
Alcohol Consumption Assessed by a Biomarker and Self-Reported Drinking in a Sample of Pregnant Women in the South of Europe: A Comparative Study

 ,
,  ,
,  , ,
, ,
Abstract
:1. Introduction
2. Materials and Methods
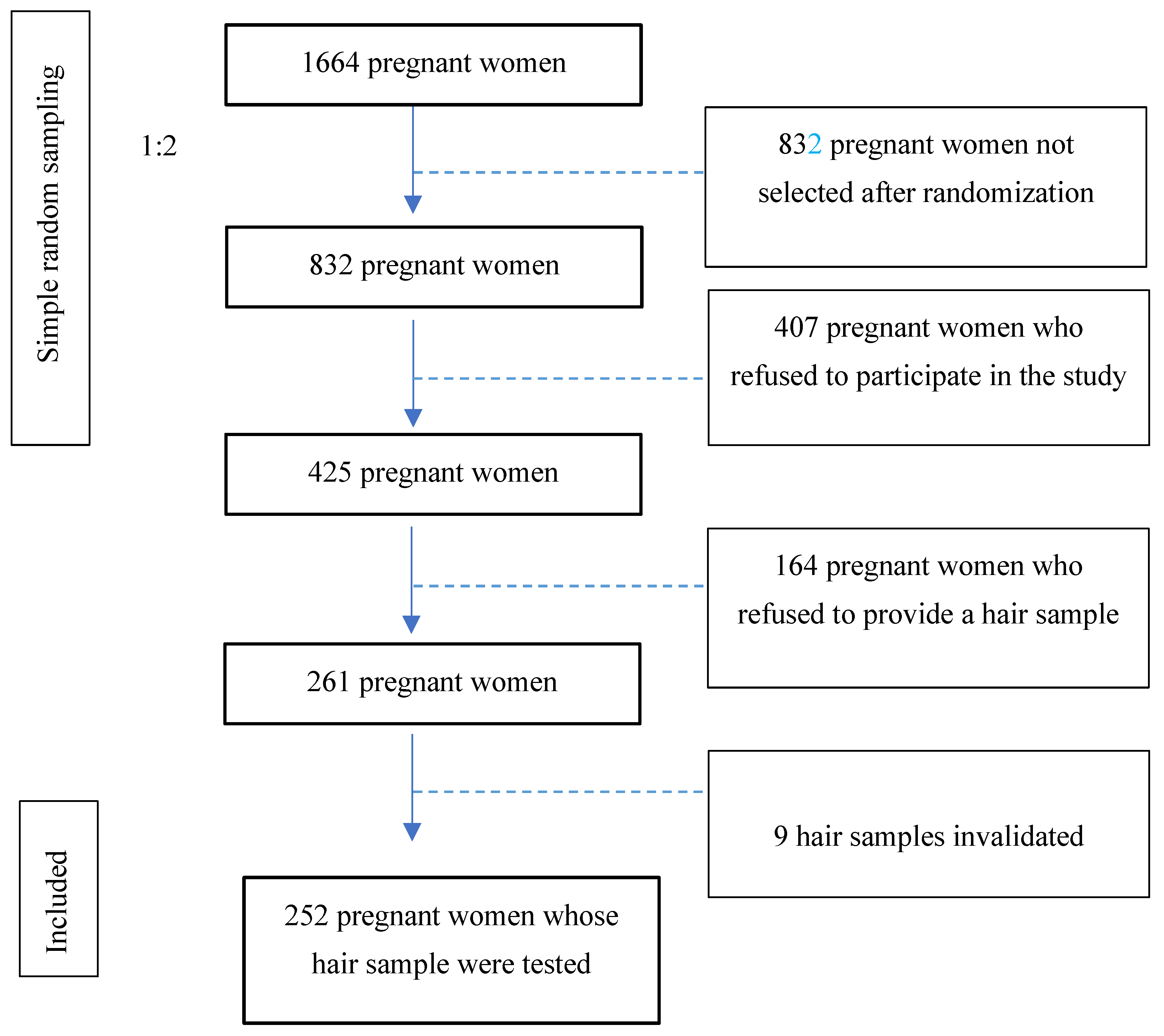
2.1. Study Design
2.2. Data Collection and Participants
2.3. Maternal Hair Sample Collection
2.4. Ethical Aspects
2.5. Questionnaire
2.6. Variables
- Sociodemographic variables: age (categorized in <25 years; 26–30 years; 31–35 years, more than 35 years old), education level (none, primary, secondary, university), employment situation (stable, vulnerable—defined as the sum of employment status groups of own-account workers and contributing family workers—self-definition as “housewife”, or other) if the pregnant woman has a partner or not, her country of origin (Spain or another country), size and weight (used to calculate body mass index according to the World Health Organization, classified as thinness (below 18.5), normal weight (18.6–24.9), pre-obesity (25–29.9), class 1 obesity (30–34.9), and class 2–3 obesity regrouped (more than 35)).
- Obstetric variable: number of pregnancies, including the current one, classified as 1 or more than one.
- Alcohol Consumption-Related Variables
- -
- Average number of grams of pure alcohol consumed per day during pregnancy, according to self-reported alcohol consumption (including days without consumption). From a selection of items from the AUDIT screening tool [18], the average amount of alcohol grams consumed per day was estimated in each pregnant woman according to the frequency of consumption of each type of beverage, their average level of alcohol, and the usual volume of each type of glass used to drink them in the city of Seville. Subsequently, this variable (grammes of pure alcohol per day consumed during pregnancy) was classified into three values: non-consumption, lower than or equal to 1.96 g/day, and more than 1.96 g/day, being 1.96 g, the average amount consumed per day by pregnant women who declared to drink alcohol during their pregnancy [19].
- -
- Alcohol consumption was determined from the analysis to detect the EtG metabolite, evaluating the concentration of pg/mg in hair. This variable was categorized into 3 groups: Negative: no EtG detected; Abstinence (<5 pg/mg); and Consumption (>5 pg/mg).
2.7. Hair Analysis for the Detection of Alcohol Consumption (EtG)
2.8. Data Analysis
3. Results
3.1. Descriptive Analysis of the Sample
3.2. Alcohol Consumption in Pregnant Women, According to Metabolite Analysis
3.3. Comparison between Self-Reported Consumption and the One Detected in the Metabolite
3.4. Sociodemographic and Obstetric Variability of Alcohol Consumption Evaluated through Metabolite Analysis
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Lemoine, P.; Harousseau, H.; Borteyru, J.P.; Menuet, J.C. Children of Alcoholic Parents—Observed Anomalies: Discussion of 127 Cases. Ther. Drug Monit. 2003, 25, 132–136. [Google Scholar] [CrossRef] [PubMed]
- Keum, D.; Pultorak, K.; Meredith, M.A.; Medina, A.E. Effects of developmental alcohol exposure on cortical multisensory integration. Eur. J. Neurosci. 2023, 57, 784–795. [Google Scholar] [CrossRef]
- Popova, S.; Charness, M.E.; Burd, L.; Crawford, A.; Hoyme, H.E.; Mukherjee, R.A.; Riley, E.P.; Elliott, E.J. Fetal alcohol spectrum disorders. Nat. Rev. Dis. Primer. 2023, 9, 11. [Google Scholar] [CrossRef] [PubMed]
- Pichini, S.; Busardò, F.P.; Garcia-Algar, O. Only Total Abstinence from Alcohol Consumption During Pregnancy Guarantees Absolute Absence of Any Deleterious Effect in the Fetus and Child. J. Stud. Alcohol. Drugs. 2020, 81, 220–221. [Google Scholar] [CrossRef] [PubMed]
- Popova, S.; Lange, S.; Probst, C.; Gmel, G.; Rehm, J. Estimation of national, regional, and global prevalence of alcohol use during pregnancy and fetal alcohol syndrome: A systematic review and meta-analysis. Lancet Glob. Health 2017, 5, e290–e299. [Google Scholar] [CrossRef]
- World Health Organization. Global Status Report on Alcohol and Health 2018; WHO: Geneva, Switzerland, 2018; Available online: https://www.who.int/publications/i/item/9789241565639 (accessed on 3 August 2023).
- Corrales-Gutierrez, I.; Mendoza, R.; Gomez-Baya, D.; Leon-Larios, F. Pregnant Women’s Risk Perception of the Teratogenic Effects of Alcohol Consumption in Pregnancy. J. Clin. Med. 2019, 8, 907. [Google Scholar] [CrossRef]
- Pichini, S.; Busardò, F.P.; Ceccanti, M.; Tarani, L.; Pacifici, R. Unreliable estimation of prevalence of fetal alcohol syndrome. Lancet Glob. Health 2017, 5, e574. [Google Scholar] [CrossRef] [PubMed]
- Strandberg-Larsen, K.; Andersen, A.M.N.; Kesmodel, U.S. Unreliable estimation of prevalence of fetal alcohol syndrome. Lancet Glob. Health 2017, 5, e573. [Google Scholar] [CrossRef]
- Sordo, L.; Barrio, G.; Bravo, M.J.; Villalbí, J.R.; Espelt, A.; Neira, M.; Regidor, E. Estimating average alcohol consumption in the population using multiple sources: The case of Spain. Popul. Health Metr. 2016, 14, 21. [Google Scholar] [CrossRef]
- Skagerstróm, J.; Chang, G.; Nilsen, P. Predictors of Drinking During Pregnancy: A Systematic Review. J. Womens Health 2011, 20, 901–913. [Google Scholar] [CrossRef]
- Tappin, D.; Mackay, D.; Reynolds, L.; Fitzgerald, N. Minimizing sample bias due to stigmatized behaviours: The representativeness of participants in a cohort study of alcohol in pregnancy. BMC Med. Res. Methodol. 2022, 22, 138. [Google Scholar] [CrossRef] [PubMed]
- Joya, X.; Friguls, B.; Ortigosa, S.; Papaseit, E.; Martínez, S.E.; Manich, A.; Garcia-Algar, O.; Pacifici, R.; Vall, O.; Pichini, S. Determination of maternal-fetal biomarkers of prenatal exposure to ethanol: A review. J. Pharm. Biomed. Anal. 2012, 69, 209–222. [Google Scholar] [CrossRef] [PubMed]
- Manich, A.; Velasco, M.; Joya, X.; García-Lara, N.R.; Pichini, S.; Vall, O.; García-Algar, O. Validez del cuestionario de consumo materno de alcohol para detectar la exposición prenatal. An. Pediatría 2012, 76, 324–328. [Google Scholar] [CrossRef] [PubMed]
- Cabarcos, P.; Álvarez, I.; Tabernero, M.J.; Bermejo, A.M. Determination of direct alcohol markers: A review. Anal. Bioanal. Chem. 2015, 407, 4907–4925. [Google Scholar] [CrossRef]
- Chiandetti, A.; Hernandez, G.; Mercadal-Hally, M.; Alvarez, A.; Andreu-Fernandez, V.; Navarro-Tapia, E.; Bastons-Compta, A.; Garcia-Algar, O. Prevalence of prenatal exposure to substances of abuse: Questionnaire versus biomarkers. Reprod. Health 2017, 14, 137. [Google Scholar] [CrossRef]
- Skagerström, J.; Alehagen, S.; Häggström-Nordin, E.; Årestedt, K.; Nilsen, P. Prevalence of alcohol use before and during pregnancy and predictors of drinking during pregnancy: A cross sectional study in Sweden. BMC Public Health 2013, 13, 780. [Google Scholar] [CrossRef]
- Zammit, S.L.; Skouteris, H.; Wertheim, E.H.; Paxton, S.J.; Milgrom, J. Pregnant Women’s Alcohol Consumption: The Predictive Utility of Intention to Drink and Prepregnancy Drinking Behavior. J. Womens Health 2008, 17, 1513–1522. [Google Scholar] [CrossRef]
- Higgins-Biddle, J.C.; Babor, T.F. A review of the Alcohol Use Disorders Identification Test (AUDIT), AUDIT-C, and USAUDIT for screening in the United States: Past issues and future directions. Am. J. Drug Alcohol Abuse 2018, 44, 578–586. [Google Scholar] [CrossRef]
- Marchei, E.; Gomez-Ruiz, L.M.; Acosta-López, A.; Ramos-Gutiérrez, R.Y.; Varela-Busaka, M.B.; Lombroni, C.; Andreu-Fernandez, V.; Pichini, S.; Garcia-Algar, O. Assessment of alcohol consumption in Mexican pregnant women by hair testing of ethyl glucuronide. Alcohol 2023, 111, 59–65. [Google Scholar] [CrossRef]
- Biondi, A.; Freni, F.; Carelli, C.; Moretti, M.; Morini, L. Ethyl glucuronide hair testing: A review. Forensic. Sci. Int. 2019, 300, 106–119. [Google Scholar] [CrossRef]
- Soht. Consensus for the Use of Alcohol Markers in Hair for Supporting the Assessment of Abstinence and Chronic Alcohol Consumption [Internet]. 2019. Available online: http://www.soht.org/images/pdf/Revision_2019_Alcoholmarkers.pdf (accessed on 3 August 2023).
- Triolo, V.; Spanò, M.; Buscemi, R.; Gioè, S.; Malta, G.; Čaplinskiene, M.; Vaiano, F.; Bertol, E.; Zerbo, S.; Albano, G.D.; et al. EtG Quantification in Hair and Different Reference Cut-Offs in Relation to Various Pathologies: A Scoping Review. Toxics 2022, 10, 682. [Google Scholar] [CrossRef] [PubMed]
- Kerekes, I.; Yegles, M. Coloring, Bleaching, and Perming: Influence on EtG Content in Hair. Ther. Drug Monit. 2013, 35, 527–529. [Google Scholar] [CrossRef] [PubMed]
- Testa, M.; Reifman, A. Individual differences in perceived riskiness of drinking in pregnancy: Antecedents and consequences. J. Stud. Alcohol. 1996, 57, 360–367. [Google Scholar] [CrossRef]
- Corrales-Gutierrez, I.; Mendoza, R.; Gomez-Baya, D.; Leon-Larios, F. Understanding the Relationship between Predictors of Alcohol Consumption in Pregnancy: Towards Effective Prevention of FASD. Int. J. Environ. Res. Public Health 2020, 17, 1388. [Google Scholar] [CrossRef] [PubMed]
- Muggli, E.; O’Leary, C.; Donath, S.; Orsini, F.; Forster, D.; Anderson, P.J.; Lewis, S.; Nagle, C.; Craig, J.M.; Elliott, E.; et al. “Did you ever drink more?” A detailed description of pregnant women’s drinking patterns. BMC Public Health 2016, 16, 683. [Google Scholar] [CrossRef] [PubMed]
- Mårdby, A.C.; Lupattelli, A.; Hensing, G.; Smedberg, J.; Nordeng, H. Factors associated with alcohol consumption during pregnancy—A cross-sectional study in 15 European countries. Eur. J. Public Health 2014, 24 (Suppl. S2), cku164-106. [Google Scholar] [CrossRef]
- Jarque, P.; Roca, A.; Gomila, I.; Marchei, E.; Tittarelli, R.; Elorza, M.Á.; Sanchís, P.; Barceló, B. Role of Neonatal Biomarkers of Exposure to Psychoactive Substances to Identify Maternal Socio-Demographic Determinants. Biology 2021, 10, 296. [Google Scholar] [CrossRef]
- Cameron, C.M.; Davey, T.M.; Kendall, E.; Wilson, A.; McClure, R.J. Changes in alcohol consumption in pregnant Australian women between 2007 and 2011. Med. J. Aust. 2013, 199, 355–357. [Google Scholar] [CrossRef]
- Romero-Rodríguez, E.; Cuevas, L.; Simón, L.; ECEMC Peripheral Group; Bermejo-Sánchez, E.; Galán, I. Changes in Alcohol Intake During Pregnancy in Spain, 1980 to 2014. Alcohol Clin. Exp. Res. 2019, 43, 2367–2373. [Google Scholar] [CrossRef]
- Doherty, E.; Kingsland, M.; Wolfenden, L.; Wiggers, J.; Dray, J.; Hollis, J.; Elliott, E.J.; Daly, J.B.; Bailey, K.A.; Attia, J.; et al. Implementation strategies to improve preconception and antenatal care for tobacco smoking, alcohol consumption and weight management: A systematic review protocol. Syst. Rev. 2019, 8, 285. [Google Scholar] [CrossRef]
- Dahl, B.; Johannessen, A.; Bondas, T. Opening Pandora’s box: A meta-ethnography aboutalcohol use in pregnancy from midwives’ and otherhealthcare providers’ perspectives. Eur. J. Midwifery 2023, 7, 14. [Google Scholar] [CrossRef] [PubMed]
- Taylor, A.; Whittaker, A.; Chandler, A.; Carnegie, E. Accounts of women identified as drinking at ‘high risk’ during pregnancy: A meta-ethnography of missing voices. Int. J. Drug Policy 2023, 117, 104061. [Google Scholar] [CrossRef] [PubMed]
- Bennett, R.; Bowden, C. Can routine screening for alcohol consumption in pregnancy be ethically and legally justified? J. Med. Ethics 2022, 48, 512–516. [Google Scholar] [CrossRef] [PubMed]




{kind=link}
{kind=link}
{kind=link}
| Variables | Categories | Percentage | n |
|---|---|---|---|
| Age | Up to 25 years old | 12.5 | 53 |
| 26–30 years old | 23.3 | 99 | |
| 31–35 years old | 37.9 | 161 | |
| >35 years old | 26.4 | 112 | |
| Educational level | None | 2.4 | 10 |
| Primary | 37.9 | 161 | |
| Secondary | 22.1 | 94 | |
| University | 37.6 | 160 | |
| Employment situation | Stable | 39.4 | 167 |
| Vulnerable | 45.4 | 193 | |
| Housewife | 5.9 | 25 | |
| Other | 9.2 | 39 | |
| Partner | Yes | 98.1 | 417 |
| No | 1.9 | 8 | |
| Country of origin | Spain | 92.2 | 390 |
| Other | 7.8 | 33 | |
| BMI | Thinness (<18.5) | 0.2 | 1 |
| Normal weight (18.6–24.9) | 52.3 | 218 | |
| Overweight (25–29.9) | 28.8 | 120 | |
| Class 1 Obesity (30–34.9) | 13.2 | 55 | |
| Class 2–3 Obesity (>35) | 5.5 | 23 | |
| Number of pregnancies (including the current one) | One | 40.5 | 171 |
| More than one | 59.5 | 251 |
| No Consumption | N (%) |
|---|---|
| Negative | 160 (63.5%) |
| Minimum levels of EtG, comparable to abstinence | 41 (16.3%) |
| Consumption | |
| Social drinker | 49 (19.4%) |
| Chronic consumption | 2 (0.8%) |
| Prevalence of consumption | 51 (20.2%) |
| EtG Categorized Consumption | Total | |||||
|---|---|---|---|---|---|---|
| Negative | Abstinence | Consumption | ||||
| Self-reported consumption | 0 g/day | N | 122 | 27 | 30 | 179 |
| % | 68.2 | 15.1 | 16.8 | 100 | ||
| Adjusted residuals | 3.1 | −0.7 | −3.1 | |||
| <1.96 g/day | N | 14 | 7 | 16 | 37 | |
| % | 37.8 | 18.9 | 43.2 | 100 | ||
| Adjusted residuals | −3.4 | 0.5 | 3.6 | |||
| >1.96 g/day | N | 9 | 3 | 3 | 15 | |
| % | 60 | 20 | 20 | 100 | ||
| Adjusted residuals | ||||||
| Total | N | 145 | 37 | 49 | 231 | |
| % | 62.8 | 16 | 21.2 | 100 | ||
| EtG No Consumption n | EtG Consumption n | |
|---|---|---|
| Self-reported No Consumption | 149 | 30 |
| Self-reported Consumption | 33 | 19 |
| Negative n (%) | Abstinence n (%) | Consumption n (%) | χ2 | p | Cramér’s V | ||
|---|---|---|---|---|---|---|---|
| Age | 1.37 | 0.968 | 0.052 | ||||
| Less than 25 | 21 (63.6) | 7 (21.2) | 5 (15.2) | ||||
| 26–30 | 41 (63.1) | 11 (16.9) | 13 (20) | ||||
| 31–35 | 60 (62.5) | (15) 15.6 | (21) 21.9 | ||||
| >35 | 38 (65.5) | 8 (13.8) | 12 (20.7) | ||||
| Country of origin | 4.58 | 0.101 | 0.135 | ||||
| Spain | 148 (64.1) | 40 (17.3) | 43 (18.6) | ||||
| Other | 11 (57.9) | 1 (5.3) | 7 (36.8) | ||||
| Employment situation | 10.31 | 0.112 | 0.143 | ||||
| Stable | 64 (62.7) | 18 (17.6) | 20 (19.6) | ||||
| Vulnerable | 75 (68.2) | 18 (16.4) | 17 (15.5) | ||||
| Housewife | 8 (40) | 3 (15) | 9 (45) | ||||
| Other | 13 (65) | 2 (10) | 5 (25) | ||||
| Partner | 1.53 | 0.465 | 0.078 | ||||
| Yes | 156 (63.4) | 41 (16.7) | 49 (19.9) | ||||
| No | 4 (66.7) | 0 | 2 (33.3) | ||||
| Educational level | 6.56 | 0.363 | 0.114 | ||||
| None | 5 (83.3) | 0 | 1 (16.7) | ||||
| Primary | 55 (55) | 21 (21) | 24 (24) | ||||
| Secondary | 34 (68) | 8 (16) | 8 (16) | ||||
| University | 66 (68.8) | 12 (12.5) | 18 (18.8) | ||||
| Number of pregnancies | 2.81 | 0.246 | 0.106 | ||||
| (including this one) | One | 61 (64.2) | 19 (20) | 15 (15.8) | |||
| More than one | 99 (63.1) | 22 (14) | 36 (22.9) | ||||
| BMI | 11.04 | 0.199 | 0.148 | ||||
| Thinness | 0 | 0 | 1 (100) | ||||
| Normal weight | 89 (64) | 26 (18.7) | 24 (17.3) | ||||
| Overweight | 45 (64.3) | 6 (8.6) | 19 (27.1) | ||||
| Class 1 obesity | 18 (62.1) | 7 (24.1) | 4 (13.8) | ||||
| Class 2–4 obesity | 8 (61.5) | 2 (15.4) | 3 (23.1) |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Corrales-Gutierrez, I.; Gomez-Baya, D.; Leon-Larios, F.; Medero-Canela, R.; Marchei, E.; Mendoza-Berjano, R.; García-Algar, Ó. Alcohol Consumption Assessed by a Biomarker and Self-Reported Drinking in a Sample of Pregnant Women in the South of Europe: A Comparative Study. Toxics 2023, 11, 930. https://doi.org/10.3390/toxics11110930
Corrales-Gutierrez I, Gomez-Baya D, Leon-Larios F, Medero-Canela R, Marchei E, Mendoza-Berjano R, García-Algar Ó. Alcohol Consumption Assessed by a Biomarker and Self-Reported Drinking in a Sample of Pregnant Women in the South of Europe: A Comparative Study. Toxics. 2023; 11(11):930. https://doi.org/10.3390/toxics11110930
Chicago/Turabian StyleCorrales-Gutierrez, Isabel, Diego Gomez-Baya, Fatima Leon-Larios, Rocío Medero-Canela, Emilia Marchei, Ramon Mendoza-Berjano, and Óscar García-Algar. 2023. "Alcohol Consumption Assessed by a Biomarker and Self-Reported Drinking in a Sample of Pregnant Women in the South of Europe: A Comparative Study" Toxics 11, no. 11: 930. https://doi.org/10.3390/toxics11110930