Oxidative Stress Markers in Chronic Kidney Disease with Emphasis on Diabetic Nephropathy


1
Department of Nephrology, Clinic for Internal Medicine, University Medical Centre Maribor, Ljubljanska 5, 2000 Maribor, Slovenia
2
Faculty of Medicine, University of Maribor, Taborska 8, 2000 Maribor, Slovenia
3
Department of Dialysis, Clinic for Internal Medicine, University Medical Centre Maribor, Ljubljanska 5, 2000 Maribor, Slovenia
*
Author to whom correspondence should be addressed.
Antioxidants 2020, 9(10), 925; https://doi.org/10.3390/antiox9100925
Submission received: 26 August 2020
/
Revised: 20 September 2020
/
Accepted: 24 September 2020
/
Published: 27 September 2020
(This article belongs to the Special Issue Antioxidants and Chronic Inflammation)
Abstract
:Diabetes prevalence is increasing worldwide, especially through the increase of type 2 diabetes. Diabetic nephropathy occurs in up to 40% of diabetic patients and is the leading cause of end-stage renal disease. Various factors affect the development and progression of diabetic nephropathy. Hyperglycaemia increases free radical production, resulting in oxidative stress, which plays an important role in the pathogenesis of diabetic nephropathy. Free radicals have a short half-life and are difficult to measure. In contrast, oxidation products, including lipid peroxidation, protein oxidation, and nucleic acid oxidation, have longer lifetimes and are used to evaluate oxidative stress. In recent years, different oxidative stress biomarkers associated with diabetic nephropathy have been found. This review summarises current evidence of oxidative stress biomarkers in patients with diabetic nephropathy. Although some of them are promising, they cannot replace currently used clinical biomarkers (eGFR, proteinuria) in the development and progression of diabetic nephropathy.
1. Introduction
Chronic kidney disease (CKD) is a common and serious disease that affects 8 to 16% of the global population [1]. Management of CKD is costly and it presents a significant challenge for societies and health care systems [2]. In 2016, CKD was the 16th leading cause of years of life lost worldwide, mainly due to cardiovascular diseases and infections, and is expected to rise to 5th place by 2040 [3]. The increasing prevalence of CKD is associated with the increase in patients with diabetes and hypertension [4,5,6]. In 2019, 463 million people had diabetes and the International Diabetes Federation estimates that there will be 700 million adults with diabetes by 2045 [6]. Diabetes prevalence is increasing, especially through an increase in type 2 diabetes [6]. Diabetes is the main cause of CKD in many developed countries and is quickly becoming the leading cause in developing countries [4]. Diabetic nephropathy (DN) occurs in up to 40% of type 1 or type 2 diabetic patients [7]. Other frequent causes of CKD are hypertension, glomerulonephritides, etc.; in many cases, the cause of CKD is unknown [2,8].
Oxidative stress contributes to many pathological conditions. It is involved in the onset and/or progression of cancer, atherosclerosis, neurological disorders, cardiovascular diseases, pulmonary diseases, and diabetes [9,10,11,12,13,14,15]. Diabetes mellitus is a chronic disease with either a lack of insulin production or, more commonly, resistance to insulin, leading to hyperglycaemia. Hyperglycaemia increases free radical production, leading to oxidative stress [16]. Experimental and clinical studies suggest an association between hyperglycaemia, oxidative stress, and diabetic complications [16,17,18,19]. Oxidative stress plays an important role in the pathogenesis of DN and its progression to end-stage renal disease (ESRD) [16,20,21,22].
In the current review, we will present the role of oxidative stress in patients with diabetes and CKD. Our emphasis will be presenting the oxidative stress markers in the development and progression of diabetic nephropathy used in clinical studies.
2. Oxidative Stress
Oxidative stress is a state of imbalance between oxidants and antioxidants [23]. It is dependent on the production and accumulation of oxidant radicals in cells and tissues and the ability of a biological system to detoxify these reactive products [24]. Oxidant compounds (reactive oxygen species (ROS), reactive nitrogen species (RNS)) are products of normal cellular metabolism. We can divide them into free radicals and nonradicals [25]. Free radicals have one or more unpaired electrons and are therefore highly reactive [23,25]. Examples of the most important ROS and RNS of physiological significance are superoxide anion (O2•−), hydroxyl radical (•OH), nitric oxide radical (NO•), and nitrogen dioxide radical (NO2•) [9]. When two free radicals share their unpaired electrons, nonradicals are formed. More often, free radicals attack nonradical molecules and a new radical molecule is formed, triggering a chain reaction [23]. Examples of nonradical oxidants are hydrogen peroxide (H2O2), ozone (O3), singlet oxygen (1O2), hypochlorous acid (HOCl), nitrous acid (HNO2), dinitrogen trioxide (N2O3), peroxynitrite (ONOO−), and lipid peroxides [23].
At low to moderate concentrations, ROS and RNS act as secondary messengers and regulate intracellular signal transduction pathways regulating cell growth and differentiation, mitogenic responses, extracellular matrix production and breakdown, apoptosis, oxygen sensing, and inflammation [26,27]. ROS and RNS act as part of the immune defence system [27]. At high concentrations, they produce unwanted modifications to lipids, proteins, DNA, etc. [25]. ROS are very unstable with short half-lives (only seconds) and are therefore difficult to measure [23]. In contrast, oxidation products have longer lifetimes (from hours to weeks) and are used to assess the redox state [23,28]. The most important markers of oxidative stress are presented in Table 1.
2.1. Sources of Oxidative Stress
Normal aerobic metabolism is a major source of ROS; the most important in ROS generation are mitochondrial nicotinamide adenine dinucleotide phosphate (NADPH) oxidase (NOX), xanthine oxidase (XO), myeloperoxidase (MPO), and endothelium nitric oxide synthase (eNOS) [23,25,29]. Other enzyme sources are prostaglandin synthase, lipoxygenase, and flavoprotein dehydrogenase [23,25,29]. The main exogenous sources of oxidative stress are cigarette smoke, environmental pollution, heavy metals (Cd, Hg, Pb, Fe, and As), drugs (gentamycin, bleomycin, etc.), alcohol, chemical solvents, and radiation [23,24,25,29].
2.2. Antioxidants
The human body has defence mechanism that counterbalances the effects of oxidants: the antioxidants. They can be divided into enzymatic and nonenzymatic antioxidants. The major enzymatic antioxidants are superoxide dismutase (SOD), catalase, glutathione peroxidase (GSH-Px), haem oxygenase-1 (HO-1), and thioredoxin [23,24,25,30,31,32,33,34]. The major nonenzymatic antioxidants are glutathione (GSH), vitamins (vitamins C and E), and β-carotene [23,24,25,35,36,37]. They are low-molecular-weight compounds and are found in the plasma, extracellular fluids, intracellular fluids, lipoproteins, and membranes [9]. An important endogenous antioxidant with good antioxidant capacity is serum albumin [23,38]. There are also several exogenous antioxidant molecules (polyphenols, flavonoids) which are mainly introduced by the diet or by nutritional supplementation [23,25,39]. Enzymatic and nonenzymatic antioxidants are presented in Table 1.
3. Oxidative Stress in CKD
Oxidative stress is not only an important factor in the development of type 1 and type 2 diabetes, but it also has a significant role in the development of diabetic complications, including DN [11,14,16,17,18,19,20,21,22,40,41,42]. Oxidative stress is linked with metabolic changes and alterations in renal haemodynamics. Both mechanisms have adverse synergistic effects [40]. Oxidative stress is directly linked to podocyte damage, proteinuria, and tubulointerstitial fibrosis [43]. Additionally, vascular oxidative stress has an important role in CKD progression (Figure 1) [43,44,45,46].
3.1. Oxidative Stress and Glomerular Injury
Podocytes are vulnerable to oxidative damage [43]. Mature podocytes are highly differentiated cells and respond to injury with detachment from the glomerular basement membrane, dedifferentiation, autophagy, and apoptosis [47]. An important consequence of podocyte injury is proteinuria, which is a well-known marker of kidney damage and is associated with CKD progression [47,48]. Proteinuria is an important factor in inducing mesangial and tubular toxicity and is involved in local and systemic inflammatory pathways [48,49].
In early studies, it was shown that puromycin aminonucleoside, a podocyte toxin, induced glomerular injury in rats through ROS [43,50,51]. In these studies, antioxidants also provided protection against the changes in podocytes [51]. Later, ROS-mediated DNA damage was also shown [52]. Podocyte injury and dysfunctional glomerular filtration barrier is important in the process of focal segmental glomerular sclerosis (FSGS). The development and progression of FSGS is associated with transforming growth factor beta (TGF-β) activation in podocytes [53]. TGF-β is involved in crosstalk between podocytes and the glomerular endothelium [54]. TGF-β promotes synthesis of endothelin precursors in podocytes and expression of endothelin receptors. The binding of endothelin with its receptors suppresses mitochondrial function and induces oxidative stress in the glomerular endothelium [54]. Mitochondrial oxidative DNA damage was evident before podocyte injury [54].
Other oxidative stress markers are advanced oxidation protein products (AOPPs). They are dityrosine-containing products of plasma proteins [43]. Higher AOPP levels were found in patients with CKD compared to controls [55,56]. Podocyte injury, proteinuria, and glomerulosclerosis were associated with AOPPs through a NOX-dependent mechanism [57]. In normal rats, chronic administration of AOPPs increased proteinuria and urinary 8-hydroxydeoxyguanosine (8-OHdG) excretion. On the other hand, chronic inhibition of NOX by apocynin prevented podocyte apoptosis and decreased proteinuria in these rats [57]. AOPPs interacted with the receptor of advanced glycation end products (RAGE) on podocytes [58]. Additionally, blocking RAGE by anti-RAGE immunoglobulin G or its silencing by siRNA significantly protected podocytes from AOPP-induced apoptosis and ameliorated proteinuria in AOPP-challenged mice [58]. AOPPs are involved in the activation of Wnt/β-catenin signalling. Wnts are a family of secretory proteins that induce a series of signals which results in the phosphorylation of β-catenin [59]. After activation, β-catenin enters the nucleus and promotes the transcription of Wnt target genes [59]. Wnt/β-catenin signalling is silent in normal adults. AOPPs induce NOX activation via plasma membrane receptor RAGE, which promotes the activation of the nuclear factor kappa B (NF-κB) transcription factor. The NF-κB transcription factor leads to the induction of Wnt ligands, such as Wnt1 and Wnt7a, and the activation of β-catenin [60]. Accumulating evidence suggests that Wnt/β-catenin has an important role in oxidative stress-induced podocyte damage and proteinuria [60]. Recently, it was demonstrated that a blockade of Wnt signalling preserves podocyte integrity and ameliorates proteinuria [60]. According to the mentioned data, targeting Wnt/β-catenin could be a new therapeutic modality for proteinuric CKD [60].
In the middle-aged general population, a marker of oxidative DNA damage, urinary 8-hydroxyguanosine (8-OHG) excretion, was independently associated with incident low-grade albuminuria during almost 6 years of follow-up [61].
Additionally, oxidative stress is also associated with progressive renal failure. Finnish-type congenital nephrotic syndrome (NPHS1) is a rare genetic kidney disease caused by mutations in the NPHS1 gene, which codes for the podocyte protein nephrin [62]. The disease is characterised by heavy proteinuria and hypoproteinaemia from birth [62]. In nephrectomised kidneys from children with NPHS1, interstitial expression of MPO was demonstrated [62]. This enzyme generates hypoclorous acid (HOCl), which causes irreversible tissue damage [62]. The concentration of free GSH in the cortex of the NPHS1 kidneys, which is a major antioxidant, was extremely low as compared to controls [62]. All these findings support the fact that proteinuric kidneys are under heavy oxidative stress.
In proteinuric CKD, tubulointerstitial injury with subsequent progressive loss of renal function is common. During urinary albumin endocytosis in the proximal tubule, protein kinase C-dependent NOX-mediated ROS generation is induced and this is responsible for enhanced NF-κB activity and the induction of NF-κB-dependent pathways of interstitial inflammation [63,64].
Less is known about the role of antioxidants in proteinuric CKD. Enzyme superoxide dismutase (SOD) protects the kidney from superoxide. Downregulation of cytosolic CuZn-SOD (SOD1) and extracellular CuZn-SOD (SOD3), but not mitochondrial Mn-SOD (SOD2), was observed in the kidney of KK/Ta-Akita mice that exhibit progressive DN [65]. In this study, no change in renal SOD expression in DN-resistant C57BL/6-Akita mice was observed [65]. In another study, a murine model of adriamycin-induced nephropathy was used. Levels of SOD3 diminished throughout the course of disease progression [66]. Interestingly, similar to findings in mice, a decrease in SOD3 in human CKD biopsy samples was found [66]. The authors concluded that SOD3 protects against proteinuric renal injury in vivo. It offers protection through the inhibition of NOX upregulation and downregulation of pathologic β-catenin signalling [66].
3.2. Oxidative Stress and Interstitial Fibrosis
Disregarding the initial injury, renal fibrosis is the common final pathway leading to ESRD, and the degree of fibrosis or fibroblast number are robust pathologic markers of progression [67]. Tubulointerstitial fibrosis includes the deposition of interstitial matrix with inflammatory cells, tubular cell loss, fibroblast accumulation, and rarefaction of the peritubular microvasculature [67]. Renal scarring is a result of complex interactions of molecular pathways, growth factors, cytokines, and cells [68,69,70,71].
Fibroblasts/myofibroblasts are most responsible for interstitial matrix accumulation and subsequent structural changes [72]. Collagen-producing myofibroblasts in the kidney can be derived from resident fibroblasts, pericytes, perivascular adventitial, epithelial, and/or endothelial sources [72]. Regardless of the origin of the cells, TGF-β1 is the main molecule responsible for myofibroblast activation with the expression of α-smooth muscle actin (α-SMA), which gives the myofibroblasts their contractility [72,73,74]. TGF-β1 increases the activity of NOX and expression of NOX2 and NOX4, homologues of the NOX family, indicating that this growth factor induces the production of ROS [74]. NOX2 and NOX4 have an important role in the conversion of fibroblasts to myofibroblasts [72,74]. It was shown that inhibition of NOX4 inhibited TGF-β-induced stimulation of NOX activity and reduced α-SMA expression [74]. Additionally, inhibition of TGF-β receptor type I reduced TGF-β-enhanced NOX activity and decreased expression of NOX4 and α-SMA [74].
As was shown, NOX synthesises ROS that are involved in fibrosis progression. On the other hand, their effect on renal disease progression is not well understood. In the model of chronic renal injury due to unilateral urinary obstruction, leading to renal fibrosis, wild-type and NOX4-deficient mice were used [75]. In the NOX4-deficient mice, more interstitial fibrosis was found in the obstructed kidney compared to the wild-type mice [75]. More TGF-β1-mediated tubular apoptosis, reduced expression of hypoxia-inducible factor-1α, and vascular endothelial growth factor was also found in the obstructed kidneys of the NOX4-deficient mice [75]. It was shown that the absence of NOX4 increases interstitial kidney fibrosis, independent of NOX2. [75]. NOX4 deficiency increased fibrosis due to enhanced tubular cell apoptosis, decreased microvascularisation, and enhanced oxidative stress [75]. The NOX4-mediated protection might be a consequence of Nrf2 pathway upregulation [76]. The Nrf2/Keap1 system controls the expression of antioxidant genes [76]. Furthermore, Nrf2 plays a protective role in CKD animal models, including DN [77,78].
Uraemic toxins are also involved in the progression of CKD. In the last decade, indoxyl sulphate (IS) and p-cresyl sulphate (PCS), which accumulate with CKD progression, have appeared as key nephrotoxins [79,80]. IS and PCS enhance ROS production in renal tubular cells, which activate the NF-kB pathway, resulting in both oxidative stress and inflammation [80,81]. These mechanisms have been confirmed in studies showing that fibrosis of renal tubules and oxidative stress are significantly enhanced after toxin administration and suppressed after IS reduction [80,81,82]. Additionally, it was shown that antioxidant treatment dose-dependently inhibits the fibrotic and oxidative effects of IS and PCS [83,84].
Recently, it was demonstrated that oxidative stress and autophagy are involved in kidney health and disease [85]. Autophagy is a crucial cellular homeostatic process that cells use to degrade and recycle cellular proteins and remove damaged organelles. It involves the formation of double membrane-bound vesicles called autophagosomes, which later fuse with lysosomes [86]. Basal levels of redox signalling and autophagy signalling are necessary to maintain cellular homeostasis. Under distinct circumstances, changes in autophagic flux have been shown to regulate ROS formation and redox signalling [85]. It is also suggested that ROS and RNS induce autophagy and vice versa [85,87].
3.3. Oxidative Stress and Microvascular Dysfunction
The endothelium is a fundamental layer in the arterial wall and is essential for the regulation and maintenance of normal renal function [43,44]. Oxidative stress is related to endothelial dysfunction and plays a critical role in CKD progression [44,45,88]. The endothelium secretes nitric oxide (NO), which is produced from arginine by the enzyme NOS [88]. NO is involved in several biological processes, including vasodilatation in smooth muscle cells, inflammation, and immune responses [88]. NOS is expressed as various isoforms: endothelial NOS (eNOS), neuronal NOS (nNOS), inducible NOS (iNOS), and constitutive NOS (cNOS); all have been isolated from the kidney [43,88,89]. The cNOS is expressed in the vessels, glomeruli, and tubules, iNOS is expressed in vascular smooth muscle cells and the mesangium, and eNOS is associated with the vascular endothelium [45,88,90]. Low levels of NO in the endothelium induce the expression of antioxidative genes and protect renal endothelial and mesangial cells from apoptosis and fibrosis but, on the other hand, increased levels of ROS reduce the production of NO via inhibition and/or uncoupling of NOS enzymes [45,88,89,90]. The NO production in the kidney can be blocked by NOS inhibition with asymmetric dimethylarginine (ADMA). ADMA is a natural product formed by the methylation of arginine which accumulates in the plasma of CKD patients in the early stages of CKD [45,89]. The decrease in NO leads to an increase in vascular resistance [89]. Additionally, it was shown in patients with CKD stages 1-5 that levels of serum ADMA and oxidative stress markers (plasma malondialdehyde (MDA), erythrocyte SOD, and GSH-Px) were directly associated with CKD stages [45]. It was shown that the glomerular filtration rate correlated negatively with plasma MDA and ADMA levels and positively with erythrocyte SOD and GSH-Px [45]. Patients with CKD, compared to a control group of healthy subjects, had higher levels of MDA and ADMA and lower levels of erythrocyte SOD and GSH-Px [45]. Furthermore, it was shown that levels of oxidative stress markers and ADMA are independently associated with endothelial function [45].
Autoregulation is important in maintaining renal blood flow, glomerular filtration rate, and tubular fluid flow over a wide range of perfusion pressures. It is dependent on afferent arteriole contraction followed by a tubuloglomerular feedback [91,92]. Impairment of renal autoregulation is associated with CKD progression. In experimental studies, it was documented that ROS mediate myogenic responses of afferent arterioles in CKD models [93]. It was also shown that NOX2 plays an important role in regulating tone and reactivity of afferent arterioles, also in response to angiotensin II (ANG II) and/or adenosine [94]. NOX2-derived ROS scavenges NO, causing subsequent NO deficiency [94]. It was demonstrated that an increase in perfusion pressure increases superoxide (O2•−) in afferent arterioles in normal mice or mice with a genetic deletion of SOD and is involved in the myogenic contractions of afferent arterioles [95,96]. H2O2 impaired autoregulation of afferent arterioles in five out of six nephrectomised mice [92,95,96].
3.4. Oxidative Stress and Chronic Inflammation
Oxidative stress and inflammation, as well as their interaction, have an important role in the pathogenesis and progression of CKD [97]. Both promote renal injury through damage of molecular components [98]. The primary pathological mechanism that links oxidative stress, inflammation, and CKD progression includes an initial injury to the kidney by intra- and extracellular oxygen-derived radicals and the resultant inflammation [98]. In recent years, some important review papers have been published showing the importance of inflammation in the pathogenesis and progression of CKD [16,20,23,43,99,100,101,102,103]. More details about the role of inflammation in CKD is beyond the scope of this review.
4. Biomarkers of Oxidative Stress in Patients with CKD
ROS are highly reactive and unstable compounds with short half-lives of only seconds. Using them as clinical biomarkers of oxidative stress is difficult or even impossible. ROS produce unwanted modifications to lipids, proteins, DNA, etc. These oxidation products have longer lifetimes and, together with antioxidants, are used to assess the redox state.
4.1. Lipid Peroxidation
Oxidation of polyunsaturated fatty acids (linoleic acid, arachidonic acid, etc.) by free radicals is known as lipid peroxidation and it can cause major tissue damage [104]. Lipids are the main component of cellular membranes and peroxidation alters their properties and consequently affects their function [105]. The most frequently studied lipid peroxidation markers are MDA, 4-hydroxynonenal (HNE), thiobarbituric acid reactive substances (TBARSs), and isoprostanes such as 8-iso-prostaglandin F2α (8-iso-PGF2α) [106,107,108].
MDA is formed through lipid peroxidation and during prostaglandin and thromboxane synthesis [105]. It can attack macromolecules, leading to alterations in their functions [105]. In several studies, higher serum MDA levels were found in CKD patients compared to healthy control subjects [109,110,111]. MDA correlated negatively with the glomerular filtration rate and was significantly different among CKD patients with stages 2, 3, 4, and 5 [31]. Higher levels of serum MDA were also found in haemodialysis patients [31,112]. In haemodialysis patients, the value of serum MDA is limited because it is a water-soluble low-molecular-weight product and could be removed by haemodialysis [105]. Serum MDA levels in transplant patients were significantly lower than in dialysis patients [113]. Furthermore, serum MDA decreased after kidney transplantation [114].
TBARSs are a nonspecific marker of lipid peroxidation, therefore, serum MDA or F2-isoprostanes are preferred alternatives. It was shown that the production of TBARSs was higher in advanced CKD stages and in haemodialysis patients [115].
F2-isoprostanes are lipid peroxidation products with a prostaglandin-like structure formed by the nonenzymatic oxidation of arachidonic acid, and could be detected in serum and urine samples [105]. The values of plasma F2-isoprostanes were higher in CKD patients and in ESRD patients (both haemodialysis and peritoneal dialysis) compared to control subjects [116,117,118]. F2-isoprostanes increased significantly as the CKD stage advanced and were inversely related to the glomerular filtration rate [119]. Moreover, F2-isoprostanes significantly decreased after kidney transplantation [120].
4.2. Protein Oxidation
Protein oxidation is a covalent modification induced directly by ROS and/or RNS or indirectly by reaction with secondary products of oxygen stress [107]. Oxidative modifications lead to changes in protein properties and the consequences are loss of enzymatic activity, altered cellular functions, interference with the creation of membrane potentials, and changes in the type and level of cellular proteins [121,122].
Protein tyrosine nitration is mediated by RNS such as peroxynitrite (ONOO−) and nitrogendioxide (NO2) and results in structural and functional changes, leading to altered cell homeostasis [123]. It was shown that nitrotyrosine was higher in haemodialysis patients compared to controls [124]. It is important to note that methods of detecting nitrotyrosine are quite costly and impractical for daily screening and analysis [123].
AOPPs and AGEs are markers of protein oxidation and proinflammatory mediators [107]. AOPPs are increased in CKD and ESRD patients and higher levels were found in dialysis patients [125]. All of them showed increased AOPP levels in comparison to age-matched controls [125]. It is important to note that AOPP levels are overestimated in patients with hypertriglyceridaemia [125].
AGEs, such as pentosidine, were increased in CKD and ESRD patients [126]. In nondialysis CKD patients, pentosidine was associated inversely with the glomerular filtration rate [126].
Protein carbonylation is the oxidation of proteins that can be promoted by ROS, and protein carbonyls are used as markers of oxidative stress. Plasma protein carbonyl levels were higher in CKD and haemodialysis patients compared to normal volunteers [127]. In this study, no significant difference in the plasma protein carbonyl group concentration between CKD patients and chronic haemodialysis patients was found [127]. Results from another study showed that carbonylation of albumin in CKD patients gradually increased during the development of the disease [128]. The carbonylation of albumin was even higher in the plasma of haemodialysis patients, while a comparison of peritoneal dialysis patients with controls found no difference [128]. Protein carbonyls were inversely related to the glomerular filtration rate and a significant reduction in plasma carbonyls after renal transplantation was documented [129].
4.3. Nucleic Acid Oxidation
Oxidative damage to DNA includes fragmentation products, single/double-strand breaks, inter/intra-strand cross-links, DNA protein cross-links, and DNA bases damage [107]. Sensitive biomarkers of DNA damage are 8-hydroxyguanosine (8-OHG) and 8-hydroxy-2′-deoxyguanosine (8-OHdG).
8-OHdG levels in peripheral leukocyte DNA were higher in CKD patients compared to healthy controls. The highest values were observed in peritoneal dialysis patients [130]. Furthermore, in nondialysed CKD patients, 8-OHdG levels inversely correlated with renal creatinine clearance [130]. An increased 8-OHdG level in leukocyte DNA was also found in haemodialysis patients [131]. They had the greatest 8-OHdG level, followed by undialysed CKD patients and healthy controls [131]. The 24 h urinary 8-OHdG excretion in patients with proteinuria was significantly higher than in the control subjects [132].
4.4. Antioxidants
An antioxidant is a substance that delays or inhibits cell damage caused by free radicals [133]. Total antioxidant status is determined by different measurement techniques and the results are difficult to compare across studies [107]. Patients with CKD, including haemodialysis patients, have diminished total antioxidant capacity [134,135]. It was reported that total antioxidant capacity was also lower in peritoneal dialysis patients [136].
The first line of enzymatic antioxidant defence is SOD, which dismutes superoxide hydrogen peroxide and molecular oxygen [107]. Results from studies examining SOD in CKD patients are contradictory and difficult to interpret [107]. Some authors found no significant difference in SOD between CKD patients and controls [88,137], while others found reduced SOD activity in haemodialysis and peritoneal dialysis patients compared to controls [138], or that plasma SOD activity increased in CKD patients with the progression of renal insufficiency [139]. On the other hand, plasma SOD values were lower in CKD patients than controls and the glomerular filtration rate correlated positively with SOD [31]. Erythrocyte SOD levels increased following renal transplantation [140]. The lack of consistency in SOD expression encourages careful interpretation of the results [107].
Catalase reduces H2O2 to water; selenium-containing GSH-Px reduces all organic lipid peroxides and requires GSH as a hydrogen donor [28,107]. Studies related to plasma or erythrocyte catalase and GSH-Px activity are conflicting and the results should be interpreted very carefully [88,135,138,139,141,142,143,144,145].
GSH, a tripeptide, is a major nonenzymatic antioxidant found in almost all living cells. It is considered as a biomarker of redox imbalance at the cellular level and its activity fluctuates less than other antioxidants, making it a more stable indicator of antioxidant status [107,137]. Plasma GSH was diminished in many studies, including CKD, haemodialysis, and peritoneal dialysis patients [144,146,147]. Interestingly, GSH concentration measured in erythrocytes showed contradictory results, it may either be decreased, unchanged, or even increased [148,149,150,151,152]. GSH is oxidised to glutathione disulphide (GSSG); GSSG and the GSH/GSSG ratio were used as markers of GSH-related activity in some studies [107,153].
5. Biomarkers of Oxidative Stress in Development and Progression of DN
Diabetes is the leading cause of CKD. The exact pathogenesis is complex and oxidative stress has a significant role in the pathogenesis of DN and its progression to ESRD. In recent years, a variety of biomarkers of oxidative stress associated with DN has been found and the most important ones used in clinical studies are presented (Table 2) [152,153,154,155,156,157,158,159,160,161,162,163,164,165,166,167,168,169,170,171,172,173,174,175,176,177,178,179,180,181,182,183,184,185,186].
5.1. Lipid Peroxidation
According to lipid peroxidation markers, an increase in MDA or TBARSs in type 2 diabetic patients with and without complications compared to healthy controls is one of the most consistent findings [105]. Furthermore, a significant increase in MDA and TBARSs in type 2 diabetic patients with micro- and macrovascular complications compared to those without was reported [154,155,156]. In these studies, up to 40% of patients with microvascular complications had DN. Unfortunately, patients with DN were not analysed separately. In type 2 diabetic patients with DN, it was shown that MDA was significantly higher in patients with DN compared to patients without DN and healthy controls [157,158,159]. Meanwhile, other studies reported no difference in MDA between patients with or without DN [160,161].
A significant increase in urinary and plasma levels of total F2-isoprostanes was found in type 2 diabetic patients with DN compared to controls [162].
5.2. Protein Oxidation
AOPPs were higher in type 2 diabetic patients compared to controls [154,156,163,164]. AOPPs were increased in patients with micro- or macrovascular complications (including DN) compared to those without them [154,156,163,164]. Patients with DN were not analysed separately in these studies. It was documented that diabetic patients with albuminuria had increased AOPP levels compared to those without albuminuria [165].
Plasma AGE levels were higher in type 2 diabetic patients compared to healthy controls and in type 2 diabetic patients with micro- or macrovascular complications (including DN) compared to those without complications [156,159,163,166,167]. In another study, AGEs were significantly higher only in type 2 diabetic patients with chronic renal failure (defined as creatinine ≥ 1.3 mg/dL) compared to patients with normo-, micro-, and macroalbuminuria without renal failure [168]. On the contrary, no difference was found in AGEs when comparing type 2 diabetic patients with or without nephropathy [161].
In type 1 diabetic patients, serum levels of AGEs were significantly increased as normal renal status advanced to microalbuminuria, clinical nephropathy, and haemodialysis; serum levels of AGEs positively correlated with urinary albumin excretion [169].
Protein carbonyls were also higher in type 2 diabetic patients compared to healthy controls and in type 2 diabetic patients with micro- or macrovascular complications (including DN) compared to those without complications [154,156,163,164]. Furthermore, increased levels of plasma and lymphocyte carbonyls were found in type 2 diabetic patients with DN compared to healthy controls [162].
5.3. Nucleic Acid Oxidation
Increased serum and urinary 8-OHdG in type 2 diabetic patients was documented compared to controls [158,170,171]. Increased serum and plasma 8-OHdG was documented in type 2 diabetic patients with DN compared to diabetic patients without complications [158,172]. It was also found that plasma 8-OHdG levels in diabetic patients with micro- and macroalbuminuria were increased compared to normoalbuminuric patients [161]. Moreover, urinary 8-OHdG levels were significantly higher in patients with microvascular complications, including DN, compared to those without complications [173]. Urinary 8-OHdG levels in type 2 diabetic patients were significantly higher in patients with macroalbuminuria compared to patients with micro- or normoalbuminuria [132,174]. Additionally, urinary 8-OHdG levels were increased in type 2 diabetic patients with micro- and macroalbuminuria compared to patients with normoalbuminuria and healthy controls; 8-OHdG levels were also significantly higher in patients with macroalbuminuria compared to patients with microalbuminuria [175]. In a prospective longitudinal study, patients with higher urinary excretion of 8-OHdG had a significant progression of DN compared to patients with moderate or lower excretion of 8-OHdG [176]. In this study, multivariate logistic regression analysis suggested that urinary 8-OHdG was the strongest predictor of nephropathy among several known risk factors [176]. Interestingly, no significant association between leukocyte 8-OHdG and the development of nephropathy was found [176]. On the other hand, no difference was found in urinary 8-OHdG levels in type 2 diabetic patients with or without DN [170]. Furthermore, an RNA oxidation marker, urinary 8-OHG, was also elevated in type 2 diabetic patients with and without complications compared to age-matched healthy controls [171].
In long-standing type 1 diabetic patients, higher plasma 8-OHdG levels were independently associated with increased risk of DN [177].
5.4. Antioxidants
Conflicting results have been reported about total antioxidant status in type 2 diabetic patients; it was reduced [154,157,164,178,179], increased [180], or unchanged [181] compared to controls.
Results from studies examining SOD in type 2 diabetic patients are contradictory, results showed either increased [179,182] or decreased [178,183] SOD activity compared to healthy controls. Studies related to catalase and GSH-Px activity in type 2 diabetic patients compared to healthy controls are also conflicting [105]. Inconsistent results on SOD, catalase, and GSH-Px were also reported in studies comparing type 2 diabetic patients with or without complications [154,155,184,185]. Among patients with complications, patients with DN were also included, but were not analysed separately in these studies. In study by Bondor et al., patients with incipient diabetes-associated nephropathy (defined as estimated glomerular filtration rate (eGFR) < 60 mL/min or urine albumin-to-creatinine ratio (UACR) ≥ 30 mg/g) were included [139]. No difference in SOD activity in patients with or without DN was found [160]. Similar results were shown in other studies [158,161].
No difference in catalase and GSH-Px levels in type 2 diabetic patients with DN compared to those without was found [161,186]. In patients with type 1 diabetes, associations between catalase allelic variations and the prevalence and incidence of DN and ESRD were observed [187].
Haem oxygenases (HOs) are fundamental enzymes in haem catabolism [188]. The HO-1 isoform acts as an antioxidant during oxidative injury [189]. Plasma HO-1 concentrations were significantly increased in newly diagnosed type 2 diabetic patients compared to controls [190].
Furthermore, urinary HO-1 levels were significantly increased in diabetic patients with micro- and macroalbuminuria compared to patients with normoalbuminuria and controls [191]. In patients with normoalbuminuria, urinary HO-1 levels were also higher compared to controls [191]. HO-1 was upregulated in lymphocytes in DN patients compared to healthy controls [162].
GSH was decreased in type 2 diabetic patients compared to controls [179,181,183]. Decreased GSH was reported in type 2 diabetic patients with complications (including DN) compared to those without [154]. Furthermore, comparing type 2 diabetic patients with and without DN, plasma GSH was significantly decreased in patients with nephropathy [157]. Interestingly, in the study by Chou et al., no difference in cellular GSH was found in type 2 diabetic patients with and without DN [161]. In the same study, patients with the highest UACR had the lowest levels of vitamin C and vitamin C levels, which correlated negatively with serum creatinine, urine albumin, and UACR [161].
6. Antioxidant Therapy
Oxidative stress is involved in the onset and progression of CKD, including DN. Therefore, antioxidant therapy could be an important treatment strategy in these patients. Experimental studies showed beneficial effects of antioxidant therapy in animals [192,193,194,195,196]. Results of antioxidant therapy use in patients with CKD or DN are limited with conflicting results. As shown by a Cochrane database systematic review (including therapy with vitamin E, coenzyme Q, acetylcysteine, bardoxolone methyl, and human recombinant superoxide dismutase), the results of antioxidant therapy have been disappointing in reducing the risk of cardiovascular and all-cause death or major cardiovascular events in CKD patients [197]. However, the authors concluded that current evidence suggests that antioxidant therapy in predialysis CKD patients may prevent progression to ESRD; this finding was based on a very small number of events [197]. Some important review papers have been published in recent years, presenting details of antioxidant therapy for CKD and DN [17,23,43,198,199]. Recently, new medications with antioxidant effects (sacubitril/valsartan, etc.) have come into the spotlight and future clinical trials will determine the efficacy of these or other new drugs in modulating the pro-oxidant milieu of CKD [43,200,201].
7. Conclusions
Despite the aggressive blockade of the renin–angiotensin–aldosterone system, many patients with diabetes still progress to ESRD. Oxidative stress is important in the development and progression of DN. A number of pathways and molecules are involved in the induction of oxidative stress in DN. The identification of biomarkers of oxidative stress contributes to our understanding of the development and progression of DN toward ESRD. In this review, we have presented oxidative stress biomarkers used in clinical studies in patients with CKD and DN. To date, these novel biomarkers of oxidative stress cannot replace currently used biomarkers in DN development and progression (eGFR, albuminuria/proteinuria).
Author Contributions
N.V.H and R.H.: writing—original draft preparation; N.V.H., S.B., R.E. and R.H.: writing—review and editing. All authors have read and agreed to the published version of the manuscript.
Funding
This work received no external funding.
Conflicts of Interest
The authors declare no conflict of interest.
References
- Jha, V.; Garcia-Garcia, G.; Iseki, K.; Li, Z.; Naicker, S.; Plattner, B.; Saran, R.; Wang, A.Y.; Yang, C. Chronic kidney disease: Global dimension and perspectives. Lancet 2013, 382, 260–272. [Google Scholar] [CrossRef]
- Elshahat, S.; Cockwell, P.; Maxwell, A.P.; Griffin, M.; O’Brien, T.; O’Neill, C. The impact of chronic kidney disease on developed countries from a health economics perspective: A systematic scoping review. PLoS ONE 2020, 15, e0230512. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Foreman, K.J.; Marquez, N.; Dolgert, A.; Fukutaki, K.; Fullman, N.; McGaughey, M.; Pletcher, M.A.; Smith, A.E.; Tang, K.; Yuan, C.; et al. Forecasting life expectancy, years of life lost, and all-cause and cause-specific mortality for 250 causes of death: Reference and alternative scenarios for 2016–40 for 195 countries and territories. Lancet 2018, 392, 2052–2090. [Google Scholar] [CrossRef] [Green Version]
- Alicic, R.Z.; Rooney, M.T.; Tuttle, K.R. Diabetic kidney disease: Challenges, progress, and possibilities. Clin. J. Am. Soc. Nephrol. 2017, 12, 2032–2045. [Google Scholar] [CrossRef] [PubMed]
- Tuttle, K.R.; Alicic, R.Z.; Duru, O.K.; Jones, C.R.; Daratha, K.B.; Nicholas, S.B.; McPherson, S.M.; Neumiller, J.J.; Bell, D.S.; Mangione, C.M.; et al. Clinical characteristics of and risk factors for chronic kidney disease among adults and children: An analysis of the CURE-CKD registry. JAMA Netw. Open 2019, 2, e1918169. [Google Scholar] [CrossRef] [PubMed]
- IDF Diabetes Atlas. Available online: https://www.diabetesatlas.org/en/ (accessed on 11 June 2020).
- MacIsaac, R.J.; Ekinci, E.I.; Jerums, G. Markers of and risk factors for the development and progression of diabetic kidney disease. Am. J. Kidney Dis. 2014, 63 (Suppl. S2), S39–S62. [Google Scholar] [CrossRef]
- Cornec-Le Gall, E.; Alam, A.; Perrone, R.D. Autosomal dominant polycystic kidney disease. Lancet 2019, 393, 919–935. [Google Scholar] [CrossRef]
- Saha, S.K.; Lee, S.B.; Won, J.; Choi, H.Y.; Kim, K.; Yang, G.; Dayem, A.A.; Cho, S. Correlation between oxidative stress, nutrition, and cancer initiation. Int. J. Mol. Sci. 2017, 18, 1544. [Google Scholar] [CrossRef] [Green Version]
- Forcados, G.E.; James, D.B.; Sallau, A.B.; Muhammad, A.; Mabeta, P. Oxidative stress and carcinogenesis: Potential of phytochemicals in breast cancer therapy. Nutr. Cancer 2017, 69, 365–374. [Google Scholar] [CrossRef] [Green Version]
- Taniyama, Y.; Griendling, K.K. Reactive oxygen species in the vasculature. Hypertension 2003, 42, 1075–1081. [Google Scholar] [CrossRef] [Green Version]
- Jenner, P. Oxidative stress in Parkinson’s disease. Ann. Neurol. 2003, 53, S26–S36. [Google Scholar] [CrossRef] [PubMed]
- Kasparova, S.; Brezova, V.; Valko, M.; Horecky, J.; Mlynarik, V.; Liptaj, T.; Vancová, O.; Ulicná, O.; Dobrota, D. Study of the oxidative stress in a rat model of chronic brain hypoperfusion. Neurochem. Int. 2005, 46, 601–611. [Google Scholar] [CrossRef] [PubMed]
- Dhalla, N.S.; Temsah, R.M.; Netticadan, T. Role of oxidative stress in cardiovascular diseases. J. Hypertens. 2000, 18, 655–673. [Google Scholar] [CrossRef] [PubMed]
- Fitzpatrick, A.M.; Teague, W.G.; Holguin, F.; Yeh, M.; Brown, L.A. Severe Asthma Research Program. Airway glutathione homeostasis is altered in children with severe asthma: Evidence for oxidant stress. J. Allergy Clin. Immunol. 2009, 123, 146–152. [Google Scholar] [CrossRef] [Green Version]
- Elmarakby, A.A.; Sullivan, J.C. Relationship between oxidative stress and inflammatory cytokines in diabetic nephropathy. Cardiovasc. Ther. 2012, 30, 49–59. [Google Scholar] [CrossRef]
- Rochette, L.; Zeller, M.; Cottin, Y.; Vergely, C. Diabetes, oxidative stress and therapeutic strategies. Biochim. Biophys. Acta 2014, 1840, 2709–2729. [Google Scholar] [CrossRef] [PubMed]
- Brown, W.V. Microvascular complications of diabetes mellitus: Renal protection accompanies cardiovascular protection. Am. J. Cardiol. 2008, 102, 10L–13L. [Google Scholar] [CrossRef]
- Wu, J.; Mei, C.; Vlassara, H.; Striker, G.E.; Zheng, F. Oxidative stress-induced JNK activation contributes to proinflammatory phenotype of aging diabetic mesangial cells. Am. J. Physiol. Renal Physiol. 2009, 297, F1622–F1631. [Google Scholar] [CrossRef] [Green Version]
- García-García, P.M.; Getino-Melián, M.A.; Domínguez-Pimentel, V.; Navarro-González, J.F. Inflammation in diabetic kidney disease. World J. Diabetes 2014, 5, 431–443. [Google Scholar] [CrossRef]
- Wolf, G. New insights into the pathophysiology of diabetic nephropathy: From hemodynamics to molecular pathology. Eur. J. Clin. Investig. 2004, 34, 785–796. [Google Scholar] [CrossRef]
- Kanwar, Y.S.; Wada, J.; Sun, L.; Xie, P.; Wallner, E.I.; Chen, S.; Chugh, S.; Danesh, F.R. Diabetic nephropathy: Mechanisms of renal disease progression. Exp. Biol. Med. 2008, 233, 4–11. [Google Scholar] [CrossRef]
- Daenen, K.; Andries, A.; Mekahli, D.; Van Schepdael, A.; Jouret, F.; Bammens, B. Oxidative stress in chronic kidney disease. Pediatr. Nephrol. 2019, 34, 975–991. [Google Scholar] [CrossRef] [Green Version]
- Pizzino, G.; Irrera, N.; Cucinotta, M.; Pallio, G.; Mannino, F.; Arcoraci, V.; Squadrito, F.; Altavilla, D.; Bitto, A. Oxidative Stress: Harms and Benefits for Human Health. Oxid. Med. Cell. Longev. 2017, 2017, 8416763. [Google Scholar] [CrossRef] [PubMed]
- Birben, E.; Sahiner, U.M.; Sackesen, C.; Erzurum, S.; Kalayci, O. Oxidative stress and antioxidant defense. World Allergy Organ. J. 2012, 5, 9–19. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Harman, D. The aging process. Proc. Natl. Acad. Sci. USA 1981, 78, 7124–7128. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gyurászová, M.; Gurecká, R.; Bábíčková, J.; Tóthová, Ľ. Oxidative stress in the pathophysiology of kidney disease: Implications for noninvasive monitoring and identification of biomarkers. Oxid. Med. Cell. Longev. 2020, 2020, 5478708. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Locatelli, F.; Canaud, B.; Eckardt, K.; Stenvinkel, P.; Wanner, C.; Zoccali, C. Oxidative stress in end-stage renal disease: An emerging threat to patient outcome. Nephrol. Dial. Transplant. 2003, 18, 1272–1280. [Google Scholar] [CrossRef] [PubMed]
- Di Meo, S.; Reed, T.T.; Venditti, P.; Victor, V.M. Role of ROS and RNS sources in physiological and pathological conditions. Oxid. Med. Cell. Longev. 2016, 2016, 1–44. [Google Scholar] [CrossRef] [PubMed]
- Zelko, I.N.; Mariani, T.J.; Folz, R.J. Superoxide dismutase multigene family: A comparison of the CuZn-SOD (SOD1), Mn-SOD (SOD2), and EC-SOD (SOD3) gene structures, evolution, and expression. Free Radic. Biol. Med. 2002, 33, 337–349. [Google Scholar] [CrossRef]
- Kirkman, H.N.; Rolfo, M.; Ferraris, A.M.; Gaetani, G.F. Mechanisms of protection of catalase by NADPH. Kinetics and stoichiometry. J. Biol. Chem. 1999, 274, 13908–13914. [Google Scholar] [CrossRef] [Green Version]
- Gonzalez-Sanchez, E.; Perez, M.J.; Nytofte, N.S.; Briz, O.; Monte, M.J.; Lozano, E.; Serrano, M.A.; Marin, J.J. Protective role of biliverdin against bile acid-induced oxidative stress in liver cells. Free Radic. Biol. Med. 2016, 97, 466–477. [Google Scholar] [CrossRef]
- Abraham, N.G.; Kappas, A. Heme oxygenase and the cardiovascular-renal system. Free Radic. Biol. Med. 2005, 39, 1–25. [Google Scholar] [CrossRef] [PubMed]
- Gromer, S.; Urig, S.; Becker, K. The thioredoxin system: From science to clinic. Med. Res. Rev. 2004, 24, 40–89. [Google Scholar] [CrossRef] [PubMed]
- Masella, R.; Di Benedetto, R.; Vari, R.; Filesi, C.; Giovannini, C. Novel mechanisms of natural antioxidant compounds in biological systems: Involvement of glutathione and glutathione-related enzymes. J. Nutr. Biochem. 2005, 16, 577–586. [Google Scholar] [CrossRef]
- Corpe, C.; Dutta, A.; Dutta, S.K.; Levine, M. Vitamin C as an antioxidant: Evaluation of its role in disease prevention. J. Am. Coll. Nutr. 2003, 22, 18–35. [Google Scholar]
- El-Agamey, A.; Lowe, G.M.; McGarvey, D.J.; Mortensen, A.; Phillip, D.M.; Truscott, T.G. Carotenoid radical chemistry and antioxidant/pro-oxidant properties. Arch. Biochem. Biophys. 2004, 430, 37–48. [Google Scholar] [CrossRef]
- Roche, M.; Rondeau, P.; Singh, N.R.; Tarnus, E.; Bourdon, E. The antioxidant properties of serum albumin. FEBS Lett. 2008, 582, 1783–1787. [Google Scholar] [CrossRef]
- Pandey, K.B.; Rizvi, S.I. Plant polyphenols as dietary antioxidants in human health and disease. Oxid. Med. Cell. Longev. 2009, 2, 270–278. [Google Scholar] [CrossRef] [Green Version]
- Sifuentes-Franco, S.; Padilla-Tejeda, D.E.; Carrillo-Ibarra, S.; Miranda-Díaz, A.G. Oxidative stress, apoptosis, and mitochondrial function in diabetic nephropathy. Int. J. Endocrinol. 2018, 2018, 1875870. [Google Scholar] [CrossRef]
- Ceriello, A.; Morocutti, A.; Mercuri, F.; Quagliaro, L.; Moro, M.; Damante, G.; Viberti, G.G. Defective intracellular antioxidant enzyme production in type 1 diabetic patients with nephropathy. Diabetes 2000, 49, 2170–2177. [Google Scholar] [CrossRef] [Green Version]
- Baynes, J.W.; Thorpe, S.R. Role of oxidative stress in diabetic complications: A new perspective on an old paradigm. Diabetes 1999, 48, 1–9. [Google Scholar] [CrossRef] [PubMed]
- Duni, A.; Liakopoulos, V.; Roumeliotis, S.; Peschos, D.; Dounousi, E. Oxidative Stress in the Pathogenesis and Evolution of Chronic Kidney Disease: Untangling Ariadne’s Thread. Int. J. Mol. Sci. 2019, 20, 3711. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zoccali, C. The endothelium as a target in renal diseases. J. Nephrol. 2007, 20, S39–S44. [Google Scholar] [PubMed]
- Yilmaz, M.I.; Saglam, M.; Caglar, K.; Cakir, E.; Sonmez, A.; Ozgurtas, T.; Aydin, A.; Eyileten, T.; Ozcan, O.; Acikel, C.; et al. The determinants of endothelial dysfunction in CKD: Oxidative stress and asymmetric dimethylarginine. Am. J. Kidney Dis. 2006, 47, 42–50. [Google Scholar] [CrossRef]
- Kielstein, J.T.; Böger, R.H.; Bode-Böger, S.M.; Frölich, J.C.; Haller, H.; Ritz, E.; Fliser, D. Marked increase of asymmetric dimethylarginine in patients with incipient primary chronic renal disease. J. Am. Soc. Nephrol. 2002, 13, 170–176. [Google Scholar]
- Nagata, M. Podocyte injury and its consequences. Kidney Int. 2016, 89, 1221–1230. [Google Scholar] [CrossRef]
- Coresh, J.; Heerspink, H.J.L.; Sang, Y.; Matsushita, K.; Arnlov, J.; Astor, B.C.; Black, C.; Brunskill, N.J.; Carrero, J.J.; Feldman, H.I.; et al. Change in albuminuria and subsequent risk of end-stage kidney disease: An individual participant-level consortium meta-analysis of observational studies. Lancet Diabetes Endocrinol. 2019, 7, 115–127. [Google Scholar] [CrossRef]
- Levin, A.; Stevens, P.E.; Bilous, R.W.; Coresh, J.; De Francisco, A.L.; De Jong, P.E.; Griffith, K.E.; Hemmelgarn, B.R.; Iseki, K.; Lamb, E.J.; et al. Kidney Disease: Improving Global Outcomes (KDIGO) CKD work group. KDIGO 2012 clinical practice guideline for the evaluation and management of chronic kidney disease. Kidney Int. Suppl. 2013, 3, 1–150. [Google Scholar]
- Gwinner, W.; Landmesser, U.; Brandes, R.P.; Kubat, B.; Plasger, J.; Eberhard, O.; Koch, K.M.; Olbricht, C.J. Reactive oxygen species and antioxidant defense in puromycin aminonucleoside glomerulopathy. J. Am. Soc. Nephrol. 1997, 8, 1722–1731. [Google Scholar]
- Ricardo, S.D.; Bertram, J.F.; Ryan, G.B. Antioxidants protect podocyte foot processes in puromycin aminonucleoside-treated rats. J. Am. Soc. Nephrol. 1994, 4, 1974–1986. [Google Scholar]
- Marshall, C.B.; Pippin, J.W.; Krofft, R.D.; Shankland, S.J. Puromycin aminonucleoside induces oxidant-dependent DNA damage in podocytes in vitro and in vivo. Kidney Int. 2006, 70, 1962–1973. [Google Scholar] [CrossRef] [Green Version]
- Bottinger, E.P. TGF-β in renal injury and disease. Semin. Nephrol. 2007, 27, 309–320. [Google Scholar] [CrossRef]
- Daehn, I.; Casalena, G.; Zhang, T.; Shi, S.; Fenninger, F.; Barasch, N.; Yu, L.; D’Agati, V.; Schlondorff, D.; Kriz, W.; et al. Endothelial mitochondrial oxidative stress determines podocyte depletion in segmental glomerulosclerosis. J. Clin. Investig. 2014, 124, 1608–1621. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Witko-Sarsat, V.; Friedlander, M.; Capeillère-Blandin, C.; Nguyen-Khoa, T.; Nguyen, A.T.; Zingraff, J.; Jungers, P.; Descamps-Latscha, B. Advanced oxidation protein products as a novel marker of oxidative stressin uremia. Kidney Int. 1996, 49, 1304–1313. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Witko-Sarsat, V.; Gausson, V.; Descamps-Latscha, B. Are advanced oxidation protein products potential uremic toxins? Kidney Int. Suppl. 2003, 84, S11–S14. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zhou, L.L.; Hou, F.F.; Wang, G.B.; Yang, F.; Xie, D.; Wang, Y.P.; Tian, J.W. Accumulation of advanced oxidation protein products induces podocyte apoptosis and depletion through NADPH dependent mechanisms. Kidney Int. 2009, 76, 1148–1160. [Google Scholar] [CrossRef] [Green Version]
- Zhou, L.L.; Cao, W.; Xie, C.; Tian, J.; Zhou, Z.; Zhou, Q.; Zhu, P.; Li, A.; Liu, Y.; Miyata, T.; et al. The receptor of advanced glycation end products plays a central role in advanced oxidation protein products-induced podocyte apoptosis. Kidney Int. 2012, 82, 759–770. [Google Scholar] [CrossRef] [Green Version]
- Zhou, L.; Liu, Y. Wnt/β-catenin signaling and podocyte dysfunction in proteinuric kidney disease. Nat. Rev. Nephrol. 2015, 11, 535–545. [Google Scholar] [CrossRef]
- Zhou, L.; Chen, X.; Lu, M.; Wu, Q.; Yuan, Q.; Hu, C.; Miao, J.; Zhang, Y.; Li, H.; Hou, F.F.; et al. Wnt/β-catenin links oxidative stress to podocyte injury and proteinuria. Kidney Int. 2019, 95, 830–845. [Google Scholar] [CrossRef]
- Schei, J.; Fuskevåg, O.M.; Stefansson, V.T.N.; Solbu, M.D.; Jenssen, T.G.; Eriksen, B.O.; Melsom, T. Urinary markers of oxidative stress Are Associated with Albuminuria but Not GFR Decline. Kidney Int. Rep. 2017, 3, 573–582. [Google Scholar] [CrossRef] [Green Version]
- Kuusniemi, A.M.; Lapatto, R.; Holmberg, C.; Karikoski, R.; Rapola, J.; Jalanko, H. Kidneys with heavy proteinuria show fibrosis, inflammation, and oxidative stress, but no tubular phenotypic change. Kidney Int. 2005, 68, 121–132. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Morigi, M.; Macconi, D.; Zoja, C.; Donadelli, R.; Buelli, S.; Zanchi, C.; Ghilardi, M.; Remuzzi, G. Protein overload-induced NF-kappaB activation in proximal tubular cells requires H2O2 through a PKC-dependent pathway. J. Am. Soc. Nephrol. 2002, 13, 1179–1189. [Google Scholar]
- Souma, T.; Abe, M.; Moriguchi, T.; Takai, J.; Yanagisawa-Miyazawa, N.; Shibata, E.; Akiyama, Y.; Toyohara, T.; Suzuki, T.; Tanemoto, M.; et al. Luminl alkalinization attenuates proteinuria induced oxidative damage in proximal tubular cells. J. Am. Soc. Nephrol. 2011, 22, 635–648. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Fujita, H.; Fujishima, H.; Chida, S.; Takahashi, K.; Qi, Z.; Kanetsuna, Y.; Breyer, M.D.; Harris, R.C.; Yamada, Y.; Takahashi, T. Reduction of renal superoxide dismutase in progressive diabetic nephropathy. J. Am. Soc. Nephrol. 2009, 20, 1303–1313. [Google Scholar] [CrossRef] [Green Version]
- Tan, R.J.; Zhou, D.; Xiao, L.; Zhou, L.; Li, Y.; Bastacky, S.I.; Oury, T.D.; Liu, Y. Extracellular superoxide dismutase protects against proteinuric kidney disease. J. Am. Soc. Nephrol. 2015, 26, 2447–2459. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zeisberg, M.; Neilson, E.G. Mechanisms of tubulointerstitial fibrosis. J. Am. Soc. Nephrol. 2010, 21, 1819–1834. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Djudjaj, S.; Boor, P. Cellular and molecular mechanisms of kidney fibrosis. Mol. Asp. Med. 2019, 65, 16–36. [Google Scholar] [CrossRef]
- Tampe, B.; Zeisberg, M. Contribution of genetics and epigenetics to progression of kidney fibrosis. Nephrol. Dial. Transplant. 2014, 29, iv72–iv79. [Google Scholar] [CrossRef] [Green Version]
- Lv, W.; Booz, G.W.; Fan, F.; Wang, Y.; Roman, R.J. Oxidative stress and renal fibrosis: Recent insights for the development of novel therapeutic strategies. Front. Physiol. 2018, 16, 105. [Google Scholar] [CrossRef] [Green Version]
- Okamura, D.M.; Pennathur, S. The balance of powers: Redox regulation of fibrogenic pathways in kidney injury. Redox Biol. 2015, 6, 495–504. [Google Scholar] [CrossRef] [Green Version]
- Barnes, J.L.; Gorin, Y. Myofibroblast diferentiation during fibrosis: Role of NAD(P)H oxidases. Kidney Int. 2011, 79, 944–956. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mack, M.; Yanagita, M. Origin of myofibroblasts and cellular events triggering fibrosis. Kidney Int. 2015, 87, 297–307. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bondi, C.D.; Manickam, N.; Lee, D.Y.; Block, K.; Gorin, Y.; Abboud, H.E.; Barnes, J.L. NAD(P)H oxidase mediates TGF-beta1 induced activation of kidney myofibroblasts. J. Am. Soc. Nephrol. 2010, 21, 93–102. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Nlandu Khodo, S.; Dizin, E.; Sossauer, G.; Szanto, I.; Martin, P.Y.; Feraille, E.; Krause, K.H.; de Seigneux, S. NADPH oxidase 4 protects against kidney fibrosis during chronic renal injury. J. Am. Soc. Nephrol. 2012, 23, 1967–1976. [Google Scholar] [CrossRef] [Green Version]
- Zoja, C.; Benigni, A.; Remuzzi, G. The Nrf2 pathway in the progression of renal disease. Nephrol. Dial. Transplant. 2014, 29, i19–i24. [Google Scholar] [CrossRef] [Green Version]
- Choi, B.H.; Kang, K.S.; Kwak, M.K. Effect of redox modulating NRF2 activators on chronic kidney disease. Molecules 2014, 19, 12727–12759. [Google Scholar] [CrossRef] [Green Version]
- Soetikno, V.; Sari, F.R.; Lakshmanan, A.P.; Arumugam, S.; Harima, M.; Suzuki, K. Curcumin alleviates oxidative stress, inflammation, and renal fibrosis in remnant kidney through the Nrf2-keap1 pathway. Mol. Nutr. Food Res. 2013, 57, 1649–1659. [Google Scholar] [CrossRef]
- Meijers, B.K.I.; Evenepoel, P. The gut-kidney axis: Indoxyl sulfate, p-cresyl sulfate and CKD progression. Nephrol. Dial. Transplant. 2011, 26, 759–761. [Google Scholar] [CrossRef]
- Rossi, M.; Campbell, K.L.; Johnson, D.W.; Stanton, T.; Vesey, D.A.; Coombes, J.S.; Weston, K.S.; Hawley, C.M.; McWhinney, B.C.; Ungerer, J.P.; et al. Protein-bound uremic toxins, inflammation and oxidative stress: A cross-sectional study in stage 3–4 chronic kidney disease. Arch. Med. Res. 2014, 45, 309–317. [Google Scholar] [CrossRef]
- Watanabe, H.; Miyamoto, Y.; Honda, D.; Tanaka, H.; Wu, Q.; Endo, M.; Noguchi, T.; Kadowaki, D.; Ishima, Y.; Kotani, S.; et al. p-Cresyl sulfate causes renal tubular cell damage by inducing oxidative stress by activation of NADPH oxidase. Kidney Int. 2013, 83, 582–592. [Google Scholar] [CrossRef] [Green Version]
- Lekawanvijit, S.; Kompa, A.R.; Manabe, M.; Wang, B.H.; Langham, R.G.; Nishijima, F.; Kelly, D.J.; Krum, H. Chronic kidney disease-induced cardiac fibrosis is ameliorated by reducing circulating levels of a non-dialysable uremic toxin, indoxyl sulfate. PLoS ONE 2012, 7, e41281. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Motojima, M.; Hosokawa, A.; Yamato, H.; Muraki, T.; Yoshioka, T. Uremic toxins of organic anions up-regulate PAI-1 expression by induction of NF-kappaB and free radical in proximal tubular cells. Kidney Int. 2003, 63, 1671–1680. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Yu, M.; Kim, Y.J.; Kang, D.H. Indoxyl sulfate-induced endothelial dysfunction in patients with chronic kidney disease via an induction of oxidative stress. Clin. J. Am. Soc. Nephrol. 2011, 6, 30–39. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sureshbabu, A.; Ryter, S.W.; Choi, M.E. Oxidative stress and autophagy: Crucial modulators of kidney injury. Redox Biol. 2015, 4, 208–214. [Google Scholar] [CrossRef] [Green Version]
- Xie, Z.; Klionsky, D.J. Autophagosome formation: Core machinery and adaptations. Nat. Cell. Biol. 2007, 9, 1102–1109. [Google Scholar] [CrossRef]
- Scherz-Shouval, R.; Elazar, Z. ROS, mitochondria and the regulation of autophagy. Trends Cell Biol. 2007, 17, 422–427. [Google Scholar] [CrossRef]
- Modlinger, P.S.; Wilcox, C.S.; Aslam, S. Nitric oxide, oxidative stress, and progression of chronic renal failure. Semin. Nephrol. 2004, 24, 354–365. [Google Scholar] [CrossRef]
- Aldámiz-Echevarría, L.; Andrade, F. Asymmetric dimethylarginine, endothelial dysfunction and renal disease. Int. J. Mol. Sci. 2012, 13, 11288–11311. [Google Scholar] [CrossRef] [Green Version]
- Sullivan, J.C.; Pollock, J.S. Coupled and uncoupled NOS: Separate but equal? Uncoupled NOS in endothelial cells is a critical pathway for intracellular signaling. Circ. Res. 2006, 98, 717–719. [Google Scholar] [CrossRef] [Green Version]
- Just, A. Mechanisms of renal blood flow autoregulation: Dynamics and contributions. Am. J. Physiol. Regul. Integr. Comp. Physiol. 2007, 292, R1–R17. [Google Scholar] [CrossRef]
- Lai, E.Y.; Wellstein, A.; Welch, W.J.; Wilcox, C.S. Superoxide modulates myogenic contractions of mouse afferent arterioles. Hypertension 2011, 58, 650–656. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Li, L.; Lai, E.Y.; Luo, Z.; Solis, G.; Griendling, K.K.; Taylor, W.R.; Jose, P.A.; Wellstein, A.; Welch, W.J.; Wilcox, C.S. Superoxide and hydrogen peroxide counterregulate myogenic contractions in renal afferent arterioles from a mouse model of chronic kidney disease. Kidney Int. 2017, 92, 625–633. [Google Scholar] [CrossRef] [PubMed]
- Carlström, M.; Lai, E.Y.; Ma, Z.; Patzak, A.; Brown, R.D.; Persson, A.E. Role of NOX2 in the regulation of afferent arteriole responsiveness. Am. J. Physiol. Regul. Integr. Comp. Physiol. 2009, 296, R72–R79. [Google Scholar] [CrossRef]
- Li, L.; Lai, E.Y.; Wellstein, A.; Welch, W.J.; Wilcox, C.S. Differential effects of superoxide and hydrogen peroxide on myogenic signaling, membrane potential, and contractions of mouse renal afferent arterioles. Am. J. Physiol. Renal. Physiol. 2016, 310, F1197–F1205. [Google Scholar] [CrossRef] [Green Version]
- Lai, E.Y.; Solis, G.; Luo, Z.; Carlstrom, M.; Sandberg, K.; Holland, S.; Wellstein, A.; Welch, W.J.; Wilcox, C.S. p47phox is required for afferent arteriolar contractile responses to angiotensin II and perfusion pressure in mice. Hypertension 2012, 59, 415–420. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Xu, G.; Luo, K.; Liu, H.; Huang, T.; Fang, X.; Tu, W. The progress of inflammation and oxidative stress in patients with chronic kidney disease. Ren. Fail. 2015, 37, 45–49. [Google Scholar] [CrossRef]
- Tucker, P.S.; Scanlan, A.T.; Dalbo, V.J. Chronic kidney disease influences multiple systems: Describing the relationship between oxidative stress, inflammation, kidney damage, and concomitant disease. Oxid. Med. Cell. Longev. 2015, 2015, 806358. [Google Scholar] [CrossRef]
- Rivero, A.; Mora, C.; Muros, M.; García, J.; Herrera, H.; Navarro-González, J.F. Pathogenic perspectives for the role of inflammation in diabetic nephropathy. Clin. Sci. 2009, 116, 479–492. [Google Scholar] [CrossRef] [Green Version]
- Rayego-Mateos, S.; Morgado-Pascual, J.L.; Opazo-Ríos, L.; Guerrero-Hue, M.; García-Caballero, C.; Vázquez-Carballo, C.; Mas, S.; Belén Sanz, A.; Herencia, C.; Mezzano, S.; et al. Pathogenic pathways and therapeutic approaches targeting inflammation in diabetic nephropathy. Int. J. Mol. Sci. 2020, 21, 3798. [Google Scholar] [CrossRef]
- Pérez-Morales, R.E.; Del Pino, M.D.; Valdivielso, J.M.; Ortiz, A.; Mora-Fernández, C.; Navarro-González, J.F. Inflammation in Diabetic Kidney Disease. Nephron 2019, 143, 12–16. [Google Scholar] [CrossRef] [Green Version]
- Mihai, S.; Codrici, E.; Popescu, I.D.; Enciu, A.M.; Albulescu, L.; Necula, L.G.; Mambet, C.; Anton, G.; Tanase, C. Inflammation-related mechanisms in chronic kidney disease prediction, progression, and outcome. J. Immunol. Res. 2018, 2018, 2180373. [Google Scholar] [CrossRef] [PubMed]
- Qian, Q. Inflammation: A key contributor to the genesis and progression of chronic kidney disease. Contrib. Nephrol. 2017, 191, 72–83. [Google Scholar]
- Fatani, S.H.; Babakr, A.T.; NourEldin, E.M.; Almarzouki, A.A. Lipid peroxidation is associated with poor control of type-2 diabetes mellitus. Diabetes Metab. Syndr. 2016, 10 (Suppl. S1), S64–S67. [Google Scholar] [CrossRef] [PubMed]
- Bigagli, M.; Lodovici, M. Circulating oxidative stress biomarkers in clinical studies on type 2 diabetes and its complications. Oxid. Med. Cell. Longev. 2019, 2019, 5953685. [Google Scholar] [CrossRef] [PubMed]
- Handelman, G.J. Evaluation of oxidant stress in dialysis patients. Blood Purif. 2000, 18, 343–349. [Google Scholar] [CrossRef]
- Tucker, P.S.; Dalbo, V.J.; Han, T.; Kingsley, M.I. Clinical and research markers of oxidative stress in chronic kidney disease. Biomarkers 2013, 18, 103–115. [Google Scholar] [CrossRef] [PubMed]
- Marrocco, I.; Altieri, F.; Peluso, I. Measurement and clinical significance of biomarkers of oxidative stress in humans. Oxid. Med. Cell. Longev. 2017, 2017, 6501046. [Google Scholar] [CrossRef]
- Martin-Mateo, M.C.; Sanchez-Portugal, M.; Iglesias, S.; de Paula, A.; Bustamante, J. Oxidative stress in chronic renal failure. Ren. Fail. 1999, 21, 155–167. [Google Scholar] [CrossRef]
- Atamer, A.; Kocyigit, Y.; Ecder, S.A.; Selek, S.; Ilhan, N.; Ecder, T.; Atamer, Y. Effect of oxidative stress on antioxidant enzyme activities, homocysteine and lipoproteins in chronic kidney disease. J. Nephrol. 2008, 21, 924–930. [Google Scholar]
- De Vecchi, A.F.; Bamonti, F.; Novembrino, C.; Ippolito, S.; Guerra, L.; Lonati, S.; Salini, S.; Aman, C.S.; Scurati, M.E.; Cighetti, G. Free and total plasma malondialdehyde in chronic renal insufficiency and in dialysis patients. Nephrol. Dial. Transplant. 2009, 24, 2524–2529. [Google Scholar] [CrossRef] [Green Version]
- Kaya, Y.; Ari, E.; Demir, H.; Soylemez, N.; Cebi, A.; Alp, H.; Bakan, E.; Gecit, I.; Asicioglu, E.; Beytur, A. Accelerated atherosclerosis in haemodialysis patients; Correlation of endothelial function with oxidative DNA damage. Nephrol. Dial. Transplant. 2012, 27, 1164–1169. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Emre, H.; Keles, M.; Yildirim, S.; Uyanik, A.; Kara, F.; Tamer, F.; Aydinli, B. Comparison of the oxidant-antioxidant parameters and sialic acid levels in renal transplant patients and peritoneal dialysis patients. Transplant. Proc. 2011, 43, 809–812. [Google Scholar] [CrossRef] [PubMed]
- Zahmatkesh, M.; Kadkhodaee, M.; Mahdavi-Mazdeh, M.; Ghaznavi, R.; Hemati, M.; Seifi, B.; Golab, F.; Hasani, K.; Lessan, P.M.; Einollahi, B. Oxidative stress status in renal transplant recipients. Exp. Clin. Transplant. 2010, 8, 38–44. [Google Scholar] [PubMed]
- Tbahriti, H.F.; Kaddous, A.; Bouchenak, M.; Mekki, K. Effect of different stages of chronic kidney disease and renal replacement therapies on oxidant-antioxidant balance in uremic patients. Biochem. Res. Int. 2013, 2013, 358985. [Google Scholar] [CrossRef] [PubMed]
- Oberg, B.P.; McMenamin, E.; Lucas, F.L.; McMonagle, E.; Morrow, J.; Ikizler, T.A.; Himmelfarb, J. Increased prevalence of oxidant stress and inflammation in patients with moderate to severe chronic kidney disease. Kidney Int. 2004, 65, 1009–1016. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lim, P.S.; Chang, Y.M.; Thien, L.M.; Wang, N.P.; Yang, C.C.; Chen, T.T.; Hsu, W.M. 8-iso-prostaglandin F2alpha as a useful clinical biomarker of oxidative stress in ESRD patients. Blood Purif. 2002, 20, 537–542. [Google Scholar] [CrossRef] [PubMed]
- Handelman, G.J.; Walter, M.F.; Adhikarla, R.; Gross, J.; Dallal, G.E.; Levin, N.W.; Blumberg, J.B. Elevated plasma F2-isoprostanes in patients on long-term hemodialysis. Kidney Int. 2001, 59, 1960–1966. [Google Scholar] [CrossRef] [Green Version]
- Dounousi, E.; Papavasiliou, E.; Makedou, A.; Ioannou, K.; Katopodis, K.P.; Tselepis, A.; Siamopoulos, K.C.; Tsakiris, D. Oxidative stress is progressively enhanced with advancing stages of CKD. Am. J. Kidney Dis. 2006, 48, 752–760. [Google Scholar] [CrossRef] [Green Version]
- Ramezani, M.; Nazemian, F.; Shamsara, J.; Koohrokhi, R.; Mohammadpour, A.H. Effect of omega-3 fatty acids on plasma level of 8-isoprostane in kidney transplant patients. J. Ren. Nutr. 2011, 21, 196–199. [Google Scholar] [CrossRef]
- Berlett, B.S.; Stadtman, E.R. Protein oxidation in aging, disease, and oxidative stress. J. Biol. Chem. 1997, 272, 20313–20316. [Google Scholar] [CrossRef] [Green Version]
- Kohen, R.; Nyska, A. Oxidation of biological systems: Oxidative stress phenomena, antioxidants, redox reactions, and methods for their quantification. Toxicol. Pathol. 2002, 30, 620–650. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ho, E.; Karimi Galougahi, K.; Liu, C.C.; Bhindi, R.; Figtree, G.A. Biological markers of oxidative stress: Applications to cardiovascular research and practice. Redox Biol. 2013, 1, 483–491. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Namiduru, E.S.; Tarakcioglu, M.; Tiryaki, O.; Usalan, C. Evaluation of oxidative and nitrosative stress in hemodialysis patients. Minerva Med. 2010, 101, 305–310. [Google Scholar] [PubMed]
- Valli, A.; Suliman, M.E.; Meert, N.; Vanholder, R.; Lindholm, B.; Stenvinkel, P.; Watanabe, M.; Barany, P.; Alvestrand, A.; Anderstam, B. Overestimation of advanced oxidation protein products in uremic plasma due to presence of triglycerides and other endogenous factors. Clin. Chim. Acta 2007, 379, 87–94. [Google Scholar] [CrossRef]
- Machowska, A.; Sun, J.; Qureshi, A.R.; Isoyama, N.; Leurs, P.; Anderstam, B.; Heimburger, O.; Barany, P.; Stenvinkel, P.; Lindholm, B. Plasma Pentosidine and Its Association with Mortality in Patients with Chronic Kidney Disease. PLoS ONE 2016, 11, e0163826. [Google Scholar] [CrossRef] [Green Version]
- Himmelfarb, J.; McMonagle, E.; McMenamin, E. Plasma protein thiol oxidation and carbonyl formation in chronic renal failure. Kidney Int. 2000, 58, 2571–2578. [Google Scholar] [CrossRef] [Green Version]
- Mitrogianni, Z.; Barbouti, A.; Galaris, D.; Siamopoulos, K.C. Oxidative modification of albumin in predialysis, hemodialysis, and peritoneal dialysis patients. Nephron Clin. Pract. 2009, 113, c234–c240. [Google Scholar] [CrossRef]
- Aveles, P.R.; Criminácio, C.R.; Gonçalves, S.; Bignelli, A.T.; Claro, L.M.; Siqueira, S.S.; Nakao, L.S.; Pecoits-Filho, R. Association between biomarkers of carbonyl stress with increased systemic inflammatory response in different stages of chronic kidney disease and after renal transplantation. Nephron Clin. Pract. 2010, 116, c294–c299. [Google Scholar] [CrossRef]
- Tarng, D.C.; Wen Chen, T.; Huang, T.P.; Chen, C.L.; Liu, T.Y.; Wei, Y.H. Increased oxidative damage to peripheral blood leukocyte DNA in chronic peritoneal dialysis patients. J. Am. Soc. Nephrol. 2002, 13, 1321–1330. [Google Scholar] [CrossRef] [Green Version]
- Tarng, D.C.; Huang, T.P.; Wei, Y.H.; Liu, T.Y.; Chen, H.W.; Wen Chen, T.; Yang, W.C. 8-hydroxy-2′-deoxyguanosine of leukocyte DNA as a marker of oxidative stress in chronic hemodialysis patients. Am. J. Kidney Dis. 2000, 36, 934–944. [Google Scholar] [CrossRef]
- Shimoike, T.; Inoguchi, T.; Umeda, F.; Nawata, H.; Kawano, K.; Ochi, H. The meaning of serum levels of advanced glycosylation end products in diabetic nephropathy. Metabolism 2000, 49, 1030–1035. [Google Scholar] [CrossRef]
- Lobo, V.; Patil, A.; Phatak, A.; Chandra, N. Free radicals, antioxidants and functional foods: Impact on human health. Pharmacogn. Rev. 2010, 4, 118–126. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Fatouros, I.G.; Pasadakis, P.; Sovatzidis, A.; Chatzinikolaou, A.; Panagoutsos, S.; Sivridis, D.; Michailidis, I.; Douroudos, I.; Taxildaris, K.; Vargemezis, V. Acute exercise may exacerbate oxidative stress response in hemodialysis patients. Nephron Clin. Pract. 2008, 109, c55–c64. [Google Scholar] [CrossRef] [PubMed]
- Coaccioli, S.; Standoli, M.L.; Biondi, R.; Panaccione, A.; Landucci, P.; Del Giorno, R.; Paladini, A.; Standoli, M.; Puxeddu, A. Open comparison study of oxidative stress markers between patients with chronic renal failure in conservative therapy and patients in haemodialysis. Clin. Ther. 2010, 161, 435–439. [Google Scholar]
- Filiopoulos, V.; Hadjiyannakos, D.; Takouli, L.; Metaxaki, P.; Sideris, V.; Vlassopoulos, D. Inflammation and oxidative stress in end-stage renal disease patients treated with hemodialysis or peritoneal dialysis. Int. J. Artif. Organs 2009, 32, 872–882. [Google Scholar] [CrossRef] [PubMed]
- Zima, T.; Stípek, S.; Crkovská, J.; Nĕmecek, K.; Fialová, J.; Pláteník, J.; Bártová, V. Lipid peroxidation and antioxidant enzymes in CAPD patients. Ren. Fail. 1996, 18, 113–119. [Google Scholar] [CrossRef]
- Shurtz-Swirski, R.; Mashiach, E.; Kristal, B.; Shkolnik, T.; Shasha, S.M. Antioxidant enzymes activity in polymorphonuclear leukocytes in chronic renal failure. Nephron 1995, 71, 176–179. [Google Scholar] [CrossRef]
- Mimić-Oka, J.; Simić, T.; Djukanović, L.; Reljić, Z.; Davicević, Z. Alteration in plasma antioxidant capacity in various degrees of chronic renal failure. Clin. Nephrol. 1999, 51, 233–241. [Google Scholar]
- Vural, A.; Yilmaz, M.I.; Caglar, K.; Aydin, A.; Sonmez, A.; Eyileten, T.; Acikel, C.; Gulec, B.; Kozak, O.; Oner, K. Assessment of oxidative stress in the early posttransplant period: Comparison of cyclosporine A and tacrolimus-based regimens. Am. J. Nephrol. 2005, 25, 250–255. [Google Scholar] [CrossRef]
- Ongajyooth, L.; Ong-ajyooth, S.; Likidlilid, A.; Chantachum, Y.; Shayakul, C.; Nilwarangkur, S. Role of lipid peroxidation, trace elements and anti-oxidant enzymes in chronic renal disease patients. J. Med. Assoc. Thail. 1996, 79, 791–800. [Google Scholar]
- Romeu, M.; Nogues, R.; Marcas, L.; Sánchez-Martos, V.; Mulero, M.; Martinez-Vea, A.; Mallol, J.; Giralt, M. Evaluation of oxidative stress biomarkers in patients with chronic renal failure: A case control study. BMC Res. Notes 2010, 3, 20. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Canestrari, F.; Buoncristiani, U.; Galli, F.; Giorgini, A.; Albertini, M.C.; Carobi, C.; Pascucci, M.; Bossù, M. Redox state, antioxidative activity and lipid peroxidation in erythrocytes and plasma of chronic ambulatory peritoneal dialysis patients. Clin. Chim. Acta 1995, 234, 127–136. [Google Scholar] [CrossRef]
- Ceballos-Picot, I.; Witko-Sarsat, V.; Merad-Boudia, M.; Nguyen, A.T.; Thévenin, M.; Jaudon, M.C.; Zingraff, J.; Verger, C.; Jungers, P.; Descamps-Latscha, B. Glutathione antioxidant system as a marker of oxidative stress in chronic renal failure. Free Radic. Biol. Med. 1996, 21, 845–853. [Google Scholar] [CrossRef]
- Cristol, J.P.; Vela, C.; Maggi, M.F.; Descomps, B.; Mourad, G. Oxidative stress and lipid abnormalities in renal transplant recipients with or without chronic rejection. Transplantation 1998, 65, 1322–1328. [Google Scholar] [CrossRef] [PubMed]
- Drai, J.; Bannier, E.; Chazot, C.; Hurot, J.M.; Goedert, G.; Jean, G.; Charra, B.; Laurent, G.; Baltassat, P.; Revol, A. Oxidants and antioxidants in long-term haemodialysis patients. Farmaco 2001, 56, 463–465. [Google Scholar] [CrossRef]
- Santangelo, F.; Witko-Sarsat, V.; Drüeke, T.; Descamps-Latscha, B. Restoring glutathione as a therapeutic strategy in chronic kidney disease. Nephrol. Dial. Transplant. 2004, 19, 1951–1955. [Google Scholar] [CrossRef]
- Ross, E.A.; Koo, L.C.; Moberly, J.B. Low whole blood and erythrocyte levels of glutathione in hemodialysis and peritoneal dialysis. Am. J. Kidney Dis. 1997, 30, 489–494. [Google Scholar] [CrossRef]
- Galli, F.; Rovidati, S.; Benedetti, S.; Buoncristiani, U.; Covarelli, C.; Floridi, A.; Canestrari, F. Overexpression of erythrocyte glutathione S-transferase in uremia and dialysis. Clin. Chem. 1999, 45, 1781–1788. [Google Scholar] [CrossRef] [Green Version]
- Daschner, M.; Lenhartz, H.; Botticher, D.; Schaefer, F.; Wollschläger, M.; Mehls, O.; Leichsenring, M. Influence of dialysis on plasma lipid peroxidation products and antioxidant levels. Kidney Int. 1996, 50, 1268–1272. [Google Scholar] [CrossRef] [Green Version]
- Suliman, M.E.; Divino Filho, J.C.; Barany, P.; Anderstam, B.; Lindholm, B.; Bergström, J. Effects of highdose folic acid and pyridoxine on plasma and erythrocyte sulfur amino acids in hemodialysis patients. J. Am. Soc. Nephrol. 1999, 10, 1287–1296. [Google Scholar]
- Cristol, J.P.; Bosc, J.Y.; Badiou, S.; Leblanc, M.; Lorrho, R.; Descomps, B.; Canaud, B. Erythropoietin and oxidative stress in haemodialysis: Beneficial effects of vitamin E supplementation. Nephrol. Dial. Transplant. 1997, 12, 2312–2317. [Google Scholar] [CrossRef] [Green Version]
- Annuk, M.; Fellström, B.; Akerblom, O.; Zilmer, K.; Vihalemm, T.; Zilmer, M. Oxidative stress markers in pre-uremic patients. Clin. Nephrol. 2001, 56, 308–314. [Google Scholar] [PubMed]
- Adeshara, K.A.; Diwan, A.G.; Jagtap, T.R.; Advani, K.; Siddiqui, A.; Tupe, R.S. Relationship between plasma glycation with membrane modification, oxidative stress and expression of glucose trasporter-1 in type 2 diabetes patients with vascular complications. J. Diabetes Complicat. 2017, 31, 439–448. [Google Scholar] [CrossRef] [PubMed]
- Bigagli, E.; Raimondi, l.; Mannucci, E.; Colombi, C.; Bardini, G.; Rotella, C.M.; Lodovici, M. Lipid and protein oxidation products, antioxidant status and vascular complications in poorly controlled type 2 diabetes. Br. J. Diabetes Vasc. Dis. 2012, 12, 33–39. [Google Scholar] [CrossRef]
- Chawla, D.; Bansal, S.; Banerjee, B.D.; Madhu, S.V.; Kalra, O.P.; Tripathi, A.K. Role of advanced glycation end product (AGE)-induced receptor (RAGE) expression in diabetic vascular complications. Microvasc. Res. 2014, 95, 1–6. [Google Scholar] [CrossRef] [PubMed]
- Gupta, S.; Gambhir, J.K.; Kalra, O.; Gautam, A.; Shukla, K.; Mehndiratta, M.; Agarwal, S.; Shukla, R. Association of biomarkers of inflammation and oxidative stress with the risk of chronic kidney disease in Type 2 diabetes mellitus in North Indian population. J. Diabetes Complicat. 2013, 27, 548–552. [Google Scholar] [CrossRef]
- Pan, H.Z.; Zhang, L.; Guo, M.Y.; Sui, H.; Li, H.; Wu, W.H.; Qu, N.Q.; Liang, M.H.; Chang, D. The oxidative stress status in diabetes mellitus and diabetic nephropathy. Acta Diabetol. 2010, 47 (Suppl. S1), 71–76. [Google Scholar] [CrossRef]
- Piarulli, F.; Sartore, G.; Ceriello, A.; Ragazzi, E.; Reitano, R.; Nollino, L.; Cosma, C.; Fedele, D.; Lapolla, A. Relationship between glyco-oxidation, antioxidant status and microalbuminuria in type 2 diabetic patients. Diabetologia 2009, 52, 1419–1425. [Google Scholar] [CrossRef] [Green Version]
- Bondor, C.I.; Potra, A.R.; Moldovan, D.; Rusu, C.C.; Pop, M.C.; Muresan, A.; Vladutiu, D.S.; Kacso, I.M. Relationship of adiponectin to markers of oxidative stress in type 2 diabetic patients: Influence of incipient diabetes-associated kidney disease. Int. Urol. Nephrol. 2015, 47, 1173–1180. [Google Scholar] [CrossRef] [PubMed]
- Chou, S.T.; Tseng, S.T. Oxidative stress markers in type 2 diabetes patients with diabetic nephropathy. Clin. Exp. Nephrol. 2017, 21, 283–292. [Google Scholar] [CrossRef]
- Calabrese, V.; Mancuso, C.; Sapienza, M.; Puleo, E.; Calafato, S.; Cornelius, C.; Finocchiaro, M.; Mangiameli, A.; Di Mauro, M.; Giuffrida Stella, A.M.; et al. Oxidative stress and cellular stress response in diabetic nephropathy. Cell Stress Chaperones 2007, 12, 299–306. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Jakuš, V.; Sándorová, E.; Kalninová, J.; Krahulec, B. Monitoring of glycation, oxidative stress and inflammation in relation to the occurrence of vascular complications in patients with type 2 diabetes mellitus. Physiol. Res. 2014, 63, 297–309. [Google Scholar] [PubMed]
- Pandey, K.B.; Mishra, N.; Rizvi, S.I. Protein oxidation biomarkers in plasma of type 2 diabetic patients. Clin. Biochem. 2010, 43, 508–511. [Google Scholar] [CrossRef] [PubMed]
- Piwowar, A.; Knapik-Kordecka, M.; Warwas, M. Comparison of the usefulness of plasma levels of oxidatively modified forms of albumin in estimating kidney dysfunction in diabetic patients. Clin. Investig. Med. 2010, 33, E109. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Guerin-Dubourg, A.; Cournot, M.; Planesse, C.; Debussche, X.; Meilhac, O.; Rondeau, P.; Bourdon, E. Association between fluorescent advanced glycation end-products and vascular complications in type 2 diabetic patients. BioMed. Res. Int. 2017, 2017, 7989180. [Google Scholar] [CrossRef]
- Kerkeni, M.; Saïdi, A.; Bouzidi, H.; Letaief, A.; Ben Yahia, S.; Hammami, M. Pentosidine as a biomarker for microvascular complications in type 2 diabetic patients. Diab. Vasc. Dis. Res. 2013, 10, 239–245. [Google Scholar] [CrossRef]
- Hirata, K.; Kubo, K. Relationship between blood levels of N-carboxymethyl-lysine and pentosidine and the severity of microangiopathy in type 2 diabetes. Endocr. J. 2004, 51, 537–544. [Google Scholar] [CrossRef] [Green Version]
- Miura, J.; Yamagishi, S.I.; Uchigata, Y.; Takeuchi, M.; Yamamoto, H.; Makita, Z.; Iwamoto, Y. Serum levels of non-carboxymethyllysine advanced glycation end products are correlated to severity of microvascular complications in patients with Type 1 diabetes. J. Diabetes Complicat. 2003, 17, 16–21. [Google Scholar] [CrossRef]
- Serdar, M.; Sertoglu, E.; Uyanik, M.; Tapan, S.; Akin, K.; Bilgi, K.; Kurtet, I. Comparison of 8-hydroxy-2′-deoxyguanosine (8-OHdG) levels using mass spectrometer and urine albumin creatinine ratio as a predictor of development of diabetic nephropathy. Free Radic. Res. 2012, 46, 1291–1295. [Google Scholar] [CrossRef]
- Liu, X.; Gan, W.; Zou, Y.; Yang, B.; Su, Z.; Deng, J.; Wang, L.; Cai, J. Elevated Levels of Urinary Markers of Oxidative DNA and RNA Damage in Type 2 Diabetes with Complications. Oxid. Med. Cell. Longev. 2016, 2016, 4323198. [Google Scholar] [CrossRef] [Green Version]
- Waris, S.; Winklhofer-Roob, B.M.; Roob, J.M.; Fuchs, S.; Sourij, H.; Rabbani, N.; Thornalley, P.J. Increased DNA dicarbonyl glycation and oxidation markers in patients with type 2 diabetes and link to diabetic nephropathy. J. Diabetes Res. 2015, 2015, 915486. [Google Scholar] [CrossRef] [PubMed]
- Tatsch, E.; De Carvalho, J.A.; Hausen, B.S.; Bollick, Y.S.; Torbitz, V.D.; Duarte, T.; Scolari, R.; Duarte, M.M.; Londero, S.W.; Vaucher, R.A.; et al. Oxidative DNA damage is associated with inflammatory response, insulin resistance and microvascular complications in type 2 diabetes. Mutat. Res. 2015, 782, 17–22. [Google Scholar] [CrossRef] [PubMed]
- Xu, G.W.; Yao, Q.H.; Weng, Q.F.; Su, B.L.; Zhang, X.; Xiong, J.H. Study of urinary 8-hydroxydeoxyguanosine as a biomarker of oxidative DNA damage in diabetic nephropathy patients. J. Pharm. Biomed. Anal. 2004, 36, 101–104. [Google Scholar] [CrossRef] [PubMed]
- Zhang, D.; Ye, S.; Pan, T. The role of serum and urinary biomarkers in the diagnosis of early diabetic nephropathy in patients with type 2 diabetes. PeerJ 2019, 7, e7079. [Google Scholar] [CrossRef] [Green Version]
- Hinokio, Y.; Suzuki, S.; Hirai, M.; Suzuki, C.; Suzuki, M.; Toyota, T. Urinary excretion of 8-oxo-7, 8-dihydro-2′-deoxyguanosine as a predictor of the development of diabetic nephropathy. Diabetologia 2002, 45, 877–882. [Google Scholar] [CrossRef] [Green Version]
- Sanchez, M.; Roussel, R.; Hadjadj, S.; Moutairou, A.; Marre, M.; Velho, G.; Mohammedi, K. Plasma concentrations of 8-hydroxy-2′-deoxyguanosine and risk of kidney disease and death in individuals with type 1 diabetes. Diabetologia 2018, 61, 977–984. [Google Scholar] [CrossRef] [Green Version]
- Huang, M.; Que, Y.; Shen, X. Correlation of the plasma levels of soluble RAGE and endogenous secretory RAGE with oxidative stress in pre-diabetic patients. J. Diabetes Complicat. 2015, 29, 422–426. [Google Scholar] [CrossRef]
- Jiménez-Osorio, A.S.; Picazo, A.; González-Reyes, S.; Barrera-Oviedo, D.; Rodríguez-Arellano, M.E.; Pedraza-Chaverri, J. Nrf2 and redox status in prediabetic and diabetic patients. Int. J. Mol. Sci. 2014, 15, 20290–20305. [Google Scholar] [CrossRef]
- Gawlik, K.; Naskalski, J.W.; Fedak, D.; Pawlica-Gosiewska, D.; Grudzień, U.; Dumnicka, P.; Małecki, M.T.; Solnica, B. Markers of antioxidant defense in patients with type 2 diabetes. Oxid. Med. Cell. Longev. 2016, 2016, 2352361. [Google Scholar] [CrossRef] [Green Version]
- Picu, A.; Petcu, L.; Ştefan, S.; Mitu, M.; Lixandru, D.; Ionescu-Tîrgovişte, C.; Grădișteanu Pîrcălăbioru, G.; Ciulu-Costinescu, F.; Bubulica, M.V.; Chifiriuc, M.C. Markers of oxidative stress and antioxidant defense in romanian patients with type 2 diabetes mellitus and obesity. Molecules 2017, 22, 714. [Google Scholar] [CrossRef]
- Bandeira, S.M.; Guedes, G.S.; da Fonseca, L.J.; Pires, A.S.; Gelain, D.P.; Moreira, J.C.F.; Rabelo, L.A.; Vasconcelos, S.M.L.; Goulart, M.O.F. Characterization of blood oxidative stress in type 2 diabetes mellitus patients: Increase in lipid peroxidation and SOD activity. Oxid. Med. Cell. Longev. 2012, 2012, 819310. [Google Scholar]
- Strom, A.; Kaul, K.; Brüggemann, J.; Ziegler, I.; Rokitta, I.; Püttgen, S.; Szendroedi, J.; Müssig, K.; Roden, M.; Ziegler, D. Lower serum extracellular superoxide dismutase levels are associated with polyneuropathy in recent-onset diabetes. Exp. Mol. Med. 2017, 49, e394. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lodovici, M.; Bigagli, E.; Luceri, C.; Mannucci, E.; Rotella, C.M.; Raimondi, L. Gender-related drug effect on several markers of oxidation stress in diabetes patients with and without complications. Eur. J. Pharmacol. 2015, 766, 86–90. [Google Scholar] [CrossRef] [PubMed]
- Grindel, A.; Guggenberger, B.; Eichberger, L.; Pöppelmeyer, C.; Gschaider, M.; Tosevska, A.; Mare, G.; Briskey, D.; Brath, H.; Wagner, K.H. Oxidative Stress, DNA damage and DNA repair in female patients with diabetes mellitus type. PLoS ONE 2016, 11, e0162082. [Google Scholar] [CrossRef] [Green Version]
- Noce, A.; Fabrini, R.; Dessì, M.; Bocedi, A.; Santini, S.; Rovella, V.; Pastore, A.; Tesauro, M.; Bernardini, S.; Di Daniele, N.; et al. Erythrocyte glutathione transferase activity: A possible early biomarker for blood toxicity in uremic diabetic patients. Acta Diabetol. 2014, 51, 219–224. [Google Scholar] [CrossRef]
- Mohammedi, K.; Patente, T.A.; Bellili-Muñoz, N.; Driss, F.; Monteiro, M.B.; Roussel, R.; Pavin, E.J.; Seta, N.; Fumeron, F.; Azevedo, M.J.; et al. Catalase activity, allelic variations in the catalase gene and risk of kidney complications in patients with type 1 diabetes. Diabetologia 2013, 56, 2733–2742. [Google Scholar] [CrossRef]
- Choi, A.M.K.; Alam, J. Heme oxygenase-1: Function, regulation, and implication of a novel stress-inducible protein in oxidant-induced lung injury. Am. J. Respir. Cell Mol. Biol. 1996, 15, 9–19. [Google Scholar] [CrossRef]
- Nath, K.A. Heme oxygenase-1: A provenance for cytoprotective pathways in the kidney and other tissues. Kidney Int. 2006, 70, 432–443. [Google Scholar] [CrossRef] [Green Version]
- Bao, W.; Song, F.; Li, X.; Rong, S.; Yang, W.; Rong, S.; Yang, W.; Zhang, M.; Yao, P.; Hao, L.; et al. Plasma heme oxygenase-1 concentration is elevated in individuals with type 2 diabetes mellitus. PLoS ONE 2010, 5, e12371. [Google Scholar] [CrossRef]
- Li, Z.; Xu, Y.; Liu, X.; Nie, Y.; Zhao, Z. Urinary heme oxygenase-1 as a potential biomarker for early diabetic nephropathy. Nephrology 2017, 22, 58–64. [Google Scholar] [CrossRef]
- Welt, K.; Weiss, J.; Martin, R.; Hermsdorf, T.; Drews, S.; Fitzl, G. Ginkgo biloba extract protects rat kidney from diabetic and hypoxic damage. Phytomedicine 2007, 14, 196–203. [Google Scholar] [CrossRef] [PubMed]
- Nascimento Gomes, G.; Barbos, F.T.; Radaeli, R.F.; Cavanal, M.F.; Mello Aires, M.; Zaladek Gil, F. Effect of Dalpha-tocopherol on tubular nephron acidification by rats with induced diabetes mellitus. Braz. J. Med. Biol. Res. 2005, 38, 1043–1051. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kim, S.S.; Galaher, D.D.; Csallany, A.S. Vitamin E and probucol reduce urinary lipophilic aldehydes and renal enlargement in streptozotocin-induced diabetic rats. Lipids 2003, 35, 1225–1237. [Google Scholar] [CrossRef] [PubMed]
- Tavafi, M.; Ahmadvand, H.; Tamjidipoor, A.; Delfan, B.; Khalatbari, A. Satureja khozestanica essential oil ameliorates progression of diabetic nephropathy in uninephrectomized diabetic rats. Tissue Cell 2011, 43, 45–51. [Google Scholar] [CrossRef]
- Ohno, T.; Takemura, G.; Murata, I.; Kagawa, T.; Akao, S.; Minatoguchi, S.; Fujiwara, T.; Fujiwara, H. Water extract of the root of Lindera strychnifolia slows down the progression of diabetic nephropathy in db/db mice. Life Sci. 2005, 77, 1391–1403. [Google Scholar] [CrossRef]
- Jun, M.; Venkataraman, V.; Razavian, M.; Cooper, B.; Zoungas, S.; Ninomiya, T.; Webster, A.C.; Perkovic, V. Antioxidants for chronic kidney disease. Cochrane Database Syst. Rev. 2012, 10, CD008176. [Google Scholar] [CrossRef]
- Moreno, J.A.; Gomez-Guerrero, C.; Mas, S.; Sanz, A.B.; Lorenzo, O.; Ruiz-Ortega, M.; Opazo, L.; Mezzano, S.; Egido, J. Targeting inflammation in diabetic nephropathy: A tale of hope. Expert Opin. Investig. Drugs 2018, 27, 917–930. [Google Scholar] [CrossRef]
- Rapa, S.F.; Di Iorio, B.R.; Campiglia, P.; Heidland, A.; Marzocco, S. Inflammation and oxidative stress in chronic kidney disease-potential therapeutic role of minerals, vitamins and plant-derived metabolites. Int. J. Mol. Sci. 2019, 21, 263. [Google Scholar] [CrossRef] [Green Version]
- Jing, W.; Vaziri, N.D.; Nunes, A.; Suematsu, Y.; Farzaneh, T.; Khazaeli, M.; Moradi, H. LCZ696 (Sacubitril/valsartan) ameliorates oxidative stress, inflammation, fibrosis and improves renal function beyond angiotensin receptor blockade in CKD. Am. J. Transl. Res. 2017, 9, 5473–5484. [Google Scholar]
- Kimura, Y.; Kuno, A.; Tanno, M.; Sato, T.; Ohno, K.; Shibata, S.; Nakata, K.; Sugawara, H.; Abe, K.; Igaki, Y.; et al. Canagliflozin, a sodium-glucose cotransporter 2 inhibitor, normalizes renal susceptibility to type 1 cardiorenal syndrome through reduction of renal oxidative stress in diabetic rats. J. Diabetes Investig. 2019, 10, 933–946. [Google Scholar] [CrossRef]
Figure 1.
Oxidative stress is a significant factor in the development of diabetic nephropathy. Oxidative stress is associated with metabolic changes and alterations in renal hemodynamic. MDA: malondialdehyde; TBARS: thiobarbituric acid reactive substances; HNE: 4-hydroxynonenal; AOPP: advanced oxidation protein products; AGE: advanced glycation end products; 8-OHG: 8-hydroxyguanosine; 8-OHdG: 8-hydroxy-2′-deoxyguanosine; eGFR: estimated glomerular filtration rate; ESRD: end-stage renal disease.
Figure 1.
Oxidative stress is a significant factor in the development of diabetic nephropathy. Oxidative stress is associated with metabolic changes and alterations in renal hemodynamic. MDA: malondialdehyde; TBARS: thiobarbituric acid reactive substances; HNE: 4-hydroxynonenal; AOPP: advanced oxidation protein products; AGE: advanced glycation end products; 8-OHG: 8-hydroxyguanosine; 8-OHdG: 8-hydroxy-2′-deoxyguanosine; eGFR: estimated glomerular filtration rate; ESRD: end-stage renal disease.


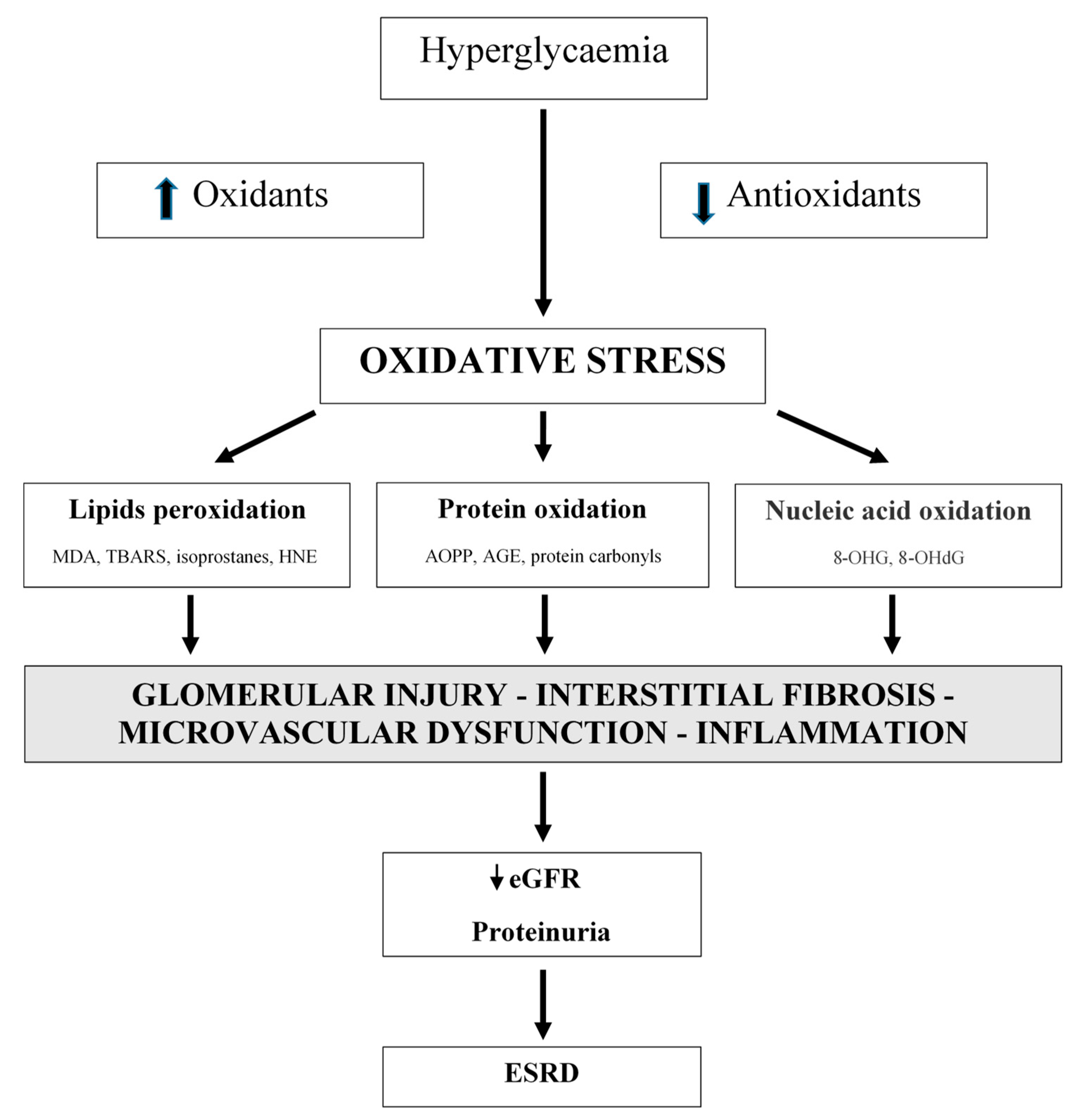{kind=link}
Table 1.
Most important markers of oxidative stress and antioxidants.
| Markers of Oxidative Stress | Antioxidants |
|---|---|
| Lipid peroxidation | Enzymatic |
| Malondialdehyde (MDA) | Superoxide dismutase (SOD) |
| Thiobarbituric acid reactive substances (TBARSs) | Catalase |
| 4-hydroxynonenal (HNE) | Glutathione peroxidase (GSH-Px) |
| F2-isoprostanes | Haem oxygenase-1 (HO-1) |
| Protein oxidation | Thioredoxin |
| Advanced oxidation protein products (AOPPs) | Nonenzymatic |
| Advanced glycation end products (AGEs) | Glutathione (GSH) |
| Protein carbonyls | Vitamins (vitamins C and E) |
| Nucleic acid oxidation | β-carotene |
| 8-hydroxyguanosine (8-OHG) | |
| 8-hydroxy-2′-deoxyguanosine (8-OHdG) |
Table 2.
Most important biomarkers of oxidative stress associated with diabetic nephropathy (DN) used in clinical studies.
Table 2.
Most important biomarkers of oxidative stress associated with diabetic nephropathy (DN) used in clinical studies.
| Biomarker | Clinical Importance | Sample | Ref. |
|---|---|---|---|
| MDA | Increased in patients with DN compared to those without | plasma serum | [152,154] [153] |
| No difference in patients with or without DN | plasma | [155] | |
| No difference in patients with normo-, micro-, and macroalbuminuria | plasma, erythrocytes | [156] | |
| HNE | Increased in patients with DN compared to controls | plasma, leukocytes | [157] |
| F2-isoprostanes | Increased in patients with DN compared to controls | plasma, leukocytes | [157] |
| AOPP | Increased in patients with DN compared to those without | serum | [153] |
| Increased in patients with DN compared to those without | plasma | [160] | |
| AGE | Increased in patients with DN compared to those without | plasma | [154] |
| Increased in patients with DN compared to controls | plasma, urine | [157] | |
| Increased in patients with renal failure compared to patients with normo-, micro-, and macroalbuminuria without renal failure | blood | [163] | |
| Increased in haemodialysis patients compared to non-dialysis; no difference in patients with normo-, micro-, and macroalbuminuria | serum | [106] | |
| No difference in patients with normo-, micro-, and macroalbuminuria | plasma | [156] | |
| Protein carbonyls | Increased in patients with DN compared to those without | serum | [153] |
| Increased in patients with DN compared to controls | plasma, leukocytes | [157] | |
| Nucleic acid oxidation | Increased in patients with DN compared to those without | serum urine | [153,167] [167] |
| Increased in patients with micro- and macroalbuminuria compared to normoalbuminuria; no difference in patients with micro- and macroalbuminuria | plasma | [156] | |
| Increased in patients with macroalbuminuria compared to micro- or normoalbuminuria | urine | [106,169] | |
| Prediction of the onset and progression of DN | urine | [170,171] | |
| No relationship with the onset and progression of DN | leukocytes | [171] | |
| No difference in patients with or without DN | urine | [165] | |
| TAS | Decreased in patients with DN compared to those without | plasma | [152] |
| No difference in patients with or without DN | plasma | [154] | |
| No difference in patients with normo-, micro-, and macroalbuminuria | erythrocytes | [156] | |
| SOD | Decreased in patients with DN compared to those without | serum | [153] |
| No difference in patients with or without DN | erythrocytes | [155] | |
| No difference in patients with normo-, micro-, and macroalbuminuria | plasma, erythrocytes | [156] | |
| Catalase | No difference in patients with or without DN | serum erythrocytes | [153] [181] |
| No difference in patients with normo-, micro-, and macroalbuminuria | plasma, erythrocytes | [156] | |
| GSH-Px | No difference in patients with or without DN | serum | [153] |
| No difference in patients with normo-, micro-, and macroalbuminuria | plasma, erythrocytes | [156] | |
| HO-1 | Increased in patients with DN, no difference in patients with micro- and macroalbuminuria | urine | [186] |
| Increased in patients with DN compared to controls | lymphocytes | [157] | |
| GSH | Decreased in patients with DN compared to those without | plasma | [152] |
| No difference in patients with normo-, micro-, and macroalbuminuria | plasma, erythrocytes | [156] | |
| Vitamin C | Decreased in DN; correlation with UACR and eGFR | tissue | [156] |
| Vitamin E | No difference in patients with or without DN | tissue plasma | [156] [154] |
MDA: malondialdehyde; HNE: 4-hydroxynonenal; AOPP: advanced oxidation protein products; AGE: advanced glycation end products; TAS: total antioxidant status; SOD: superoxide dismutase; GSH-Px: glutathione peroxidase; HO-1: haem oxygenase-1; GSH: glutathione.
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
MDPI and ACS Style
Vodošek Hojs, N.; Bevc, S.; Ekart, R.; Hojs, R. Oxidative Stress Markers in Chronic Kidney Disease with Emphasis on Diabetic Nephropathy. Antioxidants 2020, 9, 925. https://doi.org/10.3390/antiox9100925
AMA Style
Vodošek Hojs N, Bevc S, Ekart R, Hojs R. Oxidative Stress Markers in Chronic Kidney Disease with Emphasis on Diabetic Nephropathy. Antioxidants. 2020; 9(10):925. https://doi.org/10.3390/antiox9100925
Chicago/Turabian StyleVodošek Hojs, Nina, Sebastjan Bevc, Robert Ekart, and Radovan Hojs. 2020. "Oxidative Stress Markers in Chronic Kidney Disease with Emphasis on Diabetic Nephropathy" Antioxidants 9, no. 10: 925. https://doi.org/10.3390/antiox9100925
Note that from the first issue of 2016, this journal uses article numbers instead of page numbers. See further details here.