
Preoperative Repetitive Navigated TMS and Functional White Matter Tractography in a Bilingual Patient with a Brain Tumor in Wernike Area

 , , and
, , and
Abstract
:1. Introduction
2. Case Presentation
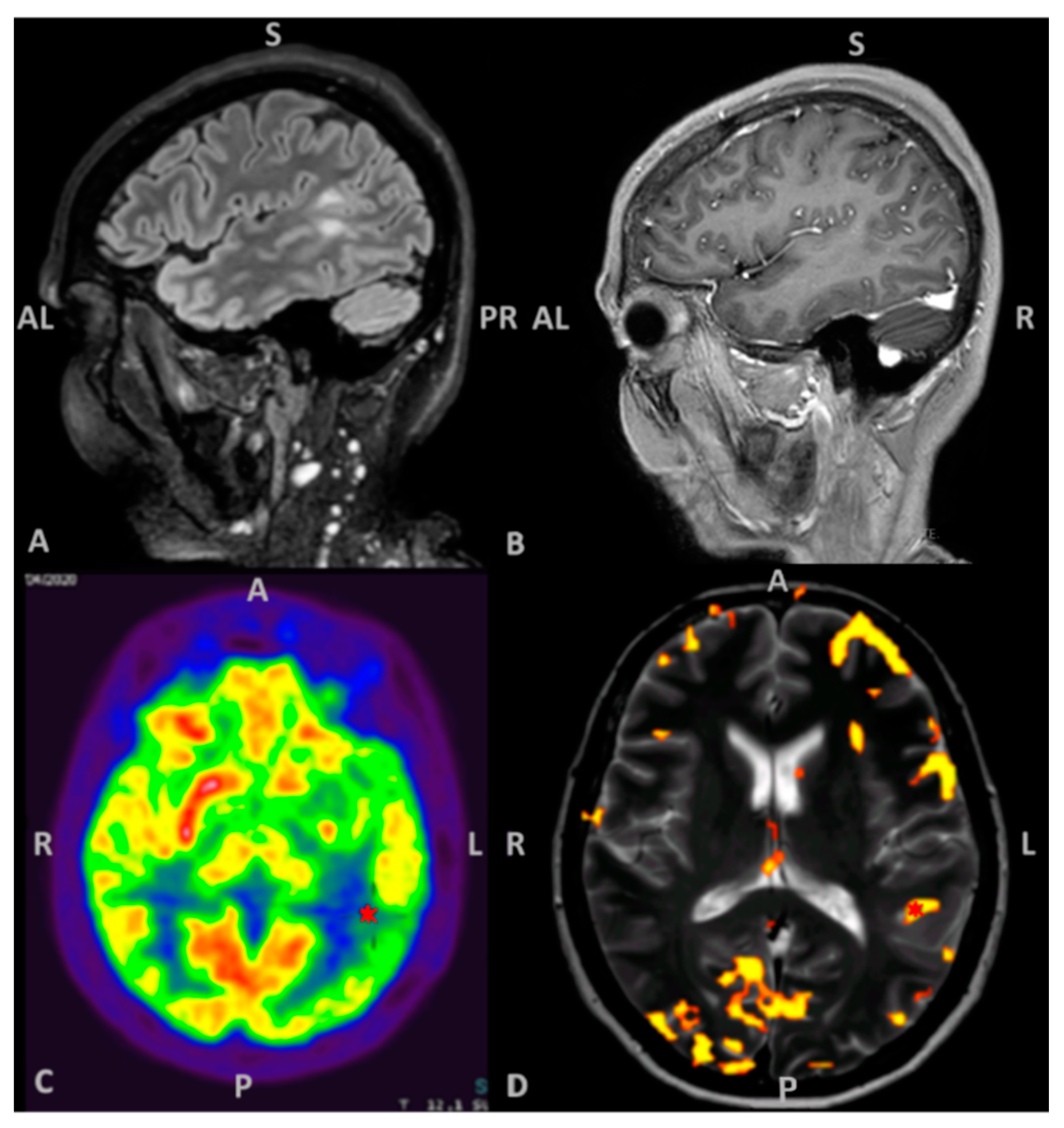
2.1. Patient Information, Clinical and Radiological Findings
2.2. Neuropsychological Evaluation
2.3. Patient’s Informed Consent
2.4. MRI Acquisition
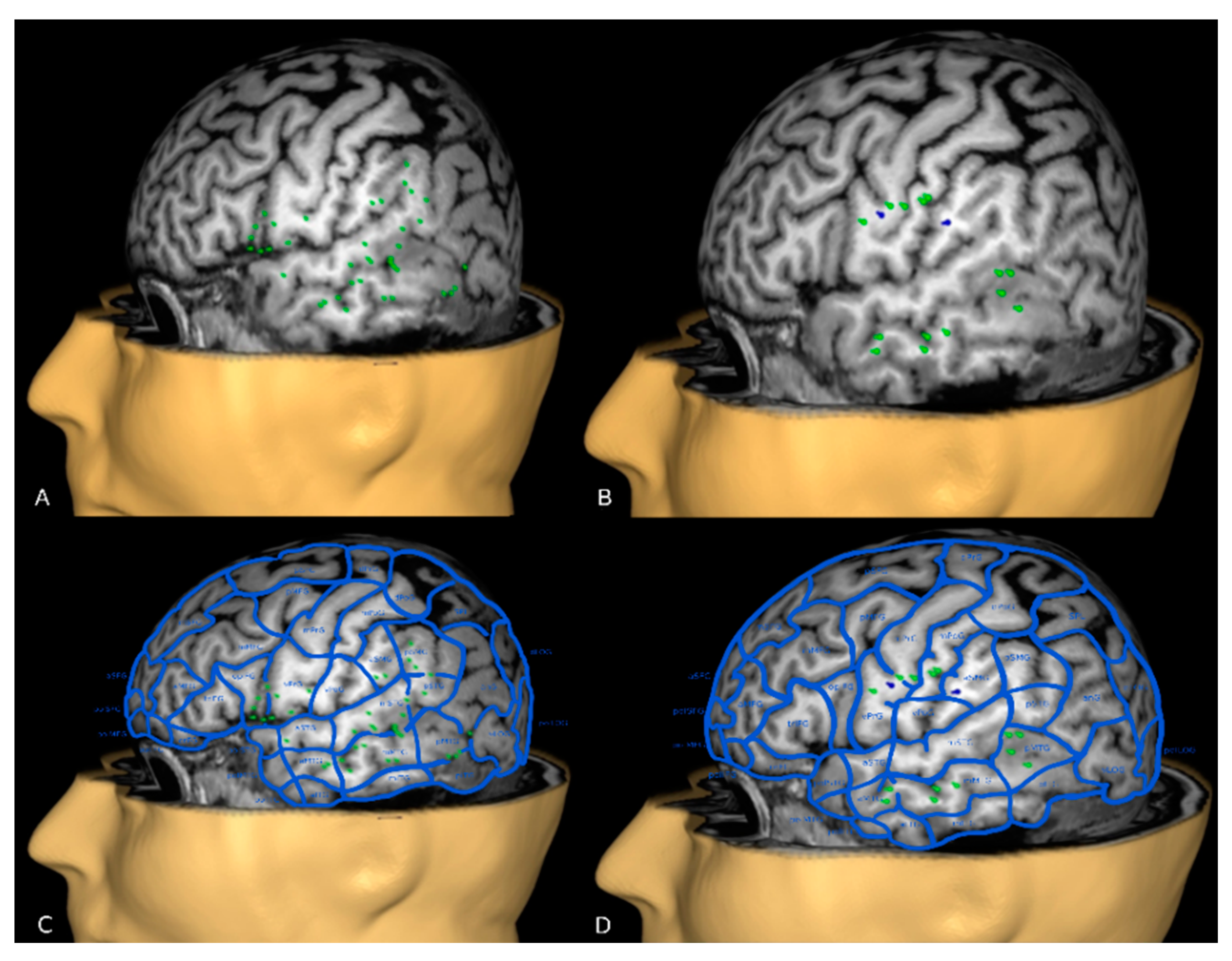
2.5. nTMS Language Cortical Mapping and Off-Line Analysis
2.6. nTMS Based DTI-FT of Language Pathway
2.7. Presurgical Planning
2.8. Surgical Intervention and Neuropsychological Follow Up
3. Discussion
4. Conclusions
Author Contributions
Funding
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Ethical Approval
Abbreviations
References
- Tarapore, P.E.; Findlay, A.M.; Honma, S.M.; Mizuiri, D.; Houde, J.F.; Berger, M.S.; Nagarajan, S.S. Language mapping with navigated repetitive TMS: Proof of technique and validation. Neuroimage 2013, 82, 260–272. [Google Scholar] [CrossRef] [Green Version]
- Picht, T.; Krieg, S.M.; Sollmann, N.; Rösler, J.; Niraula, B.; Neuvonen, T.; Savolainen, P.; Lioumis, P.; Mäkelä, J.P.; Deletis, V.; et al. A comparison of language mapping by preoperative navigated transcranial magnetic stimulation and direct cortical stimulation during awake surgery. Neurosurgery 2013, 72, 808–819. [Google Scholar] [CrossRef] [Green Version]
- Ille, S.; Sollmann, N.; Hauck, T.; Maurer, S.; Tanigawa, N.; Obermueller, T.; Negwer, C.; Droese, D.; Boeckh-Behrens, T.; Meyer, B.; et al. Impairment of preoperative language mapping by lesion location: A functional magnetic resonance imaging, navigated transcranial magnetic stimulation, and direct cortical stimulation study. J. Neurosurg. 2015, 123, 314–324. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Babajani-Feremi, A.; Narayana, S.; Rezaie, R.; Choudhri, A.F.; Fulton, S.P.; Boop, F.A.; Wheless, G.W.; Papanicolaou, A.C. Language mapping using high gamma electrocorticography, fMRI, and TMS versus electrocortical stimulation. Clin. Neurophysiol. 2016, 127, 1822–1836. [Google Scholar] [CrossRef] [PubMed]
- Lehtinen, H.; Mäkelä, J.P.; Mäkelä, T.; Lioumis, P.; Metsähonkala, L.; Hokkanen, L.; Wilenius, J.; Gaily, E. Language mapping with navigated transcranial magnetic stimulation in pediatric and adult patients undergoing epilepsy surgery: Comparison with extraoperative direct cortical stimulation. Epilepsia Open 2018, 3, 224–235. [Google Scholar] [CrossRef] [Green Version]
- Jeltema, H.R.; Ohlerth, A.K.; de Wit, A.; Wagemakers, M.; Rofes, A.; Bastiaanse, R.; Drost, G. Comparing navigated transcranial magnetic stimulation mapping and “gold standard” direct cortical stimulation mapping in neurosurgery: A systematic review. Neurosurg Rev. 2020. Online ahead of print. [Google Scholar] [CrossRef]
- Senova, S.; Lefaucheur, J.P.; Brugières, P.; Ayache, S.S.; Tazi, S.; Bapst, B.; Abhay, K.; Langeron, O.; Edakawa, K.; Palfi, S.; et al. Case Report: Multimodal Functional and Structural Evaluation Combining Pre-operative nTMS Mapping and Neuroimaging With Intraoperative CT-Scan and Brain Shift Correction for Brain Tumor Surgical Resection. Front. Hum. Neurosci. 2021, 15, 646268. [Google Scholar] [CrossRef] [PubMed]
- Haddad, A.F.; Young, J.S.; Berger, M.S.; Tarapore, P.E. Preoperative Applications of Navigated Transcranial Magnetic Stimulation. Front. Neurol. 2021, 11, 628903. [Google Scholar] [CrossRef] [PubMed]
- Hazem, S.R.; Awan, M.; Lavrador, J.P.; Patel, S.; Wren, H.M.; Lucena, O.; Semedo, C.; Irzan, H.; Melbourne, A.; Ourselin, S.; et al. Middle Frontal Gyrus and Area 55b: Perioperative Mapping and Language Outcomes. Front. Neurol. 2021, 12, 646075. [Google Scholar] [CrossRef]
- Sollmann, N.; Zhang, H.; Schramm, S.; Ille, S.; Negwer, C.; Kreiser, K.; Meyer, B.; Krieg, S.M. Function-specific Tractography of Language Pathways Based on nTMS Mapping in Patients with Supratentorial Lesions. Clin. Neuroradiol. 2020, 30, 123–135. [Google Scholar] [CrossRef] [PubMed]
- Sollmann, N.; Negwer, C.; Ille, S.; Maurer, S.; Hauck, T.; Kirschke, J.S.; Ringel, F.; Meyer, B.; Krieg, S.M. Feasibility of nTMS-based DTI fiber tracking of language pathways in neurosurgical patients using a fractional anisotropy threshold. J. Neurosci. Methods 2016, 267, 45–54. [Google Scholar] [CrossRef]
- Sollmann, N.; Ille, S.; Hauck, T.; Maurer, S.; Negwer, C.; Zimmer, C.; Ringel, F.; Meyer, B.; Krieg, S.M. The impact of preoperative language mapping by repetitive navigated transcranial magnetic stimulation on the clinical course of brain tumor patients. BMC Cancer 2015, 15, 261. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Raffa, G.; Bährend, I.; Schneider, H.; Faust, K.; Germanò, A.; Vajkoczy, P.; Picht, T. A novel technique for region and linguistic specific nTMS-based DTI fiber tracking of language pathways in brain tumor patients. Front. Neurosci. 2016, 11, 552. [Google Scholar] [CrossRef] [PubMed]
- Raffa, G.; Quattropani, M.C.; Scibilia, A.; Conti, A.; Angileri, F.F.; Esposito, F.; Sindorio, C.; Cardali, S.M.; Germanò, A.; Tomasello, F. Surgery of language-eloquent tumors in patients not eligible for awake surgery: The impact of a protocol based on navigated transcranial magnetic stimulation on presurgical planning and language outcome, with evidence of tumor-induced intra-hemispheric plasticity. Clin. Neurol. Neurosurg. 2018, 168, 127–139. [Google Scholar] [CrossRef] [PubMed]
- Sollmann, N.; Zhang, H.; Fratini, A.; Wildschuetz, N.; Ille, S.; Schröder, A.; Zimmer, C.; Meyer, B.; Krieg, S.M. Risk assessment by presurgical tractography using navigated tms maps in patients with highly motor-or language-eloquent brain tumors. BMC Cancer 2020, 12, 1124. [Google Scholar] [CrossRef] [PubMed]
- Połczyńska, M.M.; Bookheimer, S.Y. Factors modifying the amount of neuroanatomical overlap between languages in Bilinguals—a systematic review of neurosurgical language mapping studies. Brain Sci. 2020, 10, 983. [Google Scholar] [CrossRef] [PubMed]
- Hämäläinen, S.; Mäkelä, N.; Sairanen, V.; Lehtonen, M.; Kujala, T.; Leminen, A. TMS uncovers details about sub-regional language-specific processing networks in early bilinguals. Neuroimage 2018, 171, 209–221. [Google Scholar] [CrossRef] [Green Version]
- Tussis, L.; Sollmann, N.; Boeckh-Behrens, T.; Meyer, B.; Krieg, S.M. The cortical distribution of first and second language in the right hemisphere of bilinguals—An exploratory study by repetitive navigated transcranial magnetic stimulation. Brain Imaging Behav. 2020, 14, 1034–1049. [Google Scholar] [CrossRef] [PubMed]
- Demeyere, N.; Riddoch, M.J.; Slavkova, E.D.; Bickerton, W.-L.; Humphreys, G.W. The Oxford Cognitive Screen (OCS): Validation of a stroke-specific short cognitive screening tool. Psychol. Assess. 2015, 27, 883–894. [Google Scholar] [CrossRef]
- Mancuso, M.; Varalta, V.; Sardella, L.; Capitani, D.; Zoccolotti, P.; Antonucci, G. Italian normative data for a stroke specific cognitive screening tool: The Oxford Cognitive Screen (OCS). Neurol. Sci. 2016, 37, 1713–1721. [Google Scholar] [CrossRef]
- Mondini, S.; Mapelli, D.; Vestri, A.; Arcara, G.; Bisacchi, P.S. Esame Neuropsicologico Breve—Una Batteria di Test per lo Screening Neuropsicologico; Raffaello Cortina Editore: Milano, Italy, 2011. [Google Scholar]
- Monaco, M.; Costa, A.; Caltagirone, C.; Carlesimo, G.A. Forward and backward span for verbal and visuo-spatial data: Standardization and normative data from an Italian adult population. Neurol. Sci. 2013, 34, 749–754. [Google Scholar] [CrossRef]
- Kaplan, E.F.; Goodglass, H.; Weintraub, S. The Boston Naming Test: The Experimental Edition, 2nd ed.; Lea & Fabiger: Philadelphia, PA, USA, 1983. [Google Scholar]
- Capasso, R.; Miceli, M. Esame Neuropsicologico per l’Afasia, 1st ed.; Springer: Mailand, Italy, 2001. [Google Scholar]
- Krieg, S.M.; Lioumis, P.; Mäkelä, J.P.; Wilenius, J.; Karhu, J.; Hannula, H.; Savolainen, P.; Lucas, C.W.; Seidel, K.; Laakso, A.; et al. Protocol for motor and language mapping by navigated TMS in patients and healthy volunteers; workshop report. Acta Neurochir. 2017, 159, 1187–1195. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Krieg, S.M.; Tarapore, P.E.; Picht, T.; Tanigawa, N.; Houde, J.; Sollmann, N.; Meyer, B.; Vajkoczy, P.; Berger, M.S.; Ringel, F.; et al. Optimal timing of pulse onset for language mapping with navigated repetitive transcranial magnetic stimulation. Neuroimage 2014, 15, 219–236. [Google Scholar] [CrossRef] [PubMed]
- Mandonnet, E.; Sarubbo, S.; Duffau, H. Proposal of an optimized strategy for intraoperative testing of speech and language during awake mapping. Neurosurg. Rev. 2017, 40, 29–35. [Google Scholar] [CrossRef] [PubMed]
- Corina, D.P.; Loudermilk, B.C.; Detwiler, L.; Martin, R.F.; Brinkley, J.F.; Ojemann, G. Analysis of naming errors during cortical stimulation mapping: Implications for models of language representation. Brain Lang. 2010, 115, 101–112. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Corina, D.P.; Gibson, E.K.; Martin, R.; Poliakov, A.; Brinkley, J.; Ojemann, G.A. Dissociation of action and object naming: Evidence from cortical stimulation mapping. Hum. Brain. Mapp. 2005, 159, 1187–1195. [Google Scholar] [CrossRef]
- Fekonja, L.; Wang, Z.; Bährend, I.; Rosenstock, T.; Rösler, J.; Wallmeroth, L.; Vajkoczy, P.; Picht, T. Manual for clinical language tractography. Acta Neurochir. 2019, 161, 1125–1137. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Machetanz, K.; Trakolis, L.; Leão, M.T.; Liebsch, M.; Mounts, K.; Bender, B.; Ernemann, U.; Gharabaghi, A.; Tatagiba, M.; Naros, G. Neurophysiology-Driven Parameter Selection in nTMS-Based DTI Tractography: A Multidimensional Mathematical Model. Front. Neurosci. 2019, 13, 1–10. [Google Scholar] [CrossRef] [Green Version]
- Catani, M.; Howard, R.J.; Pajevic, S.; Jones, D.K. Virtual in Vivo interactive dissection of white matter fasciculi in the human brain. Neuroimage 2002, 17, 77–94. [Google Scholar] [CrossRef] [Green Version]
- Catani, M.; Thiebaut de Schotten, M. A diffusion tensor imaging tractography atlas for virtual in vivo dissections. Cortex 2008, 44, 1105–1132. [Google Scholar] [CrossRef]
- Kamali, A.; Flanders, A.E.; Brody, J.; Hunter, J.V.; Hasan, K.M. Tracing superior longitudinal fasciculus connectivity in the human brain using high resolution diffusion tensor tractography. Brain. Struct. Funct. 2014, 219, 269–281. [Google Scholar] [CrossRef]
- Brat, D.J.; Aldape, K.; Colman, H.; Figrarella-Branger, D.; Fuller, G.N.; Giannini, C.; Holland, E.C.; Jenkins, R.B.; Kleinschmidt-DeMasters, B.; Komori, T.; et al. cIMPACT-NOW update 5: Recommended grading criteria and terminologies for IDH-mutant astrocytomas. Acta Neuropathol. 2020, 139, 603–608. [Google Scholar] [CrossRef]
- Sanai, N.; Berger, M.S. Intraoperative stimulation techniques for functional pathway preservation and glioma resection. Neurosurg. Focus. 2010, 28. [Google Scholar] [CrossRef]
- Sanai, N.; Mirzadeh, Z.; Berger, M.S. Functional Outcome after Language Mapping for Glioma Resection. N. Engl. J. Med. 2008, 358, 118–127. [Google Scholar] [CrossRef]
- De Benedictis, A.; Moritz-Gasser, S.; Duffau, H. Awake mapping optimizes the extent of resection for low-grade gliomas in eloquent areas. Neurosurgery 2010, 66, 1074–1084. [Google Scholar] [CrossRef]
- Kayama, T. The Guidelines for Awake CraniotomyGuidelines Committee of The Japan Awake Surgery Conference. Neurol. Med. Chir. 2012, 52, 119–141. [Google Scholar] [CrossRef] [Green Version]
- Fujiwara, N.; Sakatani, K.; Katayama, Y.; Murata, Y.; Hoshino, T.; Fukaya, C.; Yamamoto, T. Evoked-cerebral blood oxygenation changes in false-negative activations in BOLD contrast functional MRI of patients with brain tumors. Neuroimage 2004, 21, 1464–1471. [Google Scholar] [CrossRef]
- Aubert, A.; Costalat, R.; Duffau, H.; Benali, H. Modeling of Pathophysiological Coupling between Brain Electrical Activation, Energy Metabolism and Hemodynamics: Insights for the Interpretation of Intracerebral Tumor Imaging. Acta Biotheor. 2002, 50, 281–295. [Google Scholar] [CrossRef] [PubMed]
- Giussani, C.; Roux, F.-E.; Ojemann, J.; Pietro, S.E.; Pirillo, D.; Papagno, C. Is Preoperative Functional Magnetic Resonance Imaging Reliable for Language Areas Mapping in Brain Tumor Surgery? Review of Language Functional Magnetic Resonance Imaging and Direct Cortical Stimulation Correlation Studies. Neurosurgery 2010, 66, 113–120. [Google Scholar] [CrossRef] [PubMed]
- Ulmer, J.L.; Hacein-Bey, L.; Mathews, V.P.; Mueller, W.M.; DeYoe, E.A.; Prost, R.W.; Meyer, G.A.; Krouwer, H.G.; Schmainda, K.M. Lesion-induced Pseudo-dominance at Functional Magnetic Resonance Imaging: Implications for Preoperative Assessments. Neurosurgery 2004, 55, 569–579. [Google Scholar] [CrossRef] [PubMed]
- Fitzgerald, D.B.; Cosgrove, G.R.; Ronner, S.; Jiang, H.; Buchbinder, B.R.; Belliveau, J.W.; Rosen, B.R.; Benson, R.R. Location of Language in the Cortex: A Comparison between Functional MR Imaging and Electrocortical Stimulation. AJNR Am. J. Neuroradiol. 1997, 18, 1529–1539. [Google Scholar] [PubMed]
- Roux, F.E.; Boulanouar, K.; Lotterie, J.A.; Mejdoubi, M.; LeSage, J.P.; Berry, I. Language functional magnetic resonance imaging in preoperative assessment of language areas: Correlation with direct cortical stimulation. Neurosurgery 2003, 52, 1335–1347. [Google Scholar] [CrossRef] [Green Version]
- Ottenhausen, M.; Krieg, S.M.; Meyer, B.; Ringel, F. Functional preoperative and intraoperative mapping and monitoring: Increasing safety and efficacy in glioma surgery. Neurosurg. Focus. 2015, 38, E3. [Google Scholar] [CrossRef] [PubMed]
- Rofes, A.; Mandonnet, E.; de Aguiar, V.; Rapp, B.; Tsapkini, K.; Miceli, G. Language processing from the perspective of electrical stimulation mapping. Cogn Neuropsychol. 2019, 36, 117–139. [Google Scholar] [CrossRef] [PubMed]
- Hickok, G.; Poeppel, D. Dorsal and ventral streams: A framework for understanding aspects of the functional anatomy of language. Cognition 2004, 92, 67–99. [Google Scholar] [CrossRef] [PubMed]
- Bährend, I.; Muench, M.R.; Schneider, H.; Moshourab, R.; Dreyer, F.R.; Vajkoczy, P.; Picht, T.; Faust, K. Incidence and linguistic quality of speech errors: A comparison of preoperative transcranial magnetic stimulation and intraoperative direct cortex stimulation. J. Neurosurg. 2020, 29, 1–10. [Google Scholar] [CrossRef]
- Rösler, J.; Niraula, B.; Strack, V.; Zdunczyk, A.; Schilt, S.; Savolainen, P.; Lioumis, P.; Mäkelä, P.; Vajkoczy, P.; Frey, D.; et al. Language mapping in healthy volunteers and brain tumor patients with a novel navigated TMS system: Evidence of tumor-induced plasticity. Clin. Neurophysiol. 2014, 125, 526–536. [Google Scholar] [CrossRef]
- Krieg, S.M.; Sollmann, N.; Hauck, T.; Ille, S.; Foerschler, A.; Meyer, B.; Ringel, F. Functional Language Shift to the Right Hemisphere in Patients with Language-Eloquent Brain Tumors. PLoS ONE 2013, 17, e75403. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Duffau, H. Brain plasticity and tumors. Adv. Tech. Stand. Neurosurg. 2008, 33, 3–33. [Google Scholar] [CrossRef]
- Krieg, S.M.; Sollmann, N.; Hauck, T.; Ille, S.; Meyer, B.; Ringel, F. Repeated mapping of cortical language sites by preoperative navigated transcranial magnetic stimulation compared to repeated intraoperative DCS mapping in awake craniotomy. BMC Neurosci. 2014, 159, 1187–1195. [Google Scholar] [CrossRef] [Green Version]
- Lioumis, P.; Zhdanov, A.; Mäkelä, N.; Lehtinen, H.; Wilenius, J.; Neuvonen, T.; Hannula, H.; Deletis, V.; Picht, T.; Mäkelä, J.P. A novel approach for documenting naming errors induced by navigated transcranial magnetic stimulation. J. Neurosci. Methods 2012, 15, 349–354. [Google Scholar] [CrossRef]
- Schuhmann, T.; Schiller, N.O.; Goebel, R.; Sack, A.T. Speaking of which: Dissecting the neurocognitive network of language production in picture naming. Cereb Cortex 2012, 22, 701–709. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Schwarzer, V.; Bährend, I.; Rosenstock, T.; Dreyer, F.R.; Vajkoczy, P.; Picht, T. Aphasia and cognitive impairment decrease the reliability of rnTMS language mapping. Acta Neurochir. 2018, 160, 343–356. [Google Scholar] [CrossRef] [PubMed]
- Hamed, S.A.; Tohamy, A.M.; Mohamed, K.O.; el Mageed Abd el Zaher, M.A. The Effect of Epilepsy and Antiepileptic Drugs on Cortical Motor Excitability in Patients With Temporal Lobe Epilepsy. Clin. Neuropharmacol. 2020, 43, 175–184. [Google Scholar] [CrossRef] [PubMed]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Assessment | Pre-Operative | Post-Operative | Follow-Up 1 Month | Follow-Up 4 Months | ||||
|---|---|---|---|---|---|---|---|---|
| Test | CS | Performance | CS | Performance | CS | Performance | CS | Performance |
| GLOBAL COGNITIVE FUNCTIONS | ||||||||
| Oxford Cognitive Screen (OCS) | ||||||||
| Denomination | 3 | Impaired | 3 | Impaired | 3 | Impaired | 4 | Normal |
| Semantics | 3 | Normal | 3 | Normal | 3 | Normal | 3 | Normal |
| Orientation | 4 | Normal | 4 | Normal | 4 | Normal | 4 | Normal |
| Visual field | 4 | Normal | 4 | Normal | 4 | Normal | 4 | Normal |
| Reading | 15 | Normal | 13 | Impaired | 15 | Normal | 15 | Normal |
| Number writing | 3 | Normal | 2 | Impaired | 3 | Normal | 3 | Normal |
| Calculation | 3 | Borderline | 3 | Borderline | 4 | Normal | 3 | Normal |
| Visual search | 47 | Normal | 47 | Normal | 46 | Normal | 49 | Normal |
| egocentric neglect | −1 | Normal | 1 | Normal | 2 | Normal | 1 | Normal |
| allocentric neglect | 0 | Normal | 0 | Normal | 0 | Normal | 0 | Normal |
| Imitation | ||||||||
| Right hand | 11 | Normal | 8 | Impaired | 12 | Normal | 12 | Normal |
| Left hand | 12 | Normal | 12 | Normal | 12 | Normal | 12 | Normal |
| Memory | ||||||||
| Verbal | 3 | Normal | 3 | Normal | 2 | Impaired | 3 | Normal |
| Episodic | 4 | Normal | 4 | Normal | 4 | Normal | 4 | Normal |
| Executive functions | −1 | Normal | −2 | Normal | 0 | Normal | 0 | Normal |
| LANGUAGE | ||||||||
| Boston Naming Test (15 items) | 5 | Impaired | 3 | Impaired | 6 | Impaired | 6 | Impaired |
| E.N.P.A. | ||||||||
| Verbal comprehension (words) | 18.4 | Normal | 18.4 | Normal | 18.4 | Normal | 20 | Normal |
| Verbal comprehension (sentences) | 14 | Normal | 14 | Normal | 14 | Normal | 14 | Normal |
| Repetition (words) | 10 | Normal | 10 | Normal | 10 | Normal | 10 | Normal |
| Repetition (nonwords) | 5 | Normal | 5 | Normal | 5 | Normal | 5 | Normal |
| Phonemic Fluency (Mondini, 2011) [21] | 7.7 | Impaired | 1.7 | Impaired | 1.7 | Impaired | 4.3 | Impaired |
| ATTENTION | ||||||||
| Trail Making Test | ||||||||
| A | 26″ | Normal | 37″ | Normal | 51″ | Normal | 46″ | Normal |
| B | 167″ | Impaired | 167″ | Impaired | 156″ | Impaired | 133″ | Normal |
| MEMORY | ||||||||
| Digit span | ||||||||
| Forward | 4.75 | Normal | 2.75 | Impaired | 4.75 | Normal | 4.75 | Normal |
| Backward | 3.71 | Normal | 0 | Impaired | 3.71 | Normal | 3.79 | Normal |
| Corsi Test | ||||||||
| Forward | 6.74 | Normal | 5.74 | Normal | 4.74 | Normal | 3.81 | Normal |
| Backward | 5.67 | Normal | 5.67 | Normal | 5.67 | Normal | 3.79 | Normal |
| Prose Memory | ||||||||
| Immediate | 9 | Normal | 5 | Impaired | 12 | Normal | 10 | Normal |
| Delayed | 12 | Normal | NE | Impaired | 15 | Normal | 17 | Normal |
| Memory Interference | ||||||||
| 10 s | 8 | Normal | 5 | Normal | 8 | Normal | 8 | Normal |
| 30 s | 7 | Normal | 6 | Normal | 7 | Normal | 8 | Normal |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Baro, V.; Caliri, S.; Sartori, L.; Facchini, S.; Guarrera, B.; Zangrossi, P.; Anglani, M.; Denaro, L.; d’Avella, D.; Ferreri, F.; et al. Preoperative Repetitive Navigated TMS and Functional White Matter Tractography in a Bilingual Patient with a Brain Tumor in Wernike Area. Brain Sci. 2021, 11, 557. https://doi.org/10.3390/brainsci11050557
Baro V, Caliri S, Sartori L, Facchini S, Guarrera B, Zangrossi P, Anglani M, Denaro L, d’Avella D, Ferreri F, et al. Preoperative Repetitive Navigated TMS and Functional White Matter Tractography in a Bilingual Patient with a Brain Tumor in Wernike Area. Brain Sciences. 2021; 11(5):557. https://doi.org/10.3390/brainsci11050557
Chicago/Turabian StyleBaro, Valentina, Samuel Caliri, Luca Sartori, Silvia Facchini, Brando Guarrera, Pietro Zangrossi, Mariagiulia Anglani, Luca Denaro, Domenico d’Avella, Florinda Ferreri, and et al. 2021. "Preoperative Repetitive Navigated TMS and Functional White Matter Tractography in a Bilingual Patient with a Brain Tumor in Wernike Area" Brain Sciences 11, no. 5: 557. https://doi.org/10.3390/brainsci11050557