
Efficacy and Safety of Bulevirtide plus Tenofovir Disoproxil Fumarate in Real-World Patients with Chronic Hepatitis B and D Co-Infection

 , , , , , and
, , , , , and
Abstract
:1. Introduction
2. Results
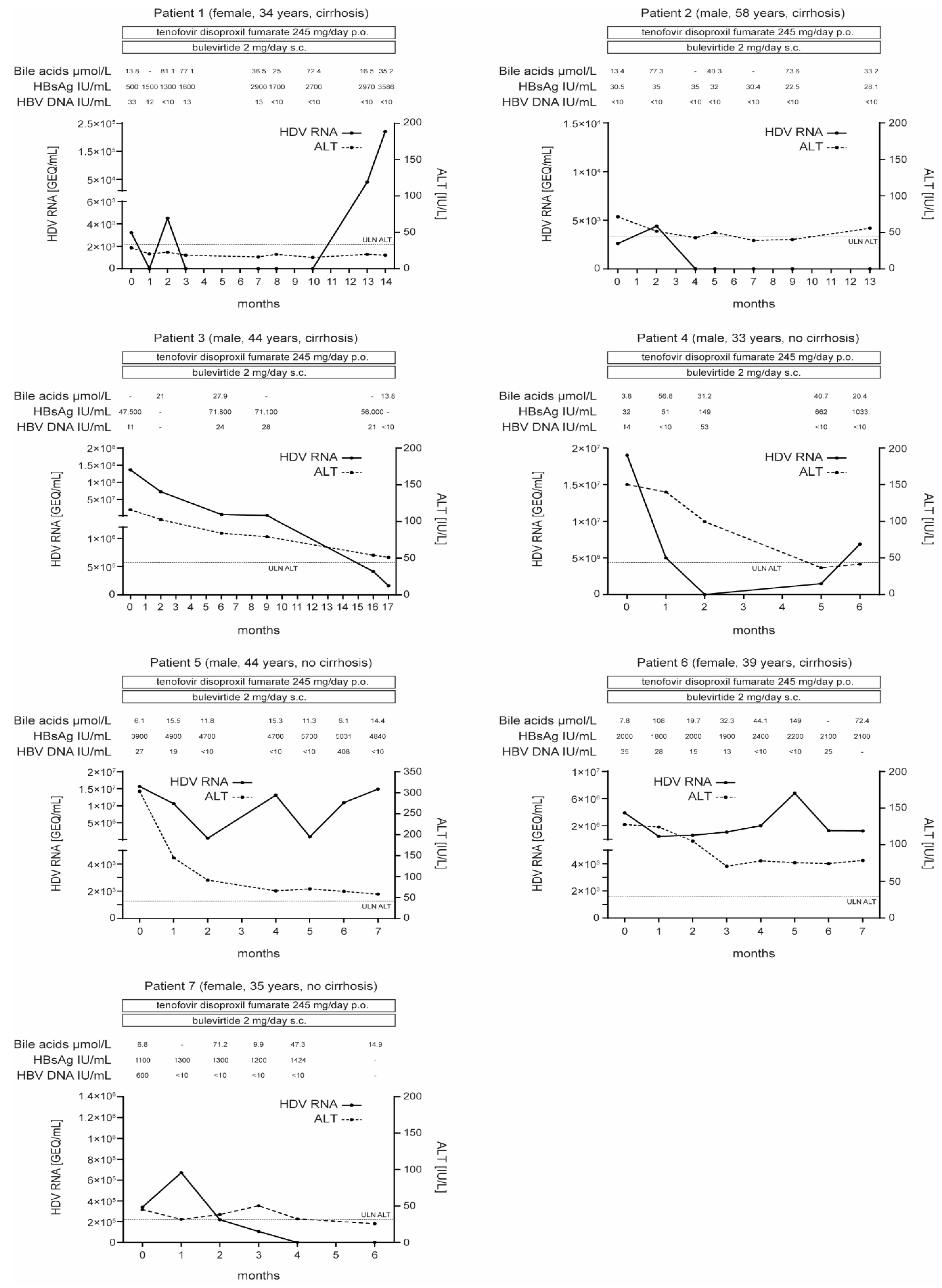
2.1. Response to Treatment after 24 Weeks
2.2. Response to Treatment after >48 Weeks
2.3. HBV Response to Treatment
2.4. Serum Bile Acid Levels during BLV Treatment
2.5. Compliance to Treatment
2.6. Adverse Events
3. Discussion
4. Patients and Methods
4.1. Patients
4.2. Ethics Statement
4.3. Molecular Diagnostic Assays
4.4. Definition of Response
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Wedemeyer, H.; Manns, M.P. Epidemiology, pathogenesis and management of hepatitis D: Update and challenges ahead. Nat. Rev. Gastroenterol. Hepatol. 2010, 7, 31–40. [Google Scholar] [CrossRef] [PubMed]
- Romeo, R.; Del Ninno, E.; Rumi, M.; Russo, A.; Sangiovanni, A.; De Franchis, R.; Ronchi, G.; Colombo, M. A 28-year study of the course of hepatitis Delta infection: A risk factor for cirrhosis and hepatocellular carcinoma. Gastroenterology 2009, 136, 1629–1638. [Google Scholar] [CrossRef] [PubMed]
- Asselah, T.; Loureiro, D.; Tout, I.; Castelnau, C.; Boyer, N.; Marcellin, P.; Mansouri, A. Future treatments for hepatitis delta virus infection. Liver Int. 2020, 40 (Suppl. 1), 54–60. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chen, H.-Y.; Shen, D.-T.; Ji, D.-Z.; Han, P.-C.; Zhang, W.-M.; Ma, J.-F.; Chen, W.-S.; Goyal, H.; Pan, S.; Xu, H.-G. Prevalence and burden of hepatitis D virus infection in the global population: A systematic review and meta-analysis. Gut 2018, 68, 512–521. [Google Scholar] [CrossRef] [PubMed]
- Stockdale, A.J.; Kreuels, B.; Henrion, M.Y.R.; Giorgi, E.; Kyomuhangi, I.; De Martel, C.; Hutin, Y.; Geretti, A.-M. The global prevalence of hepatitis D virus infection: Systematic review and meta-analysis. J. Hepatol. 2020, 73, 523–532. [Google Scholar] [CrossRef]
- Yan, H.; Zhong, G.; Xu, G.; He, W.; Jing, Z.; Gao, Z.; Huang, Y.; Qi, Y.; Peng, B.; Wang, H.; et al. Sodium taurocholate cotransporting polypeptide is a functional receptor for human hepatitis B and D virus. Elife 2012, 1, e00049. [Google Scholar] [CrossRef]
- Ni, Y.; Lempp, F.A.; Mehrle, S.; Nkongolo, S.; Kaufman, C.; Fälth, M.; Stindt, J.; Königer, C.; Nassal, M.; Kubitz, R.; et al. Hepatitis B and D viruses exploit sodium taurocholate co-transporting polypeptide for species-specific entry into hepatocytes. Gastroenterology 2014, 146, 1070–1083. [Google Scholar] [CrossRef] [PubMed]
- Hu, H.-H.; Liu, J.; Lin, Y.-L.; Luo, W.-S.; Chu, Y.-J.; Chang, C.-L.; Jen, C.-L.; Lee, M.-H.; Lu, S.-N.; Wang, L.-Y.; et al. The rs2296651 (S267F) variant on NTCP (SLC10A1) is inversely associated with chronic hepatitis B and progression to cirrhosis and hepatocellular carcinoma in patients with chronic hepatitis B. Gut 2016, 65, 1514–1521. [Google Scholar] [CrossRef]
- Wu, W.; Zeng, Y.; Lin, J.; Wu, Y.; Chen, T.; Xun, Z.; Ou, Q. Genetic variants in NTCP exon gene are associated with HBV infection status in a Chinese Han population. Hepatol. Res. 2018, 48, 364–372. [Google Scholar] [CrossRef]
- Binh, M.T.; Hoan, N.X.; Tong, H.V.; Sy, B.T.; Trung, N.T.; Bock, C.T.; Toan, N.L.; Song, L.H.; Bang, M.H.; Meyer, C.G.; et al. NTCP S267F variant associates with decreased susceptibility to HBV and HDV infection and decelerated progression of related liver diseases. Int. J. Infect. Dis. 2019, 80, 147–152. [Google Scholar] [CrossRef] [Green Version]
- Wedemeyer, H.; Bogomolov, P.; Blank, A.; Allweiss, L.; Dandri-Petersen, M.; Bremer, B.; Voronkova, N.; Schöneweis, K.; Pathil, A.; Burhenne, J.; et al. Final results of a multicenter, open-label phase 2b clinical trial to assess safety and efficacy of Myrcludex B in combination with Tenofovir in patients with chronic HBV/HDV co-infection. In Proceedings of the EASL International Liver Congress, Paris, France, 11–15 April 2018. [Google Scholar]
- Ciancio, A.; Rizzetto, M. PEG-IFN for the treatment of hepatitis D. Nat. Rev. Gastroenterol. Hepatol. 2011, 8, 304–306. [Google Scholar] [CrossRef] [PubMed]
- Abbas, Z.; Memon, M.S.; Mithani, H.; Jafri, W.; Hamid, S. Treatment of chronic hepatitis D patients with pegylated interferon: A real-world experience. Antivir. Ther. 2014, 19, 463–468. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wedemeyer, H.; Yurdaydὶn, C.; Dalekos, G.N.; Erhardt, A.; Çakaloglu, Y.; Degertekin, H.; Gürel, S.; Zeuzem, S.; Zachou, K.; Bozkaya, H.; et al. Peginterferon plus Adefovir versus Either Drug Alone for Hepatitis Delta. N. Engl. J. Med. 2011, 364, 322–331. [Google Scholar] [CrossRef] [Green Version]
- Urban, S.; Neumann-Haefelin, C.; Lampertico, P. Hepatitis D virus in 2021: Virology, immunology and new treatment approaches for a difficult-to-treat disease. Gut 2021, 70, 1782–1794. [Google Scholar] [CrossRef] [PubMed]
- Kang, C.; Syed, Y.Y. Bulevirtide: First Approval. Drugs 2020, 80, 1601–1605. [Google Scholar] [CrossRef]
- Wedemeyer, H.; Schöneweis, K.; Bogomolov, P.; Voronkova, N.; Chulanov, V.; Stepanova, T.; Bremer, B.; Allweiss, L.; Dandri, M.; Burhenne, J.; et al. Final results of a multicenter, open-label phase 2 clinical trial (MYR203) to assess safety and efficacy of myrcludex B in cwith PEG-interferon Alpha 2a in patients with chronic HBV/HDV co-infection. In Proceedings of the EASL International Liver Congress, Vienna, Austria, 10–14 April 2019. [Google Scholar]
- Wedemeyer, H.; Aleman, S.; Andreone, P.; Blank, A.; Brunetto, M.; Bogomolov, P.; Chulanov, V.; Geyvandova, N.; Hilgard, G.; Mamonova, N.; et al. Bulevirtide monotherapy at low and high dose in patients with chronic hepatitis delta: 24 weeks interim data of the phase 3 MYR301 study. In Proceedings of the EASL International Liver Congress, Digital, 23–26 June 2021. [Google Scholar]
- Wedemeyer, H.; Schöneweis, K.; Bogomolov, P.; Chulanov, V.; Stepanova, T.; Viacheslav, M.; Allweiss, L.; Dandri, M.; Ciesek, S.; Dittmer, U.; et al. 48 weeks of high dose (10 mg) bulevirtide as monotherapy or with peginterferon alfa-2a in patients with chronic HBV/HDV co-infection. J. Hepatol. 2020, 73, S52–S53. [Google Scholar] [CrossRef]
- Loglio, A.; Ferenci, P.; Renteria, S.C.U.; Tham, C.Y.L.; Scholtes, C.; Holzmann, H.; Van Bömmel, F.; Borghi, M.; Perbellini, R.; Rimondi, A.; et al. Safety and effectiveness of up to 3 years’ bulevirtide monotherapy in patients with HDV-related cirrhosis. J. Hepatol. 2022, 76, 464–469. [Google Scholar] [CrossRef] [PubMed]
- Asselah, T.; Loureiro, D.; Le Gal, F.; Narguet, S.; Brichler, S.; Bouton, V.; Abazid, M.; Boyer, N.; Giuly, N.; Gerber, A.; et al. Early virological response in six patients with hepatitis D virus infection and compensated cirrhosis treated with Bulevirtide in real-life. Liver. Int. 2021, 41, 1509–1517. [Google Scholar] [CrossRef]
- De Ledinghen, V.; Guyader, D.; Metivier, S.; Hilleret, M.-N.; Fontaine, H.; Roche, B.; Ganne-Carrie, N.; D’Alteroche, L.; Loustaud-Ratti, V.; Gervais, A.; et al. Safety and efficacy of 2 mg bulevirtide in patients with chronic HBD/HDV co-infection: First real-world results. In Proceedings of the AASLD The Liver Meeting, Digital, 13–16 November 2020; Available online: https://www.natap.org/2021/AASLD/AASLD_69.htm (accessed on 11 January 2022).
- Loglio, A.; Renteria, S.C.U.; Sambarino, D.; Borghi, M.; Perbellini, R.; Scholtès, C.; Facchetti, F.; Fraquelli, M.; Costantino, A.; Orsini, C.; et al. Early clinical and virological changes in HDV patients with advanced cirrhosis treated with bulevirtide monotherapy in a real-life setting. In Proceedings of the AASLD The Liver Meeting, Digital, 23–26 June 2021; Available online: https://www.aasld.org/sites/default/files/2021-11/TLM%202021%20Late%20Breaking%20Abstracts%2011.01.21.pdf (accessed on 11 January 2022).
- Binter, T.; Jachs, M.; Hartl, L.; Aberle, S.; Zoller, H.; Aigner, E.; Stättermayer, A.F.; Kozbial, K.; Steindl-Munda, P.E.; Bauer, D.; et al. Efficacy of long-term treatment of chronic hepatitis D patients with bulevirtide—Results of a “real world” study. In Proceedings of the AALSD The Liver Meeting, Digital, 13–16 November 2020; Available online: https://www.natap.org/2021/AASLD/AASLD_95.htm (accessed on 11 January 2022).
- Zöllner, C.; Lutz, K.; Demir, M.; Tacke, F. First real-life experiences with bulevirtide for the treatment of hepatitis delta—Data from a tertiary reference center in Germany. In Proceedings of the EASL International Liver Congress, Digital, 23–26 June 2021; Available online: https://www.postersessiononline.eu/173580348_eu/congresos/ILC2021/aula/-PO_1419_ILC2021.pdf (accessed on 11 January 2022).
- Roulot, D.; Brichler, S.; Layese, R.; BenAbdesselam, Z.; Zoulim, F.; Thibault, V.; Scholtes, C.; Roche, B.; Castelnau, C.; Poynard, T.; et al. Origin, HDV genotype and persistent viremia determine outcome and treatment response in patients with chronic hepatitis delta. J. Hepatol. 2020, 73, 1046–1062. [Google Scholar] [CrossRef]
- Casillas, R.; Tabernero, D.; Gregori, J.; Belmonte, I.; Cortese, M.F.; González, C.; Riveiro-Barciela, M.; López, R.M.; Quer, J.; Esteban, R.; et al. Analysis of hepatitis B virus preS1 variability and prevalence of the rs2296651 polymorphism in a Spanish population. World J. Gastroenterol. 2018, 24, 680–692. [Google Scholar] [CrossRef] [PubMed]
- Pan, W.; Song, I.-S.; Shin, H.-J.; Kim, M.-H.; Choi, Y.-L.; Lim, S.-J.; Kim, W.-Y.; Lee, S.-S.; Shin, J.-G. Genetic polymorphisms in Na+-taurocholate co-transporting polypeptide (NTCP) and ileal apical sodium-dependent bile acid transporter (ASBT) and ethnic comparisons of functional variants of NTCP among Asian populations. Xenobiotica 2011, 41, 501–510. [Google Scholar] [CrossRef]
- Lempp, F.A.; Schlund, F.; Rieble, L.; Nussbaum, L.; Link, C.; Zhang, Z.; Ni, Y.; Urban, S. Recapitulation of HDV infection in a fully permissive hepatoma cell line allows efficient drug evaluation. Nat. Commun. 2019, 10, 2265. [Google Scholar] [CrossRef]
- Nkongolo, S.; Hollnberger, J.; Urban, S. Bulevirtide als erster spezifischer Wirkstoff gegen Hepatitis-D-Virusinfektionen—Mechanismus und klinische Wirkung. Bundesgesundheitsblatt-Gesundh.-Gesundh. 2022, 65, 254–263. [Google Scholar] [CrossRef]
- Rizzetto, M.; Smedile, A. Pegylated interferon therapy of chronic hepatitis D: In need of revision. Hepatology 2015, 61, 1109–1111. [Google Scholar] [CrossRef]
- Belyhun, Y.; Liebert, U.G.; Maier, M. Clade homogeneity and low rate of delta virus despite hyperendemicity of hepatitis B virus in Ethiopia. Virol. J. 2017, 14, 176. [Google Scholar] [CrossRef] [PubMed] [Green Version]


{kind=link}
| Patient 1 | Patient 2 | Patient 3 | Patient 4 | Patient 5 | Patient 6 | Patient 7 | |
|---|---|---|---|---|---|---|---|
| Gender, age (years) | Female, 34 | Male, 59 | Male, 44 | Male, 33 | Male, 44 | Female, 39 | Female, 35 |
| Country of origin | Armenia | Russia | Russia | Romania | Albania | Uzbekistan | Moldova |
| Previous antiviral treatment | TDF, PEG-IFNα | TDF, PEG-IFNα | TDF, PEG-IFNα | None | TDF | None | None |
| HBV genotype | n.d. | HBV-D1 | HBV-D2 | n.d. | n.d. | n.d. | HBV-D1 |
| HBV DNA (IU/mL) | 33 | <10 | 11 | 14 | 27 | 35 | 600 |
| HBeAg | Negative | Negative | Negative | Negative | Negative | Negative | Negative |
| Anti-HBe | Positive | Positive | Positive | Positive | Negative | Positive | Positive |
| HDV genotype | HDV-1 | HDV-1 | HDV-1 | HDV-1 | HDV-1 | HDV-1 | HDV-1 |
| HDV RNA (Geq/mL) | 3220 | 2600 | 136,000,000 | 19,000,000 | 15,700,000 | 3,900,000 | 340,000 |
| Cirrhosis (Child–Pugh score) | Yes (A) | Yes (A) | Yes (A) | No | No | Yes (A) | No |
| Liver stiffness (kPa) | 21.1 | 21.5 | 13.9 | 8.4 | 14.2 | 19.9 | n.a. |
| Hepatocellular carcinoma | No | Yes | No | No | No | No | No |
| ALT (IU/L) ULN ♀ < 35, ♂ < 45 | 28.8 | 71.4 | 115.8 | 150 | 303.6 | 127.8 | 45 |
| AST (IU/L) ULN ♀ < 31, ♂ < 35 | 61.8 | 37.8 | 68.4 | 73.8 | 133.2 | 101.4 | 39 |
| GGT (IU/L) ULN ♀ < 38, ♂ < 55 | 70.8 | 174 | 204 | 34.2 | 36 | 30.6 | 28.2 |
| Total bilirubin (mg/dL) ULN ♀/♂ < 1 | 1 | 0.38 | 0.96 | 0.45 | 0.28 | 0.71 | 0.15 |
| Albumin (g/L) LLN ♀/♂ < 35 | 42.2 | 45.1 | 46.9 | 48.1 | 46.6 | 48.9 | 40 |
| Platelets (1000/µL) LLN ♀/♂ < 150 | 41 | 120 | 160 | 204 | 145 | 158 | 376 |
| SLC10A1 Polymorphism | Genotype |
|---|---|
| rs61745930 T > A | TT (wildtype) in all patients |
| rs2296651 C > G | CC (wildtype) in all patients |
| rs71547507 T > A | TT (wildtype) in all patients |
| rs72547506 A > T | AA (wildtype) in all patients |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Herta, T.; Hahn, M.; Maier, M.; Fischer, J.; Niemeyer, J.; Hönemann, M.; Böhlig, A.; Gerhardt, F.; Schindler, A.; Schumacher, J.; et al. Efficacy and Safety of Bulevirtide plus Tenofovir Disoproxil Fumarate in Real-World Patients with Chronic Hepatitis B and D Co-Infection. Pathogens 2022, 11, 517. https://doi.org/10.3390/pathogens11050517
Herta T, Hahn M, Maier M, Fischer J, Niemeyer J, Hönemann M, Böhlig A, Gerhardt F, Schindler A, Schumacher J, et al. Efficacy and Safety of Bulevirtide plus Tenofovir Disoproxil Fumarate in Real-World Patients with Chronic Hepatitis B and D Co-Infection. Pathogens. 2022; 11(5):517. https://doi.org/10.3390/pathogens11050517
Chicago/Turabian StyleHerta, Toni, Magdalena Hahn, Melanie Maier, Janett Fischer, Johannes Niemeyer, Mario Hönemann, Albrecht Böhlig, Florian Gerhardt, Aaron Schindler, Jonas Schumacher, and et al. 2022. "Efficacy and Safety of Bulevirtide plus Tenofovir Disoproxil Fumarate in Real-World Patients with Chronic Hepatitis B and D Co-Infection" Pathogens 11, no. 5: 517. https://doi.org/10.3390/pathogens11050517