
Vascular Complications in Patients with Chronic Pancreatitis

 , , , ,
, , , ,
Abstract
:1. Introduction
2. Methods
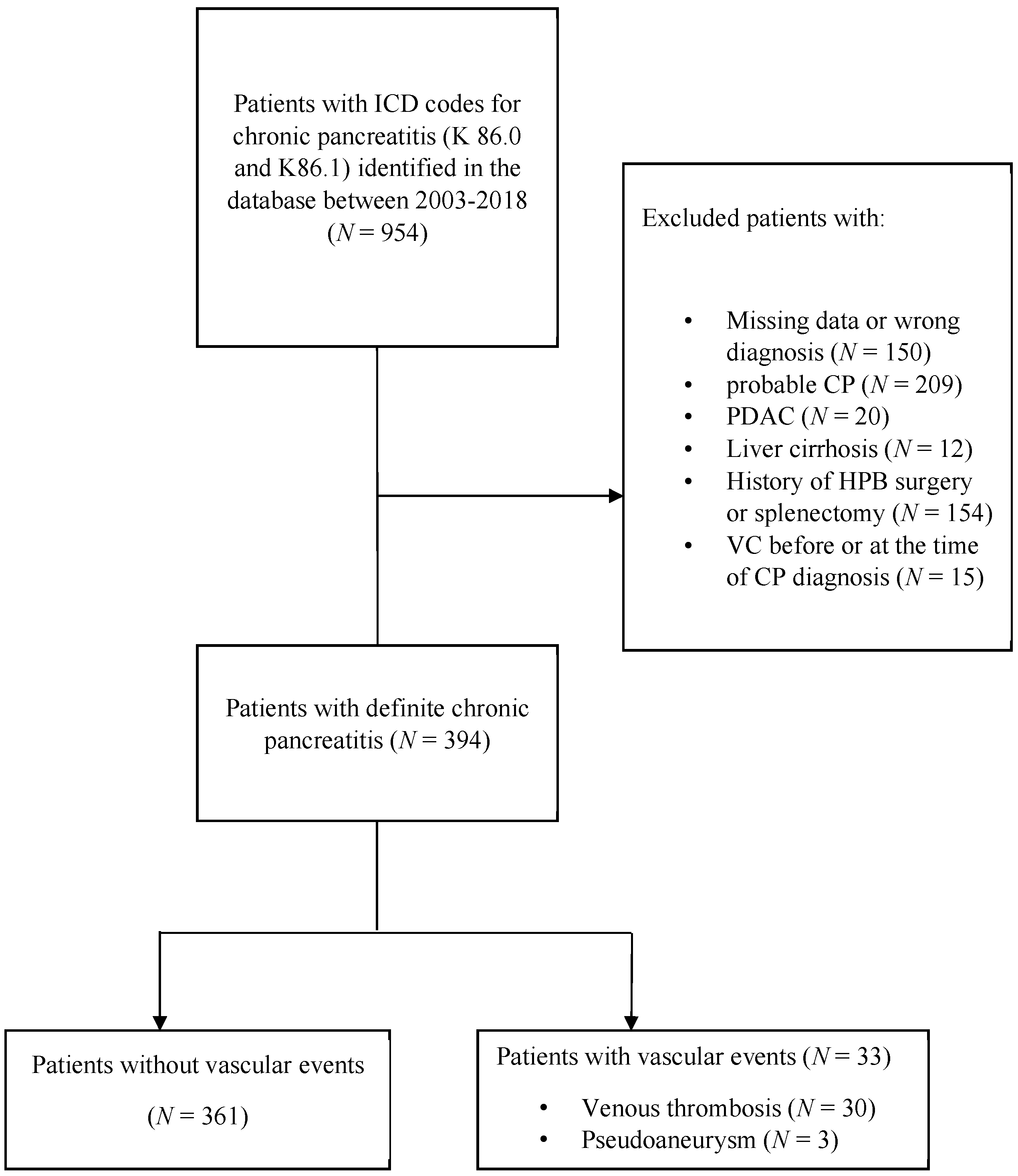
2.1. Patients
2.2. Definitions
2.3. Follow Up
2.4. Antithrombotic Treatment
2.5. Statistics
2.6. Ethics
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Conflicts of Interest
Abbreviations
| AP | acute pancreatitis |
| BMI | body mass index |
| CI | confidence interval |
| CP | chronic pancreatitis |
| IQR | interquartile range |
| LMWH | low-molecular-weight heparin |
| MVT | mesenteric vein thrombosis |
| NOAC | novel oral anticoagulants |
| NSBB | nonselective beta-blockers |
| HR | hazard ratio |
| PA | pseudoaneurysm |
| PEI | pancreatic exocrine insufficiency |
| PVT | portal vein thrombosis |
| SVT | splanchnic vein thrombosis |
| VT | venous thrombosis |
References
- Löhr, J.M.; Dominguez-Munoz, E.; Rosendahl, J.; Besselink, M.; Mayerle, J.; Lerch, M.M.; Hass, S.; Akisik, F.; Kartalis, N.; Iglesias-Garcia, J.; et al. United European Gastroenterology evidence-based guidelines for the diagnosis and therapy of chronic pancreatitis (HaPanEU). United Eur. Gastroenterol. J. 2017, 5, 153–199. [Google Scholar] [CrossRef] [PubMed]
- Xu, W.; Qi, X.; Chen, J.; Su, C.; Guo, X. Prevalence of Splanchnic Vein Thrombosis in Pancreatitis: A Systematic Review and Meta-Analysis of Observational Studies. Gastroenterol. Res. Pract. 2015, 2015, 245460. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Valeriani, E.; Riva, N.; Di Nisio, M.; Ageno, W. Splanchnic Vein Thrombosis: Current Perspectives. Vasc. Health Risk Manag. 2019, 15, 449–461. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sagar, S.; Soundarajan, R.; Gupta, P.; Kumar, M.P.; Samanta, J.; Sharma, V.; Kochhar, R. Efficacy of endovascular embolization of arterial pseudoaneurysms in pancreatitis: A systematic review and meta-analysis. Pancreatology 2021, 21, 46–58. [Google Scholar] [CrossRef] [PubMed]
- Schneider, A.; Löhr, J.M.; Singer, M.V. The M-ANNHEIM classification of chronic pancreatitis: Introduction of a unifying classification system based on a review of previous classifications of the disease. J. Gastroenterol. 2007, 42, 101–119. [Google Scholar] [CrossRef] [PubMed]
- Butler, J.R.; Eckert, G.J.; Zyromski, N.J.; Leonardi, M.J.; Lillemoe, K.D.; Howard, T.J. Natural history of pancreatitis-induced splenic vein thrombosis: A systematic review and meta-analysis of its incidence and rate of gastrointestinal bleeding. HPB 2011, 13, 839–845. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sakorafas, G.H.; Sarr, M.G.; Farley, D.R.; Farnell, M.B. The significance of sinistral portal hypertension complicating chronic pancreatitis. Am. J. Surg. 2000, 179, 129–133. [Google Scholar] [CrossRef]
- Heider, T.R.; Azeem, S.; Galanko, J.A.; Behrns, K.E. The natural history of pancreatitis-induced splenic vein thrombosis. Ann. Surg. 2004, 239, 876–880. [Google Scholar] [CrossRef] [PubMed]
- Anand, A.; Gunjan, D.; Agarwal, S.; Kaushal, K.; Sharma, S.; Gopi, S.; Mohta, S.; Madhusudhan, K.S.; Singh, N.; Saraya, A. Vascular complications of chronic pancreatitis: A tertiary center experience. Pancreatology 2020, 20, 1085–1091. [Google Scholar] [CrossRef]
- Itzchak, Y.; Glickman, M.G. Splenic vein thrombosis in patients with a normal size spleen. Investig. Radiol. 1977, 12, 158–163. [Google Scholar] [CrossRef] [PubMed]
- Köklü, S.; Yüksel, O.; Arhan, M.; Çoban, S.; Başar, O.; Yolcu, O.F.; Uçar, E.; Ibiş, M.; Ertuğrul, I.; Şahin, B. Report of 24 left-sided portal hypertension cases: A single-center prospective cohort study. Dig. Dis. Sci. 2005, 50, 976–982. [Google Scholar] [CrossRef] [PubMed]
- Sankaran, S.J.; Xiao, A.Y.; Wu, L.M.; Windsor, J.A.; Forsmark, C.E.; Petrov, M.S. Frequency of progression from acute to chronic pancreatitis and risk factors: A meta-analysis. Gastroenterology 2015, 149, 1490–1500.e1. [Google Scholar] [CrossRef] [PubMed]
- Agarwal, A.K.; Raj Kumar, K.; Agarwal, S.; Singh, S. Significance of splenic vein thrombosis in chronic pancreatitis. Am. J. Surg. 2008, 196, 149–154. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| PARAMETERS | N (%) |
|---|---|
| Total number of vascular events | 33/394 (8.4) |
| Total VT | 30/394 (7.6) |
| Vessel involved | |
| Isolated PVT | 2/30 (6.7) |
| Isolated SVT | 16/30 (53.3) |
| Isolated MVT | 1/30 (3.3) |
| PVT and SVT | 3/30 (10.0) |
| PVT and MVT | 2/30 (6.7) |
| MVT and SVT | 4/30 (13.3) |
| SVT, PVT and MVT | 2/30 (6.7) |
| Varices on endoscopy | 3/30 (10.0) |
| Variceal location | |
| Esophagus and fundus | 2/3 (66.7) |
| Fundus and other sites | 1/3 (33.3) |
| Variceal treatment | |
| Variceal acute endoscopic treatment | 0/3 (0.0) |
| Variceal bleeding-prophylaxis treatment (NSBB) | 1/3 (33.3) |
| Splenomegaly | 6/30 (20.0) |
| Abdominal collateral vessels | 25/30 (83.3) |
| Venous thrombosis treatment | |
| No treatment | 19/30 (63.3) |
| LMWH | 10/30 (33.3) |
| NOAK | 1/30 (3.3) |
| Clinical manifestation of VT | |
| Incidental finding | 30/30 (100.0) |
| Gastrointestinal bleeding | 0/30 (0.0) |
| Intraabdominal bleeding | 0/30 (0.0) |
| Total Pseudoaneurysm | 3/394 (0.8) |
| Vessel involved | |
| Splenic artery | 2/3 (66.7) |
| Left gastric artery | 1/3 (33.3) |
| Clinical manifestation of pseudoaneurysm | |
| Incidental finding | 3/3 (100.0) |
| Intraabdominal bleeding | 0/3 (0.0) |
| Characteristics | No Complications, n = 361/394 (91.6) | Vascular Complications, n = 33/394 (8.4) | p-Value |
|---|---|---|---|
| Age at time of CP diagnosis, median (IQR) | 57.5 (44–69) | 52 (43.5–54.5) | 0.019 * |
| Age at the time of occurrence of vascular complication, median (IQR) | / | 62.2 (55.1–72) | / |
| Sex male, n (%) | 223/361 (61.8) | 24/33 (72.7) | 0.213 |
| BMI at diagnosis, kg/m2, n (%) | 0.218 | ||
| ≤ 25 | 157/215 (73.0) | 14/23 (60.9) | |
| >25 | 58/215 (27.0) | 9/23 (39.1) | |
| Etiology | |||
| Alcohol, n (%) | 145/361 (40.2) | 27/33 (81.8) | <0.001 * |
| Efferent duct, n (%) | 40/361 (11.1) | 1/33 (3.0) | 0.231 |
| Family history of pancreatic disease, n (%) | 32/294 (10.9) | 1/24 (4.2) | 0.489 |
| Smoking (active or former), n (%) | 210/346 (60.7) | 27/33 (81.8) | 0.017 * |
| Diabetes at diagnosis, n (%) | 91/347 (26.2) | 6/33 (18.2) | 0.311 |
| PEI at diagnosis, n (%) | 144/361 (39.9) | 12/33 (36.4) | 0.921 |
| Calcification at diagnosis, n (%) | 206/342 (60.2) | 19/29 (65.5) | 0.576 |
| AP before CP diagnosis, n (%) | 228/359 (63.5) | 26/32 (81.3) | 0.044 * |
| Pseudocyst, n (%) | 97/361 (26.9) | 27/33 (81.8) | <0.001 * |
| Pseudocyst size, n (%) | 0.435 | ||
| <5cm | 23/44 (52.3) | 14/24 (58.3) | |
| 5–10 cm | 17/44 (38.6) | 6/24 (25.0) | |
| ≥10 cm | 4/44 (9.1) | 4/24 (16.7) |
| Variable | Univariate Analysis | Multivariable Analysis | ||
|---|---|---|---|---|
| HR (95% CIs) | p-Value | HR (95% CIs) | p-Value | |
| Alcohol | 5.07 (2.09–12.30) | <0.001 * | 3.56 (1.40–9.03) | 0.007 * |
| Smoking | 3.12 (1.29–7.56) | 0.012 * | 1.25 (0.49–3.17) | 0.643 |
| Prior AP episode | 1.11 (0.45–2.77) | 0.812 | / | / |
| Pseudocyst | 9.58 (3.90–23.53) | <0.001 * | 8.66 (3.33–22.54) | <0.001 * |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Vujasinovic, M.; Dugic, A.; Nouri, A.; Brismar, T.B.; Baldaque-Silva, F.; Asplund, E.; Rutkowski, W.; Ghorbani, P.; Sparrelid, E.; Hagström, H.; et al. Vascular Complications in Patients with Chronic Pancreatitis. J. Clin. Med. 2021, 10, 3720. https://doi.org/10.3390/jcm10163720
Vujasinovic M, Dugic A, Nouri A, Brismar TB, Baldaque-Silva F, Asplund E, Rutkowski W, Ghorbani P, Sparrelid E, Hagström H, et al. Vascular Complications in Patients with Chronic Pancreatitis. Journal of Clinical Medicine. 2021; 10(16):3720. https://doi.org/10.3390/jcm10163720
Chicago/Turabian StyleVujasinovic, Miroslav, Ana Dugic, Amar Nouri, Torkel B Brismar, Francisco Baldaque-Silva, Ebba Asplund, Wiktor Rutkowski, Poya Ghorbani, Ernesto Sparrelid, Hannes Hagström, and et al. 2021. "Vascular Complications in Patients with Chronic Pancreatitis" Journal of Clinical Medicine 10, no. 16: 3720. https://doi.org/10.3390/jcm10163720