
Comparison of Topical Hemostatic Agents in a Swine Model of Extremity Arterial Hemorrhage: BloodSTOP iX Battle Matrix vs. QuikClot Combat Gauze

 ,
,
Abstract
:
1. Introduction
2. Results
2.1. Biological Characteristics of Animals for in Vivo Experiment
2.2. Hemostasis Achievements and Blood Loss
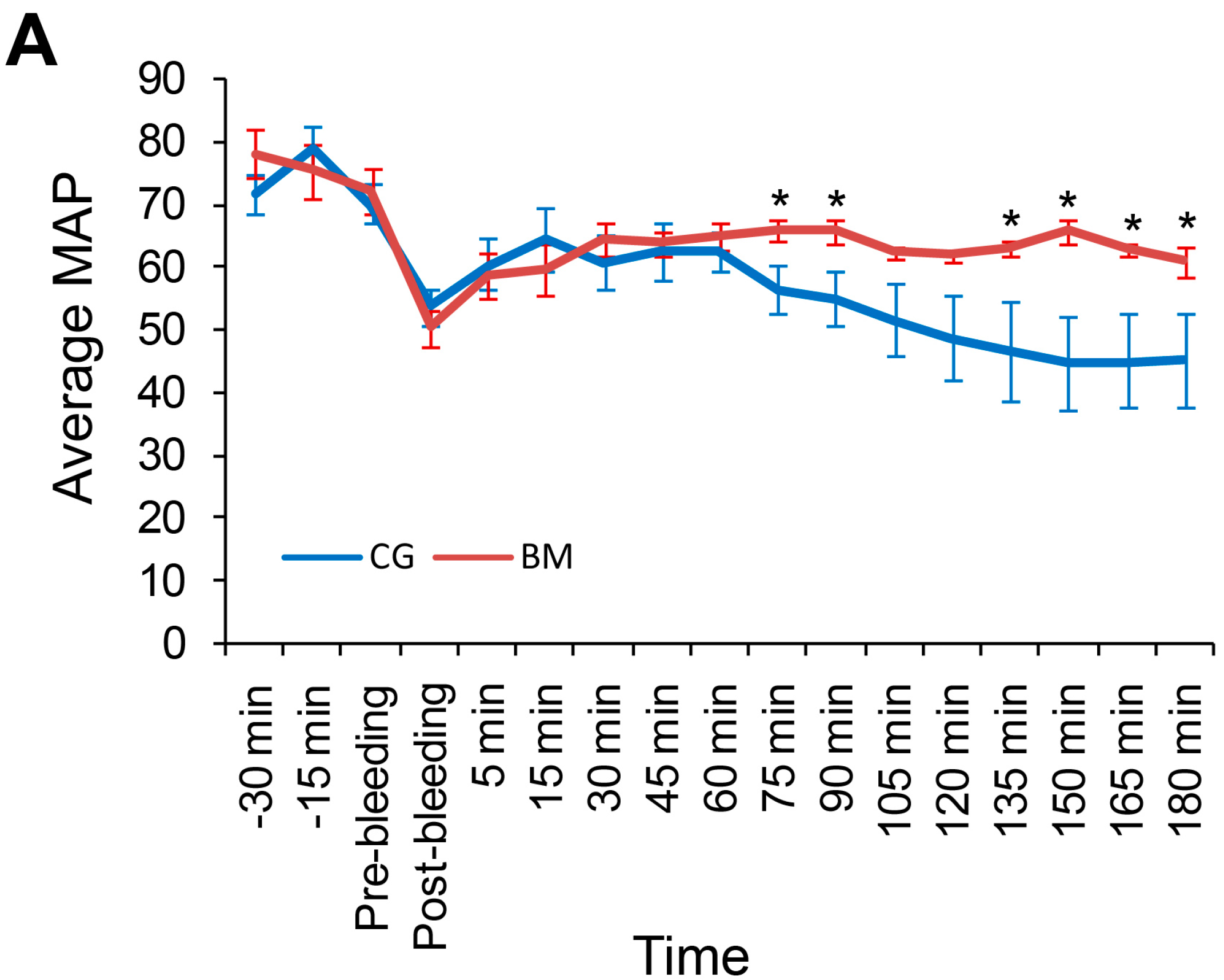
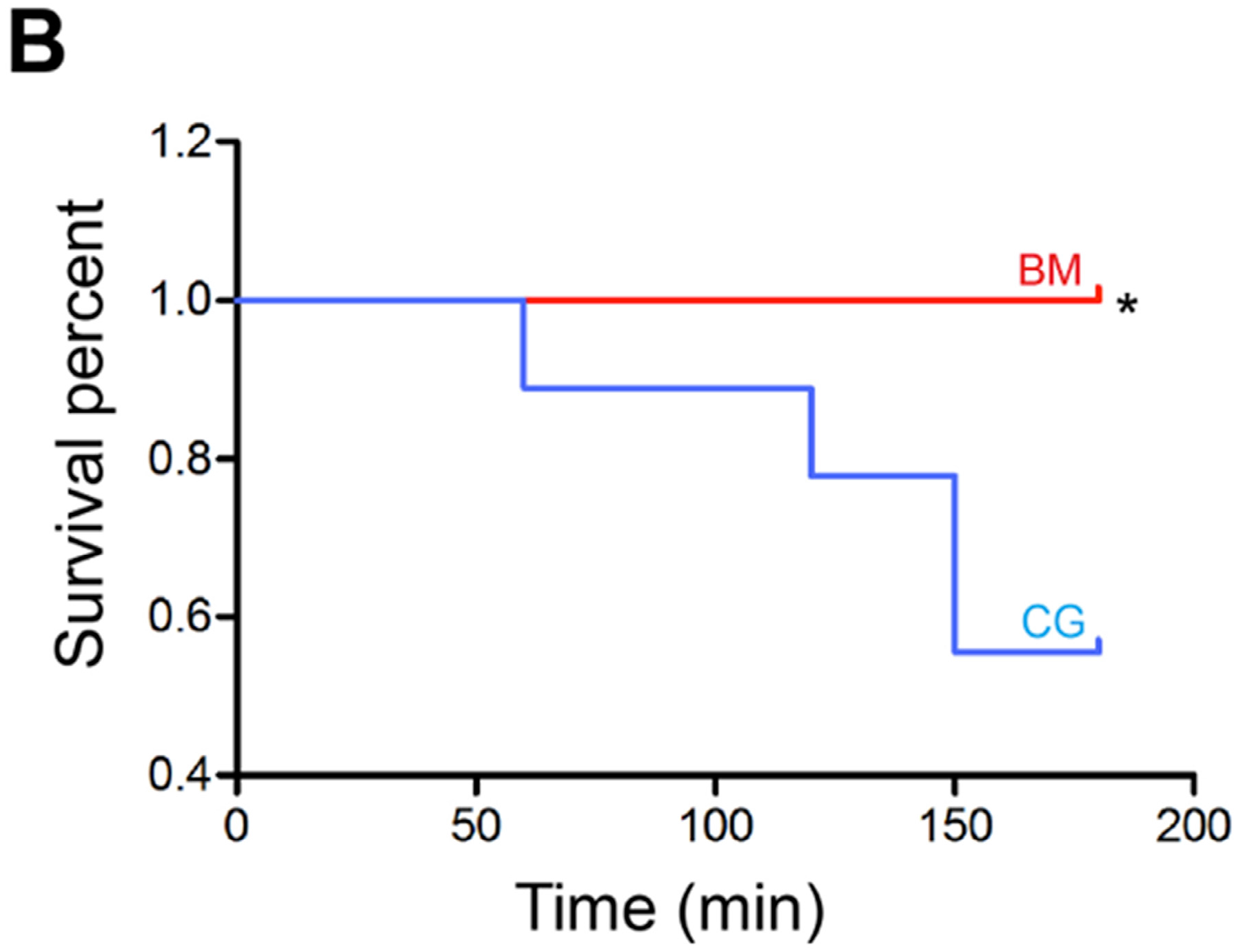
2.3. Mean Arterial Pressure and Survival
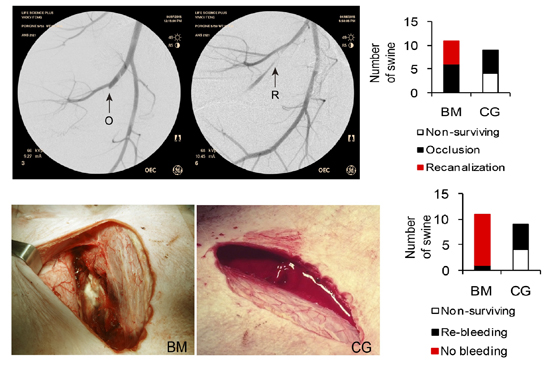
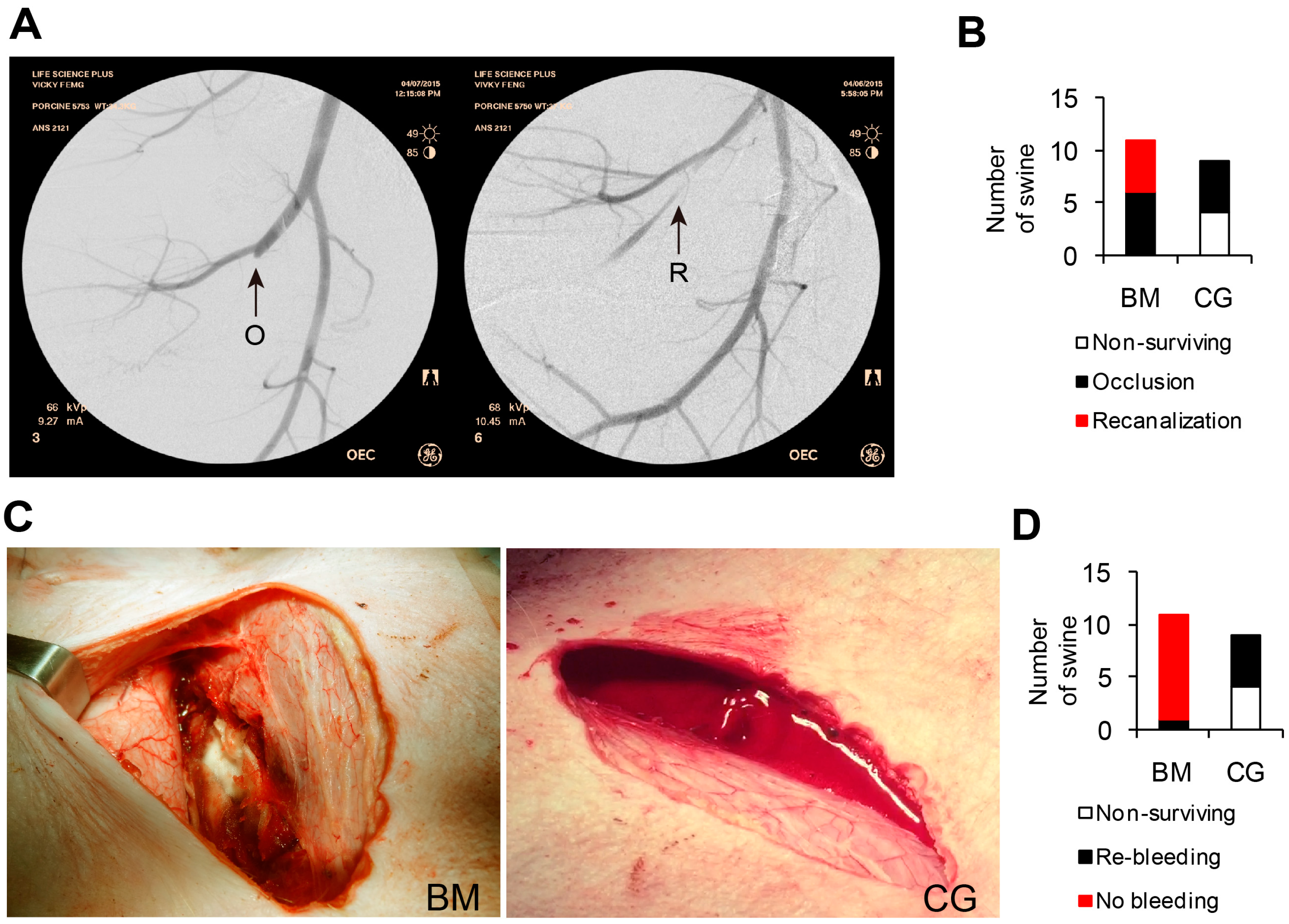
2.4. Fluoroscopic Angiography
2.5. Morphological Assessment
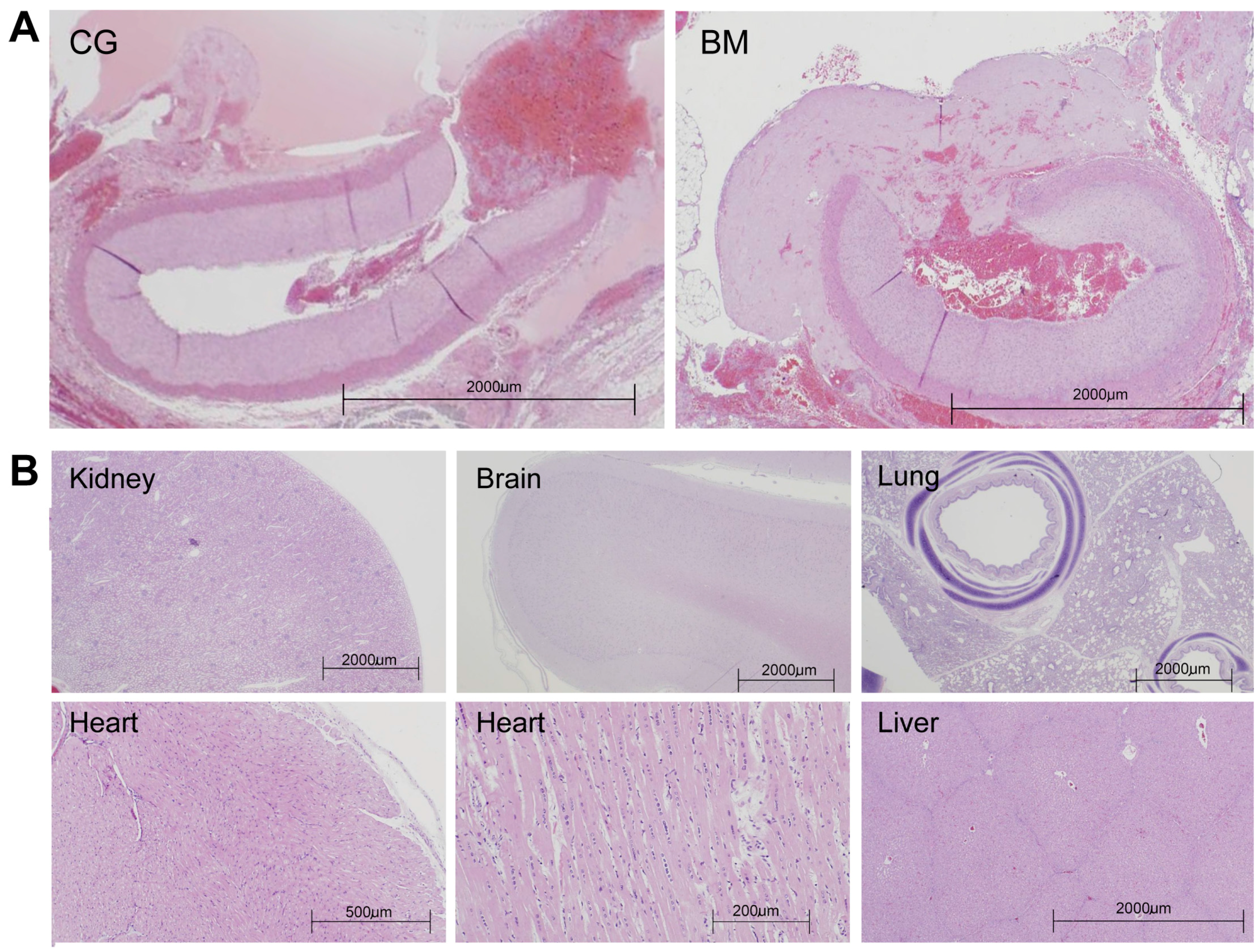
2.6. Histologic Assessment
3. Discussion
4. Materials and Methods
4.1. Test Materials
4.2. Animal Preparation
4.3. Surgical Procedures
4.4. Endpoints
4.5. Gross Pathology and Histopathology
4.6. Data Analysis
5. Conclusions
Acknowledgments
Author Contributions
Conflicts of Interest
References
- Kheirabadi, B.S.; Scherer, M.R.; Estep, J.S.; Dubick, M.A.; Holcomb, J.B. Determination of efficacy of new hemostatic dressings in a model of extremity arterial hemorrhage in swine. J. Trauma 2009, 67, 450–459. [Google Scholar] [CrossRef] [PubMed]
- Kheirabadi, B. Evaluation of topical hemostatic agents for combat wound treatment. US Army Med. Dep. J. 2011, 2, 25–37. [Google Scholar]
- Johansson, P.I.; Stensballe, J.; Ostrowski, S.R. Current management of massive hemorrhage in trauma. Scand. J. Trauma Resusc. Emerg. Med. 2012, 20. [Google Scholar] [CrossRef] [PubMed]
- Morrison, J.J.; Mountain, A.J.; Galbraith, K.A.; Clasper, J.C. Penetrating pelvic battlefield trauma: Internal use of chitosan-based haemostatic dressings. Injury 2010, 41, 239–241. [Google Scholar] [CrossRef] [PubMed]
- Watters, J.M.; Van, P.Y.; Hamilton, G.J.; Sambasivan, C.; Differding, J.A.; Schreiber, M.A. Advanced hemostatic dressings are not superior to gauze for care under fire scenarios. J. Trauma 2011, 70, 1413–1419. [Google Scholar] [CrossRef] [PubMed]
- Drew, B.; Bennett, B.L.; Littlejohn, L. Application of current hemorrhage control techniques for backcountry care: Part one, tourniquets and hemorrhage control adjuncts. Wilderness Environ. Med. 2015, 26, 236–245. [Google Scholar] [CrossRef] [PubMed]
- Littlejohn, L.; Bennett, B.L.; Drew, B. Application of current hemorrhage control techniques for backcountry care: Part two, hemostatic dressings and other adjuncts. Wilderness Environ. Med. 2015, 26, 246–254. [Google Scholar] [CrossRef] [PubMed]
- Pal, K.; Banthia, A.K.; Majumdar, D.K. Polymeric hydrogels: Characterization and biomedical applications—A mini review. Des. Monomers Polym. 2009, 12, 197–220. [Google Scholar] [CrossRef]
- Delgado, A.V.; Kheirabadi, B.S.; Fruchterman, T.M.; Scherer, M.; Cortez, D.; Wade, C.E.; Dubick, M.A.; Holcomb, J.B. A novel biologic hemostatic dressing (fibrin patch) reduces blood loss and resuscitation volume and improves survival in hypothermic, coagulopathic swine with grade V liver injury. J. Trauma 2008, 64, 75–80. [Google Scholar] [CrossRef] [PubMed]
- Rothwell, S.W.; Sawyer, E.; Dorsey, J.; Flournoy, W.S.; Settle, T.; Simpson, D.; Cadd, G.; Janmey, P.; White, C.; Szabo, K.A. Wound healing and the immune response in swine treated with a hemostatic bandage composed of salmon thrombin and fibrinogen. J. Mater. Sci. Mater. Med. 2009, 20, 2155–2166. [Google Scholar] [CrossRef] [PubMed]
- Acheson, E.M.; Kheirabadi, B.S.; Deguzman, R.; Dick, E.J., Jr.; Holcomb, J.B. Comparison of hemorrhage control agents applied to lethal extremity arterial hemorrhages in swine. J. Trauma 2005, 59, 865–874. [Google Scholar] [CrossRef] [PubMed]
- Alam, H.B.; Chen, Z.; Jaskille, A.; Querol, R.I.; Koustova, E.; Inocencio, R.; Conran, R.; Seufert, A.; Ariaban, N.; Toruno, K.; et al. Application of a zeolite hemostatic agent achieves 100% survival in a lethal model of complex groin injury in swine. J. Trauma 2004, 56, 974–983. [Google Scholar] [CrossRef] [PubMed]
- Arnaud, F.; Tomori, T.; Saito, R.; McKeague, A.; Prusaczyk, W.K.; McCarron, R.M. Comparative efficacy of granular and bagged formulations of the hemostatic agent quikclot. J. Trauma 2007, 63, 775–782. [Google Scholar] [CrossRef] [PubMed]
- Dowling, M.B.; Kumar, R.; Keibler, M.A.; Hess, J.R.; Bochicchio, G.V.; Raghavan, S.R. A self-assembling hydrophobically modified chitosan capable of reversible hemostatic action. Biomaterials 2011, 32, 3351–3357. [Google Scholar] [CrossRef] [PubMed]
- Ferretti, L.; Qiu, X.; Villalta, J.; Lin, G. Efficacy of bloodstop iX, surgicel, and gelfoam in rat models of active bleeding from partial nephrectomy and aortic needle injury. Urology 2012, 80, 1161.e1–1166.e6. [Google Scholar] [CrossRef] [PubMed]
- Mueller, G.R.; Pineda, T.J.; Xie, H.X.; Teach, J.S.; Barofsky, A.D.; Schmid, J.R.; Gregory, K.W. A novel sponge-based wound stasis dressing to treat lethal noncompressible hemorrhage. J. Trauma Acute Care Surg. 2012, 73, S134–S139. [Google Scholar] [CrossRef] [PubMed]
- Littlejohn, L.F.; Devlin, J.J.; Kircher, S.S.; Lueken, R.; Melia, M.R.; Johnson, A.S. Comparison of celox-a, chitoflex, woundstat, and combat gauze hemostatic agents vs. standard gauze dressing in control of hemorrhage in a swine model of penetrating trauma. Acad. Emerg. Med. 2011, 18, 340–350. [Google Scholar] [CrossRef] [PubMed]
- Floyd, C.T.; Rothwell, S.W.; Risdahl, J.; Martin, R.; Olson, C.; Rose, N. Salmon thrombin-fibrinogen dressing allows greater survival and preserves distal blood flow compared to standard kaolin gauze in coagulopathic swine with a standardized lethal femoral artery injury. J. Spec. Oper. Med. 2012, 12, 16–26. [Google Scholar] [PubMed]
- Gegel, B.T.; Austin, P.N.; Johnson, A.D. An evidence-based review of the use of a combat gauze (quikclot) for hemorrhage control. AANA J. 2013, 81, 453–458. [Google Scholar] [PubMed]
- Devlin, J.J.; Kircher, S.; Kozen, B.G.; Littlejohn, L.F.; Johnson, A.S. Comparison of chitoflex®, celox™, and quikclot® in control of hemorrhage. J. Emerg. Med. 2011, 41, 237–245. [Google Scholar] [CrossRef] [PubMed]
- Chappell, D.; Jacob, M.; Hofmann-Kiefer, K.; Conzen, P.; Rehm, M. A rational approach to perioperative fluid management. Anesthesiology 2008, 109, 723–740. [Google Scholar] [CrossRef] [PubMed]
- Safar, P.J.; Tisherman, S.A. Trauma resuscitation: What have we learned in the last 50 years? Curr. Opin. Anaesthesiol. 2003, 16, 133–138. [Google Scholar] [CrossRef] [PubMed]
- Gerlach, T.; Grayson, J.K.; Pichakron, K.O.; Sena, M.J.; DeMartini, S.D.; Clark, B.Z.; Estep, J.S.; Zierold, D. Preliminary study of the effects of smectite granules (woundstat) on vascular repair and wound healing in a swine survival model. J. Trauma 2010, 69, 1203–1209. [Google Scholar] [CrossRef] [PubMed]
- Kheirabadi, B.S.; Mace, J.E.; Terrazas, I.B.; Fedyk, C.G.; Estep, J.S.; Dubick, M.A.; Blackbourne, L.H. Safety evaluation of new hemostatic agents, smectite granules, and kaolin-coated gauze in a vascular injury wound model in swine. J. Trauma 2010, 68, 269–278. [Google Scholar] [CrossRef] [PubMed]
- Causey, M.W.; McVay, D.P.; Miller, S.; Beekley, A.; Martin, M. The efficacy of combat gauze in extreme physiologic conditions. J. Surg. Res. 2012, 177, 301–305. [Google Scholar] [CrossRef] [PubMed]
- Sena, M.J.; Douglas, G.; Gerlach, T.; Grayson, J.K.; Pichakron, K.O.; Zierold, D. A pilot study of the use of kaolin-impregnated gauze (combat gauze) for packing high-grade hepatic injuries in a hypothermic coagulopathic swine model. J. Surg. Res. 2013, 183, 704–709. [Google Scholar] [CrossRef] [PubMed]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Parameter | Pre-Treatment | Post-Treatment | ||||||
|---|---|---|---|---|---|---|---|---|
| Measure | BM (n = 11) | CG (n = 9) | BM (n = 11) | CG (n = 9) | ||||
| Temperature (°C) | 36.1 | ±0.3 | 36.3 | ±0.4 | 36.9 | ±0.5 | 36.4 | ±0.5 |
| MAP (mmHg) | 78.3 | ±3.7 | 70.4 | ±3.1 | 60.7 | ±2.3 * | 45.1 | ±7.5 |
| HGB (g/dL) | 9.1 | ±0.3 | 8.8 | ±0.3 | 7.1 | ±0.4 * | 4.7 | ±1.0 |
| HCT (%) | 27.9 | ±0.9 | 27.3 | ±0.8 | 21.6 | ±1.2 * | 14.7 | ±3.1 |
| PLT (1000/µL) | 334.5 | ±21.2 | 340.3 | ±20.4 | 229.5 | ±9.9 | 182.2 | ±36.6 |
| PT (s) | 13.9 | ±0.2 | 14.2 | ±0.2 | 14.9 | ±0.2 * | 22.0 | ±3.6 |
| aPTT (s) | 13.9 | ±0.4 | 14.8 | ±0.3 | 14.8 | ±0.4 * | 18.9 | ±1.7 |
| Fibrinogen (mg/dL) | 153.9 | ±7.7 | 201.3 | ±58.3 | 111.7 | ±7.5 | 87.2 | ±12.2 |
| Lactate (mM) | 16.7 | ±1.7 | 18.9 | ±2.2 | 19.8 | ±2.8 | 54.3 | ±18.5 |
| Outcome | BM (n = 11) | CG (n = 9) | ||
|---|---|---|---|---|
| Pre-treatment blood loss (mL/kg) | 6.8 | ±0.6 | 8.3 | ±0.9 |
| Post-treatment blood loss (mL/kg) | 9.5 | ±2.4 * | 29.9 | ±9.9 |
| Total resuscitation fluid (mL/kg) | 93.4 | ±16.4 | 110.0 | ±22.8 |
| Time to stable Hemostasis (min) | 4.8 | ±2.5 * | 58.0 | ±20.1 |
| Total stable hemostasis time † (min) | 175.2 | ±2.5 * | 92.4 | ±29.9 |
| Survival time (min) | 180.0 | ±0.0 | 150.4 | ±14.0 |
© 2016 by the authors; licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons by Attribution (CC-BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Li, H.; Wang, L.; Alwaal, A.; Lee, Y.-C.; Reed-Maldonado, A.; Spangler, T.A.; Banie, L.; O’Hara, R.B.; Lin, G. Comparison of Topical Hemostatic Agents in a Swine Model of Extremity Arterial Hemorrhage: BloodSTOP iX Battle Matrix vs. QuikClot Combat Gauze. Int. J. Mol. Sci. 2016, 17, 545. https://doi.org/10.3390/ijms17040545
Li H, Wang L, Alwaal A, Lee Y-C, Reed-Maldonado A, Spangler TA, Banie L, O’Hara RB, Lin G. Comparison of Topical Hemostatic Agents in a Swine Model of Extremity Arterial Hemorrhage: BloodSTOP iX Battle Matrix vs. QuikClot Combat Gauze. International Journal of Molecular Sciences. 2016; 17(4):545. https://doi.org/10.3390/ijms17040545
Chicago/Turabian StyleLi, Huixi, Lin Wang, Amjad Alwaal, Yung-Chin Lee, Amanda Reed-Maldonado, Taylor A. Spangler, Lia Banie, Reginald B. O’Hara, and Guiting Lin. 2016. "Comparison of Topical Hemostatic Agents in a Swine Model of Extremity Arterial Hemorrhage: BloodSTOP iX Battle Matrix vs. QuikClot Combat Gauze" International Journal of Molecular Sciences 17, no. 4: 545. https://doi.org/10.3390/ijms17040545