
C-Reactive Protein Is an Independent Predictor of 30-Day Bacterial Infection Post-Liver Transplantation


Abstract
:1. Introduction
2. Materials and Methods
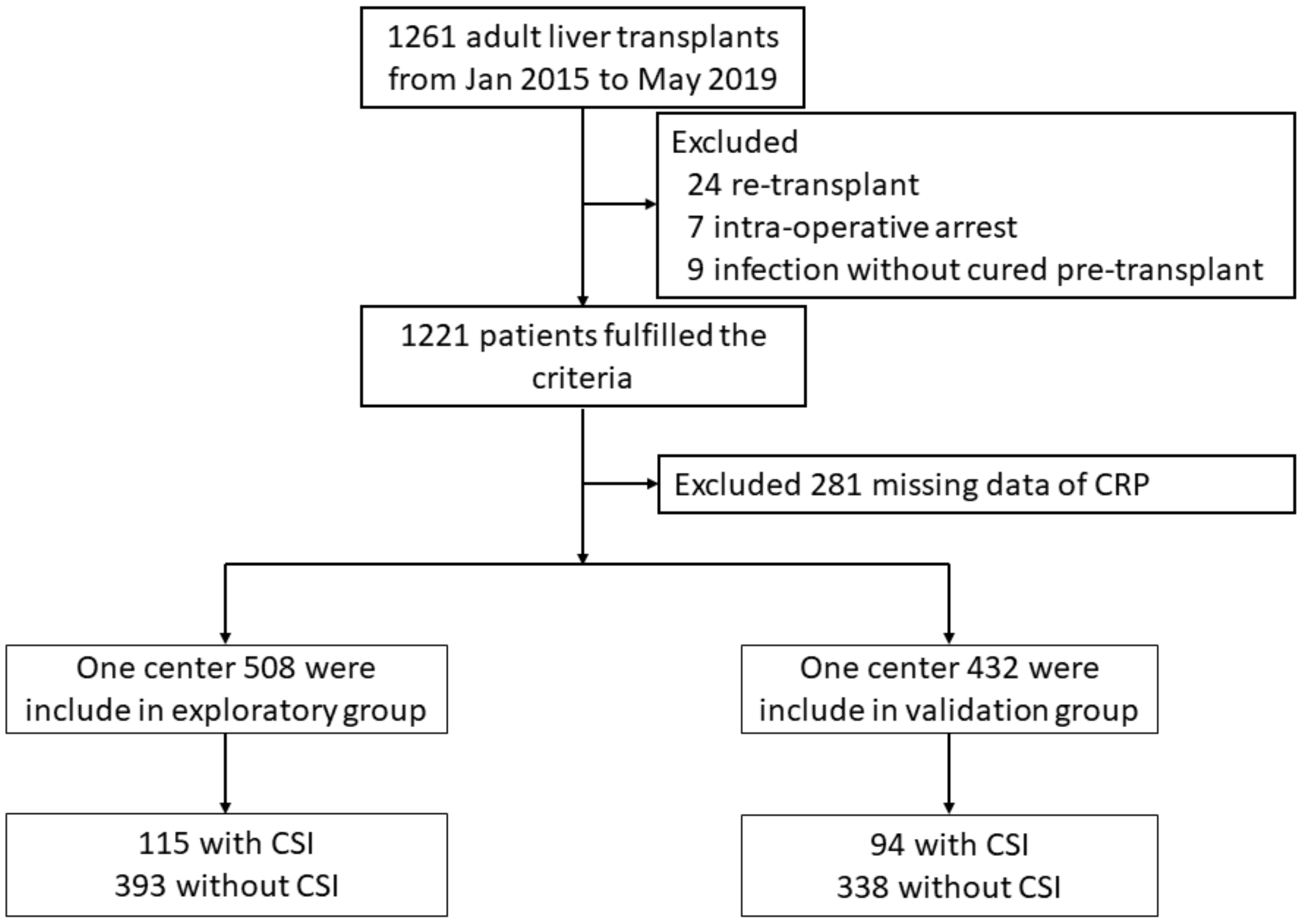
2.1. Patients
2.2. Management of Patients
2.3. Preparation of Data
2.4. Definition
2.5. Statistical Analysis
3. Results
3.1. Patients’ Characteristics
3.2. Associations of Systemic Inflammation Levels with 30-Day CSI
3.3. Effect of MELD Score, Pre-LT Infection, Liver Tumor, and Organ Failure on the Level of Systemic Inflammation
3.4. Univariate and Multivariate Analysis of Prognostic Factors for 30-Day CSI
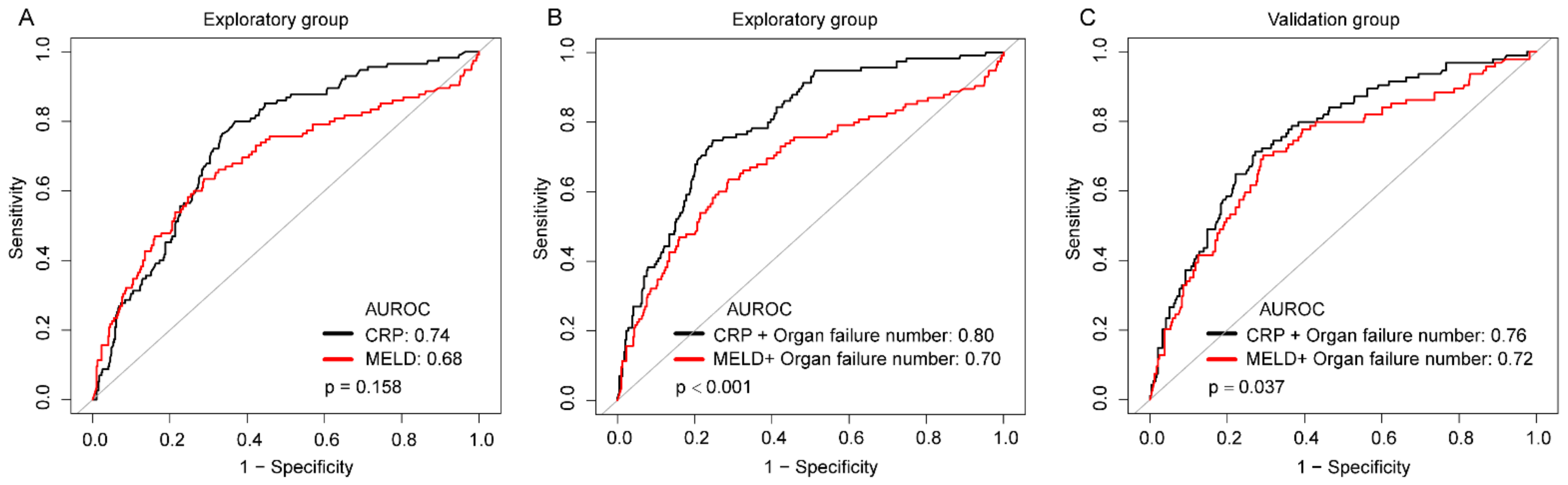
3.5. Prediction of 30-Day CSI
3.6. Potential Mechanistic Role of Systemic Inflammation Levels in 30-Day CSI
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Fishman, J.A. Infection in solid-organ transplant recipients. New Engl. J. Med. 2007, 357, 2601–2614. [Google Scholar] [CrossRef] [Green Version]
- Van Hoek, B.; de Rooij, B.J.; Verspaget, H.W. Risk factors for infection after liver transplantation. Best Pract. Research. Clin. Gastroenterol. 2012, 26, 61–72. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kusejko, K.; Neofytos, D.; Hirsch, H.H.; Meylan, P.; Boggian, K.; Hirzel, C.; Garzoni, C.; Kouyos, R.D.; Mueller, N.J.; Schreiber, P.W.; et al. Differences between infectious disease events in first liver transplant versus re-transplantation in the Swiss Transplant Cohort Study. Liver Transpl. Off. Publ. Am. Assoc. Study Liver Dis. Int. Liver Transpl. Soc. 2021. [Google Scholar] [CrossRef]
- Fagiuoli, S.; Colli, A.; Bruno, R.; Craxi, A.; Gaeta, G.B.; Grossi, P.; Mondelli, M.U.; Puoti, M.; Sagnelli, E.; Stefani, S.; et al. Management of infections pre- and post-liver transplantation: Report of an AISF consensus conference. J. Hepatol. 2014, 60, 1075–1089. [Google Scholar] [CrossRef]
- Bertuzzo, V.R.; Giannella, M.; Cucchetti, A.; Pinna, A.D.; Grossi, A.; Ravaioli, M.; Del Gaudio, M.; Cristini, F.; Viale, P.; Cescon, M. Impact of preoperative infection on outcome after liver transplantation. Br. J. Surg. 2017, 104, e172–e181. [Google Scholar] [CrossRef] [Green Version]
- Heldman, M.R.; Ngo, S.; Dorschner, P.B.; Helfrich, M.; Ison, M.G. Pre- and post-transplant bacterial infections in liver transplant recipients. Transpl. Infect. Dis. Off. J. Transpl. Soc. 2019, 21, e13152. [Google Scholar] [CrossRef] [PubMed]
- Labenz, C.; Toenges, G.; Huber, Y.; Nagel, M.; Marquardt, J.U.; Schattenberg, J.M.; Galle, P.R.; Labenz, J.; Worns, M.A. Raised serum Interleukin-6 identifies patients with liver cirrhosis at high risk for overt hepatic encephalopathy. Aliment. Pharmacol. Ther. 2019, 50, 1112–1119. [Google Scholar] [CrossRef]
- Fernandez, J.; Claria, J.; Amoros, A.; Aguilar, F.; Castro, M.; Casulleras, M.; Acevedo, J.; Duran-Guell, M.; Nunez, L.; Costa, M.; et al. Effects of Albumin Treatment on Systemic and Portal Hemodynamics and Systemic Inflammation in Patients With Decompensated Cirrhosis. Gastroenterology 2019, 157, 149–162. [Google Scholar] [CrossRef] [Green Version]
- Piano, S.; Angeli, P. Bacterial Infections in Cirrhosis as a Cause or Consequence of Decompensation? Clin. Liver Dis. 2021, 25, 357–372. [Google Scholar] [CrossRef]
- Turco, L.; Garcia-Tsao, G.; Magnani, I.; Bianchini, M.; Costetti, M.; Caporali, C.; Colopi, S.; Simonini, E.; De Maria, N.; Banchelli, F.; et al. Cardiopulmonary hemodynamics and C-reactive protein as prognostic indicators in compensated and decompensated cirrhosis. J. Hepatol. 2018, 68, 949–958. [Google Scholar] [CrossRef]
- Starlinger, P.; Ahn, J.C.; Mullan, A.; Gyoeri, G.P.; Pereyra, D.; Alva-Ruiz, R.; Hackl, H.; Reiberger, T.; Trauner, M.; Santol, J.; et al. The Addition of C-Reactive Protein and von Willebrand Factor to MELD-Na Improves Prediction of Waitlist Mortality. Hepatology 2021. [Google Scholar] [CrossRef] [PubMed]
- Sieghart, W.; Pinter, M.; Hucke, F.; Graziadei, I.; Schoniger-Hekele, M.; Muller, C.; Vogel, W.; Trauner, M.; Peck-Radosavljevic, M. Single determination of C-reactive protein at the time of diagnosis predicts long-term outcome of patients with hepatocellular carcinoma. Hepatology 2013, 57, 2224–2234. [Google Scholar] [CrossRef]
- Yu, J.; Ye, Y.; Liu, J.; Xu, Y.; Lou, B.; Zhu, J.; Sheng, X.; Feng, X.; Pan, Q.; Yang, J.; et al. The role of hepatitis B core-related antigen in predicting hepatitis B virus recurrence after liver transplantation. Aliment. Pharmacol. Ther. 2019, 50, 1025–1036. [Google Scholar] [CrossRef] [PubMed]
- Shen, T.; Lin, B.Y.; Jia, J.J.; Wang, Z.Y.; Wang, L.; Ling, Q.; Geng, L.; Yan, S.; Zheng, S.S. A modified protocol with rituximab and intravenous immunoglobulin in emergent ABO-incompatible liver transplantation for acute liver failure. Hepatobiliary Pancreat. Dis. Int. HBPD INT 2014, 13, 395–401. [Google Scholar] [CrossRef]
- Garner, J.S.; Jarvis, W.R.; Emori, T.G.; Horan, T.C.; Hughes, J.M. CDC definitions for nosocomial infections, 1988. Am. J. Infect. Control 1988, 16, 128–140. [Google Scholar] [CrossRef]
- Moreau, R.; Jalan, R.; Gines, P.; Pavesi, M.; Angeli, P.; Cordoba, J.; Durand, F.; Gustot, T.; Saliba, F.; Domenicali, M.; et al. Acute-on-chronic liver failure is a distinct syndrome that develops in patients with acute decompensation of cirrhosis. Gastroenterology 2013, 144, 1426–1437. [Google Scholar] [CrossRef] [PubMed]
- Fine, J.P.; Gray, R.J. A Proportional Hazards Model for the Subdistribution of a Competing Risk. J. Am. Stat. Assoc. 1999, 94, 496–509. [Google Scholar] [CrossRef]
- Van den Broek, M.A.; Olde Damink, S.W.; Winkens, B.; Broelsch, C.E.; Malago, M.; Paul, A.; Saner, F.H. Procalcitonin as a prognostic marker for infectious complications in liver transplant recipients in an intensive care unit. Liver Transpl. Off. Publ. Am. Assoc. Study Liver Dis. Int. Liver Transpl. Soc. 2010, 16, 402–410. [Google Scholar] [CrossRef]
- Hara, T.; Soyama, A.; Takatsuki, M.; Hidaka, M.; Carpenter, I.; Kinoshita, A.; Adachi, T.; Kitasato, A.; Kuroki, T.; Eguchi, S. The impact of treated bacterial infections within one month before living donor liver transplantation in adults. Ann. Transpl. 2014, 19, 674–679. [Google Scholar] [CrossRef] [Green Version]
- Fuji, S.; Kim, S.W.; Fukuda, T.; Mori, S.; Yamasaki, S.; Morita-Hoshi, Y.; Ohara-Waki, F.; Heike, Y.; Tobinai, K.; Tanosaki, R.; et al. Preengraftment serum C-reactive protein (CRP) value may predict acute graft-versus-host disease and nonrelapse mortality after allogeneic hematopoietic stem cell transplantation. Biol. Blood Marrow Transpl. J. Am. Soc. Blood Marrow Transpl. 2008, 14, 510–517. [Google Scholar] [CrossRef] [Green Version]
- Kanda, J.; Mizumoto, C.; Ichinohe, T.; Kawabata, H.; Saito, T.; Yamashita, K.; Kondo, T.; Takakura, S.; Ichiyama, S.; Uchiyama, T.; et al. Pretransplant serum ferritin and C-reactive protein as predictive factors for early bacterial infection after allogeneic hematopoietic cell transplantation. Bone Marrow Transpl. 2011, 46, 208–216. [Google Scholar] [CrossRef] [Green Version]
- Sato, M.; Kako, S.; Oshima, K.; Sato, K.; Terasako, K.; Kimura, S.; Nakasone, H.; Okuda, S.; Yamazaki, R.; Higuchi, T.; et al. Prediction of infectious events by high-sensitivity C-reactive protein level before undergoing chemotherapy for acute myeloid leukaemia. Scand. J. Infect. Dis. 2010, 42, 97–101. [Google Scholar] [CrossRef]
- Sato, M.; Nakasone, H.; Wada, H.; Yamasaki, R.; Ishihara, Y.; Sakamoto, K.; Kawamura, K.; Ashizawa, M.; Machishima, T.; Terasako, K.; et al. Prediction of infectious events by the high-sensitivity C-reactive protein level before autologous hematopoietic cell transplantation for lymphoma and multiple myeloma. Transpl. Infect. Dis. Off. J. Transpl. Soc. 2013, 15, E169–E171. [Google Scholar] [CrossRef] [PubMed]
- Sato, M.; Nakasone, H.; Terasako-Saito, K.; Sakamoto, K.; Yamazaki, R.; Tanaka, Y.; Akahoshi, Y.; Nakano, H.; Ugai, T.; Wada, H.; et al. Prediction of infectious complications by the combination of plasma procalcitonin level and localized infection before allogeneic hematopoietic cell transplantation. Bone Marrow Transpl. 2014, 49, 553–560. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Jansen, C.; Moller, P.; Meyer, C.; Kolbe, C.C.; Bogs, C.; Pohlmann, A.; Schierwagen, R.; Praktiknjo, M.; Abdullah, Z.; Lehmann, J.; et al. Increase in liver stiffness after transjugular intrahepatic portosystemic shunt is associated with inflammation and predicts mortality. Hepatology 2018, 67, 1472–1484. [Google Scholar] [CrossRef] [PubMed]
- China, L.; Freemantle, N.; Forrest, E.; Kallis, Y.; Ryder, S.D.; Wright, G.; Portal, A.J.; Becares Salles, N.; Gilroy, D.W.; O’Brien, A.; et al. A Randomized Trial of Albumin Infusions in Hospitalized Patients with Cirrhosis. New Engl. J. Med. 2021, 384, 808–817. [Google Scholar] [CrossRef] [PubMed]
- Qin, N.; Yang, F.; Li, A.; Prifti, E.; Chen, Y.; Shao, L.; Guo, J.; Le Chatelier, E.; Yao, J.; Wu, L.; et al. Alterations of the human gut microbiome in liver cirrhosis. Nature 2014, 513, 59–64. [Google Scholar] [CrossRef]
- Schnabl, B.; Brenner, D.A. Interactions between the intestinal microbiome and liver diseases. Gastroenterology 2014, 146, 1513–1524. [Google Scholar] [CrossRef] [Green Version]
- Wiest, R.; Lawson, M.; Geuking, M. Pathological bacterial translocation in liver cirrhosis. J. Hepatol. 2014, 60, 197–209. [Google Scholar] [CrossRef] [Green Version]
- Sawas, T.; Al Halabi, S.; Hernaez, R.; Carey, W.D.; Cho, W.K. Patients Receiving Prebiotics and Probiotics Before Liver Transplantation Develop Fewer Infections Than Controls: A Systematic Review and Meta-Analysis. Clin. Gastroenterol. Hepatol. Off. Clin. Pract. J. Am. Gastroenterol. Assoc. 2015, 13, 1567–1574. [Google Scholar] [CrossRef]
- Scheithauer, T.P.; Dallinga-Thie, G.M.; de Vos, W.M.; Nieuwdorp, M.; van Raalte, D.H. Causality of small and large intestinal microbiota in weight regulation and insulin resistance. Mol. Metab. 2016, 5, 759–770. [Google Scholar] [CrossRef]
- Sarin, S.K.; Pande, A.; Schnabl, B. Microbiome as a therapeutic target in alcohol-related liver disease. J. Hepatol. 2019, 70, 260–272. [Google Scholar] [CrossRef] [Green Version]
- Albillos, A.; de Gottardi, A.; Rescigno, M. The gut-liver axis in liver disease: Pathophysiological basis for therapy. J. Hepatol. 2020, 72, 558–577. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chen, P.; Starkel, P.; Turner, J.R.; Ho, S.B.; Schnabl, B. Dysbiosis-induced intestinal inflammation activates tumor necrosis factor receptor I and mediates alcoholic liver disease in mice. Hepatology 2015, 61, 883–894. [Google Scholar] [CrossRef] [Green Version]
- Munoz, L.; Borrero, M.J.; Ubeda, M.; Conde, E.; Del Campo, R.; Rodriguez-Serrano, M.; Lario, M.; Sanchez-Diaz, A.M.; Pastor, O.; Diaz, D.; et al. Intestinal Immune Dysregulation Driven by Dysbiosis Promotes Barrier Disruption and Bacterial Translocation in Rats With Cirrhosis. Hepatology 2019, 70, 925–938. [Google Scholar] [CrossRef] [PubMed]
- Casulleras, M.; Zhang, I.W.; Lopez-Vicario, C.; Claria, J. Leukocytes, Systemic Inflammation and Immunopathology in Acute-on-Chronic Liver Failure. Cells 2020, 9, 2632. [Google Scholar] [CrossRef] [PubMed]
- Arroyo, V.; Angeli, P.; Moreau, R.; Jalan, R.; Claria, J.; Trebicka, J.; Fernandez, J.; Gustot, T.; Caraceni, P.; Bernardi, M.; et al. The systemic inflammation hypothesis: Towards a new paradigm of acute decompensation and multiorgan failure in cirrhosis. J. Hepatol. 2021, 74, 670–685. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| Variable | Exploratory Population | Validation Population | ||
|---|---|---|---|---|
| No CSI (n = 393) | CSI (n = 115) | No CSI (n = 338) | CSI (n = 94) | |
| Age (years) | 49 (42–57) | 51 (44–60) | 49 (40–55) | 48 (40–56) |
| Female | 67 (17.1%) | 26 (22.6%) | 53 (15.7%) | 22 (23.4%) |
| BMI (kg/m2) | 21.69 (19.93–24.13) | 22.36 (19.71–24.24) | 22.10(19.61–24.17) | 22.77(20.05–25.33) |
| Diabetes mellitus | 64 (16.3%) | 20 (17.4%) | 46 (13.6%) | 22 (23.4%) * |
| MELD at transplantation | 14.40 (9.90–22.88) | 25.11 (15.48–30.87) ** | 12.97 (9.23–22.09) | 24.82 (15.41–32.72) ** |
| Sodium (mEq/L) | 139 (136–141) | 138 (135–141) | 140 (137–142) | 138 (133–140) ** |
| Serum albumin (g/L) | 35.20 (31.90–38.90) | 33.20 (31.10–37.05) | 34.65(31.90–38.80) | 33.65(31.02–37.20) |
| White blood cell(109/L) | 4.40 (2.70–7.00) | 7.80 (4.50–11.20) ** | 4.30 (2.70–7.07) | 6.40 (4.32–10.65) ** |
| CRP (mg/L) | 7.40 (4.12–12.10) | 13.90 (9.89–26.95) ** | 7.29 (4.00–12.89) | 11.55 (7.84–25.47) ** |
| NLR | 3.50 (2.08–5.75) | 6.95 (3.31–10.87) ** | 3.55 (1.94–6.23) | 5.76 (2.90–10.44) ** |
| SII | 244 (123–476) | 495 (216–913) ** | 231 (121–447) | 421 (182–694) ** |
| Liver tumor | 171 (43.5%) | 28 (24.4%) ** | 164 (48.5%) | 27 (28.7%) ** |
| Underlying disease | ||||
| Viral | 338 (86.0%) | 88 (76.5%) * | 294 (87.0%) | 80 (85.1%) |
| Alcoholic | 86 (21.9%) | 24 (20.9%) | 67 (19.8%) | 19 (20.2%) |
| Autoimmune disease | 21 (5.3%) | 9 (7.8%) | 11 (3.3%) | 6 (6.4%) |
| Other disease | 15 (3.8%) | 12 (10.43%) ** | 19 (4.5%) | 3 (2.4%) |
| Previous abdominal surgery | 82 (20.9%) | 25 (21.7%) | 68 (20.1%) | 16 (17.0%) |
| Infection pre-transplant | 51 (13.0%) | 21 (18.3%) | 35 (10.4%) | 19 (20.2%) * |
| Organ failure number | ||||
| One or two | 128 (32.6%) | 53 (46.1%) ** | 77 (22. 8%) | 42 (44.7%) ** |
| Three or more | 14 (3.6%) | 28 (24.4%) ** | 25 (7.4%) | 24 (25.5%) ** |
| Donor age (years) | 38 (28–48.55) | 42 (32–51) | 36(28–47) | 41 (30–51) |
| Cold ischemia time (hours) | 9.50 (7.30–11.80) | 9.80 (7.60–12.20) | 9.50 (7.00–12.00) | 9.00 (7.40–11.57) |
| Duration of surgery (hours) | 5.40 (4.70–6.10) | 5.10 (4.55–6.35) | 5.40 (4.70–6.20) | 5.50 (4.62–6.50) |
| Blood loss (per 100 mL) | 10 (8–18) | 10 (6–19) | 10 (8–16) | 12 (8–20) |
| ABO incompatibility | 50 (12.7%) | 22 (19.1%) | 43 (12.7%) | 24 (25.5%) ** |
| Choledocho-jejunostomy | 1 (0.3%) | 5 (4.4%) ** | 3 (0.9%) | 2 (2.1%) |
| Type of infection | ||||
| Intra-abdominal | -- | 45 (39.1%) | -- | 45 (47.9%) |
| Pneumonia | -- | 59 (51.3%) | -- | 45 (47.9%) |
| Skin and soft-tissue | -- | 28 (24.3%) | -- | 17 (18.1%) |
| Urinary tract | -- | 2 (1.7%) | -- | 2 (2.1%) |
| Primary bloodstream | -- | 7 (6.1%) | -- | 6 (6.4%) |
| Variable | Exploratory Population | Validation Population | ||
|---|---|---|---|---|
| HR (95% CI) | p-Value | HR (95% CI) | p-Value | |
| NLR | 1.08 (1.06, 1.11) | <0.001 | 1.03 (1.01, 1.05) | 0.002 |
| WBC (109/L) | 1.06 (1.04, 1.07) | <0.001 | 1.08 (1.05, 1.11) | <0.001 |
| SII | 1.0004 (1.0002, 1.0006) | <0.001 | 1.0004 (1.0002, 1.0007) | 0.001 |
| CRP (mg/L) | 1.02 (1.02, 1.03) | <0.001 | 1.02 (1.01, 1.03) | <0.001 |
| Subgroup | Events/ Patients | HR (95% CI) | p-Value |
|---|---|---|---|
| Infection pre-transplant | |||
| No | 169/814 | 1.02 (1.01, 1.03) | <0.001 |
| Yes | 40/126 | 1.02 (1.01, 1.03) | 0.003 |
| Liver tumor | |||
| No | 154/550 | 1.03 (1.02, 1.04) | <0.001 |
| Yes | 55/390 | 1.02 (1.01, 1.03) | <0.001 |
| Organ failure number | |||
| None | 62/549 | 1.02 (1.02, 1.03) | <0.001 |
| One or two | 95/300 | 1.02 (1.01, 1.03) | 0.001 |
| Three or more | 52/91 | 1.02 (1.00, 1.03) | 0.014 |
| MELD scorequartile | |||
| Quartile 1 | 30/222 | 1.02 (1.01,1.03) | 0.003 |
| Quartile 2 | 20/243 | 1.02 (1.00,1.04) | 0.048 |
| Quartile 3 | 59/235 | 1.03 (1.02, 1.05) | <0.001 |
| Quartile 4 | 100/240 | 1.02 (1.02, 1.03) | <0.001 |
| Variable | Univariate Analysis | Multivariate Analysis | ||
|---|---|---|---|---|
| HR (95% CI) | p-Value | HR (95% CI) | p-Value | |
| Liver tumor | 0.46 (0.30, 0.70) | <0.001 | ||
| MELD at transplantation | 1.07 (1.05, 1.09) | <0.001 | 1.03 (0.99, 1.07) | 0.096 |
| Organ failure number (None) | Reference | Reference | ||
| One or two | 2.69 (1.75, 4.14) | <0.001 | 1.47 (0.74, 2.93) | 0.276 |
| Three or more | 8.81 (5.32, 14.59) | <0.001 | 3.49 (1.39, 8.75) | 0.008 |
| Donor age (years) | 1.01 (1.00, 1.03) | 0.082 | ||
| ABO incompatibility | 1.55 (0.98, 2.47) | 0.064 | ||
| Choledocho-jejunostomy | 6.27 (2.55, 15.42) | <0.001 | 8.04 (3.21, 20.15) | <0.001 |
| Serum albumin (g/L) | 0.97 (0.94, 1.00) | 0.082 | ||
| NLR | 1.08 (1.06, 1.11) | <0.001 | 1.03 (1.00, 1.06) | 0.079 |
| SII | 1.0004 (1.0003, 1.0006) | <0.001 | ||
| WBC (109/L) | 1.06 (1.04, 1.07) | <0.001 | ||
| CRP (mg/L) | 1.02 (1.01, 1.03) | <0.001 | 1.02 (1.01, 1.03) | <0.001 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Yu, J.; Shi, X.; Ma, J.; Chen, R.; Dong, S.; Lu, S.; Wu, J.; Yan, C.; Wu, J.; Zheng, S.; et al. C-Reactive Protein Is an Independent Predictor of 30-Day Bacterial Infection Post-Liver Transplantation. Biomolecules 2021, 11, 1195. https://doi.org/10.3390/biom11081195
Yu J, Shi X, Ma J, Chen R, Dong S, Lu S, Wu J, Yan C, Wu J, Zheng S, et al. C-Reactive Protein Is an Independent Predictor of 30-Day Bacterial Infection Post-Liver Transplantation. Biomolecules. 2021; 11(8):1195. https://doi.org/10.3390/biom11081195
Chicago/Turabian StyleYu, Jiong, Xiaowei Shi, Jing Ma, Ronggao Chen, Siyi Dong, Sen Lu, Jian Wu, Cuilin Yan, Jian Wu, Shusen Zheng, and et al. 2021. "C-Reactive Protein Is an Independent Predictor of 30-Day Bacterial Infection Post-Liver Transplantation" Biomolecules 11, no. 8: 1195. https://doi.org/10.3390/biom11081195