
N-3 Polyunsaturated Fatty Acids and Their Lipid Mediators as A Potential Immune–Nutritional Intervention: A Molecular and Clinical View in Hepatic Disease and Other Non-Communicable Illnesses

 ,
,
Abstract
:
1. Introduction
2. Methods
3. Nutritional States in Liver Diseases
4. Immunonutrition
5. N-3 PUFAs and Inflammation
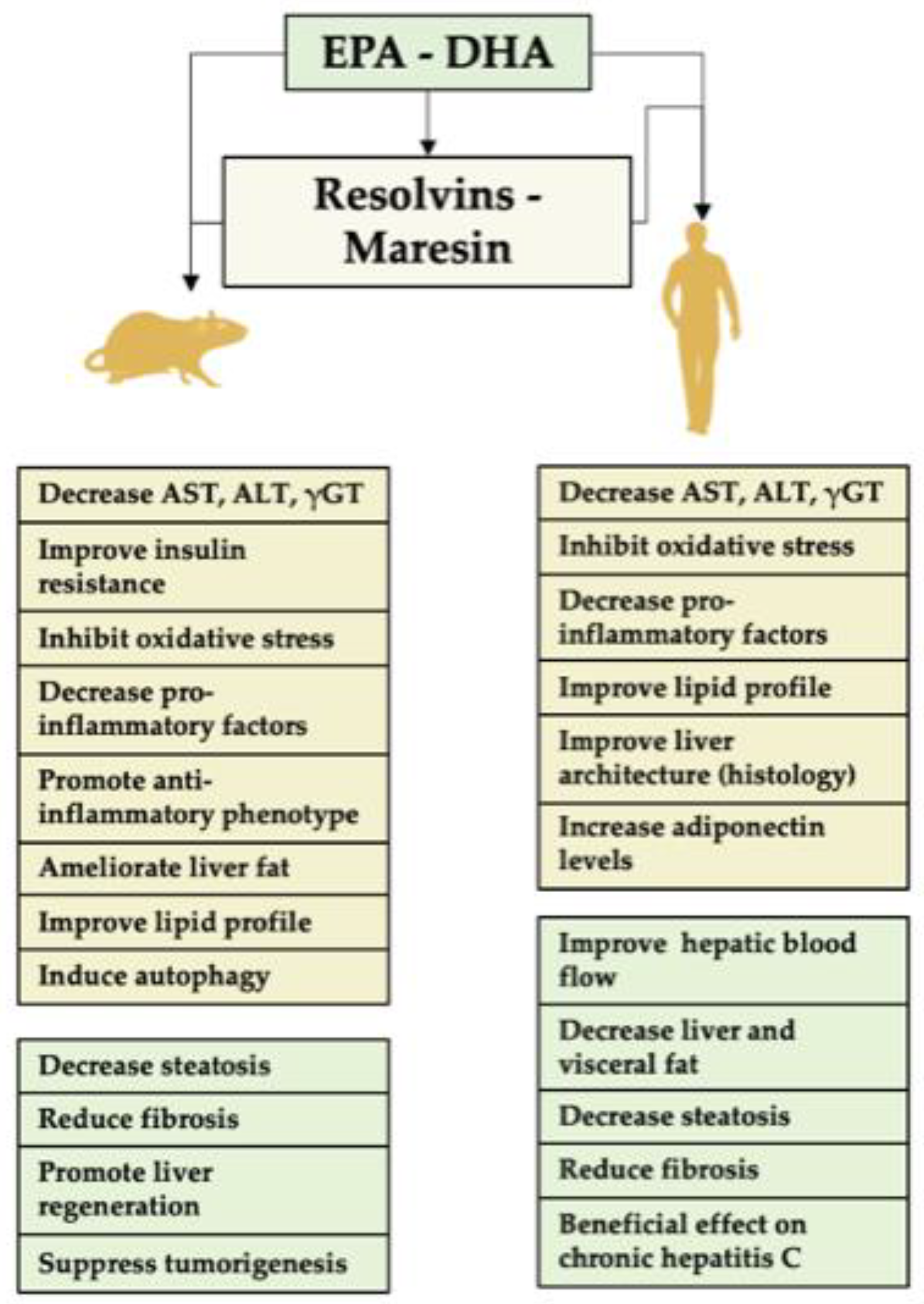
5.1. Resolvins
5.2. Protectins
5.3. Maresins
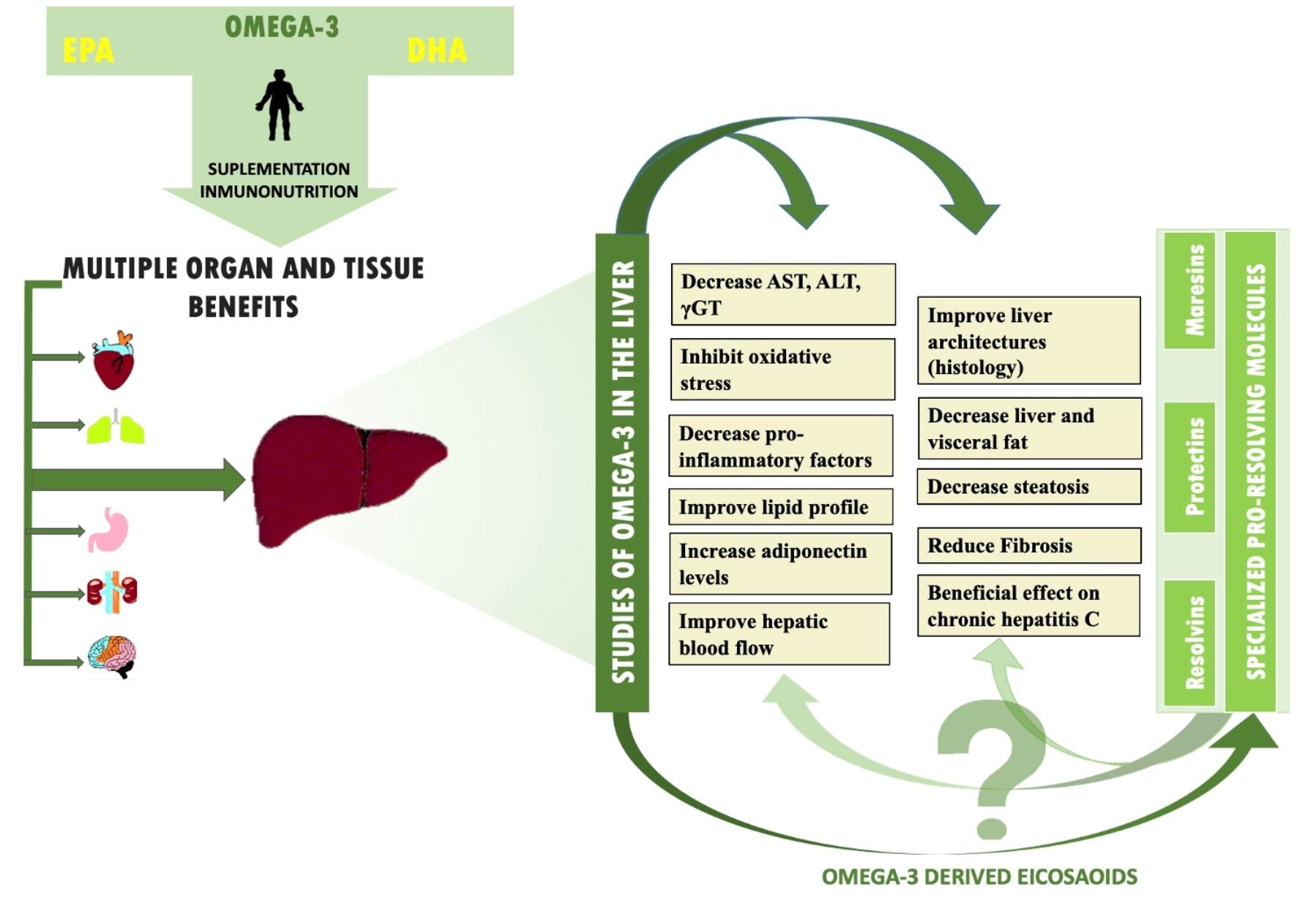
6. Beneficial Effects of N-3 PUFAs
6.1. Cardiovascular Health
6.2. Nervous System
6.3. Cancer
6.4. Inflammatory Bowel Disease, Rheumatoid Arthritis and Other Autoimmune Diseases
6.5. Ischemia–Reperfusion-Induced Damage (IR)
7. Beneficial Effects of N-3 PUFA in Liver Diseases
7.1. Evidence for n-3 PUFA Effects in Animal Models of Liver Disease
7.2. Clinical Trials with n-3 PUFAs in NAFLD and Its Progressive Disease States
7.2.1. NAFLD
7.2.2. NASH
7.2.3. Hepatitis C
7.2.4. Liver Cirrhosis
8. Supplementation with Specific Pro-Resolving Mediators (SPMs) in Liver Diseases
8.1. SMP Effects in Experimental Animals
8.2. SPM Effects in the Clinical Setting
9. Conclusions
Supplementary Materials
Authors Contribution
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Tabas, I.; Glass, C.K. Anti-Inflammatory Therapy in Chronic Disease: Challenges and Opportunities. Science 2013, 339, 166–172. [Google Scholar] [CrossRef] [Green Version]
- Serhan, C.N. Systems Approach to Inflammation Resolution: Identification of Novel Anti-Inflammatory and pro-Resolving Mediators. J. Thromb. Haemost. 2009, 7, 44–48. [Google Scholar] [CrossRef]
- Zapatera, B.; Prados, A.; Gómez-Martínez, S.; Marcos, A. Immunonutrition: Methodology and Applications. Nutr. Hosp. 2015, 31, 145–154. [Google Scholar] [CrossRef] [PubMed]
- Diaz, L.; Gómez-Martínez, S.; Nova, E.; Romeo, J.; Marcos, A. Inmunonutrición: Una Potente Herramienta Para Evaluar Situaciones Nutricionales y Beneficios de Nutrientes, Compuestos Bioactivos y Alimentos. In Manual Práctico de Nutrición y Salud Kellogg’s; Exlibris: Madrid, Spain; Digital.CSIC: Madrid, Spain, 2012; Volume 546, pp. 1–12. Available online: http://digital.csic.es/handle/10261/54350 (accessed on 12 January 2021).
- Canicoba, M.; Domínguez, N.; Gutiérrez, S. Nutrición En Las Enfermedades Hepáticas Crónicas. Nutr. Clín. Med. 2014, 8, 121–135. [Google Scholar] [CrossRef]
- Del Campo, J.A.; Gallego, P.; Grande, L. Role of Inflammatory Response in Liver Diseases: Therapeutic Strategies. World J. Hepatol. 2018, 10, 1–7. [Google Scholar] [CrossRef] [PubMed]
- Mizock, B.A. Immunonutrition and Critical Illness: An Update. Nutrition 2010, 26, 701–707. [Google Scholar] [CrossRef] [PubMed]
- Aida, T.; Furukawa, K.; Suzuki, D.; Shimizu, H.; Yoshidome, H.; Ohtsuka, M.; Kato, A.; Yoshitomi, H.; Miyazaki, M. Preoperative Immunonutrition Decreases Postoperative Complications by Modulating Prostaglandin E2 Production and T-Cell Differentiation in Patients Undergoing Pancreatoduodenectomy. Surgery 2014, 155, 124–133. [Google Scholar] [CrossRef]
- Yagnik, G.; Takahashi, Y.; Tsoulfas, G.; Reid, K.; Murase, N.; Geller, D. Blockade of the L-Arginine/NO Synthase Pathway Worsens Hepatic Apoptosis and Liver Transplant Preservation Injury. Hepatology 2002, 36, 573–581. [Google Scholar] [CrossRef]
- Mikagi, K.; Kawahara, R.; Kinoshita, H.; Aoyagi, S. Effect of Preoperative Immunonutrition in Patients Undergoing Hepatectomy; a Randomized Controlled Trial. Kurume Med. J. 2011, 58, 1–8. [Google Scholar] [CrossRef] [Green Version]
- Eghtesad, S.; Poustchi, H.; Malekzadeh, R. Malnutrition in Liver Cirrhosis:The Influence of Protein and Sodium. Middle East J. Dig. Dis. 2013, 5, 65–75. [Google Scholar] [CrossRef]
- Asrani, S.K.; Devarbhavi, H.; Eaton, J.; Kamath, P.S. Burden of Liver Diseases in the World. J. Hepatol. 2019, 70, 151–171. [Google Scholar] [CrossRef] [PubMed]
- Hoyer, D.P.; Munteanu, M.; Canbay, A.; Hartmann, M.; Gallinat, A.; Paul, A.; Saner, F.H. Liver Transplantation for Acute Liver Failure: Are There Thresholds Not to Be Crossed? Transpl. Int. 2014, 27, 625–633. [Google Scholar] [CrossRef] [PubMed]
- Germani, G.; Theocharidou, E.; Adam, R.; Karam, V.; Wendon, J.; O’Grady, J.; Burra, P.; Senzolo, M.; Mirza, D.; Castaing, D.; et al. Liver Transplantation for Acute Liver Failure in Europe: Outcomes over 20 Years from the ELTR Database. J. Hepatol. 2012, 57, 288–296. [Google Scholar] [CrossRef] [PubMed]
- Bernal, W.; Cross, T.J.S.; Auzinger, G.; Sizer, E.; Heneghan, M.A.; Bowles, M.; Muiesan, P.; Rela, M.; Heaton, N.; Wendon, J.; et al. Outcome after Wait-Listing for Emergency Liver Transplantation in Acute Liver Failure: A Single Centre Experience. J. Hepatol. 2009, 50, 306–313. [Google Scholar] [CrossRef]
- Merli, M.; Berzigotti, A.; Zelber-Sagi, S.; Dasarathy, S.; Montagnese, S.; Genton, L.; Plauth, M.; Parés, A. Association for the Study of the Liver: EASL Clinical Practice Guidelines on Nutrition in Chronic Liver Disease. J. Hepatol. 2019, 70, 172–193. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Nishikawa, H.; Nishiguchi, S. Sarcopenia and Sarcopenic Obesity Are Prognostic Factors for Overall Survival in Patients with Cirrhosis. Int. Med. 2016, 55, 863–870. [Google Scholar] [CrossRef] [Green Version]
- Rosato, V.; Abenavoli, L.; Federico, A.; Masarone, M.; Persico, M. Pharmacotherapy of Alcoholic Liver Disease in Clinical Practice. Int. J. Clin. Pract. 2016, 70, 119–131. [Google Scholar] [CrossRef]
- Osna, N.A.; Donohue, T.M.; Kharbanda, K.K. Alcoholic Liver Disease: Pathogenesis and Current Management. Alcohol Res. 2017, 38, 147–161. [Google Scholar]
- Frazier, T.H.; Mcclain, C.J.; Kershner, N.A.; Marsano, L.S. Treatment of Alcoholic Liver Disease. Ther. Adv. Gastroenterol. 2011, 4, 63–81. [Google Scholar] [CrossRef] [Green Version]
- González-Calatayud, M.; López Romero, S.; Athié Gutiérrez, C.; Valdovinos González, C.; Urbina León, D. Influence of Immunonutrition on the General and Nutritional State, and on the in-Hospital Stay, of Patients Operated Secondary to Abdominal Sepsis. Cir. Gen. 2011, 33, 236–242. [Google Scholar]
- Pollock, G.R.Y.; Van Way, C.W. Immune-Enhancing Nutrition in Surgical Critical Care. MO Med. 2012, 109, 388–392. [Google Scholar] [PubMed]
- Harkness, L. The history of enteral nutrition therapy: From Raw Eggs and Nasal Tubes to Purified Amino Acids and Early Postoperative Jejunal Delivery. J. Am. Diet. Assoc. 2002, 102, 399–404. [Google Scholar] [CrossRef]
- Uscátegui, H. Inmunonutrición: Enfoque en el paciente quirúrgico. Rev. Chil. Cir. 2010, 62, 87–92. [Google Scholar] [CrossRef] [Green Version]
- Szefel, J.; Kruszewski, W.J.; Buczek, T. Enteral Feeding and Its Impact on the Gut Immune System and Intestinal Mucosal Barrier. Prz. Gastroenterol. 2015, 10, 71–77. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cahova, M.; Bratova, M.; Wohl, P. Parenteral Nutrition-Associated Liver Disease: The Role of the Gut Microbiota. Nutrients 2017, 9, 987. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gabe, S.M.; Culkin, A. Abnormal Liver Function Tests in the Parenteral Nutrition Fed Patient. Frontline Gastroenterol. 2010, 1, 98–104. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Duarte, M.J.; Díaz, M.S.; Vargas, G.R.B.; Rubio, G.J.; Fernández, P.L.; Lee Eng, C.V.E. Inmunonutrición: Logros y Promesas. Med. Crit. 2005, 19, 183–193. [Google Scholar]
- Planas, M.; Schwartz, S.; Arbos, M.A.; Farriol, M. Plasma Glutamine Levels in Septic Patients. J. Parenter. Enteral Nutr. 1993, 17, 299–300. [Google Scholar] [CrossRef]
- Ockenga, J.; Borchert, K.; Rifai, K.; Manns, M.P.; Bischoff, S.C. Effect of Glutamine-Enriched Total Parenteral Nutrition in Patients with Acute Pancreatitis. Clin. Nutr. 2002, 21, 409–416. [Google Scholar] [CrossRef]
- Ito, A.; Higashiguchi, T. Effects of Glutamine Administration on Liver Regeneration Following Hepatectomy. Nutrition 1999, 15, 23–28. [Google Scholar] [CrossRef]
- Morris, S.M. Arginine: Beyond Protein. Am. J. Clin. Nutr. 2006, 83, 508s–512s. [Google Scholar] [CrossRef] [Green Version]
- Peranzoni, E.; Marigo, I.; Dolcetti, L.; Ugel, S.; Sonda, N.; Taschin, E.; Mantelli, B.; Bronte, V.; Zanovello, P. Role of Arginine Metabolism in Immunity and Immunopathology. Immunobiology 2008, 212, 795–812. [Google Scholar] [CrossRef] [PubMed]
- Kurokawa, T.; An, J.; Tsunekawa, K.; Shimomura, Y.; Kazama, S.; Ishikawa, N.; Nonami, T.; Sugiyama, S. Effect of L-Arginine Supplement on Liver Regeneration after Partial Hepatectomy in Rats. World J. Surg. Oncol. 2012, 10, 99. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Al-Dalaen, S.; Alzyoud, J.; Al-Qtaitat, A. The Effects of L-Arginine in Modulating Liver Antioxidant Biomarkers Within Carbon Tetrachloride Induced Hepatotoxicity: Experimental Study in Rats. Biomedical and Pharmacology Journal. Biomed. Pharmacol. 2016, 9, 293–298. [Google Scholar] [CrossRef]
- Toro-Martin, J.; Arsenault, B.; Després, J.P.; Vohl, M.-C. Precision nutrition: A review of personalized nutritional approaches for the prevention and management of metabolic syndrome. Nutrients 2017, 22, 913. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Fontana, L.; Moreira, E.; Torres, M.I.; Fernández, I.; Ríos, A.; De Medina, F.S.; Gil, A. Dietary Nucleotides Correct Plasma and Liver Microsomal Fatty Acid Alterations in Rats with Liver Cirrhosis Induced by Oral Intake of Thioacetamide. J. Hepatol. 1998, 28, 662–669. [Google Scholar] [CrossRef]
- Pérez, M.; Sánchez-Medina, F.; Torres, M.; Gil, A.; Suárez, A. Dietary Nucleotides Enhance the Liver Redox State and Protein Synthesis in Cirrhotic Rats. J. Nutr. 2004, 134, 2504–2508. [Google Scholar] [CrossRef] [Green Version]
- Torres-López, M.I.; Fernandez, I.; Fontana, L.; Gil, A.; Rios, A. Influence of Dietary Nucleotides on Liver Structural Recovery and Hepatocyte Binuclearity in Cirrhosis Induced by Thioacetamide. Gut 1996, 38, 260–264. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Dennis, E.A.; Norris, P.C. Eicosanoid Storm in Infection and Inflammation. Nat. Rev. Immunol. 2015, 15, 511–523. [Google Scholar] [CrossRef] [Green Version]
- Kar, S.; Webel, R. Fish Oil Supplementation & Coronary Artery Disease: Does It Help? MO Med. 2012, 109, 142–145. [Google Scholar]
- Nova, E.; Montero, A.; Gómez, S.; Marcos, A. Capítulo I La Estrecha Relación Entre La Nutrición y El Sistema Inmunitario. In Soporte Nutricional en el Paciente Oncológico; Gomez, C., Sastre, A., Eds.; You & Us S.A. Publisher: Madrid, Spain, 2004; pp. 9–21. [Google Scholar]
- Gerbi, A.; Maixent, J.M.; Ansaldi, J.L.; Pierlovisi, M.; Coste, T.; Pelissier, J.F.; Vague, P.; Raccah, D. Fish Oil Supplementation Prevents Diabetes-Induced Nerve Conduction Velocity and Neuroanatomical Changes in Rats. J. Nutr. 1999, 129, 207–213. [Google Scholar] [CrossRef] [Green Version]
- Rudkowska, I. Fish Oils for Cardiovascular Disease: Impact on Diabetes. Maturitas 2010, 67, 25–28. [Google Scholar] [CrossRef] [PubMed]
- Hurst, S.; Zainal, Z.; Caterson, B.; Hughes, C.E.; Harwood, J.L. Dietary Fatty Acids and Arthritis. Prostaglandins Leukot. Essent. Fat. Acids 2010, 82, 315–318. [Google Scholar] [CrossRef] [PubMed]
- Calder, P.C. Immunomodulation by Omega-3 Fatty Acids. Prostaglandins Leukot. Essent. Fat. Acids 2007, 77, 327–335. [Google Scholar] [CrossRef] [PubMed]
- Cockbain, A.J.; Toogood, G.J.; Hull, M.A. Omega-3 Polyunsaturated Fatty Acids for the Treatment and Prevention of Colorectal Cancer. Gut 2012, 61, 135–149. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lorenz, K.J.; Schallert, R.; Daniel, V. Immunonutrition—The Influence of Early Postoperative Glutamine Supplementation in Enteral/Parenteral Nutrition on Immune Response, Wound Healing and Length of Hospital Stay in Multiple Trauma Patients and Patients after Extensive Surgery. GMS Interdiscip. Plast. Reconstr. Surg. DGPW 2015, 4, Doc15. [Google Scholar] [CrossRef]
- Sambra, V.; Echeverria, F.; Valenzuela, A.; Chouinard-Watkins, R.; Valenzuela, R. Docosahexaenoic and Arachidonic Acids as Neuroprotective Nutrients throughout the Life Cycle. Nutrients 2021, 13, 986. [Google Scholar] [CrossRef]
- Kaur, N.; Chugh, V.; Gupta, A.K. Essential Fatty Acids as Functional Components of Foods—A Review. J. Food Sci. Technol. 2014, 51, 2289–2303. [Google Scholar] [CrossRef] [Green Version]
- Valenzuela, R.; Tapia, G.; González, M.; Valenzuela, A. Omega-3 Fatty Acids (EPA and DHA) and Its Application in Diverse Clinical Situations. Rev. Chil. Nutr. 2011, 38, 356–367. [Google Scholar] [CrossRef] [Green Version]
- Xi, S.; Cohen, D.; Barve, S.; Chen, L.H. Fish Oil Suppressed Cytokines and Nuclear Factor-κB Induced by Murine AIDS Virus Infection. Nutr. Res. 2001, 21, 865–878. [Google Scholar] [CrossRef]
- Duvall, M.G.; Levy, B.D. DHA- and EPA-Derived Resolvins, Protectins, and Maresins in Airway Inflammation. Eur. J. Pharmacol. 2016, 785, 144–155. [Google Scholar] [CrossRef] [Green Version]
- Valenzuela, R.; Ortiz, M.; Hernández-Rodas, M.C.; Echeverría, F.; Videla, L.A. Targeting n-3 Polyunsaturated Fatty Acids in Non-Alcoholic Fatty Liver Disease. Curr. Med. Chem. 2020, 27, 5250–5272. [Google Scholar] [CrossRef]
- Norling, L.V.; Ly, L.; Dalli, J. Resolving Inflammation by Using Nutrition Therapy: Roles for Specialized Proresolving Mediators. Curr. Opin. Clin. Nutr. Metab. Care 2017, 20, 145–152. [Google Scholar] [CrossRef] [Green Version]
- Merched, A.J.; Ko, K.; Gotlinger, K.H.; Serhan, C.N.; Chan, L. Atherosclerosis: Evidence for Impairment of Resolution of Vascular Inflammation Governed by Specific Lipid Mediators. FASEB J. 2008, 22, 3595–3606. [Google Scholar] [CrossRef]
- Carracedo, M.; Artiach, G.; Arnardottir, H.; Bäck, M. The Resolution of Inflammation through Omega-3 Fatty Acids in Atherosclerosis, Intimal Hyperplasia, and Vascular Calcification. Semin. Immunopathol. 2019, 41, 757–766. [Google Scholar] [CrossRef] [Green Version]
- Perretti, M.; Norling, L.V. Actions of SPM in Regulating Host Responses in Arthritis. Mol. Asp. Med. 2017, 58, 57–64. [Google Scholar] [CrossRef] [PubMed]
- Recchiuti, A.; Mattoscio, D.; Isopi, E. Roles, Actions, and Therapeutic Potential of Specialized Pro-Resolving Lipid Mediators for the Treatment of Inflammation in Cystic Fibrosis. Front. Pharmacol. 2019, 10, 252. [Google Scholar] [CrossRef] [PubMed]
- Miyata, J.; Arita, M. Role of Omega-3 Fatty Acids and Their Metabolites in Asthma and Allergic Diseases. Allergol. Int. 2015, 64, 27–34. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bassaganya-Riera, J.; Hontecillas, R. Dietary Conjugated Linoleic Acid and N-3 Polyunsaturated Fatty Acids in Inflammatory Bowel Disease. Curr. Opin. Clin. Nutr. Metab. Care 2010, 13, 569–573. [Google Scholar] [CrossRef] [Green Version]
- Szymanski, K.M.; Wheeler, D.C.; Mucci, L.A. Fish Consumption and Prostate Cancer Risk: A Review and Meta-Analysis. Am. J. Clin. Nutr. 2010, 92, 1223–1233. [Google Scholar] [CrossRef] [PubMed]
- Azuma, M.M.; Gomes-Filho, J.E.; Cardoso, C.B.M.; Pipa, C.B.; Narciso, L.G.; Bomfim, S.R.M.; Jacinto, R.D.C.; Cintra, L.T.A. Omega 3 Fatty Acids Reduce the Triglyceride Levels in Rats with Apical Periodontitis. Braz. Dent. J. 2018, 29, 173–178. [Google Scholar] [CrossRef] [PubMed]
- Rius, B.; López-Vicario, C.; González-Périz, A.; Morán-Salvador, E.; García-Alonso, V.; Clària, J.; Titos, E. Resolution of Inflammation in Obesity-Induced Liver Disease. Front. Immunol. 2012, 3, 257. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Serhan, C.N.; Arita, M.; Hong, S.; Gotlinger, K. Resolvins, Docosatrienes, and Neuroprotectins, Novel Omega-3-Derived Mediators, and Their Endogenous Aspirin-Triggered Epimers. Lipids 2004, 39, 1125–1132. [Google Scholar] [CrossRef]
- Schwab, J.M.; Chiang, N.; Arita, M.; Serhan, C.N. Resolvin E1 and Protectin D1 Activate Inflammation-Resolution Programmes. Nature 2007, 447, 869–874. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hasturk, H.; Kantarci, A.; Goguet-Surmenian, E.; Blackwood, A.; Andry, C.; Serhan, C.N.; Van Dyke, T.E. Resolvin E1 Regulates Inflammation at the Cellular and Tissue Level and Restores Tissue Homeostasis In Vivo. J. Immunol. 2007, 179, 7021–7029. [Google Scholar] [CrossRef] [Green Version]
- Uddin, M.; Levy, B.D. Resolvins: Natural Agonists for Resolution of Pulmonary Inflammation. Prog. Lipid Res. 2011, 50, 75–88. [Google Scholar] [CrossRef] [Green Version]
- Levy, B.D. Prostaglandins, Leukotrienes and Essential Fatty Acids Resolvins and Protectins: Natural Pharmacophores for Resolution Biology. Prostaglandins Leukot. Essent. Fat. Acids 2010, 82, 327–332. [Google Scholar] [CrossRef] [Green Version]
- Levy, B.D.; Kohli, P.; Gotlinger, K.; Haworth, O.; Hong, S.; Kazani, S.; Israel, E.; Haley, K.J.; Serhan, C.N. Protectin D1 Is Generated in Asthma and Dampens Airway Inflammation and Hyperresponsiveness. J. Glob. Ethics 2010, 18, 147–162. [Google Scholar] [CrossRef] [Green Version]
- Freire, M.O.; Van Dyke, T.E. Natural Resolution of Inflammation. Periodontol. 2000 2013, 63, 149–164. [Google Scholar] [CrossRef] [Green Version]
- Buckley, C.D.; Gilroy, D.W.; Serhan, C.N. Proresolving Lipid Mediators and Mechanisms in the Resolution of Acute Inflammation. Immunity 2014, 40, 315–327. [Google Scholar] [CrossRef] [Green Version]
- Laiglesia, L.M.; Lorente-Cebrián, S.; Martínez-Fernández, L.; Sáinz, N.; Prieto-Hontoria, P.L.; Burrell, M.A.; Rodríguez-Ortigosa, C.M.; Martínez, J.A.; Moreno-Aliaga, M.J. Maresin 1 Mitigates Liver Steatosis in Ob/Ob and Diet-Induced Obese Mice. Int. J. Obes. 2018, 42, 572–579. [Google Scholar] [CrossRef]
- Soto, G.; Rodríguez, M.J.; Fuentealba, R.; Treuer, A.V.; Castillo, I.; González, D.R.; Zúñiga-Hernández, J. Maresin 1, a Proresolving Lipid Mediator, Ameliorates Liver Ischemia-Reperfusion Injury and Stimulates Hepatocyte Proliferation in Sprague-Dawley Rats. Int. J. Mol. Sci. 2020, 21, 540. [Google Scholar] [CrossRef] [Green Version]
- Mendoza-Torres, E.; Bravo-Sagua, R.; Villa, M.; Flores, N.; Olivares, M.J.; Calle, X.; Riquelme, J.A.; Bambs, C.; Castro, P.; Lavandero, S. Enfermedades Cardiovasculares y Cáncer: ¿Dos Entidades Mutuamente Relacionadas? Rev. Chil. Cardiol. 2019, 38, 54–63. [Google Scholar] [CrossRef] [Green Version]
- Cazzola, R.; Russo-Volpe, S.; Miles, E.A.; Rees, D.; Banerjee, T.; Roynette, C.E.; Wells, S.J.; Goua, M.; Wahle, K.W.J.; Calder, P.C.; et al. Age- and Dose-Dependent Effects of an Eicosapentaenoic Acid-Rich Oil on Cardiovascular Risk Factors in Healthy Male Subjects. Atherosclerosis 2007, 193, 159–167. [Google Scholar] [CrossRef]
- Simão, A.N.C.; Lozovoy, M.A.B.; Bahls, L.D.; Morimoto, H.K.; Simão, T.N.C.; Matsuo, T.; Dichi, I. Blood Pressure Decrease with Ingestion of a Soya Product (Kinako) or Fish Oil in Women with the Metabolic Syndrome: Role of Adiponectin and Nitric Oxide. Br. J. Nutr. 2012, 108, 1435–1442. [Google Scholar] [CrossRef]
- Eslick, G.D.; Howe, P.R.C.; Smith, C.; Priest, R.; Bensoussan, A. Benefits of Fish Oil Supplementation in Hyperlipidemia: A Systematic Review and Meta-Analysis. Int. J. Cardiol. 2009, 136, 4–16. [Google Scholar] [CrossRef]
- Manzur, F.; Suárez, A.; Farmacéutico, Q.; Moneriz, C. Efectos y controversias de los ácidos grasos omega-3. Colomb. Cardiol. 2006, 13, 180–184. [Google Scholar]
- Zanetti, M.; Grillo, A.; Losurdo, P.; Panizon, E.; Mearelli, F.; Cattin, L.; Barazzoni, R.; Carretta, R. Omega-3 Polyunsaturated Fatty Acids: Structural and Functional Effects on the Vascular Wall. BioMed Res. Int. 2015, 2015, 791978. [Google Scholar] [CrossRef] [Green Version]
- Dyall, S.C.; Michael-Titus, A.T. Neurological Benefits of Omega-3 Fatty Acids. NeuroMol. Med. 2008, 10, 219–235. [Google Scholar] [CrossRef] [PubMed]
- Cavazos, D.A.; Price, R.S.; Apte, S.S.; Degraffenried, L.A. Docosahexaenoic Acid Selectively Induces Human Prostate Cancer Cell Sensitivity to Oxidative Stress through Modulation of NF-ΚB. Prostate 2011, 71, 1420–1428. [Google Scholar] [CrossRef] [PubMed]
- Hebert, J.R.; Hurley, T.G.; Olendzki, B.C.; Teas, J.; Ma, Y.; Hampl, J.S. Nutritional and Socioeconomic Factors in Relation to Prostate Cancer Mortality: A Cross-National Study. J. Natl. Cancer Inst. 1998, 90, 1637–1647. [Google Scholar] [CrossRef] [Green Version]
- Davidson, L.A.; Nguyen, D.V.; Hokanson, R.M.; Callaway, E.S.; Isett, R.B.; Turner, N.D.; Dougherty, E.R.; Wang, N.; Lupton, J.R.; Carroll, R.J.; et al. Chemopreventive n-3 polyunsaturated fatty acids reprogram genetic signatures during colon cancer initiation and progretion in the rat. Cancer Res. 2015, 64, 6797–6804. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Deans, C.; Wigmore, S.J. Systemic Inflammation, Cachexia and Prognosis in Patients with Cancer. Curr. Opin. Clin. Nutr. Metab. Care 2005, 8, 265–269. [Google Scholar] [CrossRef] [PubMed]
- Jourdan, M.L.; Mahéo, K.; Barascu, A.; Goupille, C.; De Latour, M.P.; Bougnoux, P.; Rio, P.G. Increased BRCA1 Protein in Mammary Tumours of Rats Fed Marine ω-3 Fatty Acids. Oncol. Rep. 2007, 17, 713–719. [Google Scholar] [CrossRef]
- Pilkington, S.M.; Massey, K.A.; Bennett, S.P.; Al-Aasswad, N.M.; Roshdy, K.; Gibbs, N.K.; Friedman, P.S.; Nicolau, A.; Rhodes, L.E. Randomized controlled trial of oral omega-3 PUFA in solar-stimulated radiation-induced supression of human cutaneous immune response. Am. J. Clin. Nutr. 2013, 97, 646–652. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zhang, B.; Wei, G.; Li, R.; Wang, Y.; Yu, J.; Wang, R.; Xiao, H.; Wu, C.; Leng, C.; Zhang, B.; et al. N-3 Fatty Acid-Based Parenteral Nutrition Improves Postoperative Recovery for Cirrhotic Patients with Liver Cancer: A Randomized Controlled Clinical Trial. Clin. Nutr. 2017, 36, 1239–1244. [Google Scholar] [CrossRef]
- Lim, K.; Han, C.; Dai, Y.; Shen, M.; Wu, T. Omega-3 Polyunsaturated Fatty Acids Inhibit Hepatocellular Carcinoma Cell Growth through Blocking β-Catenin and Cyclooxygenase-2. Mol. Cancer Ther. 2009, 8, 3046–3055. [Google Scholar] [CrossRef] [Green Version]
- Wessex Health Line; Hull, M. Clinical Trial Study ID:34700. A Randomised Placebo-Controlled Phase III Trial of the Effect of the Omega-3 Fatty Acid Eicosapentaenoic Acid (EPA) on Colorectal Cancer Recurrence and Survival After Surgery for Resectable Liver Metastases. Available online: https://clinicaltrials.gov/ct2/history/NCT03428477?V_2=View (accessed on 23 July 2021).
- Hassan, A.; Ibrahim, A.; Mbodji, K.; Coëffier, M.; Ziegler, F.; Bounoure, F.; Chardigny, J.; Skiba, M.; Savoye, G.; Déchelotte, P.; et al. An α-Linolenic Acid-Rich Formula Reduces Oxidative Stress and Inflammation by Regulating NF-ΚB in Rats with TNBS-Induced Colitis. J. Nutr. 2010, 140, 1714–1721. [Google Scholar] [CrossRef] [Green Version]
- Camuesco, D.; Gálvez, J.; Nieto, A.; Comalada, M.; Rodríguez-Cabezas, M.E.; Concha, A.; Xaus, J.; Zarzuelo, A. Dietary Olive Oil Supplemented with Fish Oil, Rich in EPA and DHA (n-3) Polyunsaturated Fatty Acids, Attenuates Colonic Inflammation in Rats with DSS-Induced Colitis. J. Nutr. 2005, 135, 687–694. [Google Scholar] [CrossRef] [Green Version]
- McInnes, I.B.; O’Dell, J.R. State-of-the-Art: Rheumatoid Arthritis. Ann. Rheum. Dis. 2010, 69, 1898–1906. [Google Scholar] [CrossRef]
- Bahadori, B.; Uitz, E.; Thonhofer, R.; Trummer, M.; Pestemer-Lach, I.; McCarty, M.; Krejs, G.J. ω-3 Fatty Acids Infusions as Adjuvant Therapy in Rheumatoid Arthritis. J. Parenter. Enter. Nutr. 2010, 34, 151–155. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Castellanos, T.L.; Rodriguez, D.M. The effect of omega 3 in human health and considerations to its intake. Rev. Chil. Nutr. 2015, 42, 90–95. [Google Scholar] [CrossRef] [Green Version]
- Márquez-Balbás, G.; Sánchez-Regaña, M.; Millet, U. Study on the Use of Omega-3 Fatty Acids as a Therapeutic Supplement in Treatment of Psoriasis. Clin. Cosmet. Investig. Dermatol. 2011, 4, 73. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Romanque, U.P.; Uribe, M.M.; Videla, L.A. Molecular Mechanisms in Liver Ischemic-Reperfusion Injury and Ischemic Preconditioning. Rev. Med. Chem. 2005, 133, 469–476. [Google Scholar] [CrossRef] [Green Version]
- Rampes, S.; Ma, D. Hepatic ischemia-reperfusion injury in liver transplant setting: Mechanisms and protective strategies. J. Biomed. Res. 2019, 33, 221–234. [Google Scholar] [CrossRef]
- Zúñiga, J.; Venegas, F.; Villarreal, M.; Núñez, D.; Chandía, M.; Valenzuela, R.; Tapia, G.; Varela, P.; Videla, L.A.; Fernández, V. Protection against in Vivo Liver Ischemia-Reperfusion Injury by n-3 Long-Chain Polyunsaturated Fatty Acids in the Rat. Free Radic. Res. 2010, 44, 854–863. [Google Scholar] [CrossRef]
- Meital, L.T.; Windsor, M.T.; Perissiou, M.; Schulze, K.; Magee, R.; Kuballa, A.; Golledge, J.; Bailey, T.G.; Askew, C.D.; Russell, F.D. Omega-3 Fatty Acids Decrease Oxidative Stress and Inflammation in Macrophages from Patients with Small Abdominal Aortic Aneurysm. Sci. Rep. 2019, 9, 12987. [Google Scholar] [CrossRef] [PubMed]
- Cipollina, C. Endogenous Generation and Signaling Actions of Omega-3 Fatty Acid Electrophilic Derivatives. Biomed. Res. Int. 2015, 2015, 501792. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ortiz, M.; Soto-Alarcón, S.A.; Orellana, P.; Espinosa, A.; Campos, C.; López-Arana, S.; Rincón, M.A.; Illesca, P.; Valenzuela, R.; Videla, L.A. Suppression of high-fat diet-induced obesity-associated liver mitochondrial dysfunction by docosahexaenoic acid and hydrpxytyrosol co-administration. Dig. Liver Dis. 2020, 52, 895–904. [Google Scholar] [CrossRef]
- Sekiya, M.; Yahagi, N.; Matsuzaka, T.; Najima, Y.; Nakakuki, M.; Nagai, R.; Ishibashi, S.; Osuga, J.I.; Yamada, N.; Shimano, H. Polyunsaturated Fatty Acids Ameliorate Hepatic Steatosis in Obese Mice by SREBP-1 Suppression. Hepatology 2003, 38, 1529–1539. [Google Scholar] [CrossRef]
- Levy, J.R.; Clore, J.N.; Stevens, W. Dietary N-3 Polyunsaturated Fatty Acids Decrease Hepatic Triglycerides in Fischer 344 Rats. Hepatology 2004, 39, 608–616. [Google Scholar] [CrossRef]
- Alwayn, I.P.J.; Gura, K.; Nosé, V.; Zausche, B.; Javid, P.; Garza, J.; Verbesey, J.; Voss, S.; Ollero, M.; Andersson, C.; et al. Omega-3 Fatty Acid Supplementation Prevents Hepatic Steatosis in a Murine Model of Nonalcoholic Fatty Liver Disease. Pediatr. Res. 2005, 57, 445–452. [Google Scholar] [CrossRef] [Green Version]
- González-Periz, A.; Horrillo, R.; Ferré, N.; Gronert, K.; Dong, B.; Morán-Salvador, E.; Titos, E.; Martínez-Clemente, M.; López-Parra, M.; Arroyo, V.; et al. Obesity-induced insulin resistance and hepatic steatosis are alleviated by omgea-3 fatty acids: A role for resolvins and protectins. FASEB J. 2009, 23, 1946–1957. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Shang, T.; Liu, L.; Zhou, J.; Zhang, M.; Hu, Q.; Fang, M.; Wu, Y.; Yao, P.; Gong, Z. Protective Effects of Various Ratios of DHA/EPA Supplementation on High-Fat Diet-Induced Liver Damage in Mice. Lipids Health Dis. 2017, 16, 65. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Li, Y.; Zhao, F.; Wu, Q.; Li, M.; Zhu, Y.; Song, S.; Zhu, J.; Ma, Y.; Li, H.; Shi, X.; et al. Fish Oil Diet May Reduce Inflammatory Levels in the Liver of Middle-Aged Rats. Sci. Rep. 2017, 7, 6241. [Google Scholar] [CrossRef] [Green Version]
- Moghadamnia, D.; Mokhtari, M.; Khatamsaz, S. Protective Effects of Fish Oil Omega-3 Supplement on Liver-Related Biochemical Factors Changes Induced by Thioacetamide in Male Rats. Biosci. Biotechnol. Res. Asia 2016, 13, 1253–1258. [Google Scholar] [CrossRef]
- Firat, O.; Makay, O.; Yeniay, L.; Gokce, G.; Yenisey, C.; Coker, A. Omega-3 Fatty Acids Inhibit Oxidative Stress in a Rat Model of Liver Regeneration. Ann. Surg. Treat. Res. 2017, 93, 1–10. [Google Scholar] [CrossRef] [Green Version]
- Yang, Y.; Shao, C.; Zhang, W.; Wang, G.; Lu, D.-C.; Han, W.; Wu, Z.-S.; Chen, C. Omega-3 Polyunsaturated Fatty Acids Prevent Progression of Liver Fibrosis and Promote Liver Regeneration after Partial Hepatectomy in Cirrhotic Rats. Eur. Rev. Med. Pharmacol. Sci. 2019, 23, 10151–10160. [Google Scholar] [CrossRef]
- Weylandt, K.H.; Krause, L.F.; Gomolka, B.; Chiu, C.Y.; Bilal, S.; Nadolny, A.; Waechter, S.F.; Fischer, A.; Rothe, M.; Kang, J.X. Suppressed Liver Tumorigenesis in Fat-1 Mice with Elevated Omega-3 Fatty Acids Is Associated with Increased Omega-3 Derived Lipid Mediators and Reduced TNF-α. Carcinogenesis 2011, 32, 897–903. [Google Scholar] [CrossRef] [Green Version]
- Jump, D.B.; Depner, C.M.; Tripathy, S.; Lytle, K.A. Potential for Dietary ω-3 Fatty Acids to Prevent Nonalcoholic Fatty Liver Disease and Reduce the Risk of Primary Liver Cancer. Adv. Nutr. 2015, 6, 694–702. [Google Scholar] [CrossRef] [Green Version]
- Casson, C.; Nguyen, V.; Nayak, P.; Channabasappa, N.; Berris, K.; Panczuk, J.; Bhiladvala, C.; Dasgupta, T.; Piper, H.G. A Comparison of Smoflipid® and Intralipid® in the Early Management of Infants with Intestinal Failure. J. Pediatr. Surg. 2020, 55, 153–157. [Google Scholar] [CrossRef] [Green Version]
- Strijbosch, R.A.M.; van den Hoonaard, T.L.; Olieman, J.F.; Escher, J.C.; Alwayn, I.P.; Meijers-Ijsselstijn, H. Fish Oil in Prolonged Parenteral Nutrition in Children—Omega-3-Fatty Acids Have a Beneficial Effect on the Liver. Ned. Tijdschr. Geneeskd. 2010, 154, A2003. [Google Scholar]
- Wendel, D.; Mortensen, M.; Harmeson, A.; Shaffer, M.L.; Hsu, E.; Horslen, S. Resolving Malnutrition with Parenteral Nutrition Before Liver Transplant in Biliary Atresia. J. Pediatr. Gastroenterol. Nutr. 2018, 66, 212–217. [Google Scholar] [CrossRef]
- Kobyliak, N.; Abenavoli, L.; Falalyeyeva, T.; Mykhalchyshyn, G.; Boccuto, L.; Kononenko, L.; Kyriienko, D.; Komisarenko, I.; Dynnyk, O. Beneficial effects of probiotic combination with omega-3 fatty acids in NAFLD: A randomized clinical study. Minerva Med. 2018, 109, 418–428. [Google Scholar] [CrossRef]
- Scorletti, E.; Bhatia, L.; Mccormick, K.G.; Clough, G.F.; Nash, K.; Hodson, L.; Moyses, H.E.; Calder, P.C.; Byrne, C.D. Effects of Purified Eicosapentaenoic and Docosahexaenoic Acids in Nonalcoholic Fatty Liver Disease: Results from the WELCOME* Study. Hepatology 2014, 60, 1211–1221. [Google Scholar] [CrossRef]
- Scorletti, E.; Bhatia, L.; McCormick, K.G.; Clough, G.F.; Nash, K.; Calder, P.C.; Byrne, C.D. WELCOME Trial Investigators. Design and rationale of the WELCOME trial: A randomised, placebo controlled study to test the efficacy of purified long chainomega-3 fatty acid treatment in non-alcoholic fatty liver disease [corrected]. Contemp. Clin. Trials 2014, 37, 301–311. [Google Scholar] [CrossRef] [PubMed]
- Green, C.J.; Pramfalk, C.; Charlton, C.A.; Gunn, P.J.; Cornfield, T.; Pavlides, M.; Karpe, F.; Hodson, L. Hepatic de novo lipogenesis is suppressed and fat oxidation is increased by omega-3 fatty acids at the expense of glucose metabolism. Open Diabetes Res. Care 2020, 8, e000871. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Oscarsson, J.; Önnerhag, K.; Risérus, U.; Sundén, M.; Johansson, L.; Jansson, P.A.; Moris, L.; Nilsson, P.M.; Eriksson, J.W.; Lind, L. Effects of free omega-3 carboxylic acids and fenofibrate on liver fat content in patients with hypertriglyceridemia and non-alcoholic fatty liver disease: A double-blind, randomized, placebo-controlled study. J. Clin. Lipidol. 2018, 12, 1390–1403.e4. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lewis, M.C.; Phillips, M.L.; Slavotinek, J.P.; Kow, L.; Thompson, C.H.; Toouli, J. Change in liver size and fat content after treatment with Optifast very low calorie diet. Obes. Surg. 2006, 16, 697–701. [Google Scholar] [CrossRef] [PubMed]
- Capanni, M.; Calella, F.; Biagini, M.R.; Genise, S.; Raimondi, L.; Bedogni, G.; Svegliati-Baroni, G.; Sofi, F.; Milani, S.; Abbate, R.; et al. Prolonged N-3 Polyunsaturated Fatty Acid Supplementation Ameliorates Hepatic Steatosis in Patients with Non-Alcoholic Fatty Liver Disease: A Pilot Study. Aliment. Pharmacol. Ther. 2006, 23, 1143–1151. [Google Scholar] [CrossRef]
- Spadaro, L.; Magliocco, O.; Spampinato, D.; Piro, S.; Oliveri, C.; Alagona, C.; Papa, G.; Rabuazzo, A.M.; Purrello, F. Effects of N-3 Polyunsaturated Fatty Acids in Subjects with Nonalcoholic Fatty Liver Disease. Dig. Liver Dis. 2008, 40, 194–199. [Google Scholar] [CrossRef] [PubMed]
- Iannelli, A.; Martini, F.; Schneck, A.S.; Ghavami, B.; Baudin, G.; Anty, R.; Gugenheim, J. Preoperative 4-week supplementation with omega-3 polyunsaturated fatty acids reduces liver volume and facilitates bariatric surgery in morbidly obese patients. Obes. Surg. 2013, 23, 1761–1765. [Google Scholar] [CrossRef] [PubMed]
- Van Name, M.A.; Savoye, M.; Chick, J.M.; Galuppo, B.T.; Feldstein, A.E.; Pierpont, B.; Johnson, C.; Shabanova, V.; Ekong, U.; Valentino, P.L.; et al. A Low ω-6 to ω-3 PUFA Ratio (n-6:n-3 PUFA) Diet to Treat Fatty Liver Disease in Obese Youth. J. Nutr. 2020, 150, 2314–2321. [Google Scholar] [CrossRef]
- Argo, C.K.; Patrie, J.T.; Lackner, C.; Henry, T.D.; De Lange, E.E.; Weltman, A.L.; Shah, N.L.; Al-Osaimi, A.M.; Pramoonjago, P.; Jayakumar, S.; et al. Effects of N-3 Fish Oil on Metabolic and Histological Parameters in NASH: A Double-Blind, Randomized, Placebo-Controlled Trial. J. Hepatol. 2015, 62, 190–197. [Google Scholar] [CrossRef] [Green Version]
- Della Pepa, G.; Vetrani, C.; Brancato, V.; Vitale, M.; Monti, S.; Annuzzi, G.; Lombardi, G.; Izzo, A.; Tommasone, M.; Cipriano, P. Effects of a multifactorial ecosustainable isocaloric diet on liver fat in patients with type 2 diabetes: Randomized clinical trial. Open Diabetes Res. Care 2020, 8, e001342. [Google Scholar] [CrossRef]
- Younossi, Z.M.; Gramlich, T.; Matteoni, C.A.; Boparai, N.; McCullough, A.J. Nonalcoholic fatty liver disease in patients with type 2 diabetes. Clin. Gastroenterol. Hepatol. 2004, 2, 262–265, Erratum in Clin. Gastroenterol. Hepatol. 2004, 2, 522. [Google Scholar] [CrossRef]
- Dasarathy, S.; Dasarathy, J.; Khiyami, A.; Yerian, L.; Hawkins, C.; Sargent, R; McCullough, A.J. Double-blind randomized placebo-controlled clinical trial of omega 3 fatty acids for the treatment of diabetic patients with nonalcoholic steatohepatitis. J. Clin. Gastroenterol. 2015, 49, 137–144. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Da Silva, H.E.; Arendt, B.M.; Noureldin, S.A.; Therapondos, G.; Guindi, M.; Allard, J.P. A cross-sectional study assessing dietary intake and physical activity in Canadian patients with nonalcoholic fatty liver disease vs healthy controls. J. Acad. Nutr. Diet. 2014, 114, 1181–1194. [Google Scholar] [CrossRef]
- Qin, Y.; Zhou, Y.; Chen, S.H.; Zhao, X.L.; Ran, L.; Zeng, X.L.; Wu, Y.; Chen, J.L.; Kang, C.; Shu, F.R.; et al. Fish Oil Supplements Lower Serum Lipids and Glucose in Correlation with a Reduction in Plasma Fibroblast Growth Factor 21 and Prostaglandin E2 in Nonalcoholic Fatty Liver Disease Associated with Hyperlipidemia: A Randomized Clinical Trial. PLoS ONE 2015, 10, e0133496. [Google Scholar] [CrossRef]
- Janczyk, W.; Socha, P.; Lebensztejn, D.; Wierzbicka, A.; Mazur, A.; Neuhoff-Murawska, J.; Matusik, P. Omega-3 Fatty Acids for Treatment of Non-Alcoholic Fatty Liver Disease: Design and Rationale of Randomized Controlled Trial. BMC Pediatr. 2013, 13, 85. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Pacifico, L.; Bonci, E.; Di Martino, M.; Versacci, P.; Andreoli, G.; Silvestri, L.M.; Chiesa, C. A Double-Blind, Placebo-Controlled Randomized Trial to Evaluate the Efficacy of Docosahexaenoic Acid Supplementation on Hepatic Fat and Associated Cardiovascular Risk Factors in Overweight Children with Nonalcoholic Fatty Liver Disease. Nutr. Metab. Cardiovasc. Dis. 2015, 25, 734–741. [Google Scholar] [CrossRef]
- Della Corte, C.; Carpino, G.; De Vito, R.; De Stefanis, C.; Alisi, A.; Cianfarani, S.; Overi, D.; Mosca, A.; Stronati, L.; Cucchiara, S.; et al. Docosahexanoic Acid plus Vitamin D Treatment Improves Features of NAFLD in Children with Serum Vitamin D Deficiency: Results from a Single Centre Trial. PLoS ONE 2016, 11, e0168216. [Google Scholar] [CrossRef] [Green Version]
- Parker, H.M.; Cohn, J.S.; O’connor, H.T.; Garg, M.L.; Caterson, I.D.; George, J.; Johnson, N.A. Effect of Fish Oil Supplementation on Hepatic and Visceral Fat in Overweight Men: A Randomized Controlled Trial. Nutrients 2019, 11, 475. [Google Scholar] [CrossRef] [Green Version]
- Nogueira, M.A.; Oliveira, C.P.; Ferreira Alves, V.A.; Stefano, J.T.; Rodrigues, L.S.; Torrinhas, R.S.; Cogliati, B.; Barbeiro, H.; Carrilho, F.J.; Waitzberg, D.L. Omega-3 Polyunsaturated Fatty Acids in Treating Non-Alcoholic Steatohepatitis: A Randomized, Double-Blind, Placebo-Controlled Trial. Clin. Nutr. 2016, 35, 578–586. [Google Scholar] [CrossRef] [PubMed]
- Sanyal, A.J.; Abdelmalek, M.F.; Suzuki, A.; Cummings, O.W.; Chojkier, M. No Significant Effects of Ethyl-Eicosapentanoic Acid on Histologic Features of Nonalcoholic Steatohepatitis in a Phase 2 TriaL. Gastroenterology 2014, 147, 377–384.e1. [Google Scholar] [CrossRef] [PubMed]
- Eriksson, J.W.; Lundkvist, P.; Jansson, P.A.; Johansson, L.; Kvarnström, M.; Moris, L.; Miliotis, T.; Forsberg, G.B.; Risérus, U.; Lind, L.; et al. Effects of dapagliflozin and n-3 carboxylic acids on non-alcoholic fatty liver disease in people with type 2 diabetes: A double-blind randomised placebo-controlled study. Diabetologia 2018, 61, 1923–1934. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Diamond, I.R.; Grant, R.C.; Pencharz, P.B.; de Silva, N.; Feldman, B.M.; Fitzgerald, P.; Sigalet, D.; Dicken, B.; Turner, J.; Marchand, V.; et al. Preventing the Progression of Intestinal Failure-Associated Liver Disease in Infants Using a Composite Lipid Emulsion: A Pilot Randomized Controlled Trial of SMOFlipid. J. Parenter. Enteral Nutr. 2017, 41, 866–877. [Google Scholar] [CrossRef]
- Klek, S.; Szczepanek, K.; Scislo, L.; Walewska, E.; Pietka, M.; Pisarska, M.; Pedziwiatr, M. Intravenous lipid emulsions and liver function in adult chronic intestinal failure patients: Results from a randomized clinical trial. Nutrition 2018, 55–56, 45–50. [Google Scholar] [CrossRef]
- Gura, K.M.; Lee, S.; Valim, C.; Zhou, J.; Kim, S.; Modi, B.P.; Arsenault, D.A.; Strijbosch, R.A.; Lopes, S.; Duggan, C.; et al. Safety and efficacy of a fish-oil-based fat emulsion in the treatment of parenteral nutrition-associated liver disease. Pediatrics 2008, 121, e678–e686. [Google Scholar] [CrossRef] [Green Version]
- Puder, M.; Valim, C.; Meisel, J.A.; Le, H.D.; de Meijer, V.E.; Robinson, E.M.; Zhou, J.; Duggan, C.; Gura, K.M. Parenteral fish oil improves outcomes in patients with parenteral nutrition-associated liver injury. Ann. Surg. 2009, 250, 395–402. [Google Scholar] [CrossRef] [Green Version]
- Gura, K.M.; Premkumar, M.H.; Calkins, K.L.; Puder, M. Fish Oil Emulsion Reduces Liver Injury and Liver Transplantation in Children with Intestinal Failure-Associated Liver Disease: A Multicenter Integrated Study. J. Pediatr. 2021, 230, 46–54.e2. [Google Scholar] [CrossRef]
- Gura, K.; Premkumar, M.H.; Calkins, K.L.; Puder, M. Intravenous Fish Oil Monotherapy as a Source of Calories and Fatty Acids Promotes Age-Appropriate Growth in Pediatric Patients with Intestinal Failure-Associated Liver Disease. J. Pediatr. 2020, 219, 98–105.e4. [Google Scholar] [CrossRef]
- Premkumar, M.H.; Carter, B.A.; Hawthorne, K.M.; King, K.; Abrams, S.A. High rates of resolution of cholestasis in parenteral nutrition-associated liver disease with fish oil-based lipid emulsion monotherapy. J. Pediatr. 2013, 162, 793–798.e1. [Google Scholar] [CrossRef] [PubMed]
- Jurewitsch, B.; Gardiner, G.; Naccarato, M.; Jeejeebhoy, K.N. Omega-3-enriched lipid emulsion for liver salvage in parenteral nutrition-induced cholestasis in the adult patient. J. Parenter Enteral Nutr. 2011, 35, 386–390. [Google Scholar] [CrossRef]
- Fernandes, G.; Kaila, B.; Jeejeebhoy, K.N.; Gramlich, L.; Armstrong, D.; Allard, J.P. Canadian home parenteral nutrition (HPN) registry: Validation and patient outcomes. J. Parenter. Enteral. Nutr. 2012, 36, 407–414. [Google Scholar] [CrossRef]
- Lee, S.I.; Valim, C.; Johnston, P.; Le, H.D.; Meisel, J.; Arsenault, D.A.; Gura, K.M.; Puder, M. Impact of fish oil-based lipid emulsion on serum triglyceride, bilirubin, and albumin levels in children with parenteral nutrition-associated liver disease. Pediatr. Res. 2009, 66, 698–703. [Google Scholar] [CrossRef] [PubMed]
- De Meijer, V.E.; Le, H.D.; Meisel, J.A.; Gura, K.M.; Puder, M. Parenteral fish oil as monotherapy prevents essential fatty acid deficiency in parenteral nutrition-dependent patients. J. Pediatr. Gastroenterol. Nutr. 2010, 50, 212–218. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mercer, D.F.; Hobson, B.D.; Fischer, R.T.; Talmon, G.A.; Perry, D.A.; Gerhardt, B.K.; Grant, W.J.; Botha, J.F.; Langnas, A.N.; Quiros-Tejeira, R.E.; et al. Hepatic fibrosis persists and progresses despite biochemical improvement in children treated with intravenous fish oil emulsion. J. Pediatr. Gastroenterol. Nutr. 2013, 56, 364–369. [Google Scholar] [CrossRef]
- Holvik, K.; Madar, A.A.; Meyer, H.E.; Lofthus, C.M.; Stene, L.C. Changes in the vitamin D endocrine system and bone turnover after oral vitamin D3 supplementation in healthy adults: Results of a randomised trial. BMC Endocr. Disord. 2012, 12, 7. [Google Scholar] [CrossRef] [Green Version]
- Linecker, M.; Limani, P.; Botea, F.; Popescu, I.; Alikhanov, R.; Efanov, M.; Kim, P.; Khatkov, I.; Raptis, D.A.; Tschuor, C.; et al. A randomized, double-blind study of the effects of omega-3 fatty acids (Omegaven) on outcome after major liver resection. BMC Gastroenterol. 2015, 15, 102. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Linecker, M.; Botea, F.; Aristotele, D.; Nicolaescu, D.; Limani, P.; Alikhanov, R.; Kim, P.; Wirsching, A.; Kron, P.; Schneider, M.A.; et al. Perioperative omega-3 fatty acids fail to confer protection in liver surgery: Results of a multicentric, double-blind, randomized controlled trial. J. Hepatol. 2020, 72, 498–505. [Google Scholar] [CrossRef]
- Uno, H.; Furukawa, K.; Suzuki, D.; Shimizu, H.; Ohtsuka, M.; Kato, A.; Yoshitomi, H.; Miyazaki, M. Immunonutrition Suppresses Acute Inflammatory Responses through Modulation of Resolvin E1 in Patients Undergoing Major Hepatobiliary Resection. Surgery 2016, 160, 228–236. [Google Scholar] [CrossRef] [PubMed]
- Cockbain, A.J.; Volpato, M.; Race, A.D.; Munarini, A.; Fazio, C.; Belluzzi, A.; Loadman, P.M.; Toogood, G.J.; Hull, M.A. Anticolorectal cancer activity of the omega-3 polyunsaturated fatty acid eicosapentaenoic acid. Gut 2014, 63, 1760–1768. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Al-Taan, O.; Stephenson, J.A.; Spencer, L.; Pollard, C.; West, A.L.; Calder, P.C.; Metcalfe, M.; Dennison, A.R. Changes in plasma and erythrocyte omega-6 and omega-3 fatty acids in response to intravenous supply of omega-3 fatty acids in patients with hepatic colorectal metastases. Lipids Health Dis. 2013, 12, 64. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zhu, F.S.; Liu, S.; Chen, X.M.; Huang, Z.G.; Zhang, D.W. Effects of N-3 Polyunsaturated Fatty Acids from Seal Oils on Nonalcoholic Fatty Liver Disease Associated with Hyperlipidemia. World J. Gastroenterol. 2008, 14, 6395. [Google Scholar] [CrossRef]
- Sofi, F.; Giangrandi, I.; Cesari, F.; Corsani, I.; Abbate, R.; Gensini, G.F.; Casini, A. Effects of a 1-Year Dietary Intervention with n-3 Polyunsaturated Fatty Acid-Enriched Olive Oil on Non-Alcoholic Fatty Liver Disease Patients: A Preliminary Study. Int. J. Food Sci. Nutr. 2010, 61, 792–802. [Google Scholar] [CrossRef] [PubMed]
- Tobin, D.; Brevik-Andersen, M.; Qin, Y.; Innes, J.K.; Calder, P.C. Evaluation of a High Concentrate Omega-3 for Correcting the Omega-3 Fatty Acid Nutritional Deficiency in Non-Alcoholic Fatty Liver Disease (CONDIN). Nutrients 2018, 10, 1126. [Google Scholar] [CrossRef] [Green Version]
- Yan, J.H.; Guan, B.J.; Gao, H.Y.; Peng, X.E. Omega-3 polyunsaturated fatty acid supplementation and non-alcoholic fatty liver disease: A meta-analysis of randomized controlled trials. Medicine 2018, 97, e12271. [Google Scholar] [CrossRef]
- Tanaka, N.; Sano, K.; Horiuchi, A.; Tanaka, E.; Kiyosawa, K.; Aoyama, T. Highly-purified eicosapentaenoic acid treatment improves nonalcoholic steatohepatitis. J. Clin. Gastroenterol. 2008, 42, 413–418. [Google Scholar] [CrossRef] [Green Version]
- Li, Y.H.; Yang, L.H.; Sha, K.H.; Liu, T.G.; Zhang, L.G.; Liu, X.X. Efficacy of Poly-Unsaturated Fatty Acid Therapy on Patients with Nonalcoholic Steatohepatitis. World J. Gastroenterol. 2015, 21, 7008–7013. [Google Scholar] [CrossRef]
- Zöhrer, E.; Alisi, A.; Jahnel, J.; Mosca, A.; Della Corte, C.; Crudele, A.; Fauler, G.; Nobili, V. Efficacy of Docosahexaenoic Acid–Choline–Vitamin E in Paediatric NASH: A Randomized Controlled Clinical Trial. Appl. Physiol. Nutr. Metab. 2017, 42, 948–954. [Google Scholar] [CrossRef] [PubMed]
- Tomioka, K.; Kakibuchi, N.; Murakami, Y.; Kawakami, T.; Takaguchi, K.; Kita, K.; Okita, M. Effects of Eicosapentaenoic Acid Supplementation in the Treatment of Chronic Hepatitis C Patients. J. Nutr. Sci. Vitaminol. 2005, 51, 419–425. [Google Scholar] [CrossRef] [Green Version]
- Takaki, S.; Kawakami, Y.; Imamura, M.; Aikata, H.; Takahashi, S.; Ishihara, H.; Tsuji, K.; Aimitsu, S.; Kawakami, H.; Nakanishi, T.; et al. Eicosapentaenoic Acid Could Permit Maintenance of the Original Ribavirin Dose in Chronic Hepatitis C Virus Patients during the First 12 Weeks of Combination Therapy with Pegylated Interferon-α and Ribavirin: A Prospective Randomized Controlled Trial. Intervirology 2008, 50, 439–446. [Google Scholar] [CrossRef] [PubMed]
- Popa, S.G.; Mota, M. Impact of Obesity and Omega-3 Polyunsaturated Fatty Acids on Fibrogenesis and Responsiveness to Antiviral Therapy in Chronic Hepatitis C. Rom. J. Intern. Med. 2007, 45, 165–170. [Google Scholar] [PubMed]
- Pazirandeh, S.; Ling, P.R.; Ollero, M.; Gordon, F.; Burns, D.L.; Bistrian, B.R. Supplementation of Arachidonic Acid plus Docosahexaenoic Acid in Cirrhotic Patients Awaiting Liver Transplantation: A Preliminary Study. J. Parenter. Enter. Nutr. 2007, 31, 511–516. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mariqueo, T.A.; Zúñiga-Hernández, J. Omega-3 Derivatives, Specialized pro-Resolving Mediators: Promising Therapeutic Tools for the Treatment of Pain in Chronic Liver Disease. Prostaglandins Leukot. Essent. Fat. Acids 2020, 158, 102095. [Google Scholar] [CrossRef] [PubMed]
- Serhan, C.N. Controlling the Resolution of Acute Inflammation: A New Genus of Dual Anti-Inflammatory and Proresolving Mediators. J. Periodontol. 2008, 79, 1520–1526. [Google Scholar] [CrossRef] [PubMed]
- Qiu, W.; Guo, K.; Yi, L.; Gong, Y.; Huang, L.; Zhong, W. Resolvin E1 Reduces Hepatic Fibrosis in Mice with Schistosoma Japonicum Infection. Exp. Ther. Med. 2014, 7, 1481–1485. [Google Scholar] [CrossRef]
- Kuang, H.; Hua, X.; Zhou, J.; Yang, R. Resolvin D1 and E1 Alleviate the Progress of Hepatitis toward Liver Cancer in Long-Term Concanavalin A-Induced Mice through Inhibition of NF-ΚB Activity. Oncol. Rep. 2016, 35, 307–317. [Google Scholar] [CrossRef]
- Maciejewska, D.; Drozd, A.; Skonieczna-Żydecka, K.; Skórka-Majewicz, M.; Dec, K.; Jakubczyk, K.; Pilutin, A.; Stachowska, E. Eicosanoids in Nonalcoholic Fatty Liver Disease (NAFLD) Progression. Do Serum Eicosanoids Profile Correspond with Liver Eicosanoids Content during NAFLD Development and Progression? Molecules 2020, 25, 2026. [Google Scholar] [CrossRef]
- Jung, T.W.; Hwang, H.J.; Hong, H.C.; Choi, H.Y.; Yoo, H.J.; Baik, S.H.; Choi, K.M. Resolvin D1 Reduces ER Stress-Induced Apoptosis and Triglyceride Accumulation through JNK Pathway in HepG2 Cells. Mol. Cell. Endocrinol. 2014, 391, 30–40. [Google Scholar] [CrossRef] [PubMed]
- Sun, L.; Wang, Y.; Wang, L.; Yao, B.; Chen, T.; Li, Q.; Liu, Z.; Liu, R.; Niu, Y.; Song, T.; et al. Resolvin D1 Prevents Epithelial-Mesenchymal Transition and Reduces the Stemness Features of Hepatocellular Carcinoma by Inhibiting Paracrine of Cancer-Associated Fibroblast-Derived COMP. J. Exp. Clin. Cancer Res. 2019, 38, 170. [Google Scholar] [CrossRef] [PubMed]
- Kang, J.W.; Lee, S.M. Resolvin D1 Protects the Liver from Ischemia/Reperfusion Injury by Enhancing: M2 Macrophage Polarization and Efferocytosis. Biochim. Biophys. Acta Mol. Cell Biol. Lipids 2016, 1861, 1025–1035. [Google Scholar] [CrossRef]
- Abshagen, K.; Hartmann, A.; Grüner, L.; Liebig, M.; Vollmar, B. Limited Potential of Resolvin D1 in Treatment of Cholestatic Liver Fibrosis. Hepatobiliary Surg. Nutr. 2019, 9, 587–596. [Google Scholar] [CrossRef]
- Li, R.; Wang, Y.; Zhao, E.; Wu, K.; Li, W.; Shi, L.; Wang, D.; Xie, G.; Yin, Y.; Deng, M.; et al. Maresin 1, a Proresolving Lipid Mediator, Mitigates Carbon Tetrachloride-Induced Liver Injury in Mice. Oxid. Med. Cell. Longev. 2016, 2016, 9203716. [Google Scholar] [CrossRef] [PubMed]
- Hwang, S.M.; Chung, G.; Kim, Y.H.; Park, C.K. The Role of Maresins in Inflammatory Pain: Function of Macrophages in Wound Regeneration. Int. J. Mol. Sci. 2019, 21, 5849. [Google Scholar] [CrossRef] [Green Version]
- Abdolmaleki, F.; Kovanen, P.T.; Mardani, R.; Gheibi-hayat, S.M.; Bo, S.; Sahebkar, A. Resolvins: Emerging Players in Autoimmune and Inflammatory Diseases. Clin. Rev. Allergy Immunol. 2020, 58, 82–91. [Google Scholar] [CrossRef]
- Giera, M.; Ioan-Facsinay, A.; Toes, R.; Gao, F.; Dalli, J.; Deelder, A.M.; Serhan, C.N.; Mayboroda, O.A. Lipid and Lipid Mediator Profiling of Human Synovial Fluid in Rheumatoid Arthritis Patients by Means of LC-MS/MS. Biochim. Biophys. Acta 2012, 1821, 1415–1421. [Google Scholar] [CrossRef] [Green Version]
- Herrera, B.S.; Hasturk, H.; Kantarci, A.; Freire, M.O.; Nguyen, O.; Kansal, S.; van Dyke, T.E. Impact of Resolvin E1 on Murine Neutrophil Phagocytosis in Type 2 Diabetes. Infect. Immun. 2015, 83, 792–801. [Google Scholar] [CrossRef] [Green Version]
- Sima, C.; Paster, B.; Van Dyke, T.E. Function of Pro-Resolving Lipid Mediator Resolvin E1 in Type 2 Diabetes. Crit. Rev. Immunol. 2018, 38, 343–365. [Google Scholar] [CrossRef]
- Freire, M.O.; Dalli, J.; Serhan, C.N.; Van Dyke, T.E. Neutrophil Resolvin E1 Receptor Expression and Function in Type 2 Diabetes. J. Immunol. 2017, 198, 718–728. [Google Scholar] [CrossRef] [Green Version]
- Hasturk, H.; Abdallah, R.; Kantarci, A.; Nguyen, D.; Giordano, N.; Hamilton, J.; Van Dyke, T.E. Resolvin E1 (RvE1) Attenuates Atherosclerotic Plaque Formation in Diet and Inflammation-Induced Atherogenesis. Arterioscler. Thromb. Vasc. Biol. 2015, 35, 1123–1133. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Colas, R.A.; Shinohara, M.; Dalli, J.; Chiang, N.; Serhan, C.N. Identification and Signature Profiles for Pro-Resolving and Inflammatory Lipid Mediators in Human Tissue. Am. J. Physiol. Cell Physiol. 2014, 307, C39–C54. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mas, E.; Croft, K.D.; Zahra, P.; Barden, A.; Mori, T.A. Resolvins D1, D2, and Other Mediators of Self-Limited Resolution of Inflammation in Human Blood Following n-3 Fatty Acid Supplementation. Clin. Chem. 2012, 58, 1476–1484. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Souza, P.R.; Marques, R.M.; Gomez, E.A.; Colas, R.A.; De Matteis, R.; Zak, A.; Patel, M.; Collier, D.J.; Dalli, J. Enriched Marine Oil Supplements Increase Peripheral Blood Specialized Pro-Resolving Mediators Concentrations and Reprogram Host Immune Responses: A Randomized Double-Blind Placebo-Controlled Study. Circ. Res. 2020, 126, 75–90. [Google Scholar] [CrossRef] [PubMed]
- Barden, A.; Shinde, S.; Tsai, I.J.; Croft, K.D.; Beilin, L.J.; Puddey, I.B.; Mori, T.A. Effect of Weight Loss on Neutrophil Resolvins in the Metabolic Syndrome. Prostaglandins Leukot. Essent. Fat. Acids 2019, 148, 25–29. [Google Scholar] [CrossRef]
- Cata, J.P.; Velasquez, J.F.; Ramirez, M.F.; Vauthey, J.N.; Gottumukkala, V.; Conrad, C.; Kim, B.J.; Aloia, T. Inflammation and Pro-Resolution Inflammation after Hepatobiliary Surgery. World J. Surg. Oncol. 2017, 15, 152. [Google Scholar] [CrossRef] [Green Version]



{kind=link}
{kind=link}
{kind=link}
| Liver Conditions or Diseases | Number of Studies | Most Common Dosage Used (Daily) ** | Duration of Studios (Average in Months) | Others Clinical Conditions Evaluated or of Interest | General Analysis Realized or Proposed |
|---|---|---|---|---|---|
| NAFLD [117,118,119,120,121,122,123,124,125,126,127,128,129,130,131,132,133,134,135,136,137] | 32 | 4 g (32%) *** | 6 (0.5 to 24) | Three assays are related to morbid obesity and one of them to bariatric surgery One study is related to diabetics with PNPLA3 genotype | Liver parameters of injury measured by biochemical analysis and echography/tomography/MRI Lipids profile and liver fat fraction Insulin resistance Oxidative stress and inflammatory markers Abdominal adiposity (waist circumference) |
| NASH [125,138,139] | 8 | 4 g (50%) | 8 (0.75 to 12) | One study comprises long term parenteral immunonutrition related to hepatic steatosis | Liver parameters of injury measured by biochemical analysis and biopsy, echography/tomography/MRI Lipids profile and liver fat fraction Gut microbiota, abdominal adiposity (waist circumference) and other anthropometric measures |
| Hepatic disease related to parenteral nutrition [140,141,142,143,144,145,146,147,148,149,150,151] | 22 | 1 g/kg/day (59%) | 3 (1.5 to 60) | - | Liver parameters of injury measures by biochemical analysis General metabolic and fatty acid profile Inflammatory markers Gain of weight |
| HCC [88] | 3 | 100 mL (10 g) (66.6%) | 3 | - | Postoperatory complications Hepatic and renal function Hospital stays Survival analysis |
| Healthy people [152] | 2 | 0.5–1.2 g | 1 | - | Liver profile Changes in vitamin D and parathyroid hormone production Free fatty acids profile |
| Hepatitis C (chronic infection) | 2 | 4 g | No specified | One assay related to insulin resistance | General biochemical analysis Analysis related to omega-3 as coadjuvant to interferon |
| Mayor liver resection [153,154,155] | 2 | 100 mL (10 g) | 1 | One assay includes liver donor for transplant | Postoperatory complications Liver regeneration analysis |
| Hepatic metastasis [156,157] | 4 | 4 g | 12.5 (0.5 to 24) | Most of the studies are related to colorectal cancer | Quality of life General survival Changes in corporal lean fat Omega-3 distribution Ki67 and cancer proliferation Inflammation and angiogenesis |
| Liver transplants | 3 | 1g/kg/day (75%) or 100 mL (10 g) (25%) | From the surgery until 5 days postoperatory and one month later | - | Analysis of neurologic complications Liver general parameters Allographic dysfunction Liver regeneration Survival analysis |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Herrera Vielma, F.; Valenzuela, R.; Videla, L.A.; Zúñiga-Hernández, J. N-3 Polyunsaturated Fatty Acids and Their Lipid Mediators as A Potential Immune–Nutritional Intervention: A Molecular and Clinical View in Hepatic Disease and Other Non-Communicable Illnesses. Nutrients 2021, 13, 3384. https://doi.org/10.3390/nu13103384
Herrera Vielma F, Valenzuela R, Videla LA, Zúñiga-Hernández J. N-3 Polyunsaturated Fatty Acids and Their Lipid Mediators as A Potential Immune–Nutritional Intervention: A Molecular and Clinical View in Hepatic Disease and Other Non-Communicable Illnesses. Nutrients. 2021; 13(10):3384. https://doi.org/10.3390/nu13103384
Chicago/Turabian StyleHerrera Vielma, Francisca, Rodrigo Valenzuela, Luis A. Videla, and Jessica Zúñiga-Hernández. 2021. "N-3 Polyunsaturated Fatty Acids and Their Lipid Mediators as A Potential Immune–Nutritional Intervention: A Molecular and Clinical View in Hepatic Disease and Other Non-Communicable Illnesses" Nutrients 13, no. 10: 3384. https://doi.org/10.3390/nu13103384