
Effectiveness of Propolis in the Treatment of Periodontal Disease: Updated Systematic Review with Meta-Analysis

 , , ,
, , ,  , , ,
, , ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Protocol
2.2. Data Sources and Search Strategy
2.3. Inclusion and Exclusion Criteria
- (a)
- Articles published in English,
- (b)
- Randomized controlled clinical trials,
- (c)
- Non-randomized studies assessing the effectiveness of propolis in the treatment of periodontal diseases.
- (a)
- In vitro studies,
- (b)
- Animal studies,
- (c)
- Comparative studies,
- (d)
- Systematic reviews,
- (e)
- Clinical cases,
- (f)
- Non-relevant studies (e.g., effectiveness of propolis in the treatment of other conditions, narrative reviews…), duplicate studies and those that did not meet the inclusion criteria stated above.
2.4. Data Extraction and Analysis
2.5. Quality of the Reports of the Included Randomized Trials
2.6. Statistical Analysis
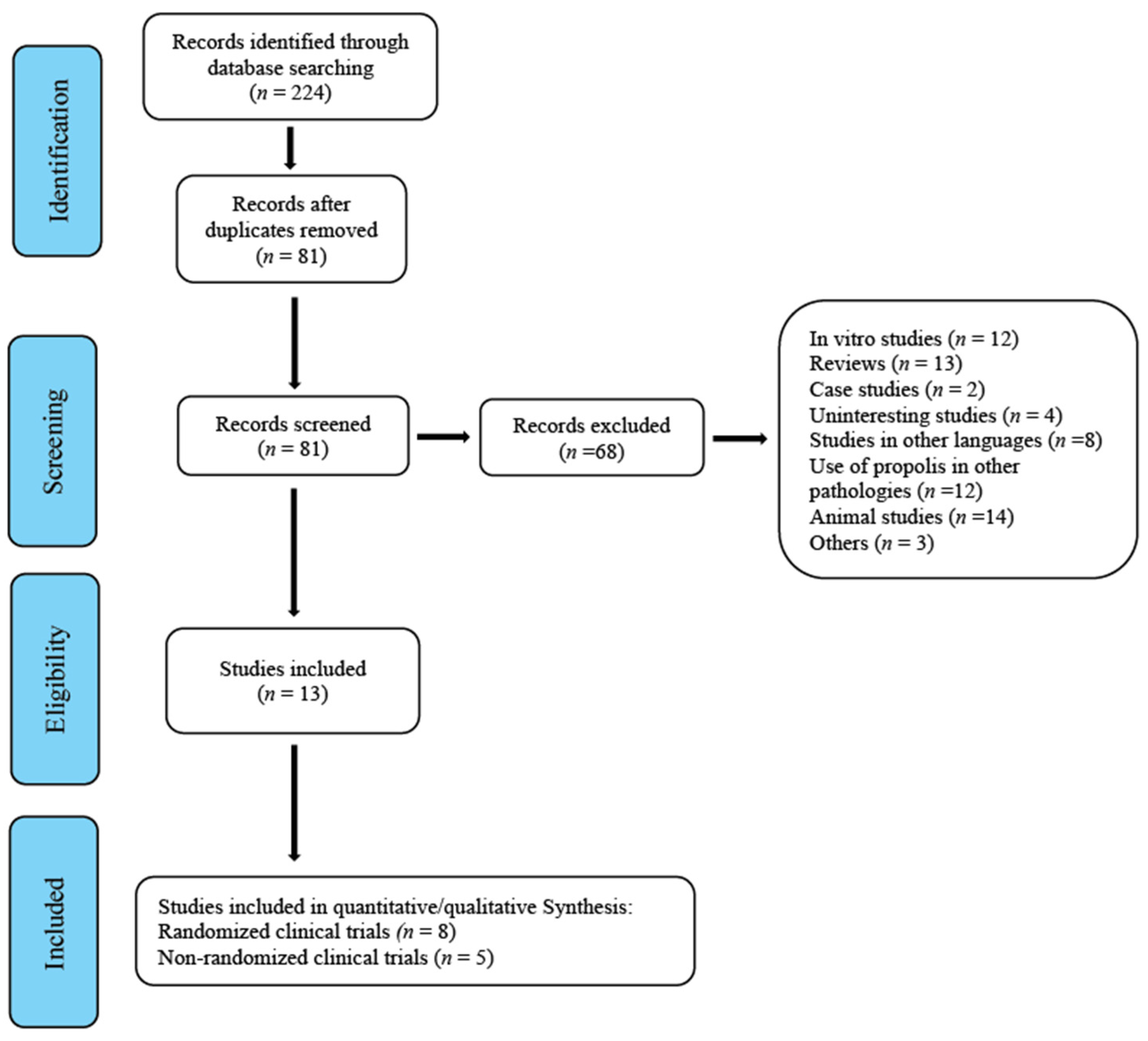
3. Results
3.1. Characteristics of the Studies
3.2. Methodological Quality of the Included Randomized Studies
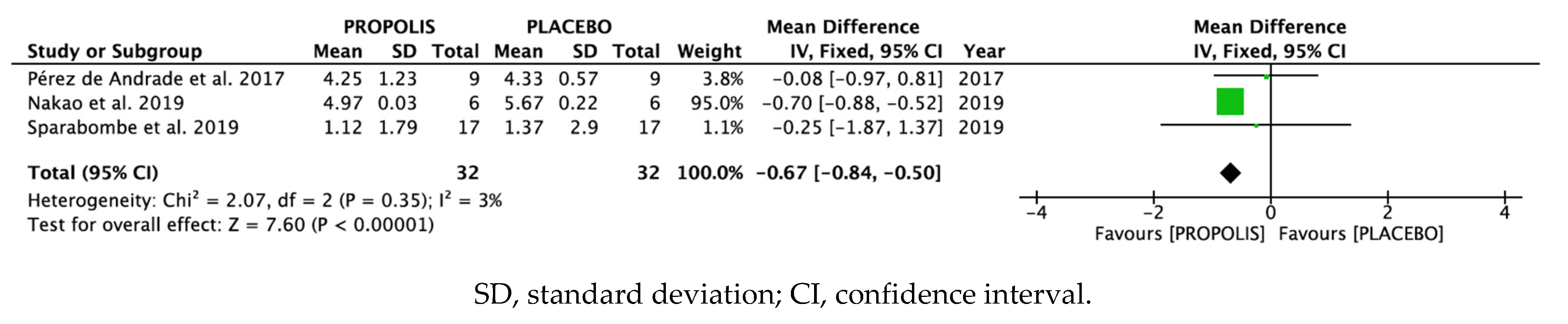
3.3. Results of the Meta-Analysis
3.4. Publication Bias and Heterogeneity
3.5. Results of Systematic Review
3.6. Assessment of Non-Randomized Clinical Trials
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Abbreviations
| ROS | Reactive oxygen substances |
| OS | Oxidative Stress |
| SAT | Salivary antioxidant test |
| IL | Interleukin |
| TNF-α | Tumor Necrosis Factor α |
| PP | Periodontal pockets |
| PPD | Probing pocket depth |
| PI | Plaque Index |
| PS | Plaque Score |
| PCR | Plaque Control Record |
| OHI | Oral Hygiene Index |
| API | Approximal Plaque Index |
| SBI | Sulcus Bleeding Index |
| PD | Pocket depth |
| GI | Gingival Index |
| BI | Bleeding Index |
| BoP | Bleeding on Probing |
| CAL | Clinical attachment level |
| SRP | Scaling and root planing |
| PBS | Papillary Bleeding Score |
| NOS | Newcastle–Ottawa Scale |
| GCF | Gingival crevicular fluid |
| EIBI | Eastman Interdental Bleeding Index |
References
- Przybyłek, I.; Karpiński, T.M. Antibacterial properties of propolis. Molecules 2019, 24, 2047. [Google Scholar] [CrossRef] [Green Version]
- Martinello, M.; Mutinelli, F. Antioxidant activity in bee products: A review. Antioxidants 2021, 10, 71. [Google Scholar] [CrossRef]
- Huang, S.; Zhang, C.P.; Wang, K.; Li, G.Q.; Hu, F.L. Recent advances in the chemical composition of propolis. Molecules 2014, 19, 19610–19632. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Şenel, E.; Demir, E. Bibliometric analysis of apitherapy in complementary medicine literature between 1980 and 2016. Compl. Ther. Clin. Pract. 2018, 31, 47–52. [Google Scholar] [CrossRef]
- Bankova, V.; De Castro, S.; Marcucci, M. Propolis: Recent advances in chemistry and plant origin. Apidologie 2000, 31, 3–15. [Google Scholar] [CrossRef]
- Marcucci, M.C.; Ferreres, F.; Garcıa-Viguera, C.; Bankova, V.; De Castro, S.; Dantas, A.; Valente, P.; Paulino, N. Phenolic compounds from Brazilian propolis with pharmacological activities. J. Ethnopharmacol. 2001, 74, 105–112. [Google Scholar] [CrossRef]
- Almuhayawi, M.S. Propolis as a novel antibacterial agent. Saudi J. Biol. Sci. 2020, 27, 3079–3086. [Google Scholar] [CrossRef] [PubMed]
- Pasupuleti, V.R.; Sammugam, L.; Ramesh, N.; Gan, S.H. Honey, propolis, and royal jelly: A comprehensive review of their biological actions and health benefits. Oxid. Med. Cell Longev. 2017, 2017, 1259510. [Google Scholar] [CrossRef] [PubMed]
- Richards, D. Review finds that severe periodontitis affects 11% of the world population. Evid. Based Dent. 2014, 15, 70–71. [Google Scholar] [CrossRef] [PubMed]
- Loesche, W.J. Grossman NS. Periodontal disease as a specific, albeit chronic, infection: Diagnosis and treatment. Clin. Microbiol. Rev. 2001, 14, 727–752. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Armitage, G.C.; Robertson, P.B. The biology, prevention, diagnosis and treatment of periodontal diseases: Scientific advances in the United States. J. Am. Dent. Assoc. 2009, 140, 36S–43S. [Google Scholar] [CrossRef]
- Nazir, M.A. Prevalence of periodontal disease, its association with systemic diseases and prevention. Int. J. Health Sci. 2017, 11, 72–80. [Google Scholar]
- Hasturk, H.; Kantarci, A. Activation and resolution of periodontal inflammation and its systemic impact. Periodontol. 2000 2015, 69, 255–273. [Google Scholar] [CrossRef] [PubMed]
- Kesarwala, A.H.; Krishna, M.C.; Mitchell, J.B. Oxidative stress in oral diseases. Oral Dis. 2016, 22, 9–18. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sculley, D.; Langley-Evans, S. Periodontal disease is associated with lower antioxidant capacity in whole saliva and evidence of increased protein oxidation. Clin. Sci. 2003, 105, 167–172. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Pendyala, G.; Thomas, B.; Kumari, S. The challenge of antioxidants to free radicals in periodontitis. J. Ind. Soc. Periodontol. 2008, 12, 79–83. [Google Scholar] [CrossRef]
- Borges, I., Jr.; Moreira, E.A.; Filho, D.W.; de Oliveira, T.B.; da Silva, M.B.; Fröde, T.S. Proinflammatory and oxidative stress markers in patients with periodontal disease. Mediators Inflamm. 2007, 2007, 45794. [Google Scholar] [CrossRef] [PubMed]
- Wang, Y.; Andrukhov, O.; Rausch-Fan, X. Oxidative stress and antioxidant system in periodontitis. Front. Physiol. 2017, 8, 910. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hutton, B.; Ferrán Catalá-López, F.; Moher, D. The PRISMA statement extension for systematic reviews incorporating network meta-analysis: PRISMA-NMA. Med. Clin. 2016, 16, 262–266. [Google Scholar] [CrossRef]
- Jadad, A.R.; Moore, R.A.; Carroll, D.; Jenkinson, C.; Reynolds, D.J.; Gavaghan, D.J.; McQuay, H.J. Assessing the quality of reports of randomized clinical trials: Is blinding necessary? Control. Clin. Trials 1996, 17, 1–12. [Google Scholar] [CrossRef]
- Nakao, R.; Senpuku, H.; Ohnishi, M.; Takai, H.; Ogata, Y. Effect of topical administration of propolis in chronic periodontitis. Odontology 2020, 108, 704–714. [Google Scholar] [CrossRef]
- Sparabombe, S.; Monterubbianesi, R.; Tosco, V.; Orilisi, G.; Hosein, A.; Ferrante, L.; Putignano, A.; Orsini, G. Efficacy of an all-natural polyherbal mouthwash in patients with periodontitis: A single-blind randomized controlled trial. Front. Physiol. 2019, 22, 10632. [Google Scholar] [CrossRef]
- Giammarinaro, E.; Marconcini, S.; Genovesi, A.; Poli, G.; Lorenzi, C.; Covani, U. Propolis as an adjuvant to non-surgical periodontal treatment: A clinical study with salivary antioxidant capacity assessment. Minerva Stomatol. 2018, 67, 183–188. [Google Scholar]
- Piekarz, T.; Mertas, A.; Wiatrak, K.; Rój, R.; Kownacki, P.; Śmieszek-Wilczewska, J.; Kopczyńska, E.; Wrzoł, M.; Cisowska, M.; Szliszka, E.; et al. The influence of toothpaste containing Australian melaleuca alternifolia oil and ethanolic extract of polish propolis on oral hygiene and microbiome in patients requiring conservative procedures. Molecules 2017, 22, 1957. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Andrade, D.P.; Carvalho, I.C.S.; Gadoi, B.H.; Rosa, L.C.L.; Barreto, L.M.R.C.; Pallos, D. Subgingival irrigation with a solution of 20% propolis extract as an adjunct to non-surgical periodontal treatment: A preliminary study. J. Int. Acad. Periodontol. 2017, 19, 145–151. [Google Scholar] [PubMed]
- El-Sharkawy, H.M.; Anees, M.M.; Van Dyke, T.E. Propolis Improves periodontal status and glycemic control in patients with type 2 diabetes mellitus and chronic periodontitis: A randomized clinical trial. J. Periodontol. 2016, 87, 1418–1426. [Google Scholar] [CrossRef] [PubMed]
- Anauate-Netto, C.; Anido-Anido, A.; Leegoy, H.R.; Matsumoto, R.; Alonso, R.C.; Marcucci, M.C.; Paulino, N.; Bretz, W.A. Randomized, double-blind, placebo-controlled clinical trial on the effects of propolis and chlorhexidine mouthrinses on gingivitis. Braz. Dent. Sci. 2014, 17, 11–15. [Google Scholar] [CrossRef]
- Sanghani, N.N.; Bm, S.S.S. Health from the hive: Propolis as an adjuvant in the treatment of chronic periodontitis—A clinicomicrobiologic study. J. Clin. Diagn. Res. 2014, 8, ZC41–ZC44. [Google Scholar] [PubMed]
- Borgnakke, W.S. Systemic propolis (adjuvant to nonsurgical periodontal treatment) may aid in glycemic control and periodontal health in type 2 diabetes of long duration. J. Evid Based Dent. Pract. 2017, 17, 132–134. [Google Scholar] [CrossRef] [PubMed]
- Akhavan Karbassi, M.H.; Yazdi, M.F.; Ahadian, H.; SadrAbad, M.J. Randomized double blind placebo controlled trial of propolis for oral mucositis in patients receiving chemotherapy for head and neck cancer. Asian Pac. J. Cancer Prev. 2016, 17, 3611–3614. [Google Scholar]
- Bretz, W.A.; Paulino, N.; Nör, J.E.; Moreira, A. The effectiveness of propolis on gingivitis: A randomized controlled trial. J. Altern. Compl. Med. 2014, 20, 943–948. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mohsin, S.; Manohar, B.; Rajesh, S.; Asif, Y. The effects of a dentifrice containing propolis on Mutans Streptococci: A clinico-microbiological study. Ethiop. J. Health Sci. 2015, 25, 9–16. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Coutinho, A. Honeybee propolis extract in periodontal treatment: A clinical and microbiological study of propolis in periodontal treatment. Ind. J. Dent. Res. 2012, 23, 294. [Google Scholar] [CrossRef]
- Tanasiewicz, M.; Skucha-Nowak, M.; Dawiec, M.; Król, W.; Skaba, D.; Twardawa, H. Influence of hygienic preparations with a 3% content of ethanol extract of Brazilian propolis on the state of the oral cavity. Adv. Clin. Exp. Med. 2012, 21, 81–92. [Google Scholar] [PubMed]
- Pereira, E.M.; da Silva, J.L.; Silva, F.F.; De Luca, M.P.; Ferreira, E.F.; Lorentz, T.C.; Santos, V.R. Clinical evidence of the efficacy of a mouthwash containing propolis for the control of plaque and gingivitis: A phase II study. Evid. Based Compl. Alter. Med. 2011, 2011, 750249. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gebaraa, E.C.; Pustiglioni, A.N.; de Lima, L.A.; Mayer, M.P. Propolis extract as an adjuvant to periodontal treatment. Oral Health Prev. Dent. 2003, 1, 29–35. [Google Scholar]
- Gebaraa, E.C.; Lima, A.; Mayer, P.A. Propolis antimicrobial activity against periodontopathic bacteria. Braz. J. Microbiol. 2002, 33, 365–369. [Google Scholar] [CrossRef]
- Stang, A. Critical evaluation of the Newcastle-Ottawa scale for the assessment of the quality of nonrandomized studies in meta-analyses. Eur. J. Epidemiol. 2010, 5, 603–605. [Google Scholar] [CrossRef] [Green Version]
- Jayalekshmi, J.L.; Lakshmi, R.; Mukerji, A. Honey on oral mucositis: A randomized controlled trial. Gulf J. Oncol. 2016, 1, 30–37. [Google Scholar]
- Münstedt, K.; Männle, H. Using bee products for the prevention and treatment of oral mucositis induced by cancer treatment. Molecules 2019, 24, 3023. [Google Scholar] [CrossRef] [Green Version]
- Cherniack, E.P. Bugs as drugs, Part 1: Insects: The “new” alternative medicine for the 21st century? Altern. Med. Rev. 2010, 15, 124–135. [Google Scholar]
- Ozan, F.; Sümer, Z.; Polat, Z.A.; Er, K.; Ozan, U.; Deger, O. Effect of mouthrinse containing propolis on oral microorganisms and human gingival fibroblasts. Eur. J. Dent. 2007, 1, 195–201. [Google Scholar]
- Shabbir, A.; Rashid, M.; Tipu, H.N. Propolis—A hope for the future in treating resistant periodontal pathogens. Cureus 2016, 8, e682. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Eick, S.; Schäfer, G.; Kwieciński, J.; Atrott, J.; Henle, T.; Pfister, W. Honey—A potential agent against Porphyromonas gingivalis: An in vitro study. BMC Oral Health 2014, 14, 24. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Yoshimasu, Y.; Ikeda, T.; Sakai, N.; Yagi, A.; Hirayama, S.; Morinaga, Y.; Furukawa, S.; Nakao, R. Rapid bactericidal action of propolis against Porphyromonas gingivalis. J. Dent. Res. 2018, 97, 928–936. [Google Scholar] [CrossRef]
- Sharma, N.; Charles, C.H.; Lynch, M.C.; Qaqish, J.; Mcguire, J.A.; Galustians, J.G.; Kumar, L.D. Adjunctive benefit of an essential oil–containing mouthrinse in reducing plaque and gingivitis in patients who brush and floss regularly. J. Am. Dent. Assoc. 2004, 135, 496–504. [Google Scholar] [CrossRef]
- Cortelli, S.C.; Cortelli, J.R.; Holzhausen, M.; Franco, G.C.N.; Rebelo, R.Z.; Sonagere, A.S.; Queiroz Cda, S.; Costa, F.O. Essential oils in one-stage full-mouth disinfection: Double-blind, randomized clinical trial of long-term clinical, microbial and salivary effects. J. Clin. Periodontol. 2009, 36, 333–342. [Google Scholar] [CrossRef]
- Varela-López, A.; Quiles, J.L.; Cordero, M.; Giampieri, F.; Bullón, P. Oxidative stress and dietary fat type in relation to periodontal disease. Antioxidants 2015, 4, 322–344. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Toczewska, J.; Konopka, T. Activity of enzymatic antioxidants in periodontitis: A systematic overview of the literature. Dent. Med. Probl. 2019, 56, 419–426. [Google Scholar] [CrossRef] [Green Version]
- Tartaglia, G.M.; Gagliano, N.; Zarbin, L.; Tolomeo, G.; Sforza, C. Antioxidant capacity of human saliva and periodontal screening assessment in healthy adults. Arch. Oral Biol. 2017, 78, 34–38. [Google Scholar] [CrossRef]
- Miricescu, D.; Totan, A.; Calenic, B.; Mocanu, B.; Didilescu, A.; Mohora, M.; Spinu, T.; Greabu, M. Salivary biomarkers: Relationship between oxidative stress and alveolar bone loss in chronic periodontitis. Acta Odontol. Scand. 2014, 72, 47. [Google Scholar] [CrossRef] [PubMed]
- Wei, D.; Zhang, X.L.; Wang, Y.Z.; Yang, C.X.; Chen, G. Lipid peroxidation levels, total oxidant status and superoxide dismutase in serum, saliva and gingival crevicular fluid in chronic periodontitis patients before and after periodontal therapy. Aust. Dent. J. 2010, 55, 70–78. [Google Scholar] [CrossRef] [PubMed]
- Brock, G.R.; Butterworth, C.J.; Matthews, J.B.; Chapple, I.L. Local and systemic total antioxidant capacity in periodontitis and health. J. Clin. Periodontol. 2004, 31, 515–521. [Google Scholar] [CrossRef] [PubMed]
- Tsai, C.; Chen, H.S.; Chen, S.L.; Ho, Y.P.; Ho, K.Y.; Wu, Y.M.; Hung, C.C. Lipid peroxidation: A possible role in the induction and progression of chronic periodontitis. J. Periodontal. Res. 2005, 40, 378–384. [Google Scholar] [CrossRef] [PubMed]
- Aghel, S.; Pouramir, M.; Moghadamnia, A.A.; Moslemi, D.; Molania, T.; Ghassemi, L.; Motallebnejad, M. Effect of Iranian propolis on salivary total antioxidant capacity in gamma-irradiated rats. J. Dent. Res. Dent. Clin. Dent. Prosp. 2014, 8, 235–239. [Google Scholar]
- Murray, M.C.; Worthington, H.V.; Blinkhorn, A.S. A study to investigate the effect of a propolis-containing mouthrinse on the inhibition of de novo plaque formation. J. Clin. Periodontol. 1997, 24, 796–798. [Google Scholar] [CrossRef] [PubMed]
- Vanni, R.; Waldner-Tomic, N.M.; Belibasakis, G.N.; Attin, T.; Schmidlin, P.R.; Thurnheer, T. Antibacterial efficacy of a propolis toothpaste and mouthrinse against a supragingival multispecies biofilm. Oral Health Prev. Dent. 2015, 3, 531–535. [Google Scholar]
- Paulino, N.; Abreu, S.R.; Uto, Y.; Koyama, D.; Nagasawa, H.; Hori, H.; Dirsch, V.M.; Vollmar, A.M.; Scremin, A.; Bretz, W.A. Anti-inflammatory effects of a bioavailable compound, Artepillin C, in Brazilian propolis. Eur. J. Pharmacol. 2008, 10, 296–301. [Google Scholar] [CrossRef] [PubMed]
- Peterson, S.N.; Snesrud, E.; Schork, N.J.; Bretz, W.A. Dental caries pathogenicity: A genomic and metagenomic perspective. Int. Dent. J. 2011, 61, 11–22. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Matsha, T.E.; Prince, Y.; Davids, S.; Chikte, U.; Erasmus, R.T.; Kengne, A.P.; Davison, G.M. Oral microbiome signatures in diabetes mellitus and periodontal disease. J. Dent. Res. 2020, 99, 658–665. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| Study and Year | Randomization | Blinding | Dropouts | Total Score |
|---|---|---|---|---|
| Nakao et al. 2019 [21] | 2 | 2 | 1 | 5 |
| Sparabombe et al. 2019 [22] | 2 | 1 | 1 | 4 |
| Giammarinaro et al. 2018 [23] | 2 | 1 | 1 | 4 |
| Piekarz et al. 2017 [24] | 2 | 1 | 1 | 4 |
| Perez de Andrade et al. 2017 [25] | 1 | 2 | 1 | 4 |
| Sharkawy et al. 2016 [26] | 2 | 1 | 1 | 4 |
| Anauate-Netto et al. 2014 [27] | 2 | 1 | 1 | 4 |
| Sanghani et al. 2014 [28] | 2 | 1 | 1 | 4 |
| Study and Aim | Participants | Interventions | Outcomes |
|---|---|---|---|
| Nakao et al. 2019. | 24 patients with moderate to severe chronic periodontitis. | Propolis ointments were administered to each study group (three times at 1-month intervals) to a tooth with periodontal pockets ≥ 5 mm without local anesthesia. The deepest pocket in the mouth of each subject was chosen. | Treatment with propolis significantly improved PPD and CAL. Reduction of P. gingivalis in the gingival crevicular fluid. |
| Aim: clinical applicability of propolis as an alternative/adjuvant therapy against periodontitis [21]. | |||
| Sparabombe et al. 2019. | 40 patients with periodontitis. | For 3 months, a polyherbal mouthwash (propolis resin extract, Plantago lanceolata, Salvia) was prescribed to the test group and a placebo mouthwash to the control group. | Polyherbal mouthwash for 3 months |
| Aim: evaluate the anti-inflammatory effect of polyherbal mouthwash (propolis resin extract, Plantago lanceolata, Salvia) | reduced inflammation and plaque | ||
| in patients with periodontitis [22]. | accumulation. Beneficial effect in patients with moderate or severe periodontitis. | ||
| Giammarinaro et al. 2018. | 40 patients with gingivitis, PPD < 3 mm. | Hydroalcoholic propolis solution (6%) as a mouthwash twice a day for 2 weeks. No propolis in the control group. | Test patients (propolis) had better results in reducing oxidative stress. |
| Aim: evaluate the effectiveness of a propolis and herbal formula, compared with chlorhexidine-based formulas [23]. | |||
| Piekarz et al. 2017 | 51 patients. | Both groups brushed their teeth twice a day with the received toothpaste for 2 min. Evaluation of the OHI, API and SBI indices, and collection of material for microbiological examination were carried out at the initial visit, at 7 days and at 4 weeks. | Significant reduction in the PI and the SBI in the propolis group. Candida albicans was eradicated in the group of patients using the active preparation. Bacteria responsible for the development of gingivitis were eradicated in the study group. |
| Aim: evaluate toothpaste with active ingredients of plant origin, ethanolic extract of propolis and tea tree oil on the microbiome compared with patients treated with preventive procedures [24]. | the study group received toothpaste with ethanolic extract of propolis. The control group received the placebo. | ||
| Perez de Andrade et al. 2017. | 18 patients diagnosed with mild to moderate and moderate to severe chronic periodontal disease, with PP ≥ 5 mm deep in uniradicular teeth. | Hydroalcoholic solution of propolis extract 20%. | Probing was reduced with irrigation of 20% propolis extract hydroalcoholic solution as an adjunct in periodontal treatment compared with the control (saline solution). |
| Aim: evaluate the effect of subgingival irrigation of periodontal pockets with a hydroalcoholic solution of 20% propolis extract as a complement to periodontal therapy [25]. | |||
| Sharkawy et al. 2016. | Patients with Type 2 diabetes, with chronic periodontitis with PPD on probing and clinical attachment loss ≥ 5 mm with detectable bleeding on probing in at least one site of each sextant. | Propolis and corresponding placebo capsules. The patients were instructed to take only one capsule per day. All people received SRP. | PD reduction and the increase in CAL were significantly greater in the propolis group than in the placebo group at 3 and 6 months. |
| Aim: evaluate propolis supplementation in individuals with chronic periodontitis and Type 2 diabetes mellitus who received SRP [26]. | |||
| Anauate-Netto et al. 2014. | 60 participants; | Groups (1) 2% propolis, (2) 0.12% chlorhexidine and (3) placebo; two rinses a day for 28 days. Papillary bleeding was measured at the beginning of the study and 28 days later. | Reduction in papillary bleeding for the propolis group only. |
| Aim: compare the effects of propolis and chlorhexidine mouthrinses on gingival health [27]. | three groups | ||
| Sanghani et al. 2014. | 20 patients; two groups. | Propolis (not exposed to the oral cavity) was placed on the test sites after completing the SRP. The clinical parameters were evaluated at 15 days and 1 month after treatment. | Reduction of GI, BI, PPD and CAL in the test group treated with scaling and root planing and propolis. |
| Aim: clinical and microbiological evaluation of the subgingival propolis extract as a complement to SRP in the treatment of periodontitis [28]. | Lower prevalence of Porphyromona gingivalis, Porphyromona intermedia and Fusobacterium nucleatum as compared with the control group. |
| Study and Aim | Participants | Interventions | Outcomes | Experimental Propolis Group p-Values |
|---|---|---|---|---|
| Mohsin et al. 2015 Aim: to evaluate the antibacterial efficacy of a propolis-based toothpaste on streptococcus mutans that colonized the oral cavity of young patients [32]. | 30 | Subjects were instructed to brush once a day for 3 min for a period of 4 weeks with propolis toothpaste. After 24 h of oral prophylaxis, reference samples were collected. | Statistically significant reduction in mean value of mutant streptococci after 4 weeks compared with the baseline. | 1st week p = 0.000; 4th week p = 0.000. |
| Coutinho et al. 2012 Aim: to evaluate the effects of subgingival irrigation with propolis extract in deep periodontal pockets by means of clinical and microbiological parameters [33]. | 20 | Subgingival plaque sampling was performed at the beginning of the study and root scaling and planing. Two weeks later, the selected periodontal areas underwent the following treatments: irrigation with a hydroalcoholic solution of propolis extract (Group A), irrigation with a placebo (Group B) or no additional treatment (Group C). | Decrease in Group A anaerobic bacteria compared with the other groups. Porphyromona gingivalis: minor levels in test group. | Group A (propolis). A decrease in the total viable counts of anaerobic bacteria; p = 0.007. |
| Tanasiewicz et al. 2012 Aim: influence of the application of toothpaste with 3% ethanol–propolis extract on the state of the oral cavity [34]. | 80 | Pastes/gels: toothpaste with propolis, toothpaste without propolis, gel with propolis and gel without propolis. | Efficacy of preparations containing 3% ethanolic propolis extract in all groups. | API after 8 weeks compared with the first week; p = 0.0679 OHI: not statistically significant. |
| Pereira et al. 2011. Aim: clinical efficacy of a 5.0% Brazilian green propolis mouthwash for plaque and gingivitis control [35]. | 25 | Subjects were instructed to brush their teeth and rinse with 10 mL of 5% green propolis twice daily. | Evidence of the efficacy of alcohol-free mouthwash containing 5% Brazilian green propolis for plaque and gingivitis control. | GI at 45 and 90 days: reduction of gingivitis greater than 40%, statistically significant; p < 0.05. PI at 45 and 90 days: reduction in plaque index, statistically significant; p < 0.05. |
| Gebaraa et al. 2003 Aim: to evaluate subgingival irrigation with propolis extract [36]. | 20 | Group A: irrigation with propolis extract twice a week for 2 weeks. Group B: irrigation with 3 mL of a placebo. Group C (control group): no treatment. | Decrease in anaerobic bacteria and increase in P. gingivalis. Absence of bleeding on probing at the end of the study. | Decrease in total counts of anaerobic bacteria; p = 0.007. Increase in sites with low levels of Porphyromonas gingivalis; p = 0.005. |
| First Author, Publication Year | Quality Evaluation | Case definition | Representativeness | Selection of Controls | Definition of Controls | Comparability | Ascertainment of Exposure | Same Method? | Non-Response Rate | Score |
|---|---|---|---|---|---|---|---|---|---|---|
| Mohsin et al. 2015 [32] | 1 | 1 | 1 | 1 | 1 | 1 | 0 | 1 | 0 | 7 |
| Coutinho et al. 2012 [33] | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 0 | 8 |
| Tanasiewicz et al. 2012 [34] | 1 | 1 | 1 | 1 | 1 | 1 | 0 | 1 | 1 | 8 |
| Pereira et al. 2011 [35] | 1 | 1 | 1 | 1 | 1 | 1 | 0 | 1 | 0 | 7 |
| Gebaraa et al. 2003 [36] | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 0 | 8 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
López-Valverde, N.; Pardal-Peláez, B.; López-Valverde, A.; Flores-Fraile, J.; Herrero-Hernández, S.; Macedo-de-Sousa, B.; Herrero-Payo, J.; Ramírez, J.M. Effectiveness of Propolis in the Treatment of Periodontal Disease: Updated Systematic Review with Meta-Analysis. Antioxidants 2021, 10, 269. https://doi.org/10.3390/antiox10020269
López-Valverde N, Pardal-Peláez B, López-Valverde A, Flores-Fraile J, Herrero-Hernández S, Macedo-de-Sousa B, Herrero-Payo J, Ramírez JM. Effectiveness of Propolis in the Treatment of Periodontal Disease: Updated Systematic Review with Meta-Analysis. Antioxidants. 2021; 10(2):269. https://doi.org/10.3390/antiox10020269
Chicago/Turabian StyleLópez-Valverde, Nansi, Beatriz Pardal-Peláez, Antonio López-Valverde, Javier Flores-Fraile, Silvia Herrero-Hernández, Bruno Macedo-de-Sousa, Julio Herrero-Payo, and Juan Manuel Ramírez. 2021. "Effectiveness of Propolis in the Treatment of Periodontal Disease: Updated Systematic Review with Meta-Analysis" Antioxidants 10, no. 2: 269. https://doi.org/10.3390/antiox10020269