
25-Hydroxyvitamin D Serum Levels Linked to Single Nucleotide Polymorphisms (SNPs) (rs2228570, rs2282679, rs10741657) in Skeletal Muscle Aging in Institutionalized Elderly Men Not Supplemented with Vitamin D

 , ,
, ,
Abstract
:1. Introduction
2. Results
2.1. Sample and Lifestyle Characteristics
2.2. Physical Fitness Condition
2.3. Clinical Description
2.4. 25-OH/D Level
2.5. Sarcopenia Degrees
2.6. Comparisons between Single Nucleotide Polymorphisms vs. 25-Hydroxy Vitamin D
2.7. Correlations between the Concentration of 25-Hydroxy Vitamin D and Single Nucleotide Polymorphisms
2.8. Single Nucleotide Polymorphisms Associated with 25-Hydroxy Vitamin D Concentration
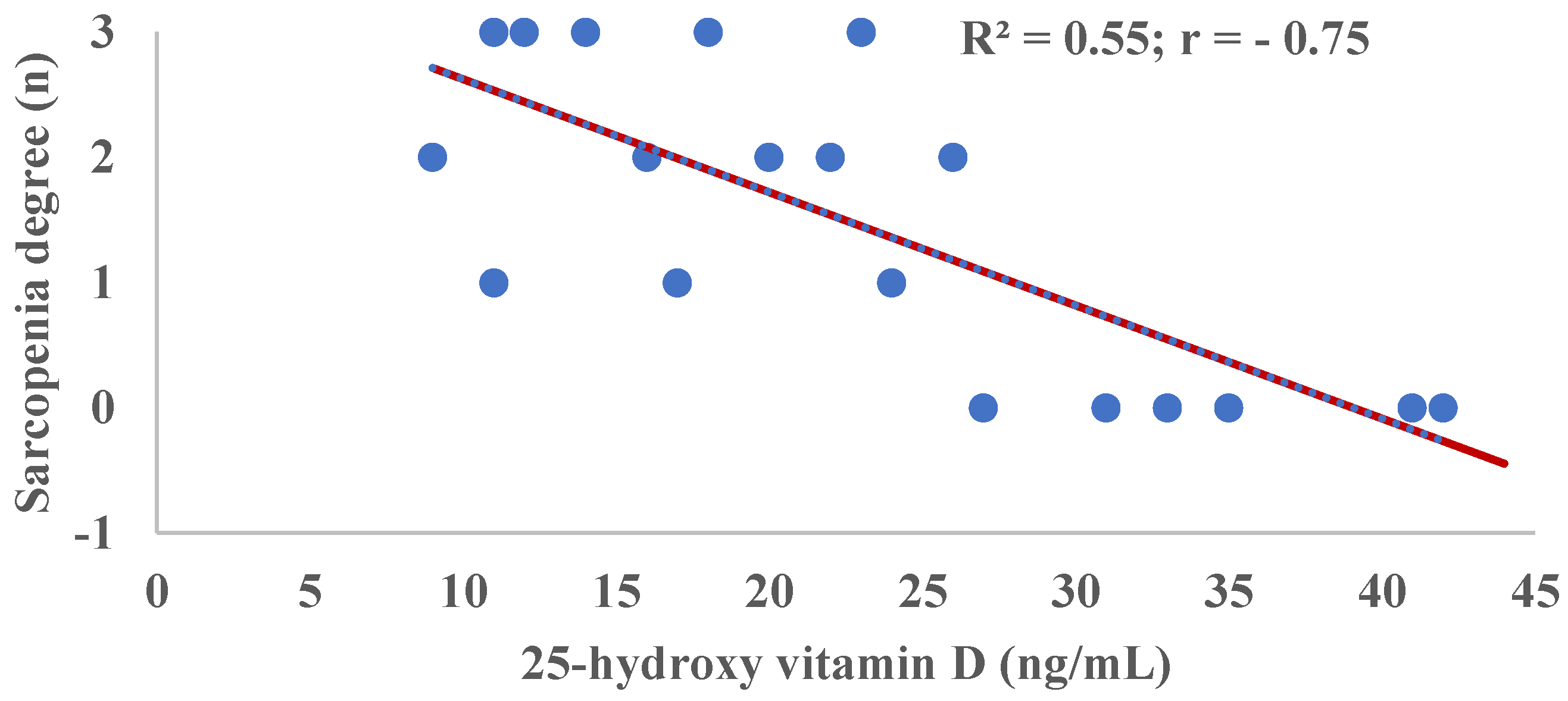
2.9. Correlation of Sarcopenia Degree and 25-Hydroxy Vitamin D (25-OH/D) Concentration
3. Discussion
Limitations and Strengths
4. Material and Methods
4.1. Study Design
4.2. Data Collection
4.2.1. Sociodemographic and Lifestyle
4.2.2. Physical Fitness
4.2.3. Clinical Characteristics
4.3. 25-OH/D Level Determination in Peripheral Blood
4.4. Sarcopenia Degree
4.5. Single Nucleotide Polymorphism (SNPs) Selection
4.6. DNA Isolation and Genotyping
4.7. Data Management and Statistical Analysis
4.8. Ethical Considerations
5. Conclusions
6. Applications
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Cruz-Jentoft, A.J.; Sayer, A.A. Sarcopenia. Lancet 2019, 393, 2636–2646. [Google Scholar] [CrossRef]
- Rosenberg, I.H. Sarcopenia: Origins and Clinical Relevance. Clin. Geriatr. Med. 2011, 27, 337–339. [Google Scholar] [CrossRef] [PubMed]
- Bhasin, S.; Travison, T.G.; Manini, T.M.; Patel, S.; Pencina, C.M.; Fielding, R.A.; Magaziner, J.M.; Newman, A.B.; Keil, D.P.; Cooper, C.; et al. Sarcopenia Definition: The Position Statements of the Sarcopenia Definition and Outcomes Consortium. J Am Geriatr Soc. 2020, 68, 1410–1418. [Google Scholar] [CrossRef] [PubMed]
- Bendik, I.; Friedel, A.; Roos, F.F.; Weber, P.; Eggersdorfer, M. Vitamin D: A critical and essential micronutrient for human health. Front Physiol. 2014, 5, 248. [Google Scholar] [CrossRef] [PubMed]
- Dzik, K.P.; Kaczor, J.J. Mechanisms of vitamin D on skeletal muscle function: Oxidative stress, energy metabolism and anabolic state. Eur. J. Appl. Physiol. 2019, 119, 825–839. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ceglia, L. Vitamin D and skeletal muscle tissue and function. Mol. Asp. Med. 2008, 29, 407–414. [Google Scholar] [CrossRef]
- Wintermeyer, E.; Ihle, C.; Ehnert, S.; Stöckle, U.; Ochs, G.; de Zwart, P.; Flesch, I.; Bahrs, C.; Nussler, A.K. Crucial Role of Vitamin D in the Musculoskeletal System. Nutrients 2016, 8, 319. [Google Scholar] [CrossRef] [Green Version]
- Houston, D.K.; Tooze, J.A.; Neiberg, R.H.; Hausman, D.B.; Johnson, M.A.; Cauley, J.A.; Bauer, D.C.; Cawthon, P.M.; Shea, M.K.; Schwartz, G.G.; et al. 25-hydroxyvitamin D status and change in physical performance and strength in older adults: The Health, Aging, and Body Composition Study. Am. J. Epidemiol. 2012, 176, 1025–1034. [Google Scholar] [CrossRef]
- Palacios, C.; Gonzalez, L. Is vitamin D deficiency a major global public health problem? J. Steroid. Biochem. Mol. Biol. 2014, 144, 138–145. [Google Scholar] [CrossRef] [Green Version]
- Sousa, S.E.S.; Sales, M.C.; Araújo, J.R.T.; Sena-Evangelista, K.C.M.; Lima, K.C.; Pedrosa, L.F.C. High Prevalence of Hypovitaminosis D in Institutionalized Elderly Individuals is Associated with Summer in a Region with High Ultraviolet Radiation Levels. Nutrients 2019, 11, 1516. [Google Scholar] [CrossRef]
- Remelli, F.; Vitali, A.; Zurlo, A.; Volpato, S. Vitamin D Deficiency and Sarcopenia in Older Persons. Nutrients. 2019, 11, 2861. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gallagher, J.C. Vitamin D and Aging. Endocrinol. Metab. Clin. 2013, 42, 319–332. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wang, T.J.; Zhang, F.; Richards, J.B.; Kestenbaum, B.; van Meurs, J.B.; Berry, D.; Kiel, D.P.; Streeten, E.A.; Ohlsson, C.; Koller, D.L.; et al. Common genetic determinants of vitamin D insufficiency: A genome-wide association study. Lancet 2010, 376, 180–188. [Google Scholar] [CrossRef] [Green Version]
- Shea, M.K.; Benjamin, E.J.; Dupuis, J.; Massaro, J.M.; Jacques, P.F.; D’Agostino, R.B., Sr.; Ordovas, J.M.; O’Donnell, C.J.; Dawson-Hughes, B.; Vasan, R.S.; et al. Genetic and non-genetic correlates of vitamins K and D. Eur. J. Clin. Nutr. 2009, 63, 458–464. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Levin, G.P.; Robinson-Cohen, C.; de Boer, I.H.; Houston, D.K.; Lohman, K.; Liu, Y.; Kritchevsky, S.B.; Cauley, J.A.; Tanaka, T.; Ferrucci, L.; et al. Genetic Variants and Associations of 25-Hydroxyvitamin D Concentrations With Major Clinical Outcomes. JAMA 2012, 308, 1898–1905. [Google Scholar] [CrossRef]
- Yang, A.; Lv, Q.; Chen, F.; Wang, Y.; Liu, Y.; Shi, W.; Liu, Y.; Wang, D. The effect of vitamin D on sarcopenia depends on the level of physical activity in older adults. J. Cachexia Sarcopenia Muscle 2020, 11, 678–689. [Google Scholar] [CrossRef] [PubMed]
- Cheng, J.B.; Levine, M.A.; Bell, N.H.; Mangelsdorf, D.J.; Russell, D.W. Genetic evidence that the human CYP2R1 enzyme is a key vitamin D 25-hydroxylase. Proc. Natl. Acad. Sci. USA 2004, 1011, 7711–7715. [Google Scholar] [CrossRef] [Green Version]
- Slater, N.A.; Rager, M.L.; Havrda, D.E.; Harralson, A.F. Genetic Variation in CYP2R1 and GC Genes Associated With Vitamin D Deficiency Status. J. Pharm. Pract. 2017, 30, 31–36. [Google Scholar] [CrossRef]
- Engelman, C.D.; Meyers, K.J.; Iyengar, S.K.; Liu, Z.; Karki, C.K.; Igo, R.P., Jr.; Truitt, B.; Robinson, J.; Sarto, G.E.; Wallace, R.; et al. Vitamin D intake and season modify the effects of the GC and CYP2R1 genes on 25-hydroxyvitamin D concentrations. J. Nutr. 2013, 143, 17–26. [Google Scholar] [CrossRef] [Green Version]
- Pike, J.W.; Meyer, M.B. The Vitamin D Receptor: New Paradigms for the Regulation of Gene Expression by 1,25-Dihydroxyvitamin D3. Endocrinol. Metab. Clin. North Am. 2010, 39, 255–269. [Google Scholar] [CrossRef]
- Kamyshna, I.I.; Pavlovych, L.B.; Malyk, I.V.; Kamyshnyi, A.M. 25-OH Vitamin D blood serum linkage with VDR gene polymorphism (rs2228570) in thyroid pathology patients in the West-Ukrainian population. J. Med. Life 2021, 14, 549–556. [Google Scholar] [CrossRef] [PubMed]
- Redenšek, S.; Kristanc, T.; Blagus, T.; Trošt, M.; Dolžan, V. Genetic Variability of the Vitamin D Receptor Affects Susceptibility to Parkinson’s Disease and Dopaminergic Treatment Adverse Events. Front Aging Neurosci. 2022, 14, 853277. [Google Scholar] [CrossRef] [PubMed]
- McGrath, J.J.; Saha, S.; Burne, T.H.J.; Eyles, D.W. A systematic review of the association between common single nucleotide polymorphisms and 25-hydroxyvitamin D concentrations. J. Steroid. Biochem. Mol. Biol. 2010, 121, 471–477. [Google Scholar] [CrossRef] [PubMed]
- Caixàs, A.; Villaró, M.; Arraiza, C.; Montalvá, J.C.; Lecube, A.; Fernández-García, J.M.; Corio, R.; Bellido, D.; Llisterri, J.L.; Tinahones, F.J. Consensus document of the Spanish Obesity Society (SEEDO) and the Spanish Society of Primary Care Physicians (SEMERGEN) on continuity of care in obesity between Primary Care and Specialized Hospital Units 2019. Med. Clin. 2020, 155, e1–e267. [Google Scholar]
- Trichopoulou, A.; Costacou, T.; Bamia, C.; Trichopoulos, D. Adherence to a Mediterranean Diet and Survival in a Greek Population. N. Engl. J. Med. 2003, 348, 2599–2608. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gould, D.; Crichton, N. Information point: Visual Analogue Scale (VAS). Rev. Enf. Cli. 2001, 10, 697–706. [Google Scholar]
- Janssen, I.; Heymsfield, S.B.; Baumgartner, R.N.; Ross, R. Estimation of skeletal muscle mass by bioelectrical impedance analysis. J. Appl. Physiol. 2000, 89, 465–471. [Google Scholar] [CrossRef] [Green Version]
- Bohannon, R.W. Dynamometer Measurements of Hand-Grip Strength Predict Multiple Outcomes. Percept. Mot. Skills 2001, 93, 323–328. [Google Scholar] [CrossRef]
- Gálvez Cano, M.; Varela Pinedo, L.F.; Helver Chávez, J.; Cieza, Z. Correlation of the Get-Up-And-Go Test With The Tinetti Test when assessing the risk for falls in elderly persons. Acta Med. Peru 2010, 27, 8–11. [Google Scholar]
- Cruz-Jentoft, A.J.; Bahat, G.; Bauer, J.; Boirie, Y.; Bruyère, O.; Cederholm, T.; Cooper, C.; Landi, F.; Rolland, Y.; Sayer, A.A.; et al. Sarcopenia: Revised European consensus on definition and diagnosis. Age Ageing 2019, 48, 16–31. [Google Scholar] [CrossRef] [Green Version]
- Casado, E.; Quesada, J.; Naves, M.; Peris, P.; Jódar, E.; Giner, M.; Neyro, J.L.; Del Pino, J.; Sosa, M.; De Paz, H.D.; et al. SEIOMM recommendations for the prevention and treatment of vitamin D deficiency. Rev. Osteoporos. Metab. Miner. 2021, 13, 84–97. [Google Scholar]
- Fernández-Lázaro, D.; García Hernández, J.L.G.; Caballero García, A.; Córdova Martínez, A.; Mielgo-Ayuso, J.; Cruz-Hernández, J.J. Liquid Biopsy as Novel Tool in Precision Medicine: Origins, Properties, Identification and Clinical Perspective of Cancer’s Biomarkers. Diagnostics 2020, 10, 215. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Shastry, B.S. SNP alleles in human disease and evolution. J. Hum. Genet. 2002, 47, 561–566. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Guest, N.S.; Horne, J.; Vanderhout, S.M.; El-Sohemy, A. Sport Nutrigenomics: Personalized Nutrition for Athletic Performance. Front. Nutr. 2019, 6, 8. [Google Scholar] [CrossRef]
- Vidigal, V.M.; Silva, T.D.; de Oliveira, J.; Pimenta, C.A.M.; Felipe, A.V.; Forones, N.M. Genetic polymorphisms of vitamin D receptor (VDR), CYP27B1 and CYP24A1 genes and the risk of colorectal cancer. Int. J. Biol. Markers 2017, 32, e224–e230. [Google Scholar] [CrossRef]
- Karaky, M.; Alcina, A.; Fedetz, M.; Barrionuevo, C.; Potenciano, V.; Delgado, C.; Izquierdo, G.; Matesanz, F. The multiple sclerosis-associated regulatory variant rs10877013 affects expression of CYP27B1 and VDR under inflammatory or vitamin D stimuli. Mult. Scler. 2016, 22, 999–1006. [Google Scholar] [CrossRef]
- Whitfield, G.K.; Remus, L.S.; Jurutka, P.W.; Zitzer, H.; Oza, A.K.; Dang, H.T.; Haussler, C.A.; Galligan, M.A.; Thatcher, M.L.; Encinas Dominguez, C.; et al. Functionally relevant polymorphisms in the human nuclear vitamin D receptor gene. Mol. Cell Endocrinol. 2010, 177, 145–159. [Google Scholar] [CrossRef]
- Ucan, B.; Sahin, M.; Sayki Arslan, M.; Colak Bozkurt, N.; Kizilgul, M.; Güngünes, A.; Cakal, E.; Ozbek, M. Vitamin D Treatment in Patients with Hashimoto’s Thyroiditis may Decrease the Development of Hypothyroidism. Int. J. Vitam. Nutr. Res. 2016, 86, 9–17. [Google Scholar] [CrossRef]
- Bischoff-Ferrari, H.A.; Dietrich, T.; Orav, E.J.; Hu, F.B.; Zhang, Y.; Karlson, E.W.; Dawson-Hughes, B. Higher 25-hydroxyvitamin D concentrations are associated with better lower-extremity function in both active and inactive persons aged > or =60 y. Am. J. Clin. Nutr. 2004, 80, 752–758. [Google Scholar] [CrossRef] [Green Version]
- Garcia, L.A.; King, K.K.; Ferrini, M.G.; Norris, K.C.; Artaza, J.N. 1,25(OH)2vitamin D3 stimulates myogenic differentiation by inhibiting cell proliferation and modulating the expression of promyogenic growth factors and myostatin in C2C12 skeletal muscle cells. Endocrinology 2011, 152, 2976–2986. [Google Scholar] [CrossRef] [Green Version]
- Ksiażek, A.; Zagrodna, A.; Słowińska-Lisowska, M. Vitamin D, Skeletal Muscle Function and Athletic Performance in Athletes—A Narrative Review. Nutrients 2019, 11, 1800. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Brunner, F.; Schmid, A.; Sheikhzadeh, A.; Nordin, M.; Yoon, J.; Frankel, V. Effects of aging on Type II muscle fibers: A systematic review of the literature. J. Aging Phys. Act. 2007, 15, 336–348. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Fernández-Lázaro, D.; Garrosa, E.; Seco-Calvo, J.; Garrosa, M. Potential Satellite Cell-Linked Biomarkers in Aging Skeletal Muscle Tissue: Proteomics and Proteogenomics to Monitor Sarcopenia. Proteomes 2022, 10, 29. [Google Scholar] [CrossRef] [PubMed]
- Girgis, C.M.; Cha, K.M.; So, B.; Tsang, M.; Chen, J.; Houweling, P.J.; Schindeler, A.; Stokes, R.; Swarbrick, M.M.; Evesson, F.J.; et al. Mice with myocyte deletion of vitamin D receptor have sarcopenia and impaired muscle function. J. Cachexia Sarcopenia Muscle 2019, 10, 1228–1240. [Google Scholar] [CrossRef] [PubMed]
- van der Wielen, R.P.J.; de Groot, L.C.P.G.M.; van Staveren, W.A.; Löwik, M.R.H.; van den Berg, H.; Haller, J.; Moreiras, O. Serum vitamin D concentrations among elderly people in Europe. Lancet 1995, 346, 207–210. [Google Scholar] [CrossRef]
- Mateo-Pascual, C.; Julián-Viñals, R.; Alarcón-Alarcón, T.; Castell-Alcalá, M.V.; Iturzaeta-Sánchez, J.M.; Otero-Piume, A. Vitamin D deficiency in a cohort of over 65-year-olds: Prevalence and association with sociodemographic and health factors. Rev. Esp. Geriatr. Gerontol. 2014, 49, 210–216. [Google Scholar] [CrossRef]
- Vaqueiro, M.; Baré, M.L.; Anton, E.; Andreu, E.; Gimeno, C.; Moya, A.; D’AVIS Group. Evaluation assessment of the cut-off point of vitamin D in the population older than 64 years old. Med. Clin. 2016, 127, 648–650. [Google Scholar] [CrossRef]
- Formiga, F.; Ferrer, A.; Almeda, J.; San Jose, A.; Gil, A.; Pujol, R. Utility of geriatric assessment tools to identify 85-years old subjects with vitamin D deficiency. J. Nutr. Health Aging 2011, 15, 110–114. [Google Scholar] [CrossRef]
- Ginde, A.A.; Liu, M.C.; Camargo, C.A. Demographic Differences and Trends of Vitamin D Insufficiency in the US Population, 1988–2004. Arch. Intern. Med. 2009, 169, 626–632. [Google Scholar] [CrossRef] [Green Version]
- Cashman, K.D.; van den Heuvel, E.G.H.M.; Schoemaker, R.J.W.; Prévéraud, D.P.; Macdonald, H.M.; Arcot, J. 25-Hydroxyvitamin D as a Biomarker of Vitamin D Status and Its Modeling to Inform Strategies for Prevention of Vitamin D Deficiency within the Population. Adv. Nutr. 2017, 8, 947–957. [Google Scholar] [CrossRef]


{kind=link}
| Characteristics | Full Cohort (n = 19) |
|---|---|
| Sociodemographic and Lifestyle | |
| Gender, n (%) | |
| Male | 19 (100.0) |
| Female | 0 (0.0) |
| Age (years), mean (SD) | 82.9 (6.7) |
| Nationality, n (%) | |
| Spanish | 17 (89.5) |
| Other | 2 (10.5) |
| 1 Body mass index (BMI), (kg/m2), mean (SD) | 27.2 (5.2) |
| 2 Skeletal Muscle Mass (SMM), (kg), mean (SD) | 23.8 (6.8) |
| Skeletal Muscle Mass Index (SMMI) (kg/m2), mean (SD) | 9.1 (2.6) |
| Sun exposure, (min·day−1) | 17.37 (6.76) |
| <15 min·day−1, n (%) | 5 (26.3) |
| > 15 min·day−1, n (%) | 14 (73.6) |
| Smoker, n (%) | 6 (31.5) |
| Non-Smoker | 10 (52.6) |
| Never Smoker | 3 (15.7) |
| 3 Trichopoulou’s MedDiet score, mean (SD) | 10.4 (1.9) |
| 4 Self-perceived health status g (%), mean (SD) | 72.9 (14.7) |
| Physical Fitness | |
| 5 Manual pressure dynamometry (kg/cm2), mean (SD) | |
| Dominant hand | 26.4 (5.6) |
| Non-dominant hand | 19.6 (4.3) |
| 6 Get-Up-And-Go Test (seconds), mean (SD) | 15.6 (6.5) |
| Yes (<20 seg), n (%) | 14 (73.6) |
| No (≥20 seg), n (%) | 5 (26.3) |
| Clinics | |
| Known allergies, n (%) | |
| Yes | 5 (26.3) |
| No | 14 (73.6) |
| Previously passed COVID-19 infection, n (%) | |
| Yes | 12 (63.15) |
| No | 7 (36.8) |
| Pathologies, n (%) | |
| Arterial hypertension | 17 (89.9) |
| Obesity | 1 (5.2) |
| Insulin-dependent diabetes mellitus | 2 (10.5) |
| 7 Respiratory | 2 (10.5) |
| Cancer | 1 (5.2) |
| 8 Cardiovascular | 14 (73.6) |
| Usual treatment, n (%) | |
| Antihypertensives | 17 (89.9) |
| Anticoagulants | 3 (15.7) |
| Immunosuppressants | 1 (5.2) |
| Anxiolytics/Sedatives | 16 (84.2) |
| Lipid lowering agents | 3 (15.7) |
| Antidiabetics | 2 (10.5) |
| Cardiovascular | 14 (73.6) |
| Use of oxygen therapy, n (%) | |
| Currently | 1 (5.2) |
| Previous/Occasional | 2 (10.5) |
| Never | 16 (84.2) |
| Vital signs, mean (SD) | |
| Blood pressure | |
| SBP (mmHg) | 127 (14.0) |
| DBT (mmHg) | 72.3 (12.4) |
| Heart rate (bpm) | 76.1 (12.7) |
| Temperature (°C) | 35.8 (0.5) |
| Oxygen saturation (%) | 98.9 (1.9) |
| Age (Years) | Sample (n) | 25-OH/D (ng/mL) Mean (SD) | Deficiency n (%) <10 ng/mL | Insufficiency (%) 10–30 ng/mL | Normal (%) >30 ng/mL |
|---|---|---|---|---|---|
| <70 | 8 | 26.5 (11.8) | 1 (5.2) | 4 (50.0) | 3 (37.5) |
| >70 | 11 | 19.5 (7.8) | - | 9 (81.8) | 2 (18.2) |
| 82.9 (6.7) | 19 | 22.7 (10.1) | 1 (5.2) | 13 (68.4) | 5 (26.3) |
| Gen | SNPs | Allele | n (%) | Degrees of Sarcopenia (n°) | Sarcopenia | |||
|---|---|---|---|---|---|---|---|---|
| Absence (0°) | Probable (1°) | Confirmed (2°) | Severe (3°) | Full Cohort (n = 19) | ||||
| CYP2R1 | rs10741657 | AA | 5 (26.3) | 4 | 0 | 1 | 0 | 1 |
| GA | 8 (42.1) | 1 | 3 | 2 | 2 | 4 | ||
| GG | 6 (31.5) | 1 | 0 | 2 | 3 | 5 | ||
| AA/GA/GG | 19 (100) | 6 | 3 | 5 | 5 | 10 | ||
| GC | rs2282679 | TT | 4 (21.1) | 4 | 0 | 0 | 0 | 0 |
| GT | 8 (42.2) | 1 | 2 | 2 | 3 | 5 | ||
| GG | 7 (36.8) | 1 | 1 | 3 | 2 | 5 | ||
| TT/GT/GG | 19 (100) | 5 | 3 | 5 | 5 | 10 | ||
| VDR | rs228570 | AA | 9 (47.3) | 6 | 1 | 1 | 1 | 2 |
| GA | 5 (26.3) | 0 | 2 | 1 | 2 | 3 | ||
| GG | 5 (26.3) | 0 | 0 | 3 | 2 | 5 | ||
| AA/GA/GG | 19 (100) | 6 | 3 | 5 | 5 | 10 | ||
| Gen | SNPs | Alleles | 25-OH/D (ng/mL), Mean (SD) | p-Value |
|---|---|---|---|---|
| CYP2R1 | rs10741657 | AA | 30.0 (12.4) | 0.084 |
| GA | 22.7 (8.7) | |||
| GG | 16.6 (5.9) | |||
| GC | rs2282679 | TT | 37.7 (4.4) | <0.001 |
| GT * | 20.5 (6.9) | |||
| GG * | 16.7 (6.2) | |||
| VDR | rs228570 | AA | 29.9 (9.5) | <0.001 |
| GA & | 18.6 (3.7) | |||
| GG & | 14.0 (5.1) |
| Gen (SNPs) | Full Cohort (n = 19) | |
|---|---|---|
| r | p-Value | |
| CYP2R1 (rs10741657) | ||
| AA | 0.18 | 0.035 |
| GA | 0.09 | 0.436 |
| GG | −0.32 | 0.013 |
| GC (rs2282679) | ||
| TT | 0.27 | 0.038 |
| GT | 0.08 | 0.541 |
| GG | −0.34 | 0.011 |
| VDR (rs228570) | ||
| AA | 0.16 | 0.031 |
| GA | 0.05 | 0.169 |
| GG | −0.41 | <0.001 |
| SNPs | Bi-Allelic Variant | Full Cohort (n = 19) | |
|---|---|---|---|
| OR (IC 95%) Crude | OR (IC 95%) 1 Multivariate Analysis | ||
| GC (rs2282679) | GT | 1.00 (ref.) | 1.00 (ref.) |
| TT | 1.03 (0.56–1.74) | 1.23 (0.78–1.76) | |
| GG | 0.95 (0.74–1.17) | 0.88 (0.56–1.25) | |
| CYP2R1 (rs10741657) | GA | 1.00 (ref.) | 1.00 (ref.) |
| AA | 1.18 (0.63–1.89) | 1.21 (0.92–2.07) | |
| GG | 0.92 (0.54–1.17) | 0.84 (0.69–1.49) | |
| VDR (rs228570) | GA | 1.00 (ref.) | 1.00 (ref.) |
| AA | 1.10 (0.64–2.03) | 1.19 (0.82–1.88) | |
| GG | 0.78 (0.51–1.28) | 0.64 (0.49–1.15) | |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Fernández-Lázaro, D.; Hernández, J.L.G.; Lumbreras, E.; Mielgo-Ayuso, J.; Seco-Calvo, J. 25-Hydroxyvitamin D Serum Levels Linked to Single Nucleotide Polymorphisms (SNPs) (rs2228570, rs2282679, rs10741657) in Skeletal Muscle Aging in Institutionalized Elderly Men Not Supplemented with Vitamin D. Int. J. Mol. Sci. 2022, 23, 11846. https://doi.org/10.3390/ijms231911846
Fernández-Lázaro D, Hernández JLG, Lumbreras E, Mielgo-Ayuso J, Seco-Calvo J. 25-Hydroxyvitamin D Serum Levels Linked to Single Nucleotide Polymorphisms (SNPs) (rs2228570, rs2282679, rs10741657) in Skeletal Muscle Aging in Institutionalized Elderly Men Not Supplemented with Vitamin D. International Journal of Molecular Sciences. 2022; 23(19):11846. https://doi.org/10.3390/ijms231911846
Chicago/Turabian StyleFernández-Lázaro, Diego, Juan Luis García Hernández, Eva Lumbreras, Juan Mielgo-Ayuso, and Jesús Seco-Calvo. 2022. "25-Hydroxyvitamin D Serum Levels Linked to Single Nucleotide Polymorphisms (SNPs) (rs2228570, rs2282679, rs10741657) in Skeletal Muscle Aging in Institutionalized Elderly Men Not Supplemented with Vitamin D" International Journal of Molecular Sciences 23, no. 19: 11846. https://doi.org/10.3390/ijms231911846