zhang, F.; Lui, G.C.Y.; Yeoh, Y.K.; Li, A.Y.L.; Zhan, H.; Wan, Y.; Chung, A.C.K.; Cheung, C.P.; Chen, N.; et al. Alterations in Gut Microbiota of Patients With COVID-19 During Time of Hospitalization. Gastroenterology 2020, 159, 944–955. [Google Scholar] [CrossRef] [PubMed]
- Ma, W.T.; Yao, X.T.; Peng, Q.; Chen, D.K. The protective and pathogenic roles of IL-17 in viral infections: Friend or foe? Open Biol. 2019, 9, 190109. [Google Scholar] [CrossRef] [Green Version]
- Park, G.T.; Choi, K.C. Advanced new strategies for metastatic cancer treatment by therapeutic stem cells and oncolytic virotherapy. Oncotarget 2016, 7, 58684–58695. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Pasin, F.; Mascalchi Calveri, M.; Calabrese, A.; Pizzarelli, G.; Bongiovanni, I.; Andreoli, M.; Cattaneo, C.; Rignanese, G. Oncolytic effect of SARS-CoV2 in a patient with NK lymphoma. Acta Biomed. 2020, 91. [Google Scholar] [CrossRef]
- Zheng, M.; Gao, Y.; Wang, G.; Song, G.; Liu, S.; Sun, D.; Xu, Y.; Tian, Z. Functional exhaustion of antiviral lymphocytes in COVID-19 patients. Cell Mol. Immunol. 2020, 17, 533–535. [Google Scholar] [CrossRef] [Green Version]
- Gujar, S.; Pol, J.G.; Kim, Y.; Kroemer, G. Repurposing CD8+ T cell immunity against SARS-CoV-2 for cancer immunotherapy: A positive aspect of the COVID-19 pandemic? Oncoimmunology 2020, 9, 1794424. [Google Scholar] [CrossRef]
- Society, A.C. Cancer Facts & Figures 2020. Atlanta Am. Cancer Soc. 2020. [Google Scholar] [CrossRef]
- Louis, P.; Hold, G.L.; Flint, H.J. The gut microbiota, bacterial metabolites and colorectal cancer. Nat. Rev. Microbiol. 2014, 12, 661–672. [Google Scholar] [CrossRef]
- den Besten, G.; van Eunen, K.; Groen, A.K.; Venema, K.; Reijngoud, D.J.; Bakker, B.M. The role of short-chain fatty acids in the interplay between diet, gut microbiota, and host energy metabolism. J. Lipid Res. 2013, 54, 2325–2340. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Dhar, D.; Mohanty, A. Gut microbiota and Covid-19- possible link and implications. Virus Res. 2020, 285, 198018. [Google Scholar] [CrossRef] [PubMed]
- Dang, A.T.; Marsland, B.J. Microbes, metabolites, and the gut–lung axis. Mucosal. Immunol. 2019, 12, 843–850. [Google Scholar] [CrossRef] [Green Version]
- Carabotti, M.; Scirocco, A.; Maselli, M.A.; Severi, C. The gut-brain axis: Interactions between enteric microbiota, central and enteric nervous systems. Ann. Gastroenterol. 2015, 28, 203–209. [Google Scholar] [PubMed]
- Terruzzi, I.; Senesi, P. Does intestinal dysbiosis contribute to an aberrant inflammatory response to severe acute respiratory syndrome coronavirus 2 in frail patients? Nutrition 2020, 79–80, 110996. [Google Scholar] [CrossRef]
- Scanlan, P.D.; Shanahan, F.; Clune, Y.; Collins, J.K.; O’Sullivan, G.C.; O’Riordan, M.; Holmes, E.; Wang, Y.; Marchesi, J.R. Culture-independent analysis of the gut microbiota in colorectal cancer and polyposis. Env. Microbiol. 2008, 10, 789–798. [Google Scholar] [CrossRef]
- Gopalakrishnan, V.; Helmink, B.A.; Spencer, C.N.; Reuben, A.; Wargo, J.A. The Influence of the Gut Microbiome on Cancer, Immunity, and Cancer Immunotherapy. Cancer Cell 2018, 33, 570–580. [Google Scholar] [CrossRef] [Green Version]
- Sanapareddy, N.; Legge, R.M.; Jovov, B.; McCoy, A.; Burcal, L.; Araujo-Perez, F.; Randall, T.A.; Galanko, J.; Benson, A.; Sandler, R.S.; et al. Increased rectal microbial richness is associated with the presence of colorectal adenomas in humans. ISME J. 2012, 6, 1858–1868. [Google Scholar] [CrossRef] [Green Version]
- Zackular, J.P.; Baxter, N.T.; Iverson, K.D.; Sadler, W.D.; Petrosino, J.F.; Chen, G.Y.; Schloss, P.D. The gut microbiome modulates colon tumorigenesis. mBio 2013, 4, e00692–e00713. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Raskov, H.; Burcharth, J.; Pommergaard, H.C. Linking Gut Microbiota to Colorectal Cancer. J. Cancer 2017, 8, 3378–3395. [Google Scholar] [CrossRef] [PubMed]
- Vitetta, L.; Vitetta, G.; Hall, S. Immunological Tolerance and Function: Associations Between Intestinal Bacteria, Probiotics, Prebiotics, and Phages. Front. Immunol. 2018, 9, 2240. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Binda, C.; Lopetuso, L.R.; Rizzatti, G.; Gibiino, G.; Cennamo, V.; Gasbarrini, A. Actinobacteria: A relevant minority for the maintenance of gut homeostasis. Dig. Liver Dis. 2018, 50, 421–428. [Google Scholar] [CrossRef]
- Iwabuchi, N.; Takahashi, N.; Xiao, J.Z.; Miyaji, K.; Iwatsuki, K. In vitro Th1 cytokine-independent Th2 suppressive effects of bifidobacteria. Microbiol. Immunol. 2007, 51, 649–660. [Google Scholar] [CrossRef] [Green Version]
- Kramer, A.; Green, J.; Pollard, J., Jr.; Tugendreich, S. Causal analysis approaches in Ingenuity Pathway Analysis. Bioinformatics 2014, 30, 523–530. [Google Scholar] [CrossRef] [PubMed]
- Ridlon, J.M.; Wolf, P.G.; Gaskins, H.R. Taurocholic acid metabolism by gut microbes and colon cancer. Gut Microbes 2016, 7, 201–215. [Google Scholar] [CrossRef] [Green Version]
- Molinero, N.; Ruiz, L.; Sanchez, B.; Margolles, A.; Delgado, S. Intestinal Bacteria Interplay With Bile and Cholesterol Metabolism: Implications on Host Physiology. Front. Physiol. 2019, 10, 185. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bernstein, C.; Holubec, H.; Bhattacharyya, A.K.; Nguyen, H.; Payne, C.M.; Zaitlin, B.; Bernstein, H. Carcinogenicity of deoxycholate, a secondary bile acid. Arch. Toxicol. 2011, 85, 863–871. [Google Scholar] [CrossRef] [Green Version]
- Mendes, M.C.S.; Paulino, D.S.; Brambilla, S.R.; Camargo, J.A.; Persinoti, G.F.; Carvalheira, J.B.C. Microbiota modification by probiotic supplementation reduces colitis associated colon cancer in mice. World J. Gastroenterol. 2018, 24, 1995–2008. [Google Scholar] [CrossRef]
- Shin, N.R.; Whon, T.W.; Bae, J.W. Proteobacteria: Microbial signature of dysbiosis in gut microbiota. Trends Biotechnol. 2015, 33, 496–503. [Google Scholar] [CrossRef]
- Rizzatti, G.; Lopetuso, L.R.; Gibiino, G.; Binda, C.; Gasbarrini, A. Proteobacteria: A Common Factor in Human Diseases. Biomed. Res. Int. 2017, 2017, 9351507. [Google Scholar] [CrossRef] [Green Version]
- de Oliveira, A.P.; Lopes, A.L.F.; Pacheco, G.; de Sa Guimaraes Noleto, I.R.; Nicolau, L.A.D.; Medeiros, J.V.R. Premises among SARS-CoV-2, dysbiosis and diarrhea: Walking through the ACE2/mTOR/autophagy route. Med. Hypotheses 2020, 144, 110243. [Google Scholar] [CrossRef]
- Imai, Y.; Kuba, K.; Penninger, J.M. The discovery of angiotensin-converting enzyme 2 and its role in acute lung injury in mice. Exp. Physiol. 2008, 93, 543–548. [Google Scholar] [CrossRef]
- Silhol, F.; Sarlon, G.; Deharo, J.C.; Vaisse, B. Downregulation of ACE2 induces overstimulation of the renin-angiotensin system in COVID-19: Should we block the renin-angiotensin system? Hypertens. Res. 2020, 43, 854–856. [Google Scholar] [CrossRef] [PubMed]
- Kuba, K.; Imai, Y.; Rao, S.; Gao, H.; Guo, F.; Guan, B.; Huan, Y.; Yang, P.; Zhang, Y.; Deng, W.; et al. A crucial role of angiotensin converting enzyme 2 (ACE2) in SARS coronavirus-induced lung injury. Nat. Med. 2005, 11, 875–879. [Google Scholar] [CrossRef]
- Monkemuller, K.; Fry, L.C.; Rickes, S. Systemic inflammatory response and thrombosis due to alterations in the gut microbiota in COVID-19. Rev. Esp. Enferm. Dig. 2020, 112, 584–585. [Google Scholar] [CrossRef]
- Gu, S.; Chen, Y.; Wu, Z.; Chen, Y.; Gao, H.; Lv, L.; Guo, F.; Zhang, X.; Luo, R.; Huang, C.; et al. Alterations of the Gut Microbiota in Patients with COVID-19 or H1N1 Influenza. Clin. Infect. Dis. 2020. [Google Scholar] [CrossRef]
- Tang, L.; Gu, S.; Gong, Y.; Li, B.; Lu, H.; Li, Q.; Zhang, R.; Gao, X.; Wu, Z.; Zhang, J.; et al. Clinical Significance of the Correlation between Changes in the Major Intestinal Bacteria Species and COVID-19 Severity. Engineering 2020. [Google Scholar] [CrossRef]
- Tao, W.; Zhang, G.; Wang, X.; Guo, M.; Zeng, W.; Xu, Z.; Cao, D.; Pan, A.; Wang, Y.; Zhang, K.; et al. Analysis of the intestinal microbiota in COVID-19 patients and its correlation with the inflammatory factor IL-18. Med. Microecol. 2020. [Google Scholar] [CrossRef]
- Zhang, H.; Ai, J.W.; Yang, W.; Zhou, X.; He, F.; Xie, S.; Zeng, W.; Li, Y.; Yu, Y.; Gou, X.; et al. Metatranscriptomic Characterization of COVID-19 Identified A Host Transcriptional Classifier Associated With Immune Signaling. Clin. Infect. Dis. 2020. [Google Scholar] [CrossRef]
- Zuo, T.; Liu, Q.; Zhang, F.; Lui, G.C.; Tso, E.Y.; Yeoh, Y.K.; Chen, Z.; Boon, S.S.; Chan, F.K.; Chan, P.K.; et al. Depicting SARS-CoV-2 faecal viral activity in association with gut microbiota composition in patients with COVID-19. Gut 2020. [Google Scholar] [CrossRef]
- Jayasimhan, A.; Marino, E. Dietary SCFAs, IL-22, and GFAP: The Three Musketeers in the Gut-Neuro-Immune Network in Type 1 Diabetes. Front. Immunol. 2019, 10, 2429. [Google Scholar] [CrossRef]
- McNabney, S.M.; Henagan, T.M. Short Chain Fatty Acids in the Colon and Peripheral Tissues: A Focus on Butyrate, Colon Cancer, Obesity and Insulin Resistance. Nutrients 2017, 9, 1348. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bultman, S.J. The microbiome and its potential as a cancer preventive intervention. Semin. Oncol. 2016, 43, 97–106. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Encarnacao, J.C.; Abrantes, A.M.; Pires, A.S.; Botelho, M.F. Revisit dietary fiber on colorectal cancer: Butyrate and its role on prevention and treatment. Cancer Metastasis Rev. 2015, 34, 465–478. [Google Scholar] [CrossRef] [PubMed]
- Lo, B.C.; Shin, S.B.; Canals Hernaez, D.; Refaeli, I.; Yu, H.B.; Goebeler, V.; Cait, A.; Mohn, W.W.; Vallance, B.A.; McNagny, K.M. IL-22 Preserves Gut Epithelial Integrity and Promotes Disease Remission during Chronic Salmonella Infection. J. Immunol. 2019, 202, 956. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wolff, L.; Martiny, D.; Deyi, V.Y.M.; Maillart, E.; Clevenbergh, P.; Dauby, N. COVID-19-Associated Fusobacterium nucleatum Bacteremia, Belgium. Emerg. Infect. Dis. 2021, 27, 975–977. [Google Scholar] [CrossRef]
- Sun, C.H.; Li, B.B.; Wang, B.; Zhao, J.; Zhang, X.Y.; Li, T.T.; Li, W.B.; Tang, D.; Qiu, M.J.; Wang, X.C.; et al. The role of Fusobacterium nucleatum in colorectal cancer: From carcinogenesis to clinical management. Chronic Dis. Transl. Med. 2019, 5, 178–187. [Google Scholar] [CrossRef]
- Zuo, T.; Zhan, H.; Zhang, F.; Liu, Q.; Tso, E.Y.K.; Lui, G.C.Y.; Chen, N.; Li, A.; Lu, W.; Chan, F.K.L.; et al. Alterations in Fecal Fungal Microbiome of Patients with COVID-19 During Time of Hospitalization until Discharge. Gastroenterology 2020, 159, 1302–1310. [Google Scholar] [CrossRef]
- Leviner, S. Recognizing the Clinical Sequelae of COVID-19 in Adults: COVID-19 Long-Haulers. J. Nurse Pract. 2021. [Google Scholar] [CrossRef]
- Nalbandian, A.; Sehgal, K.; Gupta, A.; Madhavan, M.V.; McGroder, C.; Stevens, J.S.; Cook, J.R.; Nordvig, A.S.; Shalev, D.; Sehrawat, T.S.; et al. Post-acute COVID-19 syndrome. Nat. Med. 2021, 27, 601–615. [Google Scholar] [CrossRef]
- Amenta, E.M.; Spallone, A.; Rodriguez-Barradas, M.C.; El Sahly, H.M.; Atmar, R.L.; Kulkarni, P.A. Postacute COVID-19: An Overview and Approach to Classification. Open Forum. Infect. Dis. 2020, 7, ofaa509. [Google Scholar] [CrossRef]
- Carfì, A.; Bernabei, R.; Landi, F.; The Gemelli against COVID-19 Post-Acute Care Study Group. Persistent Symptoms in Patients after Acute COVID-19. JAMA 2020, 324, 603–605. [Google Scholar] [CrossRef] [PubMed]
- Gao, Q.Y.; Chen, Y.X.; Fang, J.Y. 2019 Novel coronavirus infection and gastrointestinal tract. J. Dig. Dis. 2020, 21, 125–126. [Google Scholar] [CrossRef] [Green Version]
- Yasui, H.; Kiyoshima, J.; Hori, T.; Shida, K. Protection against influenza virus infection of mice fed Bifidobacterium breve YIT4064. Clin. Diagn. Lab. Immunol. 1999, 6, 186–192. [Google Scholar] [CrossRef] [Green Version]
- Zhang, Q.; Hu, J.; Feng, J.W.; Hu, X.T.; Wang, T.; Gong, W.X.; Huang, K.; Guo, Y.X.; Zou, Z.; Lin, X.; et al. Influenza infection elicits an expansion of gut population of endogenous Bifidobacterium animalis which protects mice against infection. Genome Biol. 2020, 21, 99. [Google Scholar] [CrossRef]
- Baindara, P.; Chakraborty, R.; Holliday, Z.M.; Mandal, S.M.; Schrum, A.G. Oral probiotics in coronavirus disease 2019: Connecting the gut-lung axis to viral pathogenesis, inflammation, secondary infection and clinical trials. New Microbes New Infect. 2021, 40, 100837. [Google Scholar] [CrossRef]
- Broderick, N.A. A common origin for immunity and digestion. Front. Immunol. 2015, 6, 72. [Google Scholar] [CrossRef]
- Levin, B.R.; Antia, R. Why we don’t get sick: The within-host population dynamics of bacterial infections. Science 2001, 292, 1112–1115. [Google Scholar] [CrossRef] [PubMed]
- Levin, B.R.; Baquero, F.; Ankomah, P.P.; McCall, I.C. Phagocytes, Antibiotics, and Self-Limiting Bacterial Infections. Trends Microbiol. 2017, 25, 878–892. [Google Scholar] [CrossRef]
- Azkur, A.K.; Akdis, M.; Azkur, D.; Sokolowska, M.; van de Veen, W.; Bruggen, M.C.; O’Mahony, L.; Gao, Y.; Nadeau, K.; Akdis, C.A. Immune response to SARS-CoV-2 and mechanisms of immunopathological changes in COVID-19. Allergy 2020, 75, 1564–1581. [Google Scholar] [CrossRef] [PubMed]
- McFall-Ngai, M.; Hadfield, M.G.; Bosch, T.C.; Carey, H.V.; Domazet-Loso, T.; Douglas, A.E.; Dubilier, N.; Eberl, G.; Fukami, T.; Gilbert, S.F.; et al. Animals in a bacterial world, a new imperative for the life sciences. Proc. Natl. Acad Sci. USA 2013, 110, 3229–3236. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Troisi, J.; Venutolo, G.; Pujolassos Tanya, M.; Delli Carri, M.; Landolfi, A.; Fasano, A. COVID-19 and the gastrointestinal tract: Source of infection or merely a target of the inflammatory process following SARS-CoV-2 infection? World J. Gastroenterol. 2021, 27, 1406–1418. [Google Scholar] [CrossRef] [PubMed]
- Saltiel, A.R.; Olefsky, J.M. Inflammatory mechanisms linking obesity and metabolic disease. J. Clin. Investig. 2017, 127, 1–4. [Google Scholar] [CrossRef] [PubMed]
- Garbarino, J.; Sturley, S.L. Saturated with fat: New perspectives on lipotoxicity. Curr. Opin Clin. Nutr. Metab. Care 2009, 12, 110–116. [Google Scholar] [CrossRef]
- Gonzalez, O.; Tobia, C.; Ebersole, J.; Novak, M.J. Caloric restriction and chronic inflammatory diseases. Oral. Dis. 2012, 18, 16–31. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Whisner, C.M.; Athena Aktipis, C. The Role of the Microbiome in Cancer Initiation and Progression: How Microbes and Cancer Cells Utilize Excess Energy and Promote One Another’s Growth. Curr. Nutr. Rep. 2019, 8, 42–51. [Google Scholar] [CrossRef] [Green Version]
- Xiao, Y.; Angulo, M.T.; Lao, S.; Weiss, S.T.; Liu, Y.Y. An ecological framework to understand the efficacy of fecal microbiota transplantation. Nat. Commun. 2020, 11, 3329. [Google Scholar] [CrossRef]
Figure 1.
SARS-CoV-2 Infection: Implications for CRC. (A) Ingenuity Pathway Analysis (IPA)-generated network map showing known connections among butyrate, IL-18, IL-22, and CRC in IPA. (B) Simplified schematic of (A), showing gut dysbiosis caused by a decrease in butyrate-producing bacteria and a subsequent lack of IL-22 production, which allows bacterial metabolites to enter the circulatory system leading to an increase in inflammatory markers, thus increasing colitis-associated colon cancer.
Figure 1.
SARS-CoV-2 Infection: Implications for CRC. (A) Ingenuity Pathway Analysis (IPA)-generated network map showing known connections among butyrate, IL-18, IL-22, and CRC in IPA. (B) Simplified schematic of (A), showing gut dysbiosis caused by a decrease in butyrate-producing bacteria and a subsequent lack of IL-22 production, which allows bacterial metabolites to enter the circulatory system leading to an increase in inflammatory markers, thus increasing colitis-associated colon cancer.

Figure 2.
Schematic showing changes in the gut microbiome caused by SARS-CoV-2 infection, their correlation with COVID-19 severity, and the biological consequences of these changes [24,57,58,59,61].

Figure 3.
SARS-CoV-2 Infection, Butyrate, and Gut Barrier Integrity. (A) Ingenuity Pathway Analysis (IPA) (Qiagen)-generated network map showing known connections among butyrate, IL-18, IL-22, and gut barrier integrity. (B,C) A reduction in butyrate-producing bacteria disrupts gut epithelial barrier integrity via IL-22 signaling and promotes inflammatory signaling through IL-18.
Figure 3.
SARS-CoV-2 Infection, Butyrate, and Gut Barrier Integrity. (A) Ingenuity Pathway Analysis (IPA) (Qiagen)-generated network map showing known connections among butyrate, IL-18, IL-22, and gut barrier integrity. (B,C) A reduction in butyrate-producing bacteria disrupts gut epithelial barrier integrity via IL-22 signaling and promotes inflammatory signaling through IL-18.

Figure 4.
Fusobacterium nucleatum Bacteremia Causes Gut inflammation. (A) Ingenuity Pathway Analysis (IPA)-generated network map showing pathway responsible for the F. nucleatum induction of inflammation. (B) F. nucleatum interacts with Toll-like receptors 2 and 4, resulting in increased miRNA-21 expression, which promotes NF-kB induction and contributes to the induction of inflammation.
Figure 4.
Fusobacterium nucleatum Bacteremia Causes Gut inflammation. (A) Ingenuity Pathway Analysis (IPA)-generated network map showing pathway responsible for the F. nucleatum induction of inflammation. (B) F. nucleatum interacts with Toll-like receptors 2 and 4, resulting in increased miRNA-21 expression, which promotes NF-kB induction and contributes to the induction of inflammation.

Figure 5.
A schematic showing COVID-19-Induced Gut Microbiome Changes Increase the Risk of Carcinogenesis and Progression of CRC. COVID-19 infection leads to an increased risk of CRC carcinogenesis and progression.
Figure 5.
A schematic showing COVID-19-Induced Gut Microbiome Changes Increase the Risk of Carcinogenesis and Progression of CRC. COVID-19 infection leads to an increased risk of CRC carcinogenesis and progression.

Figure 6.
A summary COVID-19-Induced Gut Microbiome Changes Increase the Risk of Carcinogenesis and Progression of CRC. Changes to the gut microbiota caused by SARS-CoV-2 lead to increased expression of genes involved in the inflammatory response, resulting in gut barrier disruption and increased risk of CRC.
Figure 6.
A summary COVID-19-Induced Gut Microbiome Changes Increase the Risk of Carcinogenesis and Progression of CRC. Changes to the gut microbiota caused by SARS-CoV-2 lead to increased expression of genes involved in the inflammatory response, resulting in gut barrier disruption and increased risk of CRC.

Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
MDPI and ACS Style
Howell, M.C.; Green, R.; McGill, A.R.; Dutta, R.; Mohapatra, S.; Mohapatra, S.S. SARS-CoV-2-Induced Gut Microbiome Dysbiosis: Implications for Colorectal Cancer. Cancers 2021, 13, 2676. https://doi.org/10.3390/cancers13112676
AMA Style
Howell MC, Green R, McGill AR, Dutta R, Mohapatra S, Mohapatra SS. SARS-CoV-2-Induced Gut Microbiome Dysbiosis: Implications for Colorectal Cancer. Cancers. 2021; 13(11):2676. https://doi.org/10.3390/cancers13112676
Chicago/Turabian StyleHowell, Mark C., Ryan Green, Andrew R. McGill, Rinku Dutta, Subhra Mohapatra, and Shyam S. Mohapatra. 2021. "SARS-CoV-2-Induced Gut Microbiome Dysbiosis: Implications for Colorectal Cancer" Cancers 13, no. 11: 2676. https://doi.org/10.3390/cancers13112676
Note that from the first issue of 2016, this journal uses article numbers instead of page numbers. See further details here.