Family Support, Multidimensional Health, and Living Satisfaction among the Elderly: A Case from Shaanxi Province, China



Abstract
:1. Introduction
2. Literature Review and Conceptual Framework
2.1. Family Support and Living Satisfaction
2.2. Multidimensional Health and Living Satisfaction
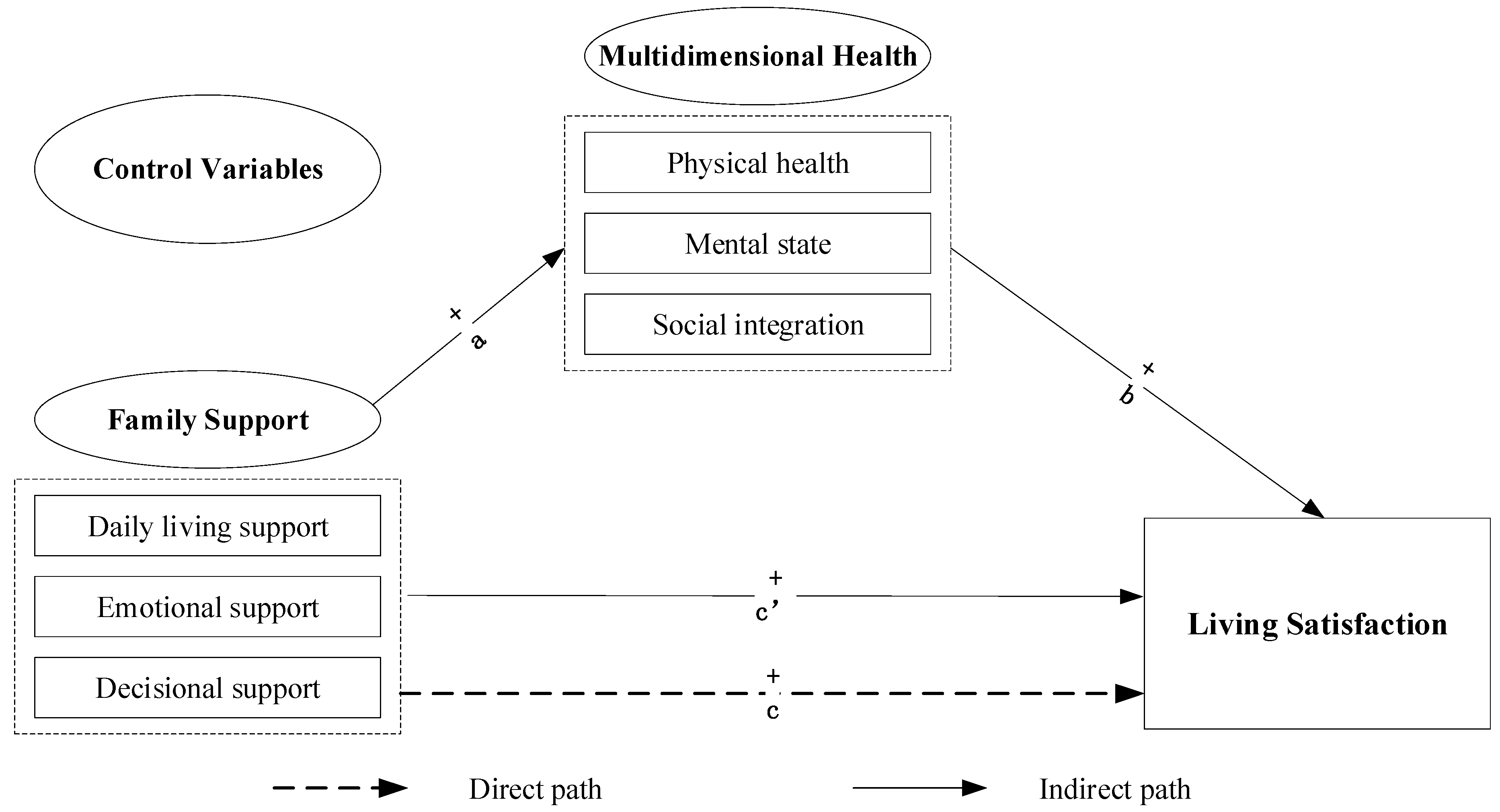
2.3. Family Support, Multidimensional Health, and Living Satisfaction
3. Materials and Methods
3.1. Study Design and Data Collection
3.1.1. Study Design and Sampling
3.1.2. Data Collection
3.2. Measurements
3.2.1. Dependent Variable: Living Satisfaction
3.2.2. Independent Variable: Family Support
3.2.3. Mediators: Multidimensional Health
3.2.4. Control Variables
3.3. Statistical Analysis
4. Results
4.1. Descriptive Statistics
4.2. Multivariate Linear Regression Analysis
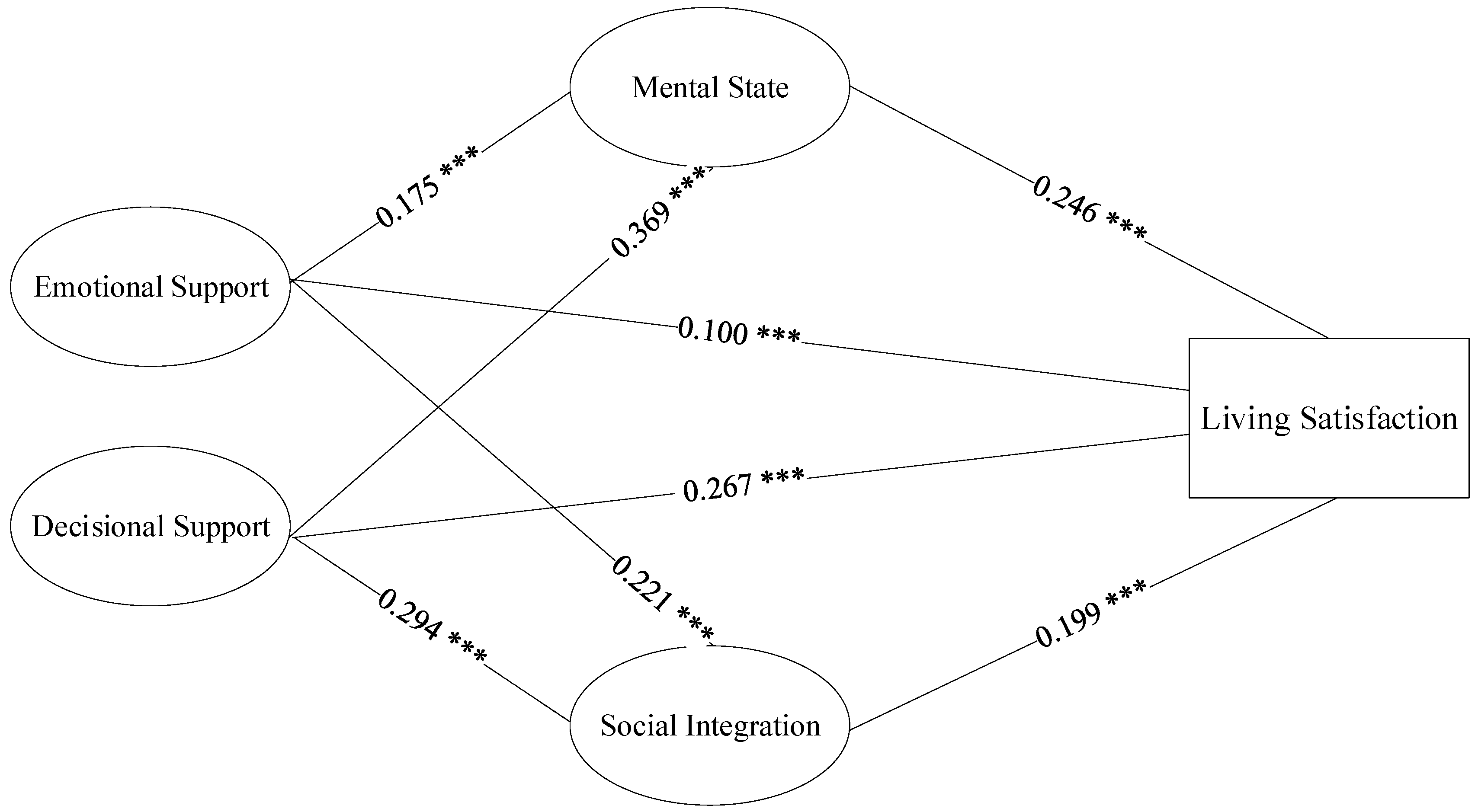
4.3. Mediation of Multidimensional Health between Family Support and Elderly Individuals’ Living Satisfaction
5. Discussion
6. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- National Bureau of Statistics. Population Age Structure in China 2019. Available online: https://data.stats.gov.cn/easyquery.htm?cn=C01 (accessed on 30 September 2020).
- Fang, E.F.; Scheibye-Knudsen, M.; Jahn, H.J.; Li, J.; Ling, L.; Guo, H.W.; Zhu, X.Q.; Preedy, V.; Lu, H.M.; Bohr, V.A.; et al. A research agenda for aging in China in the 21st century. Ageing Res. Rev. 2015, 24, 197–205. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Diener, E.; Emmons, R.A.; Larsen, R.J.; Griffin, S. The satisfaction with life scale. J. Personal. Assess. 1985, 49, 71–75. [Google Scholar] [CrossRef] [PubMed]
- Caprara, G.V.; Steca, P.; Alessandri, G.; Abela, J.R.; McWhinnie, C.M. Positive orientation: Explorations on what is common to life satisfaction, self-esteem, and optimism. Epidemiol. Psychiatr. Sci. 2010, 19, 63–71. [Google Scholar] [CrossRef] [PubMed]
- Kanning, M.; Schlicht, W. A bio-psycho-social model of successful aging as shown through the variable of physical activity. Eur. Rev. Aging Phys. Act. 2008, 5, 79–87. [Google Scholar] [CrossRef] [Green Version]
- Chou, K.L.; Chi, I. Determinants of life satisfaction in Hong Kong Chinese elderly: A longitudinal study. Aging Ment. Health 1999, 3, 328–335. [Google Scholar] [CrossRef]
- Grundy, E.; Henretta, J.C. Between elderly parents and adult children: A new look at the intergenerational care provided by the ‘sandwich generation’. Ageing Soc. 2006, 26, 707–722. [Google Scholar] [CrossRef] [Green Version]
- Merz, E.M.; Consedine, N.S. The association of family support and wellbeing in later life depends on adult attachment style. Attach. Hum. Dev. 2009, 11, 203–221. [Google Scholar] [CrossRef]
- Zhang, Y.; Goza, F.W. Who will care for the elderly in China? A review of the problems caused by China’s one-child policy and their potential solutions. J. Aging Stud. 2006, 20, 151–164. [Google Scholar] [CrossRef]
- Giles, J.; Wang, D.; Zhao, C. Can China’s rural elderly count on support from adult children? Implications of rural-to-urban migration. J. Popul. Ageing 2010, 3, 183–204. [Google Scholar] [CrossRef] [Green Version]
- Ng, K.H. Review essay: Prospects for old-age income security in Hong Kong and Singapore. J. Popul. Ageing 2011, 4, 271–293. [Google Scholar] [CrossRef]
- Heffner, A.L.; Antaramian, S.P. The role of life satisfaction in predicting student engagement and achievement. J. Happiness Stud. 2016, 17, 1681–1701. [Google Scholar] [CrossRef]
- Gouveia, E.R.; Gouveia, B.R.; Ihle, A.; Kliegel, M.; Maia, J.A.; Badia, S.B.; Freitas, D.L. Correlates of health-related quality of life in young-old and old-old community-dwelling older adults. Qual. Life Res. 2017, 26, 1561–1569. [Google Scholar] [CrossRef] [PubMed]
- Van Tilburg, T. Losing and gaining in old age: Changes in personal network size and social support in a four-year longitudinal study. J. Gerontol. Ser. B Psychol. Sci. Soc. Sci. 1998, 53, 313–323. [Google Scholar] [CrossRef] [PubMed]
- Merz, E.M.; Huxhold, O. Wellbeing depends on social relationship characteristics: Comparing different types and providers of support to older adults. Ageing Soc. 2010, 30, 843–857. [Google Scholar] [CrossRef]
- Cheng, S.T.; Chan, A.C. Filial piety and psychological well-being in well older Chinese. J. Gerontol. Psychol. Sci. 2006, 61, 262–269. [Google Scholar] [CrossRef] [PubMed]
- Zulfitri, R.; Sabrian, F. Sociodemographic characteristics and psychosocial wellbeing of elderly with chronic illnesses who live with family at home. Enferm. Clin. 2019, 29, 34–37. [Google Scholar] [CrossRef] [PubMed]
- Uchino, B.N.; Cacioppo, J.T.; Kiecolt-Glaser, J.K. The relationship between social support and physiological processes: A review with emphasis on underlying mechanisms and implications for health. Psychol. Bull. 1996, 119, 488–531. [Google Scholar] [CrossRef]
- Zunzunegui, M.V.; Beland, F.; Otero, A. Support from children, living arrangements, self-rated health and depressive symptoms of older people in Spain. Int. J. Epidemiol. 2001, 30, 1090–1099. [Google Scholar] [CrossRef] [Green Version]
- Chen, J.; Jordan, L.P. Intergenerational support and life satisfaction of young-, old-and oldest-old adults in China. Aging Ment. Health 2016, 22, 412–420. [Google Scholar] [CrossRef]
- Zhang, A.Y.; Yu, L.C. Life satisfaction among Chinese elderly in Beijing. J. Cross Cult. Gerontol. 1998, 13, 109–125. [Google Scholar] [CrossRef]
- Peng, C.H.; Kwok, C.L.; Law, Y.W.; Yip, P.S.; Cheng, Q.J. Intergenerational support, satisfaction with parent–child relationship and elderly parents’ life satisfaction in Hong Kong. Aging Ment. Health 2019, 23, 428–438. [Google Scholar] [CrossRef] [PubMed]
- Antonucci, T.C.; Akiyama, H. Social network, support, and integration. In Encyclopedia of Gerontology, 2nd ed.; Birren, J.E., Ed.; Academic Press: San Diego, CA, USA, 2007; Volume 2, pp. 531–541. [Google Scholar]
- de Guzman, A.B.; Golosinda, D.A.; Gonzales, C.P. What shapes the self-esteem of elderly Filipinos working beyond the retirement age? A structural equation model (SEM). Educ. Gerontol. 2019, 45, 34–44. [Google Scholar] [CrossRef]
- Dumitrache, C.G.; Windle, G.; Herrera, R.R. Do Social Resources Explain the Relationship between Optimism and Life Satisfaction in Community-Dwelling Older People? Testing a Multiple Mediation Model. J. Happiness Stud. 2015, 16, 633–654. [Google Scholar] [CrossRef]
- Pinto, J.M.; Fontaine, A.M.; Neri, A.L. The influence of physical and mental health on life satisfaction is mediated by self-rated health: A study with Brazilian elderly. Arch. Gerontol. Geriatr. 2016, 65, 104–110. [Google Scholar] [CrossRef]
- Pinto, J.M.; Neri, A.L. Factors associated with low life satisfaction in community-dwelling elderly: FIBRA Study. Cad. Saude Publica 2013, 29, 2447–2458. [Google Scholar] [CrossRef] [Green Version]
- Celik, S.S.; Celik, Y.; Hikmet, N.; Khan, M.M. Factors affecting life satisfaction of older adults in turkey. Int. J. Aging Hum. Dev. 2017, 87, 392–414. [Google Scholar] [CrossRef]
- Lopez-Ortega, M.; Torres-Castro, S.; Rosas-Carrasco, O. Psychometric properties of the Satisfaction with Life Scale (SWLS): Secondary analysis of the Mexican health and aging study. Health Qual. Life Outcomes 2017, 14, 170. [Google Scholar] [CrossRef] [Green Version]
- Ng, S.T.; Tey, N.P.; Asadullah, M.N. What matters for life satisfaction among the oldest-old? Evidence from China. PLoS ONE 2017, 12, e0171799. [Google Scholar] [CrossRef] [Green Version]
- Camacho, D.; Lee, Y.; Bhattacharya, A.; Vargas, L.X.; Kimberly, L.; Lukens, E. High life satisfaction: Exploring the role of health, social integration and perceived safety among Mexican midlife and older adults. J. Gerontol. Soc. Work 2019, 62, 521–542. [Google Scholar] [CrossRef]
- Breslow, L. Quantitative approach to World Health Organization definition of health—Physical, mental and social well-being. Int. J. Epidemiol. 1972, 1, 347–355. [Google Scholar] [CrossRef]
- Russell, R.D. Social health: An attempt to clarify this dimension of well-being. Int. J. Health Educ. 1973, 16, 74–82. [Google Scholar]
- Keyes, C.L. Social Well-Being. Soc. Psychol. Q. 1998, 61, 121–140. [Google Scholar] [CrossRef]
- Calvo, R.; Carr, D.C.; Matz-Costa, C. Another paradox? The life satisfaction of older Hispanic immigrants in the United States. J. Aging Health 2017, 29, 3–24. [Google Scholar] [CrossRef] [PubMed]
- Bao, C.; Chen, K. Association between subjective well-being and health status among the elderly in China: The influences of social support and social adjustment. Value Health 2016, 19, A907. [Google Scholar] [CrossRef]
- Zhang, Z.; Zhang, J.X. Social participation and subjective well-being among retirees in China. Soc. Indic. Res. 2015, 123, 143–160. [Google Scholar] [CrossRef]
- You, X.Y.; Zhang, Y.L.; Zeng, J.F.; Wang, C.J.; Sun, H.P.; Ma, Q.H.; Ma, Y.N.; Xu, Y. Disparity of the Chinese elderly’s health-related quality of life between urban and rural areas: A mediation analysis. BMJ Open 2019, 9, e024080. [Google Scholar] [CrossRef]
- Choi, N.G.; Wodarski, J.S. The relationship between social support and health status of elderly people: Does social support slow down physical and functional deterioration? Soc. Work Res. 1996, 20, 52–63. [Google Scholar]
- Lyons, A. Social support and the mental health of older gay men: Findings from a national community-based survey. Res. Aging 2016, 38, 234–253. [Google Scholar] [CrossRef]
- Koelmel, E.; Hughes, A.J.; Alschuler, K.N.; Ehde, D.M. Resilience mediates the longitudinal relationships between social support and mental health outcomes in multiple sclerosis. Arch. Phys. Med. Rehabil. 2017, 98, 1139–1148. [Google Scholar] [CrossRef]
- Bai, Y.L.; Bian, F.; Zhang, L.X.; Cao, Y.M. The impact of social support on the health of the rural elderly in China. Int. J. Environ. Res. Public Health 2020, 17, 2004. [Google Scholar] [CrossRef] [Green Version]
- Loffler, C.; Kaduszkiewicz, H.; Stolzenbach, C.; Streich, W.; Fuchs, A.; van den Bussche, H.; Stolper, F.; Altiner, A. Coping with multimorbidity in old age—A qualitative study. BMC Fam. Pract. 2012, 13, 45. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- George, L.K. Still happy after all these years: Research frontiers on subjective well-being in later life. J. Gerontol. Ser. B Psychol. Sci. Soc. Sci. 2010, 65, 331–339. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hsu, C.Y.; Chang, S.S.; Yip, P. Individual-, household-and neighbourhood- level characteristics associated with life satisfaction: A multilevel analysis of a population-based sample from Hong Kong. Urban Stud. 2017, 54, 3700–3717. [Google Scholar] [CrossRef]
- Lorraine, P.J.; Hammock, R.L.; Blanton, J.M. Predictors of self-rated health status among Texas residents. Prev. Chronic Dis. 2005, 2, A12. [Google Scholar] [PubMed]
- Diseth, A.; Kobbeltvedt, T. A mediation analysis of achievement motives, goals, learning strategies, and academic achievement. Br. J. Educ. Psychol. 2010, 80, 671–687. [Google Scholar] [CrossRef] [PubMed]
- Hayes, A.F. Beyond Baron and Kenny: Statistical mediation analysis in the new millennium. Commun. Monogr. 2009, 76, 408–420. [Google Scholar] [CrossRef]
- Preacher, K.J.; Hayes, A.F. Asymptotic and resampling strategies for assessing and comparing indirect effects in multiple mediator models. Behav. Res. Methods 2008, 40, 879–891. [Google Scholar] [CrossRef]
- Takagi, E.; Saito, Y. A longitudinal analysis of the impact of family support on the morale of older parents in Japan: Does the parent’s normative belief in filial responsibilities make a difference? Ageing Soc. 2013, 33, 1053–1976. [Google Scholar] [CrossRef] [Green Version]
- Guo, M.; Aranda, M.P.; Silverstein, M. The impact of out-migration on the inter-generational support and psychological wellbeing of older adults in rural China. Ageing Soc. 2009, 29, 1085–1104. [Google Scholar] [CrossRef]
- Fingerman, K.L.; Sechrist, J.; Birditt, K. Changing views on intergenerational ties. Gerontology 2012, 59, 64–70. [Google Scholar] [CrossRef] [Green Version]
- Silverstein, M.; Chen, X.; Heller, K. Too much of a good thing? Intergenerational social support and the psychological well-being of older parents. J. Marriage Fam. 1996, 58, 970–982. [Google Scholar] [CrossRef]
- Seeman, T.E.; Berkman, L.F. Structural Characteristics of Social Networks and Their Relationship with Social Support in the Elderly: Who Provides Support. Soc. Sci. Med. 1988, 26, 737–749. [Google Scholar] [CrossRef]
- Ng, A.C.; Phillips, D.R.; Lee, W.K. Persistence and challenges to filial piety and informal support of older persons in a modern Chinese society: A case study in Tuen Mun, Hong Kong. J. Aging Stud. 2002, 16, 135–153. [Google Scholar] [CrossRef]
- Nguyen, A.W.; Chatters, L.M.; Taylor, R.J.; Mouzon, D.M. Social Support from Family and Friends and Subjective Well-Being of Older African Americans. J. Happiness Stud. 2016, 17, 959–979. [Google Scholar] [CrossRef] [PubMed]
- Abruquah, L.A.; Yin, X.X.; Ding, Y. Old age support in urban China: The role of pension schemes, self-Support ability and intergenerational assistance. Int. J. Environ. Res. Public Health 2019, 16, 1918. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lou, V.W. Life satisfaction of older adults in Hong Kong: The role of social support from grandchildren. Soc. Indic. Res. 2010, 95, 377–391. [Google Scholar] [CrossRef]
- Lum, T.Y.; Yan, E.C.; Ho, A.H.; Shum, M.H.; Wong, G.H.; Lau, M.M.; Wang, J. Measuring filial piety in the 21st century: Development, factor structure, and reliability of the 10-Item contemporary filial piety scale. J. Appl. Gerontol. 2016, 35, 1235–1247. [Google Scholar] [CrossRef]
- Carstensen, L.L. The influence of a sense of time on human development. Science 2006, 312, 1913–1915. [Google Scholar] [CrossRef] [Green Version]
- Poulin, J.; Deng, R.; Ingersoll, T.S. Perceived family and friend support and the psychological well-being of American and Chinese elderly persons. J. Cross Cult. Gerontol. 2012, 27, 305–317. [Google Scholar] [CrossRef]
- Krause, N.; Borawski-Clark, E. Clarifying the functions of social support in later life. Res. Aging 1994, 16, 251–279. [Google Scholar] [CrossRef]
- Streib, G.F. Growing old: The Process of Disengagement—Cumming, E., Henry, W.E. Am. Sociol. Rev. 1963, 27, 561–562. [Google Scholar] [CrossRef]
- Wang, J.Y.; Xue, J.; Jiang, Y.X.; Zhu, T.F.; Chen, S.L. Mediating effects of depressive symptoms on social support and quality of life among rural older Chinese. Health Qual. Life Outcomes 2020, 18, 285–299. [Google Scholar] [CrossRef] [PubMed]
- Jang, J.M.; Park, J.I.; Oh, K.Y.; Lee, K.H.; Kim, M.S.; Yoon, M.S.; Ko, S.H.; Cho, H.C.; Chung, Y.C. Predictors of suicidal ideation in a community sample: Roles of anger, self-esteem, and depression. Psychiatry Res. 2014, 216, 74–81. [Google Scholar] [CrossRef] [PubMed]
- Li, C.C.; Chen, M.L.; Chang, T.C.; Chou, H.H.; Chen, M.Y. Social support buffers the effect of self-esteem on quality of life of early-stage cervical cancer survivors in Taiwan. Eur. J. Oncol. Nurs. 2015, 19, 486–494. [Google Scholar] [CrossRef]
- Kim, G.H.; Woo, J.Y. The Effect of Family Support and Internal-External Control on Elderly People Social Participation. Korean J. Rehabil. Psychol. 2012, 19, 317–335. [Google Scholar]
- Bohm, A.W.; Mielke, G.I.; da Cruz, M.F.; Ramires, V.V.; Wehrmeister, F.C. Social Support and Leisure-Time Physical Activity Among the Elderly: A Population-Based Study. J. Phys. Act. Health 2016, 13, 599–605. [Google Scholar] [CrossRef]
- Kim, B.J.; Chen, L.; Lee, Y.; Xu, L. Quality of life of elderly Chinese immigrants: Focusing on living arrangements and social capital. Educ. Gerontol. 2019, 45, 377–389. [Google Scholar] [CrossRef]
- Yue, Z.; Qin, X.G. The trajectory of rural elders’ attitudes toward aging: An empirical study based on the framework of active aging. South China Popul. 2020, 35, 68–80. [Google Scholar]
- Lu, N.; Spencer, M.; Sun, Q.; Lou, V.W. Family social capital and life satisfaction among older adults living alone in urban China: The moderating role of functional health. Aging Ment. Health 2020. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| Variable | Code/Definition |
|---|---|
| Age | Continuous variable |
| Gender | 0 = Male; 1 = Female |
| Marital status | 0 = Non-single; 1 = Single (contains unmarried, divorced, and widowed) |
| Household income | Categorical variable (<¥10,000; ¥10,000–¥50,000; ¥50,000–¥100,000; ¥100,000–¥200,000; >¥200,000) |
| Hukou location | 0 = Urban; 1 = Rural |
| Education level | Categorical variable (primary school or lower; junior middle school; senior middle school or higher) |
| Living mode | 0 = Living in the home/community; 1 = Living in an old age care institution |
| Having any ADL limitation | 0 = Yes; 1 = No |
| Having any chronic disease | 0 = Yes; 1 = No |
| Health insurance | 0 = Yes; 1 = No |
| Old age insurance | 0 = Yes; 1 = No |
| Variable | Frequency (n)/Mean | Percentage (%)/SD | |
|---|---|---|---|
| Age | (Mean, SD) | 72.19 | 8.36 |
| Gender | Male | 402 | 42.86 |
| Female | 536 | 57.14 | |
| Marital status | Non-single | 406 | 43.28 |
| Single | 532 | 56.72 | |
| Household income | <¥10,000 | 132 | 14.07 |
| ¥10,000–¥50,000 | 200 | 21.32 | |
| ¥50,000–¥100,000 | 99 | 10.55 | |
| ¥100,000–¥200,000 | 319 | 34.01 | |
| >¥200,000 | 188 | 20.04 | |
| Hukou location | Urban | 514 | 54.80 |
| Rural | 424 | 45.20 | |
| Education level | Primary school or lower | 447 | 47.65 |
| Junior middle school | 247 | 26.33 | |
| Senior middle school or higher | 244 | 26.01 | |
| Living mode | Living in the home/community | 687 | 73.24 |
| Living in an old age care institution | 251 | 26.76 | |
| Having any ADL limitation | Yes | 76 | 8.10 |
| Having any chronic disease | Yes | 529 | 56.40 |
| Health insurance | Yes | 914 | 97.44 |
| Old-age insurance | Yes | 887 | 94.56 |
| Variable | Minimum | Maximum | Mean | SD | |
|---|---|---|---|---|---|
| Before data normalization | Living satisfaction | 7 | 25 | 19.061 | 3.053 |
| Family support | |||||
| Daily living support | 1 | 5 | 3.472 | 1.462 | |
| Emotional support | 1 | 5 | 4.095 | 1.096 | |
| Decisional support | 1 | 5 | 4.259 | 0.731 | |
| Multidimensional health | |||||
| Self-rated physical health | 1 | 5 | 3.383 | 1.095 | |
| Mental state | 1 | 5 | 4.168 | 0.939 | |
| Social integration | 3 | 15 | 12.978 | 2.029 | |
| After data normalization | Living satisfaction | 0 | 1 | 0.670 | 0.169 |
| Family support | |||||
| Daily living support | 0 | 1 | 0.618 | 0.365 | |
| Emotional support | 0 | 1 | 0.774 | 0.274 | |
| Decisional support | 0 | 1 | 0.815 | 0.183 | |
| Multidimensional health | |||||
| Self-rated physical health | 0 | 1 | 0.596 | 0.274 | |
| Mental state | 0 | 1 | 0.792 | 0.235 | |
| Social integration | 0 | 1 | 0.817 | 0.184 | |
| Variable | Model 1 β (SE) | Model 2 β (SE) | Model 3 β (SE) |
|---|---|---|---|
| Age | −0.011 (0.024) | −0.022 (0.022) | 0.005 (0.019) |
| Gender | 0.003 (0.010) | −0.005 (0.009) | 0.003 (0.008) |
| Marital status | 0.021 (0.012) | 0.006 (0.011) | 0.004 (0.009) |
| Household income | |||
| ¥10,000–¥50,000 | 0.067 (0.016) *** | 0.044 (0.015) ** | 0.023 (0.013) |
| ¥50,000–¥100,000 | 0.116 (0.020) *** | 0.087 (0.018) *** | 0.056 (0.016) *** |
| ¥100,000–¥200,000 | 0.160 (0.015) *** | 0.124 (0.015) *** | 0.080 (0.013) *** |
| >¥200,000 | 0.228 (0.017) *** | 0.174 (0.017) *** | 0.125 (0.015) *** |
| Hukou location | 0.013 (0.011) | 0.028 (0.010) ** | 0.021 (0.008) * |
| Education level | |||
| Junior middle school | 0.033 (0.013) * | 0.026 (0.012) * | 0.020 (0.010) |
| Senior middle school or higher | 0.034 (0.013) * | 0.025 (0.012) * | 0.023 (0.010) * |
| Living mode | 0.046 (0.014) ** | 0.060 (0.013) *** | 0.045 (0.011) *** |
| Having any ADL limitation | 0.109 (0.019) *** | 0.080 (0.017) *** | 0.018 (0.015) |
| Having any chronic disease | 0.045 (0.010) *** | 0.037 (0.009) *** | 0.012 (0.008) |
| Health insurance | 0.035 (0.022) | 0.032 (0.029) | 0.029 (0.024) |
| Old age insurance | 0.034 (0.045) | 0.018 (0.020) | 0.013 (0.017) |
| Family support | |||
| Daily living support | 0.017 (0.014) | 0.012 (0.012) | |
| Emotional support | 0.101 (0.019) *** | 0.010 (0.016) | |
| Decisional support | 0.263 (0.027) *** | 0.114 (0.024) *** | |
| Multidimensional health | |||
| Self-rated physical health | 0.073 (0.016) *** | ||
| Mental state | 0.246 (0.021) *** | ||
| Social integration | 0.199 (0.026) *** | ||
| Observation | 938 | 938 | 938 |
| Adjusted R-square | 0.264 | 0.390 | 0.569 |
| Variable | Model 1 β (SE) | Model 2 β (SE) | Model 3 β (SE) | Model 4 β (SE) | Model 5 β (SE) |
|---|---|---|---|---|---|
| Y: Living Satisfaction | M1: Self-Rated Physical Health | M2: Mental State | M3: Social Integration | Y: Living Satisfaction | |
| Emotional support | 0.100 (0.019) *** | 0.046 (0.034) | 0.175 (0.027) *** | 0.221 (0.022) *** | 0.010 (0.016) |
| Decisional support | 0.267 (0.027) *** | 0.009 (0.049) | 0.369 (0.039) *** | 0.294 (0.032) *** | 0.118 (0.024) *** |
| Self-rated physical health | 0.076 (0.015) *** | ||||
| Mental state | 0.246 (0.021) *** | ||||
| Social integration | 0.199 (0.026) *** | ||||
| CV | Yes | Yes | Yes | Yes | Yes |
| Observation | 938 | 938 | 938 | 938 | 938 |
| Adjusted R-squared | 0.389 | 0.218 | 0.305 | 0.276 | 0.569 |
| Mediator | Emotional Support–Health–Living Satisfaction | Decisional Support–Health–Living Satisfaction | ||||
|---|---|---|---|---|---|---|
| Indirect Effect | BCa 95% CI | Indirect Effect | BCa 95% CI | |||
| β (SE) | Lower | Upper | β (SE) | Lower | Upper | |
| Multidimensional health | ||||||
| Self-rated physical health | 0.003 (0.003) | −0.001 | 0.011 | 0.001 (0.004) | −0.007 | 0.009 |
| Mental state | 0.043 (0.009) *** | 0.026 | 0.063 | 0.091 (0.014) *** | 0.065 | 0.121 |
| Social integration | 0.044 (0.009) *** | 0.029 | 0.063 | 0.058 (0.011) *** | 0.038 | 0.083 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Wang, L.; Yang, L.; Di, X.; Dai, X. Family Support, Multidimensional Health, and Living Satisfaction among the Elderly: A Case from Shaanxi Province, China. Int. J. Environ. Res. Public Health 2020, 17, 8434. https://doi.org/10.3390/ijerph17228434
Wang L, Yang L, Di X, Dai X. Family Support, Multidimensional Health, and Living Satisfaction among the Elderly: A Case from Shaanxi Province, China. International Journal of Environmental Research and Public Health. 2020; 17(22):8434. https://doi.org/10.3390/ijerph17228434
Chicago/Turabian StyleWang, Lijian, Liu Yang, Xiaodong Di, and Xiuliang Dai. 2020. "Family Support, Multidimensional Health, and Living Satisfaction among the Elderly: A Case from Shaanxi Province, China" International Journal of Environmental Research and Public Health 17, no. 22: 8434. https://doi.org/10.3390/ijerph17228434