
Ultrasound Technologies and the Diagnosis of Giant Cell Arteritis

 , , and
, , and 
Abstract
:1. Introduction-Giant Cell Arteritis (GCA)
- An arteritis usually interesting the aorta and its major branches, especially the branches of the external carotid and vertebral arteries (the temporal artery being often affected);
- Usually patients with an age greater than 50 years at the appearance of clinical disease;
- Frequently associated with polymyalgia rheumatica, manifested by systemic symptoms, represented by fever, pain in the shoulders and hips, malaise, weight loss;
- New onset of a medium temporal headache;
- A clinically modified temporal artery (consisting in tenderness of the vessel or reduced temporal artery pulse), associated with scalp tenderness.
- Claudication of the jaw on mastication or tongue on mastication and on deglutition.
- An augmented erythrocyte sedimentation rate, more than 50 mm/h;
2. Introduction-Ultrasonography (US)
2.1. Ultrasonography Overview
- Brightness mode (B-mode) Imaging. It uses a two-dimensional view of a portion of tissue because ultrasound signals are reflected from the target. The power of the reflected signal (named echo) is grayscale coded, being represented as a much or less bright dot, while the anatomical situation of distinct echoes depends on the depth of the insonated structure [18].
- The duplex image. It combines a B-mode image (which analyses the topography of the vessels) with pulse-wave (PW) Doppler (which focuses on flow velocities assessment). The two-dimensional B-mode view suggests that portion inside the vessel wherein a Doppler sample volume must be disposed and wherein the velocities are measured.
- c.
- Color Doppler flow imaging. This technique measures the average frequency change in each sample volume. It associates a color flow map (representing the color-coded velocity information) with a B-mode image.
- d.
- Power Doppler mode. It uses the strength of the return Doppler signal instead of the frequency shift. Signal strength is displayed as a color map superimposed on a B-mode image. Since Doppler power is determined primarily by the volume rather than the velocity of the moving blood, power Doppler imaging is free from aliasing artifacts and is much more sensitive to detect flow, especially in low-flow regions. Unfortunately, it does not include data on the direction or speed of the flow [18].
2.2. Systemic Arteries
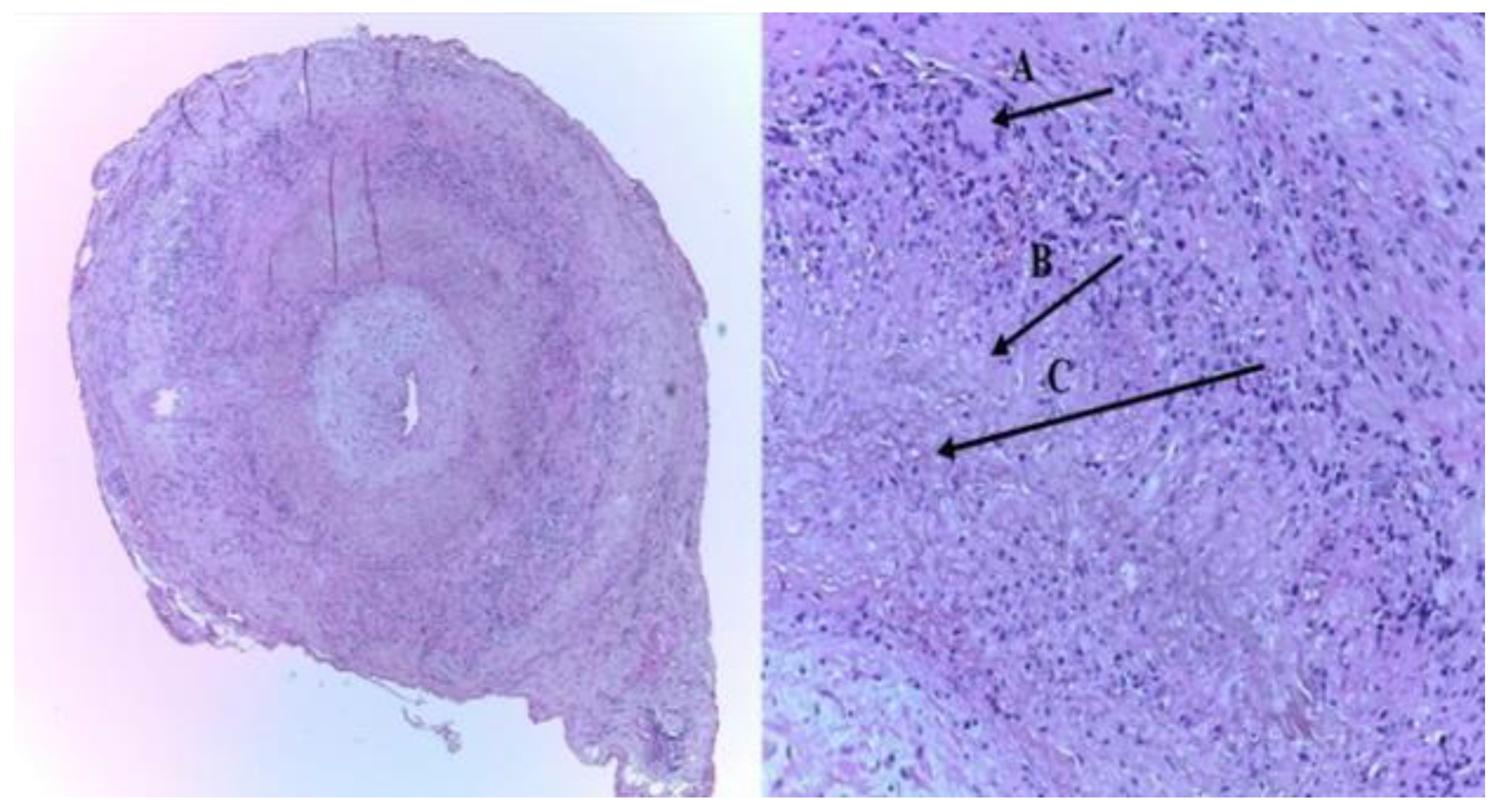
2.2.1. The Structure of the Wall of Systemic Arteries
2.2.2. Measures in the Arterial Wall
2.2.3. Carotid Intima-Media Thickness (cIMT)
2.2.4. Carotid Plaque (CP)
2.3. Advantages of Ultrasonography (US)
3. Ultrasonography (US) in Giant Cell Arteritis (GCA)
3.1. Background
- Other medium-sized arteries (branches of the ECAs): the internal maxillary artery (claudication of the jaw on mastication), the renine artery (claudication of the tongue on mastication or on deglutition), the facial, and the occipital arteries,
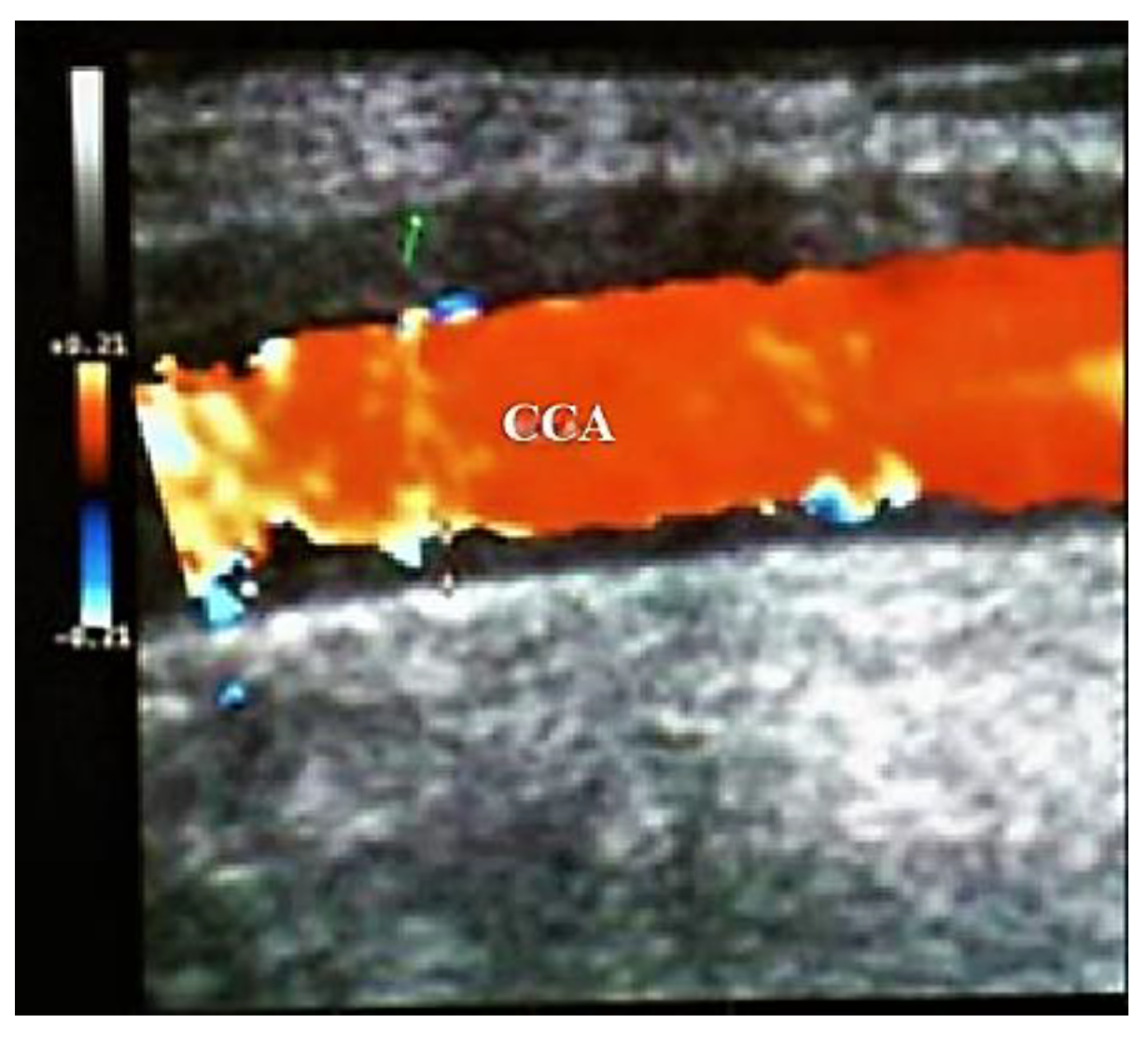
- Large size arteries: the common carotid arteries (CCAs), the ECAs, the internal carotid arteries (ICA’s), the vertebral, the subclavian, and the axillary arteries,
3.2. Ultrasonography (US) of the Temporal Arteries (TAs) and Other Medium Size Arteries
3.2.1. Technical Requirements (According to Schmidt)
3.2.2. Machine Adjustments (According to Schmidt)
3.2.3. Sequence of the US Exam (According to Schmidt)
- “Dark halo” sign: An usually homogeneous, hypoechoic wall thickening surrounding the lumen of an inflamed artery. It is well outlined towards the luminal side, visible both in longitudinal and transverse planes, most commonly concentric in transverse.
- b.
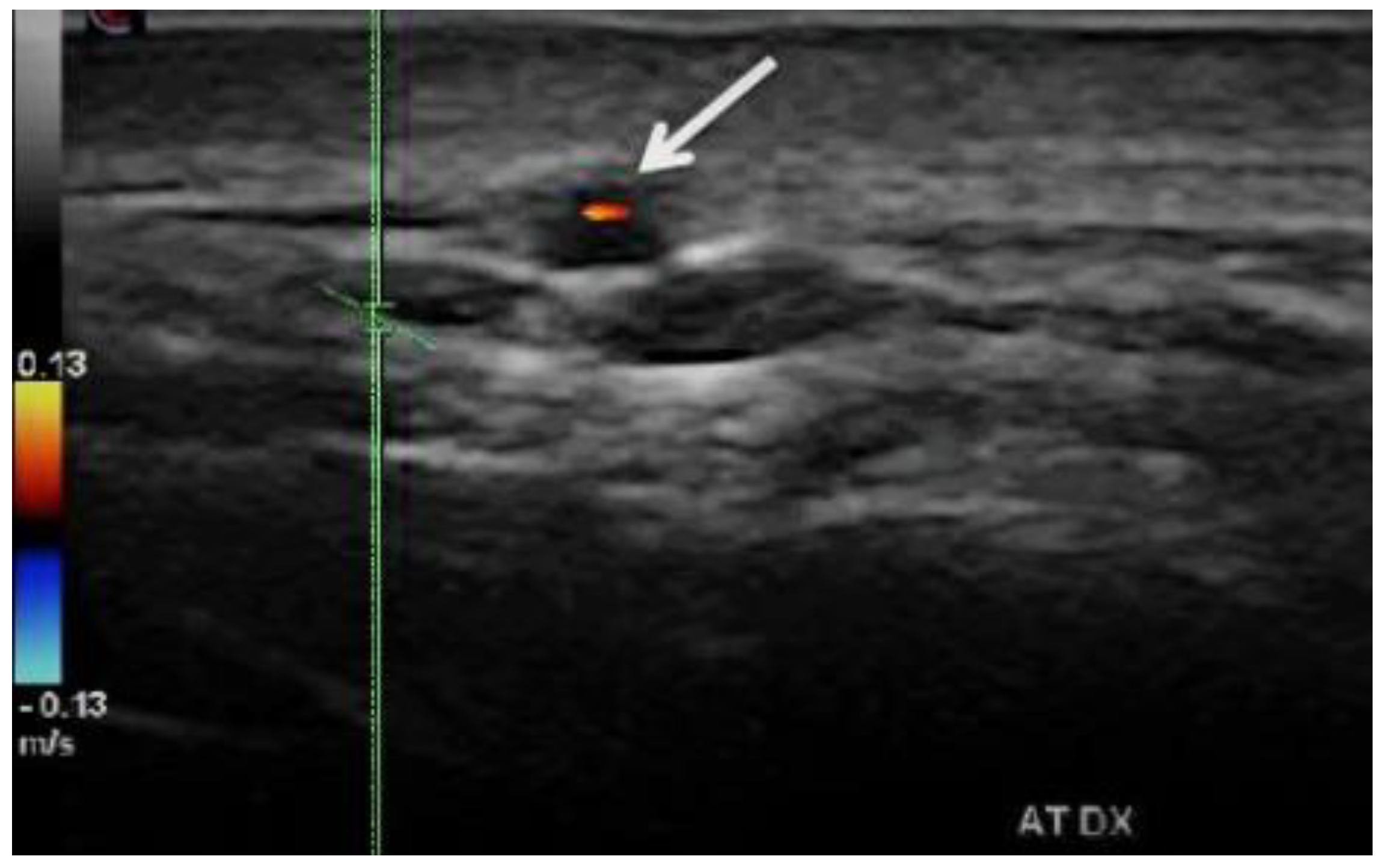
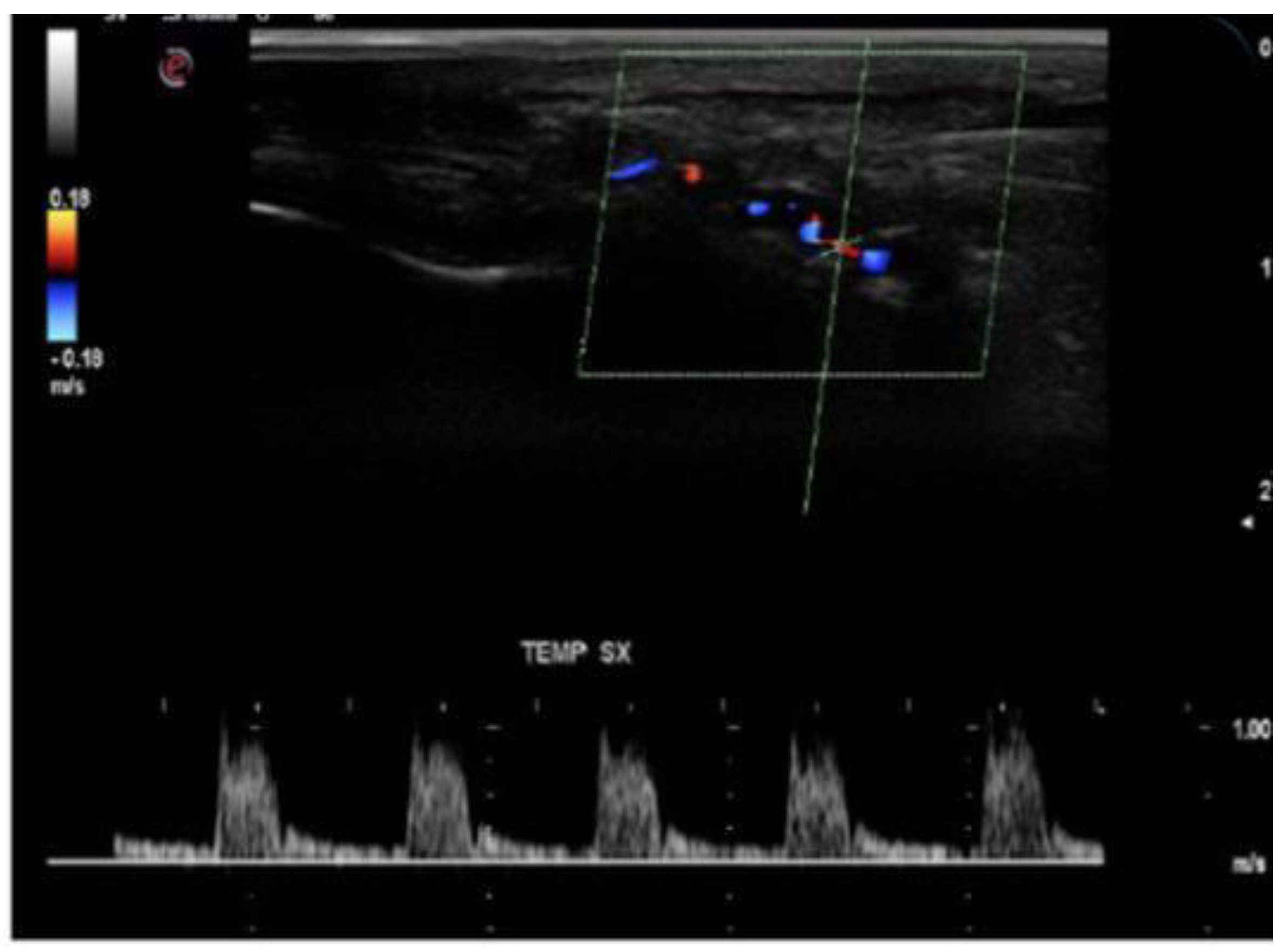
- Stenoses are characterized by aliasing and persistent diastolic flow by colour Doppler US. The peak systolic velocity (PSV) assessed within the stenosis area by pulsed-wave Doppler US is two or more times greater than the PSV recorded in the prestenotic segment of the vessel, with turbulence at the level of stenosis, associated with diminished velocities distal to the stenosis [30,31,32,33,34,35,36,37,38,39,40,41] (Figure 3) [11].
- c.
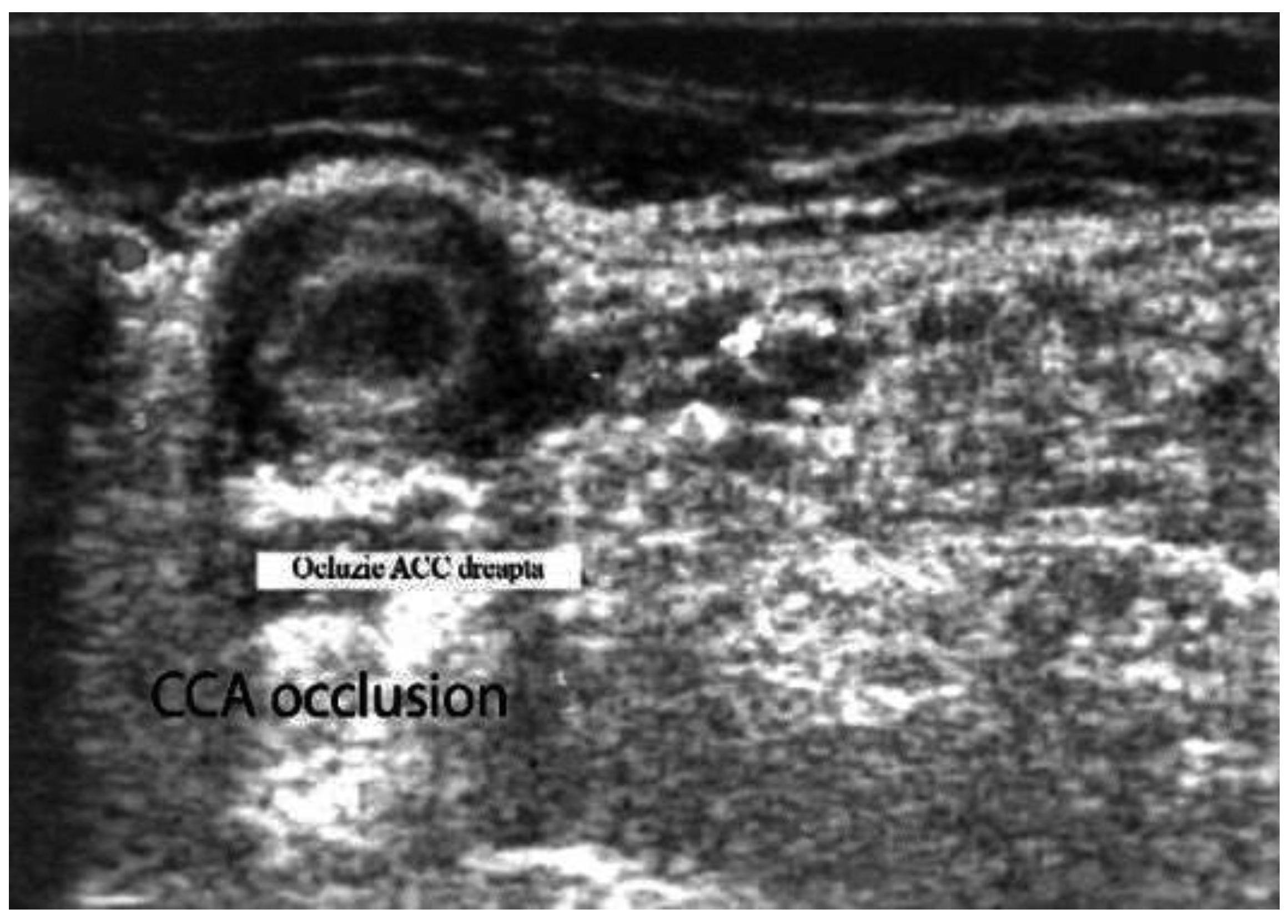
- Acute occlusions, wherein the US image is similar to that of acute embolism in different other vessels, with lack of color Doppler signals (even with low pulse repetition frequency and high color gain) in a visible artery lumen filled with hypoechoic material (cloth) [30,31,32,33,34,35,36,37,38,39,40,41].
- d.
- Compression sign. The thickened vessel wall remains visible upon compression by the ultrasound examiner; the wall swelling is hypoechogenic (in acute temporal arteritis), contrasting with the mid-echogenic to hyperechogenic surrounding tissue [38].
- The results of TAB, which is an invasive method, appear only after a few days, sometimes with inconclusive results, because skip lesions have been noted in 8.5% of the biopsies in GCA cases Biopsy may miss the lesion because of the segmental appearance of GCA [42].
- US can assess the whole length of the temporal artery and other branches of ECAs, and large supra-aortic arteries (like CCAs and axillary arteries) [43].
- US is a non-invasive procedure and can be realized as a complementary method to the clinical assessment without any delay [43].
3.3. Duplex and Color-Coded Duplex Sonography of the Large Cervical and Cervico-Brachial Vessels
- Takayasu arteritis especially affects young women (below 40 s);
- Tender scalp or polymyalgia syndrome are very rare in Takayasu arteritis.
- The involvement of CCA is more frequent in Takayasu arteritis, while temporal arteries are not affected in Takayasu arteritis.
- US image of wall thickening (“halo”) is brighter in Takayasu arteritis than in GCA, because the patient with GCA has a larger mural edema than in Takayasu arteritis (GCA being a more acute disease than Takayasu arteritis) [30].
3.4. Color Doppler Imaging (CDI) of Orbital (Retro-Bulbar) Vessels
3.4.1. The (Intra) Orbital (Retrobulbar) Arteries
Probe Selection
Technique
- Peak Systolic Velocity (PSV): The highest velocity observed during the systole of the Doppler waveform.
- End Diastolic Velocity (EDV): The lowest velocity noted during the diastole of the Doppler waveform.
- Resistivity Index (RI): PSV-EDV)/PSV.
- Mean Flow Velocity (MFV)
- Pulsatility Index (PI): PSV-EDV)/MFV.
Arterial Blood Supply of the Optic Nerve Head (ONH)
- the surface nerve fiber layer,
- the prelaminar region,
- the region of the lamina cribrosa, and
Pathophysiology of Factors Controlling Blood Flow in the ONH
- The resistance to blood flow is determined by the diameter of arteries that vascularize the ONH; this caliber depends on the following factors: the efficiency of self-regulation of the ONH arterial flow, the modifications in the arteries irrigating the head of the ON, and the rheological features of the blood, especially viscosity [11,50,51,52,53,54]
- The arterial blood pressure (BP).
- c.
- The intra-ocular pressure (IOP)
3.4.2. Anterior Ischemic Optic Neuropathies (AIONs)
Color Doppler Ultrasonography of Intraorbital Arteries in A-AIONs
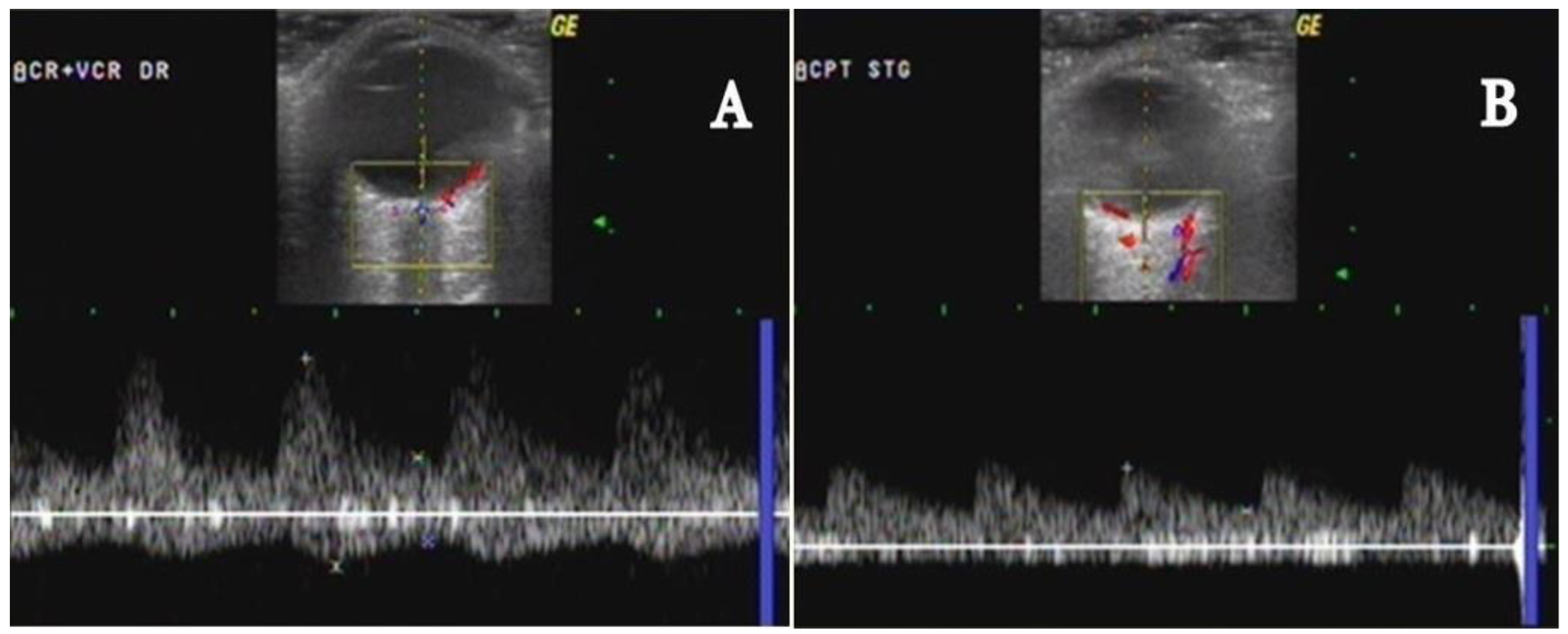
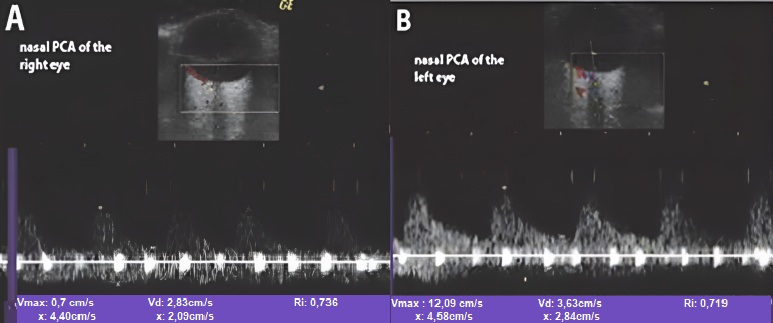
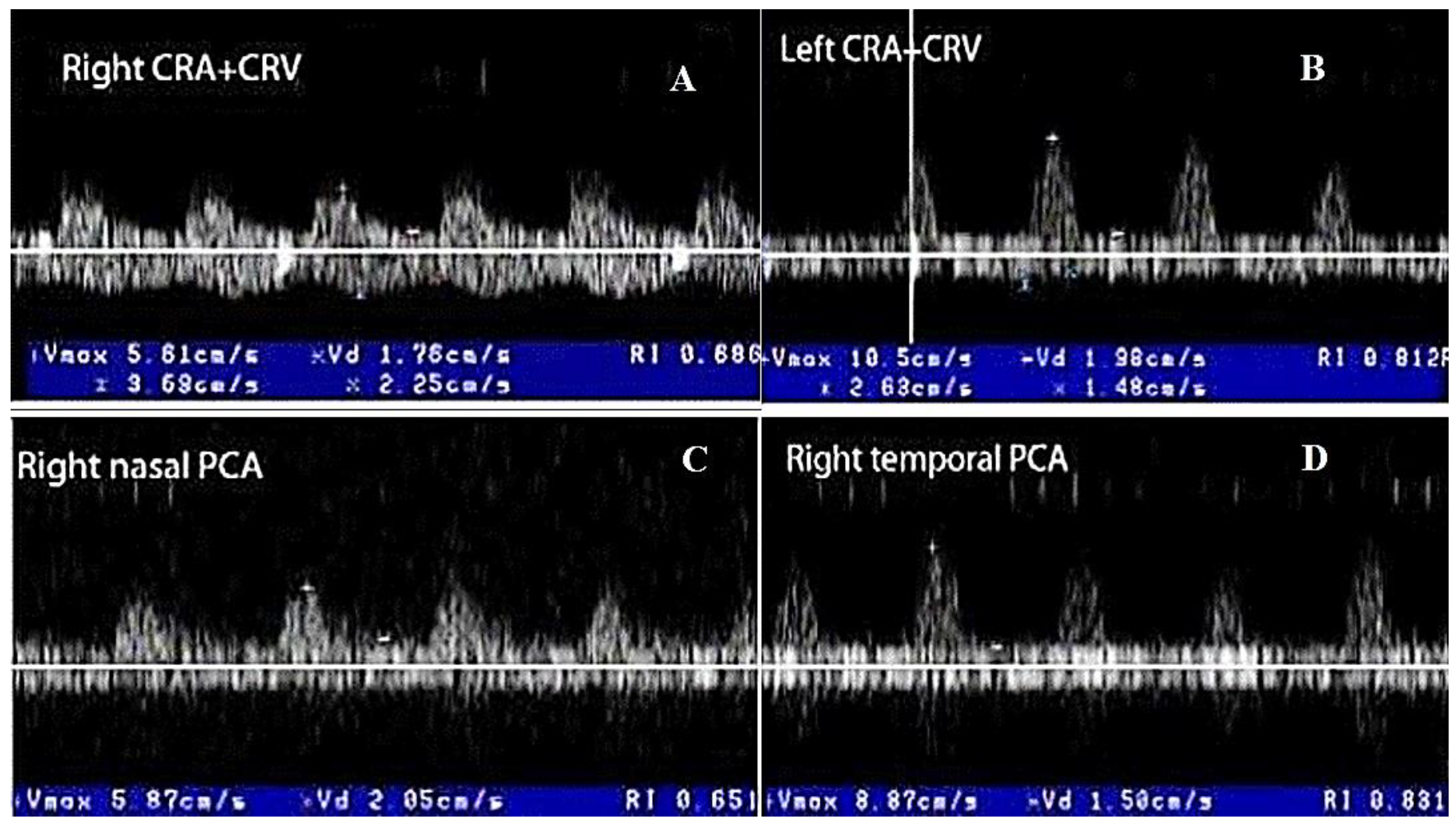
- In the acute phase of unilateral clinical eye involvement, absent (undetectable) signals in the homolateral PCAs (not corresponding to homolateral internal carotid artery occlusive disease) are classified as Doppler US features in acute arteritic AION (consecutive to GCA). In addition, we can identify a high resistance index (RI), with decreased velocities (especially EDV) in all retrobulbar vessels, in both orbits [9,10,11,12,13,14,15,60,61,62] (Table 2) [13].
- GCA acute cases with no evident clinical ocular involvement present a decrease in arterial flow in bilateral orbits, with increased RI, and diminished velocities (especially EDV). The severely diminished flow in the PCA, associated with diminished flow in the CRA and very high flow in the OA (all on the affected side) are the common US features in this type of patient. This US aspect is an essential predictor of an imminent A-AION and needs prompt treatment with high-dose corticosteroids [9,10,11,12,13,14,15,60,61,62] (Figure 7) [11].
Color Doppler Ultrasonography of Intraorbital Arteries in NA-AIONs
3.4.3. Central Retinal Artery Occlusion (CRAO)
- On funduscopy, the entire retina, with the exception of the fovea, appears pale, swollen and opaque (ischemic whitening of the retina as a result of cloudy swelling), while the central fovea still looks reddish (the so-called “cherry-red spot” in the middle of the retina). The central fovea is supplied by the cilio retinal artery, which is a rami of the short PCA. Thus, in CRAO, there is a relatively intact choroidal circulation (blood flow in PCA is normal), in contrast to the ischemic retina (where CRA is obstructed) [11,16,17,55,56,57].
Color Doppler Ultrasonography in the CRAO
4. US and Others Imaging Techniques
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Gonzalez-Gay, M. The diagnosis and management of patients with giant cell arteritis. J. Rheumatol. 2005, 32, 1186–1188. [Google Scholar]
- Salvarani, C.; Cantini, F.; Hunder, G.G. Polymyalgia rheumatica and giant-cell arteritis. Lancet 2008, 372, 234–245. [Google Scholar] [CrossRef]
- Melson, M.R.; Weyand, C.M.; Newman, N.J.; Biousse, V. The diagnosis of giant cell arteritis. Rev. Neurol Dis. 2007, 4, 128–142. [Google Scholar]
- Hayreh, S.S.; Podhajsky, P.A.; Raman, R.; Zimmerman, B. Giant cell arteritis: Validity and reliability of various diagnostic criteria. Am. J. Ophthalmol. 1997, 123, 285–296. [Google Scholar] [CrossRef]
- Levine, S.M.; Hellmann, D.B. Giant cell arteritis. Curr. Opin. Rheumatol. 2002, 14, 3–10. [Google Scholar] [CrossRef]
- Weyand, C.M.; Tetzlaff, N.; Björnsson, J.; Brack, A.; Younge, B.; Goronzy, J.J. Disease patterns and tissue cytokine profiles in giant cell arteritis. Arthritis Rheum. 1997, 40, 19–26. [Google Scholar] [CrossRef] [PubMed]
- Hunder, G.G.; Bloch, D.A.; Michel, B.A.; Stevens, M.B.; Arend, W.P.; Do, L.H.C.; Edworthy, S.M.; Fauci, A.S.; Leavitt, R.Y.; Lie, J.T.; et al. The American College of Rheumatology 1990 criteria for the classification of giant cell arteritis. Arthritis Rheum. 1990, 33, 1122–1128. [Google Scholar] [CrossRef] [PubMed]
- Jennette, J.; Falk, R.J.; Bacon, P.A.; Basu, N.; Cid, M.C.; Ferrario, F.; Flores-Suarez, L.F.; Gross, W.L.; Guillevin, L.; Hagen, E.G.; et al. 2012 Revised international Chapell Hill consensus Conference Nomenclature of Vasculitides. Arthritis Rheum. 2013, 65, 1–11. [Google Scholar] [CrossRef]
- Stanca, H.T.; Suvac, E.; Munteanu, M.; Jianu, D.C.; Motoc, A.G.M.; Roşca, G.C.; Boruga, O. Giant cell arteritis with arteritic anterior ischemic optic neuropathy. Rom. J. Morphol. Embryol. = Rev. Roum. Morphol. Embryol. 2017, 58, 281–285. [Google Scholar]
- Jianu, D.C.; Jianu, S.N.; Petrica, L.; Serpe, M. Large Giant Cell Arteritis with Eye Involvement. In Advances in the Diagnosis and Treatment of Vasculitis-Luis; Amezcua-Guerra, M., Ed.; InTech: Rijeka, Croatia, 2011; Chapter 16; pp. 311–330. [Google Scholar]
- Jianu, D.C.; Jianu, S.N.; Munteanu, G.; Dan, T.F.; Gogu, A.E.; Petrica, L. Chapter–An Integrated Approach to the Role of Neurosonology in the Diagnosis of Giant Cell Arteritis [Online First]. In Giant-Cell Arteritis-Imtiaz Chaudhry; IntechOpen: London, UK, 2021. [Google Scholar]
- Jianu, D.C.; Jianu, S.N. The role of Color Doppler Imaging in the study of optic neuropathies. In Color Doppler Imaging; Neuro-Ophthalmological Correlations; Jianu, D.C., Jianu, S.N., Eds.; Mirton: Timisoara, Romania, 2010; Chapter 8; pp. 154–174. [Google Scholar]
- Jianu, D.C.; Jianu, S.N. Giant Cell Arteritis and arteritic anterior ischemic optic neuropathies. In Updates in the Diagnosis and Treatment of Vasculitis; Sakkas, L., Katsiari, C., Eds.; InTech: Rijeka, Croatia, 2013; Chapter 5; pp. 111–130. [Google Scholar]
- Jianu, D.C.; Jianu, S.N.; Petrica, L.; Motoc, A.G.M.; Dan, T.F.; Lazureanu, D.C. Munteanu M-Clinical and color Doppler imaging features of one patient with occult giant cell arteritis presenting arteritic anterior ischemic optic neuropathy. Rom. J. Morphol. Embryol. 2016, 57, 579–583. [Google Scholar]
- Jianu, D.C.; Jianu, S.N.; Munteanu, M.; Petrica, L. Clinical and ultrasonographic features in anterior ischemic optic neuropathies-Vojnosanit. Pregl. 2018, 75, 773–779. [Google Scholar]
- Jianu, D.C.; Jianu, S.N. The role of Color Doppler Imaging in the study of central retinal artery obstruction. In Color Doppler Imaging; Neuro-Ophthalmological Correlations; Jianu, D.C., Jianu, S.N., Eds.; Mirton: Timisoara, Romania, 2010; Chapter 6; pp. 125–142. [Google Scholar]
- Jianu, D.C.; Jianu, S.N.; Munteanu, M.; Vlad, D.; Rosca, C.; Petrica, L. Color Doppler imaging features of two patients presenting central retinal artery occlusion with and without giant cell arteritis. Vojnosanit. Pregl. 2016, 73, 397–401. [Google Scholar]
- Olah, L. Ultrasound principles. In Manual of Neurosonology; Csiba, L., Baracchini, C., Eds.; Cambridge University Press: Cambridge, UK, 2016; Chapter 1; pp. 1–14. [Google Scholar]
- Lee, R.M. Morphology of cerebral arteries. Pharmacol. Ther. 1995, 66, 149–173. [Google Scholar] [CrossRef]
- Nichols, W.W.; O’Rourke, M.F.; McDonald, D.A. Special circulations. In McDonald’s Blood Flow in Arteries: Theoretical, Experimental and Clinical Principles, 6th ed.; Nichols, W.W., O’Rourke, M.F., McDonald, D.A., Eds.; Hodder Arnold: London, UK, 2011; pp. 397–410. [Google Scholar]
- Ross, R. Atherosclerosis is an inflammatory disease. N. Engl. J. Med. 1999, 340, 115–126. [Google Scholar] [CrossRef] [PubMed]
- Stary, H.C.; Blankenhorn, D.H.; Chandler, A.B.; Glagov, S.; Insull, W., Jr.; Richardson, M.; Rosenfeld, M.E.; Schaffer, S.A.; Schwartz, C.J.; Wagner, W.D. A definition of the intima of human arteries and of its atherosclerosis-prone regions. A report from the Committee on Vascular Lesions of the Council on Arteriosclerosis, American Heart Association. Circulation 1992, 85, 391–405. [Google Scholar] [CrossRef] [Green Version]
- Stary, H.C.; Chandler, A.B.; Dinsmore, R.E.; Fuster, V.; Glagov, S.; Insull, W., Jr.; Rosenfeld, M.E.; Scwartz, C.J.; Wagner, W.D.; Wissler, R.W. A definition of advanced types of atherosclerotic lesions and a histological classification of atherosclerosis. Arter. Throm. Vasc. Biol. 1995, 15, 1512–1531. [Google Scholar] [CrossRef]
- Touboul, P.J.; Hennerici, M.G.; Meairs, S.; Adams, H.; Amarenco, P.; Desvarieux, M.; Ebrahim, S.; Fata, M.; Hernandez, R.; Kownator, S.; et al. Mannheim intima-media thickness consensus. Cerebrovasc. Dis. 2004, 18, 346–349. [Google Scholar] [CrossRef]
- Del Sette, M.; Saia, V. Atherosclerotic carotid disease. Carotid ultrasound imaging. In Manual of Neurosonology; Csiba, L., Baracchini, C., Eds.; Cambridge University Press: Cambridge, UK, 2016; Chapter 5A; pp. 57–63. [Google Scholar]
- Von Reutern, G.M. Atherosclerotic carotid disease. Grading carotid stenosis. In Manual of Neurosonology; Csiba, L., Baracchini, C., Eds.; Cambridge University Press: Cambridge, UK, 2016; Chapter 5C; pp. 79–86. [Google Scholar]
- Simon, A.; Megnien, J.-L.; Chironi, G. The Value of Carotid Intima-Media Thickness for Predicting Cardiovascular Risk. Arter. Thromb. Vasc. Biol. 2010, 30, 182–185. [Google Scholar] [CrossRef] [Green Version]
- Lorenz, M.W.; Polak, J.F.; Kavousi, M.; Mathiesen, E.B.; Völzke, H.; Tuomainen, T.-P.; Sander, D.; Plichart, M.; Catapano, A.L.; Robertson, C.M.; et al. Carotid intima-media thickness progression to predict cardiovascular events in the general population (the PROG-IMT collaborative project): A meta-analysis of individual participant data. Lancet 2019, 379, 2053–2062. [Google Scholar] [CrossRef] [Green Version]
- Ohira, T.; Shahar, E.; Iso, H.; Chambless, L.E.; Rosamond, W.D.; Sharrett, R.; Folsom, A.R. Carotid artery wall thickness and risk of stroke subtypes: The atherosclerosis risk in communities study. Stroke 2011, 42, 397–403. [Google Scholar] [CrossRef] [Green Version]
- Sturzenegger, M.H. Cervical artery vasculitides. In Manual of Neurosonology; Csiba, L., Baracchini, C., Eds.; Cambridge University Press: Cambridge, UK, 2016; Chapter 8; pp. 300–305. [Google Scholar]
- Schmidt, W.A. Ultrasound in the diagnosis and management of giant cell arteritis. Rheumatology 2018, 57, ii22–ii31. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Schmidt, W.A. Takayasu and temporal arteritis. In Handbook on Neurovascular Ultrasound; Baumgartner, R.W., Ed.; Karger: Basel, Switzerland, 2006; Volume 21, pp. 96–104. [Google Scholar]
- Schmidt, W.A.; Kraft, H.E.; Vorpahl, K.; Völker, L.; Gromnica-Ihle, E.J. Color Duplex Ultrasonography in the Diagnosis of Temporal Arteritis. N. Engl. J. Med. 1997, 337, 1336–1342. [Google Scholar] [CrossRef] [PubMed]
- Schmidt, W.A. Role of ultrasound in the understanding and management of vasculitis. Adv. Musculoskelet. Dis. 2013, 6, 39–47. [Google Scholar] [CrossRef] [Green Version]
- Monti, S.; Floris, A.; Ponte, C.; Schmidt, W.A.; Diamantopoulos, A.P.; Pereira, C.; Piper, J.; Luqmani, R. The use of ultrasound to assess giant cell arteritis: Review of the current evidence and practical guide for the rheumatologist. Rheumatology 2018, 57, 227–235. [Google Scholar] [CrossRef] [Green Version]
- Duftner, C.; Dejaco, C.; Moller-Dohn, U. Ultrasound definitions for vasculitis in cranial and large vessel giant cell arteritis: Results of a Delphi survey of the OMERACT ultrasound large vessel vasculitis group. Ann. Rheum. Dis. 2016, 75 (Suppl. S2), 626. [Google Scholar] [CrossRef]
- Arida, A.; Kyprianou, M.; Kanakis, M.; Sfikakis, P.P. The diagnostic value of ultrasonography-derived edema of the temporal artery wall in giant cell arteritis: A second meta-analysis. BMC Musculoskelet. Disord. 2010, 11, 44. [Google Scholar] [CrossRef] [Green Version]
- Coath, F.L.; Mukhtyar, C. Ultrasonography in the diagnosis and follow-up of giant cell arteritis. Rheumatology 2021, 60, 2528–2536. [Google Scholar] [CrossRef]
- Serodio, J.F.; Trindade, M.; Favas, C.; Alvez, J.D. Chapter—Extra-Cranial Involvement in Giant Cell Arteritis [Online First]. In Giant-Cell Arteritis-Imtiaz Chaudhry; IntechOpen: London, UK, 2021. [Google Scholar]
- Schmidt, W.A.; Krause, A.; Schicke, B.; Kuchenbecker, J.; Gromnica-Ihle, E. Do temporal artery duplex ultrasound findings correlate with ophthalmic complications in giant cell arteritis? Rheumatology 2009, 48, 383–385. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Karassa, F.B.; Matsagas, M.I.; Schmidt, W.A.; Ioannidis, J.P. Meta-analysis: Test performance of ultrasonography fogiant-cell arteritis. Ann. Intern. Med. 2005, 142, 359–369. [Google Scholar] [CrossRef]
- Poller, D.N.; van Wyk, Q.; Jeffrey, M.J. The importance of skip lesions in temporal arteritis. J. Clin. Pathol. 2000, 53, 137–139. [Google Scholar] [CrossRef] [Green Version]
- Diamantopoulos, A.P.; Haugeberg, G.; Lindland, A.; Myklebust, G. The fast-track ultrasound clinic for early diagnosis of giant cell arteritis significantly reduces permanent visual impairment: Towards a more effective strategy to improve clinical outcome in giant cell arteritis? Rheumatology 2016, 55, 66–70. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Schmidt, W.A.; Seifert, A.; Gromnica-Ihle, E.; Krause, A.; Natusch, A. Ultrasound of proximal upper extremity arteries to increase the diagnostic yield in large-vessel giant cell arteritis. Rheumatology 2008, 47, 96–101. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hayreh, S.S.; Podhajsky, P.A.; Zimmerman, B. Occult giant cell arteritis: Ocular manifestations. Am. J. Ophthalmol. 1998, 125, 521–526. [Google Scholar] [CrossRef]
- Hayreh, S.S.; Zimmerman, B.; Kardon, R.H. Visual improvement with corticosteroid therapy in giant cell arteritis. Report of a large study and review of literature. Acta Ophthalmol. Scand. 2002, 80, 355–367. [Google Scholar] [CrossRef]
- Daneshmeyer, H.; Savino, P.; Gamble, G. Poor Prognosis of Visual Outcome after Visual Loss from Giant Cell Arteritis. Ophthalmology 2005, 112, 1098–1103. [Google Scholar] [CrossRef] [PubMed]
- González-Gay, M.A.; García-Porrúa, C.; Llorca, J.; Hajeer, A.H.; Brañas, F.; Dababneh, A.; González-Louzao, C.; Rodriguez-Gil, E.; Rodríguez-Ledo, P.; Ollier, W.E.R. Visual Manifestations of Giant Cell Arteritis: Trends and Clinical Spectrum in 161 Patients. Medicine 2000, 79, 283–292. [Google Scholar] [CrossRef] [PubMed]
- Singh, A.G.; Kermani, T.A.; Crowson, C.S.; Weyand, C.M.; Matteson, E.L.; Warrington, K.J. Visual Manifestations in Giant Cell Arteritis: Trend over 5 Decades in a Population-based Cohort. J. Rheumatol. 2015, 42, 309–315. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Arnold, A.C.; Wang, M.Y. Ischemic optic neuropathy. In Ophtalmology, 5th ed.; Ianoff, M., Duker, J.S., Eds.; Elsevier: Amsterdam, The Netherlands, 2019; Chapter 9.8; pp. 892–897. [Google Scholar]
- Biousse, V.; Newman, N.J. Ischemic Optic Neuropathies. N. Engl. J. Med. 2015, 372, 2428–2436. [Google Scholar] [CrossRef]
- Hayreh, S.S. Ischemic optic neuropathies-where are we now? Graefes Arch. Clin. Exp. Oplnhalmol. 2013, 251, 1873–1884. [Google Scholar] [CrossRef] [PubMed]
- Hayreh, S.S. Ischaemic optic neuropathy. Indian J. Ophthalmol. 2000, 48, 171–194. [Google Scholar]
- Collignon-Robe, N.J.; Feke, G.T.; Rizzo, J.F. Optic nerve head circulation in nonarteritic anterior ischemic optic neuropathy and optic neuritis. Ophthalmology 2004, 111, 1663–1672. [Google Scholar] [CrossRef] [PubMed]
- Duker, J.S.; Duker, J.S. Retinal arterial obstruction. In Ophtalmology, 5th ed.; Yanoff, M., Duker, J.S., Eds.; Elsevier: Amsterdam, The Netherlands, 2019; Chapter 6.9; pp. 520–527. [Google Scholar]
- Ahuja, R.M.; Chaturvedi, S.; Elliot, D.; Joshi, N.; Puklin, J.E.; Abrams, G.W. Mechanism of retinal arterial occlusive disease in African, American and Caucasian patients. Stroke 1999, 30, 1506–1509. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Connolly, B.P.; Krishnan, A.; Shah, G.K.; Whelan, J.; Brown, G.C.; Eagle Jr, R.C.; Shakin, E.P. Characteristics of patients presenting with central retinal artery occlusion with and without giant cell arteritis. Can. J. Ophthalmol. 2000, 35, 379–384. [Google Scholar] [CrossRef]
- Siebler, M. Neuro-orbital ultrasound. In Manual of Neurosonology; Csiba, L., Baracchini, C., Eds.; Cambridge University Press: Cambridge, UK, 2016; Chapter 25; pp. 300–305. [Google Scholar]
- Lieb, W.E.; Cohen, S.M.; Merton, D.A.; Shields, J.A.; Mitchell, D.G.; Goldberg, B.B. Color Doppler Imaging of the Eye and Orbit. Arch. Ophthalmol. 1991, 109, 527–531. [Google Scholar] [CrossRef] [PubMed]
- Tranquart, F.; Bergès, O.; Koskas, P.; Arsene, S.; Rossazza, C.; Pisella, P.-J.; Pourcelot, L. Color doppler imaging of orbital vessels: Personal experience and literature review. J. Clin. Ultrasound 2003, 31, 258–273. [Google Scholar] [CrossRef]
- Ching, J.; Smith, S.M.; Dasgupta, B.; Damato, E.M. The role of vascular ultrasound in managing giant cell arteritis in ophthalmology. Surv. Ophthalmol. 2019, 65, 218–226. [Google Scholar] [CrossRef]
- Tranquart, F.; Aubert-Urena, A.S.; Arsene, S.; Audrierie, C.; Rossazza, C.; Pourcelot, L. Echo-Doppler couleur des arteres ciliaires posterieures dans la neuropathie optique ischemique anterieure aigue. JEMU 1997, 18, 6871. [Google Scholar]
- Czihal, M.; Lottspeich, C.; Köhler, A.; Prearo, I.; Hoffmann, U.; Priglinger, S.G.; Mackert, M.J. Transocular sonography in acute arterial occlusions of the eye in elderly patients: Diagnostic value of the spot sign. PLoS ONE 2021, 16, e0247072. [Google Scholar] [CrossRef]
- Hellmich, B.; Agueda, A.; Monti, S.; Buttgereit, F.; De Boysson, H.; Brouwer, E.; Cassie, R.; Cid, M.C.; Dasgupta, B.; Dejaco, C.; et al. 2018 Update of the EULAR recommendations for the management of large vessel vasculitis. Ann. Rheum. Dis. 2020, 79, 19–30. [Google Scholar] [CrossRef] [Green Version]
- Bley, T.A.; Reinhard, M.; Hauenstein, C.; Markl, M.; Warnatz, K.; Hetzel, A.; Uhl, M.; Vaith, P.; Langer, M. Comparison of duplex sonography and high-resolution magnetic resonance imaging in the diagnosis of giant cell (temporal) arteritis. Arthritis Rheum. 2008, 58, 2574–2578. [Google Scholar] [CrossRef]
- Lecler, A.; Hage, R.; Charbonneau, F.; Vignal, C.; Sené, T.; Picard, H.; Leturcq, T.; Zuber, K.; Belangé, G.; Affortit, A.; et al. Validation of a multimodal algorithm for diagnosing giant cell arteritis with imaging. Diagn. Interv. Imaging 2021. [Google Scholar] [CrossRef]
- Prieto-González, S.; Arguis, P.; García-Martínez, A.; Espígol-Frigolé, G.; Tavera-Bahillo, I.; Butjosa, M.; Sánchez, M.; Hernández-Rodríguez, J.; Grau, J.M.; Cid, M.C. Large vessel involvement in biopsy-proven giant cell arteritis: Prospective study in 40 newly diagnosed patients using CT angiography. Ann. Rheum. Dis. 2012, 71, 1170–1176. [Google Scholar] [CrossRef]
- Agard, C.; Barrier, J.H.; Dupas, B.; Ponge, T.; Mahr, A.; Fradet, G.; Chevalet, P.; Masseau, A.; Batard, E.; Pottier, P.; et al. Aortic involvement in recent-onset giant cell (temporal) arteritis: A case-control prospective study using helical aortic computed tomodensitometric scan. Arthritis Care Res. 2008, 59, 670–676. [Google Scholar] [CrossRef]
- Prieto-González, S.; Arguis, P.; Cid, M.C. Imaging in systemic vasculitis. Curr. Opin. Rheumatol. 2015, 27, 53–62. [Google Scholar] [CrossRef] [PubMed]
- Walter, M.A.; Melzer, R.A.; Schindler, C.; Müller-Brand, J.; Tyndall, A.; Nitzsche, E.U. The value of [18F] FDG-PET in the diagnosis of large vessel vasculitis and the assessment of activity and extent of disease. Eur. J. Nucl. Med. Mol. Imaging 2005, 32, 674–681. [Google Scholar] [CrossRef] [PubMed]
- Lariviere, D.; Benali, K.; Coustet, B.; Pasi, N.; Hyafil, F.; Klein, I.; Chauchard, M.; Alexandra, J.F.; Goulenok, T.; Dossier, A.; et al. Positron emission tomography and computed tomography angiography for the diagnosis of giant cell arteritis: A real-life prospective study. Medicine 2016, 96, e4146. [Google Scholar] [CrossRef] [PubMed]
- Germano, G.; Macchioni, P.; Possemato, N.; Boiardi, L.; Nicolini, A.; Casali, M.; Versari, A.; Pipitone, N.; Salvarani, C. Contrast enhanced ultrasound of the carotid artery in patients with large vessel vasculitis: Correlation with positron emission tomography findings. Arthritis Care Res. 2017, 69, 143–149. [Google Scholar] [CrossRef]
- Soussan, M.; Nicolas, P.; Schramm, C.; Katsahian, S.; Pop, G.; Fain, O.; Mekinian, A. Management of large-vessel vasculitis: A systematic literature review and meta-analysis with FDG-PET. Medicine 2015, 94, e622. [Google Scholar] [CrossRef] [PubMed]
- Imfeld, S.; Aschwanden, M.; Rottenburger, C.; Schegk, E.; Berger, C.T.; Staub, D.; Daikeler, T. 18F-FDG positron emission tomography and ultrasound in the diagnosis of giant cell arteritis: Congruent or complementary imaging methods? Rheumatology 2019, 59, 772–778. [Google Scholar] [CrossRef] [PubMed]
- Nielsen, B.D.; Hansen, I.T.; Keller, K.K.; Therkildsen, P.; Gormsen, L.C.; Hauge, E.-M. Diagnostic accuracy of ultrasound for detecting large-vessel giant cell arteritis using FDG PET/CT as the reference. Rheumatology 2019, 59, 2062–2073. [Google Scholar] [CrossRef]
- Petrica, L.; Petrica, M.; Munteanu, M.; Vlad, A.; Bob, F.; Gluhovschi, C.; Gluhovschi, G.H.; Jianu, D.C.; Schiller, A.; Velciov, S.; et al. Cerebral microangiopathy in patients with non-insulin-dependent diabetes mellitus. Ann. Acad. Med. Singap. 2007, 36, 259–266. [Google Scholar] [PubMed]
- Pierro, L.; Arrigo, A.; Aragona, E.; Cavalleri, M.; Bandello, F. Vessel Density and Vessel Tortuosity Quantitative Analysis of Arteritic and Non-arteritic Anterior Ischemic Optic Neuropathies: An Optical Coherence Tomography Angiography Study. J. Clin. Med. 2020, 9, 1094. [Google Scholar] [CrossRef] [PubMed]









{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Parameter | OA | CRA | PCA (Temporal) | PCA (Nasal) | SOV (Superior Ophthalmic Vein) |
|---|---|---|---|---|---|
| PSV (cm/s) | 45.3 ± 10.5 | 17.3 ± 2.6 | 13.3 ± 3.5 | 12.4 ± 3.4 | 10.2 ± 3.8 |
| EDV (cm/s) | 11.8 ± 4.3 | 6.2 ± 2.7 | 6.4 ± 1.5 | 5.8 ± 2.5 | 4.3 ± 2.4 |
| RI | 0.74 ± 0.07 | 0.63 ± 0.09 | 0.52 ± 0.10 | 0.53 ± 0.08 |
| Arteries | CRA | PCA t | PCA n | OA |
|---|---|---|---|---|
| Cut-off point | 0.67 | 0.71 | 0.68 | 0.81 |
| Se | 0.76 | 0.86 | 0.86 | 1 |
| Sp | 0.81 | 0.96 | 0.93 | 0.96 |
| PPV | 0.51 | 0.88 | 0.76 | 0.89 |
| NPV | 0.92 | 0.96 | 0.96 | 1 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Jianu, D.C.; Jianu, S.N.; Dan, T.F.; Munteanu, G.; Bîrdac, C.D.; Motoc, A.G.M.; Docu Axelerad, A.; Petrica, L.; Gogu, A.E. Ultrasound Technologies and the Diagnosis of Giant Cell Arteritis. Biomedicines 2021, 9, 1801. https://doi.org/10.3390/biomedicines9121801
Jianu DC, Jianu SN, Dan TF, Munteanu G, Bîrdac CD, Motoc AGM, Docu Axelerad A, Petrica L, Gogu AE. Ultrasound Technologies and the Diagnosis of Giant Cell Arteritis. Biomedicines. 2021; 9(12):1801. https://doi.org/10.3390/biomedicines9121801
Chicago/Turabian StyleJianu, Dragoș Cătălin, Silviana Nina Jianu, Traian Flavius Dan, Georgiana Munteanu, Claudiu Dumitru Bîrdac, Andrei Gheorghe Marius Motoc, Any Docu Axelerad, Ligia Petrica, and Anca Elena Gogu. 2021. "Ultrasound Technologies and the Diagnosis of Giant Cell Arteritis" Biomedicines 9, no. 12: 1801. https://doi.org/10.3390/biomedicines9121801