
Pulsed Dose Rate Brachytherapy of Lip Carcinoma: Clinical Outcome and Quality of Life Analysis

 ,
,
Abstract
:Simple Summary
Abstract
1. Introduction
2. Materials and Methods
2.1. Patients Characteristics
2.2. Brachytherapy Procedure
2.3. Follow-Up
3. Results
3.1. Patients Characteristics and Treatment Data
3.2. Toxicity
3.3. Quality of Life Analysis
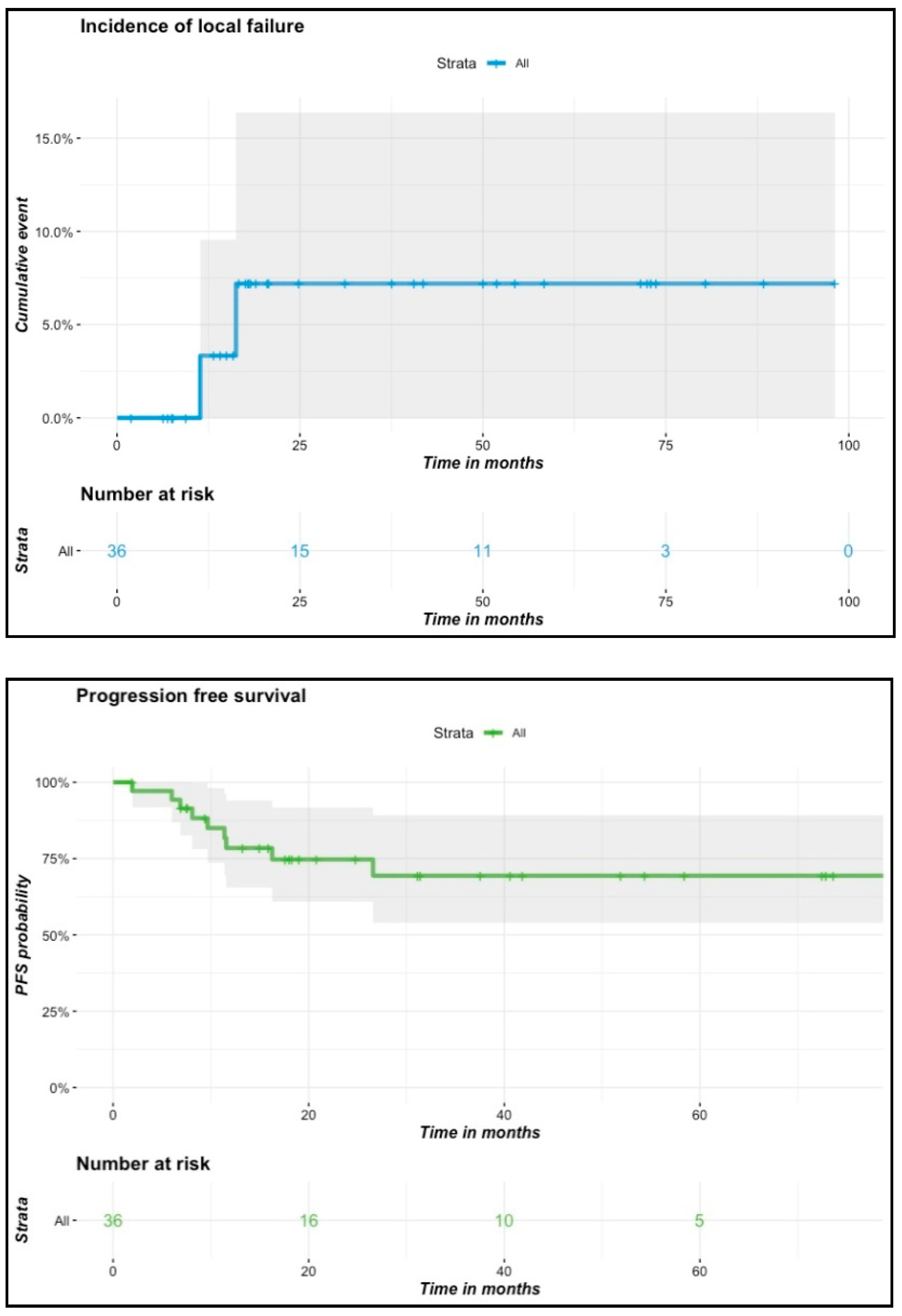
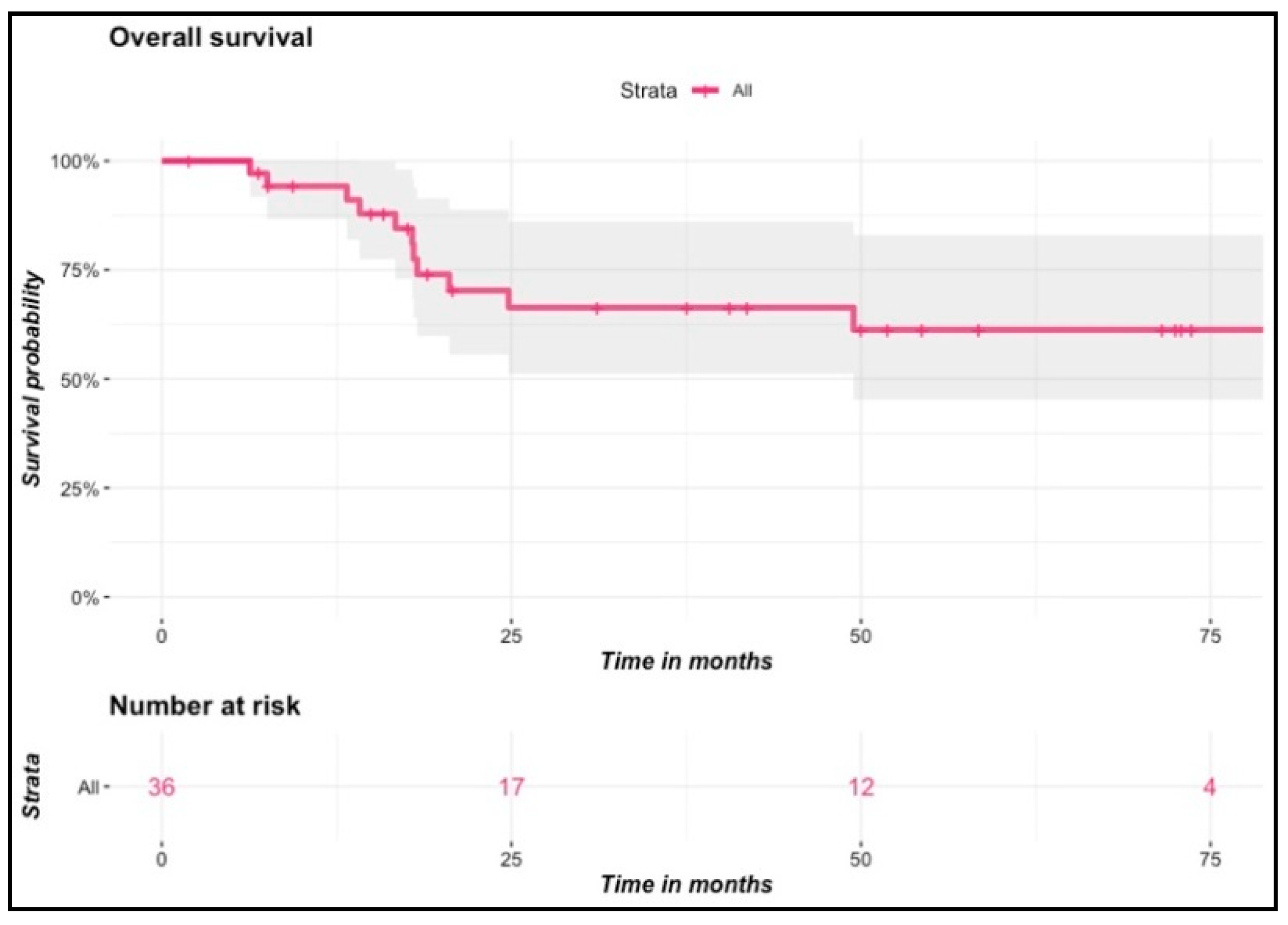
3.4. Tumor Control Analysis
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Shield, K.D.; Ferlay, J.; Jemal, A.; Sankaranarayanan, R.; Chaturvedi, A.K.; Bray, F.; Soerjomataram, I. The global incidence of lip, oral cavity, and pharyngeal cancers by subsite in 2012. CA Cancer J. Clin. 2017, 67, 51–64. [Google Scholar] [CrossRef]
- Warnakulasuriya, S. Global epidemiology of oral and oropharyngeal cancer. Oral Oncol. 2009, 45, 309–316. [Google Scholar] [CrossRef]
- van Leeuwen, M.T.; Grulich, A.E.; McDonald, S.P.; McCredie, M.R.E.; Amin, J.; Stewart, J.H.; Webster, A.C.; Chapman, J.R.; Vajdic, C.M. Immunosuppression and other risk factors for lip cancer after kidney transplantation. Cancer Epidemiol. Biomark. 2009, 18, 561–569. [Google Scholar] [CrossRef] [Green Version]
- de Visscher, J.G.; Botke, G.; Schakenraad, J.A.; van der Waal, I. A comparison of results after radiotherapy and surgery for stage I squamous cell carcinoma of the lower lip. Int. J. Oral Maxillofac. Surg. 1999, 28, 67. [Google Scholar] [CrossRef]
- Gerbaulet, A.; Pötter, R.; Mazeron, J.-J.; Meertens, H.; Limbergen, E.; Mazeron, J.-J. The GEC ESTRO Handbook of Brachytherapy; ACCO: Leuven, Belgium, 2002. [Google Scholar]
- Due, A.K.; Vogelius, I.R.; Aznar, M.C.; Bentzen, S.M.; Berthelsen, A.K.; Korreman, S.S.; Loft, A.; Kristensen, C.A.; Specht, L. Recurrences after intensity modulated radiotherapy for head and neck squamous cell carcinoma more likely to originate from regions with high baseline [18F]-FDG uptake. Radiother. Oncol. 2014, 111, 360–365. [Google Scholar] [CrossRef] [Green Version]
- Chargari, C.; Deutsch, E.; Blanchard, P.; Gouy, S.; Martelli, H.; Guérin, F.; Dumas, I.; Bossi, A.; Morice, P.; Viswanathan, A.N.; et al. Brachytherapy: An overview for clinicians. CA A Cancer J. Clin. 2019, 69, 386–401. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bacorro, W.; Escande, A.; Temam, S.; Dumas, I.; Routier, E.; Gensse, M.-C.; Blanchard, P.; Janot, F.; Mateus, C.; Tao, Y.; et al. Clinical outcomes after interstitial brachytherapy for early-stage nasal squamous cell carcinoma. Brachytherapy 2017, 16, 1021–1027. [Google Scholar] [CrossRef] [PubMed]
- Kovács, G.; Martinez-Monge, R.; Budrukkar, A.; Guinot, J.L.; Johansson, B.; Strnad, V.; Skowronek, J.; Rovirosa, A.; Siebert, F.-A. GEC-ESTRO ACROP recommendations for head & neck brachytherapy in squamous cell carcinomas: 1st update—Improvement by cross sectional imaging based treatment planning and stepping source technology. Radiother. Oncol. 2017, 122, 248–254. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- FACIT.org Home. Available online: https://www.facit.org/FACITOrg (accessed on 27 August 2020).
- Bilkay, U.; Kerem, H.; Ozek, C.; Gundogan, H.; Guner, U.; Gurler, T.; Akin, Y. Management of lower lip cancer: A retrospective analysis of 118 patients and review of the literature. Ann. Plast. Surg. 2003, 50, 50. [Google Scholar] [CrossRef]
- Vukadinovic, M.; Jezdic, Z.; Petrovic, L.; Medenica, L.M.; Lens, M. Surgical management of squamous cell carcinoma of the lip: Analysis of a 10-year experience in 223 patients. J. Oral Maxillofac. Surg. 2007, 65, 675–679. [Google Scholar] [CrossRef]
- Zitsch, R.P., 3rd; Park, C.W.; Renner, G.J.; Rea, J.L. Outcome analysis for lip carcinoma. Otolaryngol. Head Neck Surg. 1995, 113, 589–596. [Google Scholar] [CrossRef]
- Coppit, G.L.; Lin, D.T.; Burkey, B.B. Current concepts in lip reconstruction. Curr. Opin. Otolaryngol. Head Neck Surg. 2004, 12, 281–287. [Google Scholar] [CrossRef]
- Boukovalas, S.; Boson, A.L.; Hays, J.P.; Malone, C.H.; Cole, E.L.; Wagner, R.F. A Systematic Review of Lower Lip Anatomy, Mechanics of Local Flaps, and Special Considerations for Lower Lip Reconstruction. J. Drugs Dermatol. JDD 2017, 16, 1254–1261. [Google Scholar]
- Lubek, J.E.; Ord, R.A. Lip Reconstruction. Oral Maxillofac. Surg. Clin. N. Am. 2013, 25, 203–214. [Google Scholar] [CrossRef] [PubMed]
- Mut, A.; Guinot, J.L.; Arribas, L.; Díez-Presa, L.; Tortajada, M.I.; Santos, M.Á.; Samper, J.; Santamaría, P.; Vendrell, J.B. High Dose Rate Brachytherapy in Early Stage Squamous-Cell Carcinoma of the Lip. Acta Otorrinolaringol. 2016, 67, 282–287. [Google Scholar] [CrossRef] [PubMed]
- Ghadjar, P.; Bojaxhiu, B.; Simcock, M.; Terribilini, D.; Isaak, B.; Gut, P.; Wolfensberger, P.; Brömme, J.O.; Geretschläger, A.; Behrensmeier, F.; et al. High Dose-Rate Versus Low Dose-Rate Brachytherapy for Lip Cancer. Int. J. Radiat. Oncol. 2012, 83, 1205–1212. [Google Scholar] [CrossRef]
- Ayerra, A.Q.; Mena, E.P.; Fabregas, J.P.; Miguelez, C.G.; Guedea, F. HDR and LDR Brachytherapy in the Treatment of Lip Cancer: The Experience of the Catalan Institute of Oncology. J. Contemp. Brachyther. 2010, 2, 9–13. [Google Scholar] [CrossRef]
- Guinot, J.-L.; Arribas, L.; Tortajada, M.I.; Crispín, V.; Carrascosa, M.; Santos, M.; Mut, A.; Vendrell, J.B.; Pesudo, C.; Chust, M.L. From low-dose-rate to high-dose-rate brachytherapy in lip carcinoma: Equivalent results but fewer complications. Brachytherapy 2013, 12, 528–534. [Google Scholar] [CrossRef] [PubMed]
- Skowronek, J. Pulsed dose rate brachytherapy—Is it the right way? J. Contemp. Brachyther. 2010, 3, 107–113. [Google Scholar] [CrossRef]
- Johansson, B.; Karlsson, L.; Hardell, L.; Persliden, J. Clinical Investigations Long term results of PDR brachytherapy for lip cancer. J. Contemp. Brachyther. 2011, 2, 65–69. [Google Scholar] [CrossRef]
- Serkies, K.; Ziemlewski, A.; Sawicki, T.; Kaminska, J.; Dziadziuszko, R. Pulsed dose rate brachytherapy of lip cancer. J. Contemp. Brachyther. 2013, 3, 144–147. [Google Scholar] [CrossRef] [PubMed]
- Strnad, V.; Lotter, M.; Kreppner, S.; Fietkau, R. Interstitial pulsed-dose-rate brachytherapy for head and neck cancer—Single-institution long-term results of 385 patients. Brachytherapy 2013, 12, 521–527. [Google Scholar] [CrossRef] [Green Version]
- Mazeron, J.-J.; Ardiet, J.-M.; Haie-Méder, C.; Kovács, G.; Levendag, P.; Peiffert, D.; Polo, A.; Rovirosa, A.; Strnad, V. GEC-ESTRO recommendations for brachytherapy for head and neck squamous cell carcinomas. Radiother. Oncol. 2009, 91, 150–156. [Google Scholar] [CrossRef] [PubMed]
- Vartanian, J.G.; Carvalho, A.L.; Filho, M.J.D.A.; Junior, M.H.; Magrin, J.; Kowalski, L.P. Predictive factors and distribution of lymph node metastasis in lip cancer patients and their implications on the treatment of the neck. Oral Oncol. 2004, 40, 223–227. [Google Scholar] [CrossRef] [PubMed]
- Cowen, D.; Essomba, M.; Richaud, P.; Renaud-Salis, J.L.; Pigneux, J. Treatment of cervical lymph nodes in lip cancers. Bull. Cancer/Radiothérapie 1990, 77, 7. [Google Scholar]
- Guinot, J.-L.; Arribas, L.; Vendrell, J.B.; Santos, M.; Tortajada, M.I.; Mut, A.; Cruz, J.; Mengual, J.L.; Chust, M.L. Prognostic factors in squamous cell lip carcinoma treated with high-dose-rate brachytherapy. Head Neck 2014, 36, 1737–1742. [Google Scholar] [CrossRef]
- Kavabata, N.K.; Caly, D.N.; Ching, T.H.; Gonçalves, A.J.; Kowalski, L.P.; Cernea, C.R. Predictive factors for late cervical metastasis in stage I and II squamous cell carcinoma of the lip. Eur. Arch. Oto-Rhino-Laryngol. 2019, 276, 2047–2053. [Google Scholar] [CrossRef]
- Kuscu, O.; Bajin, M.D.; Süslü, N.; Hoşal, A. Şefik the role of suprahyoid neck dissection in the treatment of squamous cell carcinoma of the lower lip: 20 years’ experience at a Tertiary Center. J. Cranio-Maxillofac. Surg. 2016, 44, 1404–1407. [Google Scholar] [CrossRef]
- Eskiizmir, G.; Ozgur, E.; Karaca, G.; Temiz, P.; Yanar, N.H.; Ozyurt, B.C. Stage is a prognostic factor for surgically treated patients with early-stage lip cancer for whom a ‘wait and see’ policy in terms of neck status has been implemented. J. Laryngol. Otol. 2017, 131, 889–894. [Google Scholar] [CrossRef]
- Altinyollar, H.; Berberoğlu, U.; Celen, O. Lymphatic mapping and sentinel lymph node biopsy in squamous cell carcinoma of the lower lip. Eur. J. Surg. Oncol. 2002, 28, 72–74. [Google Scholar] [CrossRef]
- Khalil, H.H.; Elaffandi, A.H.; Afifi, A.; Alsayed, Y.; Mahboub, T.; El-Refaie, K.M. Sentinel lymph node biopsy (SLNB) in management of N0 stage T1-T2 lip cancer as a « same day » procedure. Oral Oncol. 2008, 44, 608–612. [Google Scholar] [CrossRef] [PubMed]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Characteristics | n/Median | Min–Max/% | |
|---|---|---|---|
| Age | 73 | 35–92 | |
| Gender | |||
| F | 9 | 23.7 | |
| M | 29 | 76.3 | |
| Performance status | |||
| 0 | 17 | 44.8 | |
| 1 | 20 | 52.6 | |
| 2 | 0 | 0 | |
| 3 | 1 | 2.6 | |
| Tobacco | |||
| 0 | 17 | 44.7 | |
| withdrawn | 16 | 42.1 | |
| active | 5 | 13.2 | |
| Histology | |||
| squamous cell carcinoma | 37 | 97 | |
| polymorph adenocarcinoma | 1 | 2.6 | |
| Tumor localization | |||
| lower lip | 28 | 73.7 | |
| upper lip | 8 | 28 | |
| lip and cheek | 2 | 5.3 | |
| T | |||
| 1 | 14 | 36.9 | |
| 2 | 16 | 42.1 | |
| 3 | 7 | 18.4 | |
| 4 | 1 | 2.6 | |
| n | |||
| 0 | 34 | 89.5 | |
| 1 | 2 | 5.3 | |
| 2 | 2 | 5.3 | |
| M | |||
| 0 | 38 | 100 | |
| 1 | 0 | 0 | |
| Treatment Data | Median | Min–Max | n |
|---|---|---|---|
| Catheters number | 4 | 15–2 | 38 |
| Plans number | 2 | 4–1 | 37 |
| Catheters spacing | 13 | 18–9 | 37 |
| Length activation | 65 | 50–120 | 38 |
| Dose/pulse (cGy) | 42 | 40–50 | 38 |
| Pulse number | 166.5 | 120–179 | 38 |
| Total dose (Gy) | 70.14 | 60–85 | 38 |
| V 100% (cm3) | 16.49 | 4.7–47.8 | 34 |
| V 150% (cm3) | 4.45 | 2.3–14.1 | 33 |
| V 200% (cm3) | 2.1 | 1–5.8 | 33 |
| TRAK (mGy) | 1.82 | 0.77–3.36 | 37 |
| mandible D2cc (Gy) | 28.6 | 7.2–49.4 | 31 |
| mandible D0.1cc (Gy) | 42.6 | 9.1–82.8 | 31 |
| mandible D0.01cc (Gy) | 48.4 | 11.8–101 | 31 |
| Toxicity Data (Grade) | n | % | |
|---|---|---|---|
| Radiomucitis | |||
| G0 | 0 | 0% | |
| G1 | 2 | 6% | |
| G2 | 19 | 53% | |
| G3 | 15 | 42% | |
| Odynophagia | |||
| G0 | 20 | 56 | |
| G1 | 13 | 36 | |
| G2 | 3 | 8 | |
| G3 | 0 | 0 | |
| Fibrosis | |||
| G0 | 15 | 42 | |
| G1 | 18 | 50 | |
| G2 | 3 | 8 | |
| G3 | 0 | 0 | |
| Chronic pain | |||
| G0 | 32 | 89 | |
| G1 | 3 | 8 | |
| G2 | 1 | 3 | |
| G3 | 0 | 0 | |
| Depigmentation | |||
| G0 | 19 | 53 | |
| G1 | 17 | 47 | |
| G2 | 0 | 0 | |
| Quality of Life Assessment | n/Median | %/Min–Max | |
|---|---|---|---|
| Would You Recommend the Treatment? | |||
| 0 (not at all) | 0 | 0% | |
| 1 | 0 | 0% | |
| 2 | 0 | 0% | |
| 3-neutral | 0 | 0% | |
| 4 | 2 | 18% | |
| 5 (definitively) | 9 | 82% | |
| FACT H&N scores (range) | |||
| Physical well-being score (0–28) | 25 | 15–27 | |
| Social/family well-being score (0–28) | 26.8 | 1.2–28 | |
| Emotional well-being score (0–24) | 19 | 14–24 | |
| Functional well-being score (0–28) | 23 | 11–28 | |
| Head and Neck cancer subscale (0–40) | 36 | 25–40 | |
| FACT H&N Trial Outcome Index (0–96) | 84 | 58.2–94 | |
| FACT H&N total score (0–148) | 127 | 75.4–146 | |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
El Ayachy, R.; Sun, R.; Ka, K.; Laville, A.; Duhamel, A.-S.; Tailleur, A.; Dumas, I.; Bockel, S.; Espenel, S.; Blanchard, P.; et al. Pulsed Dose Rate Brachytherapy of Lip Carcinoma: Clinical Outcome and Quality of Life Analysis. Cancers 2021, 13, 1387. https://doi.org/10.3390/cancers13061387
El Ayachy R, Sun R, Ka K, Laville A, Duhamel A-S, Tailleur A, Dumas I, Bockel S, Espenel S, Blanchard P, et al. Pulsed Dose Rate Brachytherapy of Lip Carcinoma: Clinical Outcome and Quality of Life Analysis. Cancers. 2021; 13(6):1387. https://doi.org/10.3390/cancers13061387
Chicago/Turabian StyleEl Ayachy, Radouane, Roger Sun, Kanta Ka, Adrien Laville, Anne-Sophie Duhamel, Anne Tailleur, Isabelle Dumas, Sophie Bockel, Sophie Espenel, Pierre Blanchard, and et al. 2021. "Pulsed Dose Rate Brachytherapy of Lip Carcinoma: Clinical Outcome and Quality of Life Analysis" Cancers 13, no. 6: 1387. https://doi.org/10.3390/cancers13061387