
Predictors of Moderate or Severe Cognitive Impairment at Six Months of the Hip Fracture in the Surgical Patient over 65 Years of Age

 ,
,
Abstract
:1. Introduction
2. Materials and Methods
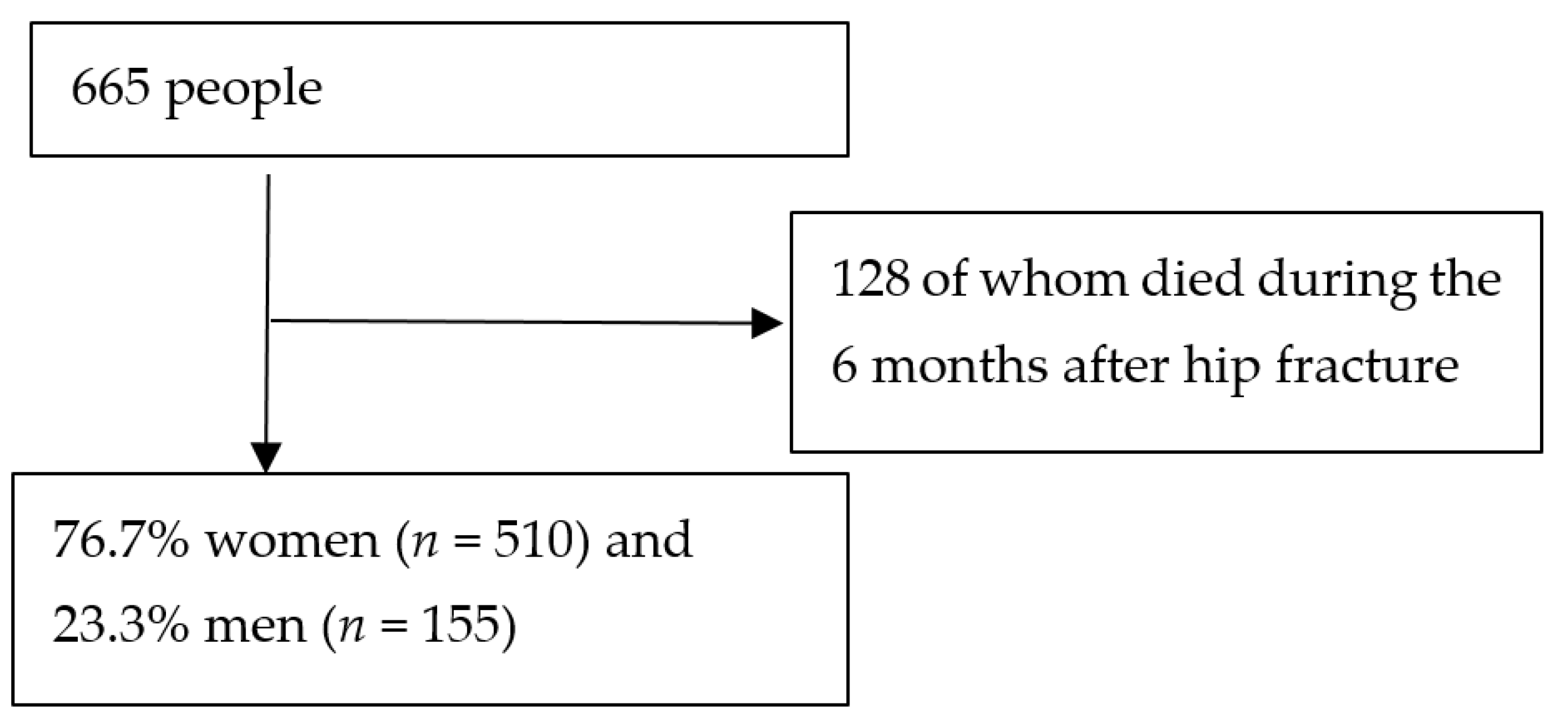
2.1. Study Design—Participants
2.2. Sample Size
2.3. Main Outcomes—Instruments
2.4. Statistical Analysis
3. Results
3.1. Characteristics at Admission and Cognitive Impairment at the Sixth Month in Patients with Hip Fracture
3.2. Complications during Admission and Characteristics at Discharge and Their Relationship with Cognitive Impairment at the Sixth Month in Patients with Hip Fracture
3.3. Characteristics at the Sixth Month and Their Relationship with Moderate or Severe Cognitive Impairment in Patients with Hip Fracture
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Conflicts of Interest
References
- Wantonoro, W.; Kuo, W.Y.; Shyu, Y.L. Changes in Health-Related Quality of Life for Older Persons with Cognitive Impairment After Hip Fracture Surgery: A Systematic Review. J. Nurs. Res. 2020, 28, e97. [Google Scholar] [CrossRef]
- Holmes, J.D.; House, A.O. Psychiatric illness in hip fracture. Age Ageing 2000, 29, 537–546. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Yiannopoulou, K.G.; Anastasiou, I.P.; Ganetsos, T.K.; Efthimiopoulos, P.; Papageorgiou, S.G. Prevalence of dementia in elderly patients with hip fracture. Hip Int. 2012, 22, 209–213. [Google Scholar] [CrossRef] [PubMed]
- Taylor, B.C.; Schreiner, P.J.; Stone, K.L.; Fink, H.A.; Cummings, S.R.; Nevitt, M.C.; Bowman, P.J.; Ensrud, K.E. Long-term prediction of incident hip fracture risk in elderly white women: Study of osteoporotic fractures. J. Am. Geriatr. Soc. 2004, 52, 1479–1486. [Google Scholar] [CrossRef] [PubMed]
- Friedman, S.M.; Menzies, I.B.; Bukata, S.V.; Mendelson, D.A.; Kates, S.L. Dementia and hip fractures: Development of a pathogenic framework for understanding and studying risk. Geriatr. Orthop. Surg. Rehabil. 2010, 1, 52–62. [Google Scholar] [CrossRef]
- Jiménez Mola, S.; Calvo-Lobo, C.; Idoate Gil, J.; Seco Calvo, J. Cognitive Impairment Level and Elderly Hip Fracture: Implications in Rehabilitation Nursing. Rehabil. Nurs. 2020, 45, 147–157. [Google Scholar] [CrossRef]
- Mattison, M.L.P. Delirium. Ann. Intern. Med. 2020, 173, 49–64. [Google Scholar] [CrossRef]
- Romero Pisonero, E.; Mora Fernández, J. Multidisciplinary geriatric rehabilitation in the patient with hip fracture and dementia. Rev. Esp. Geriatr. Gerontol. 2019, 54, 220–229. [Google Scholar] [CrossRef]
- Vega Alonso, T.; Miralles Espí, M.; Mangas Reina, J.M.; Castrillejo Pérez, D.; Rivas Pérez, A.I.; Gil Costa, M.; Lopez Maside, A.; Arrieta Anton, E.; Lozano Alonso, J.E.; Forge Gil, M. Prevalence of cognitive impairment in Spain: The Gómez de Caso study in health sentinel networks. Neurology 2018, 33, 491–498. [Google Scholar] [CrossRef]
- Rodriguez-Sanchez, E.; Mora-Simon, S.; Patino-Alonso, M.C.; García-García, R.; Escribano-Hernandez, A.; Garcia-Ortiz, L.; Perea-Bartolomé, M.V.; Gómez-Marcos, M.A. Prevalence of cognitive impairment in individuals aged over 65 in an urban area: DERIVA study. BMC Neurol. 2011, 17, 147. [Google Scholar] [CrossRef] [Green Version]
- National Registry of Hip Fractures due to Fragility. Annual Report 2017. p. 44. Available online: http://www.idipaz.es/PaginaDinamica.aspx?IdPag=219&Lang=ES (accessed on 3 December 2021).
- Alfaro Latorre, M.; Institute of Health Information. Commented Statistics: Attention to Hip Fracture in the NHS; Ministry of Health, Social Policy: Madrid, Spain, 2010. Available online: http://www.msps.es/estadEstudios/estadisticas/cmbdhome.htm (accessed on 3 December 2021).
- Katz, S.; Ford, A.B.; Moskowitz, R.W.; Jackson, B.A.; Jaffe, M.W. Studies of illness in the aged. The Index of ADL: A standardized measure of biological and psichosocial function. JAMA 1963, 185, 914–919. [Google Scholar] [CrossRef] [PubMed]
- Agüero-Torres, H.; Fratiglioni, L.; Guo, Z.; Viitanen, M.; von Strauss, E.; Winblad, B. Dementia is the major cause of functional dependence in the elderly: 3-year follow-up data from a population-based study. Am. J. Public Health 1998, 88, 1452–1456. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Pereira, J.V.; Aung Thein, M.Z.; Nitchingham, A.; Caplan, G.A. Delirium in older adults is associated with development of new dementia: A systematic review and meta-analysis. Int. J. Geriatric Psychiatry 2021, 36, 993–1003. [Google Scholar] [CrossRef] [PubMed]
- Mundi, S.; Chaudhry, H.; Bhandari, M. Systematic review on the inclusion of patients with cognitive impairment in hip fracture trials: A missed opportunity? Can. J. Surg. 2014, 57, 141–145. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- National Institute of Statistics (INE). Available online: https://www.ine.es/ (accessed on 10 December 2021).
- Alvarez-Nebreda, M.L.; Jimenez, A.B.; Rodriguez, P.; Serra, J.A. Epidemiology of hip fracture in the elderly in Spain. Bone 2008, 42, 278–285. [Google Scholar] [CrossRef] [PubMed]
- Pfeiffer, E. A short portable mental status questionnaire for the assessment of organic brain deficit in elderly patients. J. Am. Geriatr. Soc. 1975, 23, 433–441. [Google Scholar] [CrossRef]
- Martinez de la Iglesia, J.; Dueñas Herrero, R.; Onís Vilches, M.C.; Aguado Taberné, C.; Albert Colomer, C.; Luque Luque, R. Spanish language adaptation and validation of the Pfeiffer’s questionnaire (SPMSQ) to detect cognitive deterioration in people over 65 years of age. Med. Clin. 2001, 117, 129–134. [Google Scholar] [CrossRef]
- Johansen, A.; Tsang, C.; Boulton, C.; Wakeman, R.; Moppett, I. Understanding mortality rates after hip fracture repair using ASA physical status in the National Hip Fracture Database. Anaesthesia 2017, 72, 961–966. [Google Scholar] [CrossRef] [Green Version]
- Baztan, J.J.; Pérez del Molino, J.; Alarcón, T.; San Cristobal, E.; Left, G.; Manzarbeitia, I. Barthel index: Valid instrument for the functional assessment of patients with cerebrovascular disease. Rev. Esp. Geriatr. Gerontol. 1993, 28, 32–40. [Google Scholar]
- Holden, M.K.; Gill, K.M.; Magliozzi, M.R.; Nathan, J.; Piehl-Baker, L. Clinical gait assessment in the neurologically impaired. Reliability and meaningfulness. Phys. Ther. 1984, 64, 35–40. [Google Scholar] [CrossRef]
- Magaziner, J.; Simonsick, E.M.; Kashner, T.M.; Hebel, J.R.; Kenzora, J.E. Predictors of functional recovery one year following hospital discharge for hip fracture: A prospective study. J. Gerontol. 1990, 45, 101–107. [Google Scholar] [CrossRef] [PubMed]
- Gruber-Baldini, A.L.; Zimmerman, S.; Morrison, R.S.; Grattan, L.M.; Hebel, J.R.; Dolan, M.M.; Hawkes, W.; Magaziner, J. Cognitive impairment in hip fracture patients: Timing of detection and longitudinal follow-up. J. Am. Geriatr. Soc. 2003, 51, 1227–1236. [Google Scholar] [CrossRef] [PubMed]
- Söderqvist, A.; Miedel, R.; Ponzer, S.; Tidermark, J. The influence of cognitive function on outcome after a hip fracture. J. Bone Jt. Surg. Am. 2006, 88, 2115–2123. [Google Scholar] [CrossRef] [Green Version]
- Givens, J.L.; Sanft, T.B.; Marcantonio, E.R. Functional recovery after hip fracture: The combined effects of depressive symptoms.; cognitive impairment.; and delirium. J. Am. Geriatr. Soc. 2008, 56, 1075–1079. [Google Scholar] [CrossRef]
- Samuelsson, B.; Hedström, M.I.; Ponzer, S.; Söderqvist, A.; Samnegård, E.; Thorngren, K.G.; Cederholm, T.; Sääf, M.; Dalen, N. Gender differences and cognitive aspects on functional outcome after hip fracture—A 2 years’ follow-up of 2.134 patients. Age Ageing 2009, 38, 686–692. [Google Scholar] [CrossRef] [Green Version]
- Seitz, D.P.; Gill, S.S.; Gruneir, A.; Austin, P.C.; Anderson, G.M.; Bell, C.M.; Rochon, P.A. Effects of dementia on postoperative outcomes of older adults with hip fractures: A population-based study. J. Am. Med. Dir. Assoc. 2014, 15, 334–341. [Google Scholar] [CrossRef]
- Peeters, C.M.; Visser, E.; Van de Ree, C.L.; Gosens, T.; Den Oudsten, B.L.; De Vries, J. Quality of life after hip fracture in the elderly: A systematic literature review. Injury 2016, 47, 1369–1382. [Google Scholar] [CrossRef]
- Alexiou, K.I.; Roushias, A.; Varitimidis, S.E.; Malizos, K.N. Quality of life and psychological consequences in elderly patients after a hip fracture: A review. Clin. Interv. Aging 2018, 13, 143–150. [Google Scholar] [CrossRef] [Green Version]
- Larsson, G.; Strömberg, U.; Rogmark, C.; Nilsdotter, A. Cognitive status following a hip fracture and its association with postoperative mortality and activities of daily living: A prospective comparative study of two prehospital emergency care procedures. Int. J. Orthop. Trauma Nurs. 2019, 35, 100705. [Google Scholar] [CrossRef]
- Sonn, U.; Törnquist, K.; Svensson, E. The ADL taxonomy—From individual categorical data to ordinal categorical data. Scand. J. Occup. Ther. 1999, 6, 11–20. [Google Scholar] [CrossRef]
- Córcoles-Jiménez, M.P.; Villada-Munera, A.; Del Egido-Fernández, M.A.; Candel-Parra, E.; Moreno-Moreno, M.; Jimenez-Sanchez, M.D.; Piña-Martínez, A. Recovery of activities of daily living among older people one year after hip fracture. Clin. Nurs. Res. 2015, 24, 604–623. [Google Scholar] [CrossRef] [PubMed]
- Giusti, A.; Barone, A.; Pioli, G. Rehabilitation after hip fracture in patients with dementia. J. Am. Geriatr. Soc. 2007, 55, 1309–1310. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| Characteristics at the Entrance | PS 6th Month | Chi2 Test | OR | ||||
|---|---|---|---|---|---|---|---|
| PS ≤ 4 | PS ≥ 5 | χ2 χ RV2 | p-Value | Rho | Lower Limit | Upper Limit | |
| Age | |||||||
| <85 years (n = 208) | 171 (82.2%) | 37 (17.8%) | 12.85 | <0.001 <0.001 | 0.455 | 0.298 | 0.696 |
| ≥85 years (n = 329) | 223 (67.8%) | 106 (32.2%) | 14.11 | 2.197 | 1.438 | 3.357 | |
| Type of fracture | |||||||
| Intracapsular (n = 225) | 170 (43.1%) | 55 (38.5%) | 0.76 | 0.382 | p > 0.05 | ||
| Extracapsular (n = 312) | 224 (56.9%) | 88 (61.5%) | 0.95 | 0.329 | |||
| Antidepressants | |||||||
| Yes (n = 148) | 95 (64.2%) | 53 (35.8%) | 8.18 | 0.004 | 1.853 | 1.230 | 2.794 |
| No (n = 398) | 299 (76.9%) | 90 (23.1%) | 8.5 | 0.004 | 0.54 | 0.358 | 0.813 |
| Neuroleptics | |||||||
| Yes (n = 85) | 23 (27.1%) | 62 (72.9%) | 108.06 | <0.001 | 12.347 | 7.228 | 21.092 |
| No (n = 482) | 371 (82.1%) | 81 (17.9%) | 98.12 | <0.001 | 0.081 | 0.047 | 0.138 |
| Thickeners | |||||||
| Yes (n = 9) | 3 (33.3%) | 6 (66.7%) | 5.57 | 0.018 | 5.708 | 1.408 | 23.136 |
| No (n = 528) | 391 (74.1%) | 137 (25.9%) | 6.41 | 0.011 | 0.175 | 0.043 | 0.71 |
| BI | |||||||
| ≥60 (n = 552) | 476 (95.2%) | 76 (46.1) | 143.71 | <0.001 | 0.035 | 0.017 | 0.071 |
| <60 (n = 114) | 25 (4.8%) | 89 (53.9) | 131.12 | <0.001 | 28.566 | 14.046 | 58.097 |
| PS | |||||||
| ≤4 (n = 414) | 391 (94.4%) | 23 (5.6%) | 406.15 | <0.001 | 0.001 | 0.000 | 0.005 |
| ≥5 (n = 123) | 3 (2.4%) | 120 (97.6%) | 416.56 | <0.001 | 680.0 | 200.7 | 2304.2 |
| Ability to roam | |||||||
| Good or regular (n = 486) | 380 (78.2%) | 106 (21.8%) | 58.25 | <0.001 | 0.106 | 0.055 | 0.203 |
| Bad (n = 51) | 14 (27.5%) | 37 (72.5%) | 52.66 | <0.001 | 9.474 | 4.938 | 18.177 |
| Previous institutionalization | |||||||
| No (n = 391) | 338 (86.4%) | 53 (13.6%) | 123.37 | <0.001 | 0.098 | 0.063 | 0.152 |
| Yes (n = 146) | 56 (38.4%) | 90 (61.6%) | 117.72 | <0.001 | 10.249 | 6.590 | 15.942 |
| Surgical risk | |||||||
| ASA I+II (n = 265) | 213 (54.8%) | 52 (37.4%) | 11.64 | <0.001 | 0.494 | 0.332 | 0.735 |
| ASA III+IV (n = 263) | 176 (45.2%) | 87 (62.6%) | 12.43 | <0.001 | 2.025 | 1.361 | 3.013 |
| Characteristics at the Entrance | LR | OR | |||
|---|---|---|---|---|---|
| χ 2 Wald | p-Value | Rho | Lower Limit | Upper Limit | |
| Age | 4.053 | 0.044 | 1.078 | 1.002 | 1.160 |
| Gender: male | 0.289 | 0.591 | 0.733 | 0.236 | 2.277 |
| PS: ≥ 5 | 71.168 | <0.001 | 535.762 | 124.437 | 2306.709 |
| Antidepressants: Yes | 0.106 | 0.744 | 0.844 | 0.305 | 2.338 |
| Neuroleptics: Yes | 0.457 | 0.499 | 1.620 | 0.400 | 6.567 |
| Thickeners: Yes | 0.021 | 0.884 | 0.778 | 0.027 | 22.350 |
| BI: < 60 | 10.802 | 0.001 | 15.474 | 3.021 | 79.249 |
| Ability to roam: Poor | 2.116 | 0.146 | 0.221 | 0.029 | 1.689 |
| Previous institutionalization: Yes | 12.236 | <0.001 | 5.349 | 2.090 | 13.687 |
| Surgical risk: ASA III or IV | 0.148 | 0.700 | 1.205 | 0.467 | 3.108 |
| Complications During Admission and Characteristics at Discharge | PS 6th Month | Chi2 Test | OR | ||||
|---|---|---|---|---|---|---|---|
| PS ≤ 4 | PS ≥ 5 | χ2 χ RV 2 | p-Value | Rho | Lower Limit | Upper Limit | |
| Type of treatment | |||||||
| Surgical (n = 528) | 389 (73.7%) | 139 (26.3%) | 0.7 1.34 | 0.401 0.247 | p > 0.05 | ||
| Conservative (n = 9) | 5 (55.6%) | 4 (44.4%) | |||||
| Surgical intervention | |||||||
| Synthesis (n = 321) | 234 (72.9%) | 87 (27.1%) | 0.16 0.26 | 0.686 | p > 0.05 | ||
| Arthroplasty (n = 207) | 155 (74.9%) | 52 (25.1%) | 0.613 | ||||
| “Delirium” | |||||||
| Yes (n = 170) | 91 (23.1%) | 79 (55.2%) | 48.64 47.93 | <0.001 <0.001 | 4.110 | 2.743 | 6.159 |
| No (n = 367) | 303 (76.9%) | 64 (44.8%) | 0.243 | 0.162 | 0.365 | ||
| Constipation | |||||||
| Yes (n = 226) | 145 (36.8%) | 81 (56.6%) | 16.14 16.8 | <0.001 <0.001 | 2.243 | 1.521 | 3.310 |
| No (n = 311) | 249 (63.2%) | 62 (43.4%) | 0.446 | 0.302 | 0.658 | ||
| IB upon discharge | |||||||
| ≥60 (n = 390) | 340 (87.2%) | 50 (12.8%) | 136.48 130.40 | <0.001 <0.001 | 0.085 | 0.055 | 0.134 |
| <60 (n = 147) | 54 (36.7%) | 93 (63.3%) | 11.711 | 7.483 | 18.327 | ||
| Worsening BI during admission | |||||||
| No (n = 195) | 110 (56.4%) | 85 (43.6%) | 43.73 43.93 | <0.001 <0.001 | 3.784 | 2.537 | 5.644 |
| Yes (n = 342) | 284 (83%) | 58 (17%) | 0.264 | 0.177 | 0.394 | ||
| PS at discharge | |||||||
| ≤4 (n = 411) | 390 (94.9%) | 21 (5.1%) | 410.51 421.13 | <0.001 <0.001 | 0.002 | 0.001 | 0.005 |
| ≥5 (n = 126) | 4 (3.2%) | 122 (96.8%) | 566.429 | 190.746 | 1682.031 | ||
| Worsening PS during admission | |||||||
| No (n = 518) | 380 (73.4%) | 138 (26.6%) | 0.00 0.00 | >0.05 | p > 0.05 | ||
| Yes (n = 19) | 14 (73.7%) | 5 (26.3%) | >0.05 | ||||
| Ability to roam | |||||||
| Good or regular (n = 342) | 301 (88%) | 41 (12%) | 101.28 101.69 | <0.001 <0.001 | 0.124 | 0.081 | 0.191 |
| Bad (n = 195) | 93 (47.7%) | 102 (52.3%) | 8.052 | 5.235 | 12.385 | ||
| Institutionalization | |||||||
| No (n = 229) | 272 (88.3%) | 36 (11.7%) | 80.74 83.77 | <0.001 <0.001 | 0.151 | 0.098 | 0.233 |
| Yes (n = 308) | 122 (53.3%) | 107 (46.7%) | 6.627 | 4.294 | 10.226 | ||
| Complications During Admission and Characteristics at Discharge | LR | OR | |||
|---|---|---|---|---|---|
| χ 2 Wald | p-Value | Rho | Lower Limit | Upper Limit | |
| Age | 1.388 | 0.239 | 1.046 | 0.97 | 1.128 |
| Gender: male | 0.176 | 0.675 | 0.794 | 0.27 | 2.334 |
| PS at discharge: ≥ 5 | 82.215 | <0.001 | 547.91 | 140.19 | 2141.45 |
| “Delirium”: Yes | 1.697 | 0.193 | 0.510 | 0.185 | 1.405 |
| Persistent constipation: Yes | 0.218 | 0.640 | 1.245 | 0.496 | 3.124 |
| BI at discharge: < 60 | 0.194 | 0.660 | 1.266 | 0.443 | 3.619 |
| IB worsening during admission: Yes | 0.027 | 0.869 | 1.174 | 0.174 | 7.938 |
| Ability to roam: Poor | 9.105 | 0.003 | 5.071 | 1.766 | 14.556 |
| Institutionalization at discharge: Yes | 13.045 | <0.001 | 0.148 | 0.053 | 0.418 |
| Characteristics of the Sixth Month | EP 6th Month | Chi2 Test | OR | ||||
|---|---|---|---|---|---|---|---|
| PS ≤ 4 | PS ≥ 5 | χ2 χ RV 2 | p-Value | Rho | Lower Limit | Upper Limit | |
| BI | |||||||
| ≥60 (n = 405) | 358 (88.4%) | 47 (11.6%) | 187.24 176.96 | <0.001 <0.001 | 0.049 | 0.030 | 0.080 |
| <60 (n = 132) | 36 (27.3%) | 96 (72.7%) | 20.312 | 12.455 | 33.125 | ||
| Ability to roam | |||||||
| Good or regular (n = 402) | 349 (86.8%) | 53 (13.2%) | 145.23 | <0.001 <0.001 | 0.076 | 0.048 | 0.120 |
| Bad (n = 135) | 45 (33.3%) | 90 (66.7%) | 137.11 | 13.170 | 8.314 | 20.861 | |
| Recovery of initial gait capacity | |||||||
| Yes (n = 298) | 241 (80.87%) | 57 (19.13%) | 18.43 | <0.001 | 0.421 | 0.285 | 0.622 |
| No (n = 239) | 153 (64.02%) | 86 (35.98%) | 19.25 | <0.001 | 2.377 | 1.607 | 3.515 |
| Institutionalization | |||||||
| No (n = 303) | 275 (90.8%) | 28 (9.2%) | 105.57 | <0.001 <0.001 | 0.105 | 0.066 | 0.168 |
| Yes (n = 234) | 119 (50.9%) | 115 (49.1%) | 111.40 | 9.491 | 5.958 | 15.120 | |
| Worsening PS since admission | |||||||
| No (n = 459) | 370 (80.6%) | 89 (19.4%) | 82.23 | <0.001 <0.001 | 0.107 | 0.063 | 0.182 |
| Yes (n = 78) | 24 (30.8%) | 54 (69.2%) | 74.64 | 9.354 | 5.486 | 15.949 | |
| Characteristics of the Sixth Month | LR | OR | |||
|---|---|---|---|---|---|
| χ 2 Wald | p-Value | Rho | Lower Limit | Upper Limit | |
| Age | 0.523 | 0.470 | 0.985 | 0.946 | 1.026 |
| Gender: Male | 0.002 | 0.961 | 1.016 | 0.531 | 1.944 |
| BI: < 60 | 29.881 | <0.001 | 8.088 | 3.823 | 17.115 |
| Ability to roam: Poor | 2.732 | 0.098 | 1.884 | 0.889 | 3.993 |
| Recovery of initial gait capacity: No | 1.395 | 0.238 | 1.418 | 0.794 | 2.529 |
| Institutionalization: Yes | 33.357 | <0.001 | 6.317 | 3.379 | 11.807 |
| Worsening PS since admission: Yes | 27.627 | <0.001 | 7.024 | 3.396 | 14.531 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
González-Marcos, E.; González-García, E.; Rodríguez-Fernández, P.; González-Bernal, J.J.; Sánchez-González, E.; González-Santos, J. Predictors of Moderate or Severe Cognitive Impairment at Six Months of the Hip Fracture in the Surgical Patient over 65 Years of Age. J. Clin. Med. 2022, 11, 2608. https://doi.org/10.3390/jcm11092608
González-Marcos E, González-García E, Rodríguez-Fernández P, González-Bernal JJ, Sánchez-González E, González-Santos J. Predictors of Moderate or Severe Cognitive Impairment at Six Months of the Hip Fracture in the Surgical Patient over 65 Years of Age. Journal of Clinical Medicine. 2022; 11(9):2608. https://doi.org/10.3390/jcm11092608
Chicago/Turabian StyleGonzález-Marcos, Enrique, Enrique González-García, Paula Rodríguez-Fernández, Jerónimo J. González-Bernal, Esteban Sánchez-González, and Josefa González-Santos. 2022. "Predictors of Moderate or Severe Cognitive Impairment at Six Months of the Hip Fracture in the Surgical Patient over 65 Years of Age" Journal of Clinical Medicine 11, no. 9: 2608. https://doi.org/10.3390/jcm11092608