
Quantitative Assessment Method of Force Tracking Capabilities for Detection of Motor Intentional Disorders



Abstract
:1. Introduction
2. Force Tracking System
2.1. System Configuration
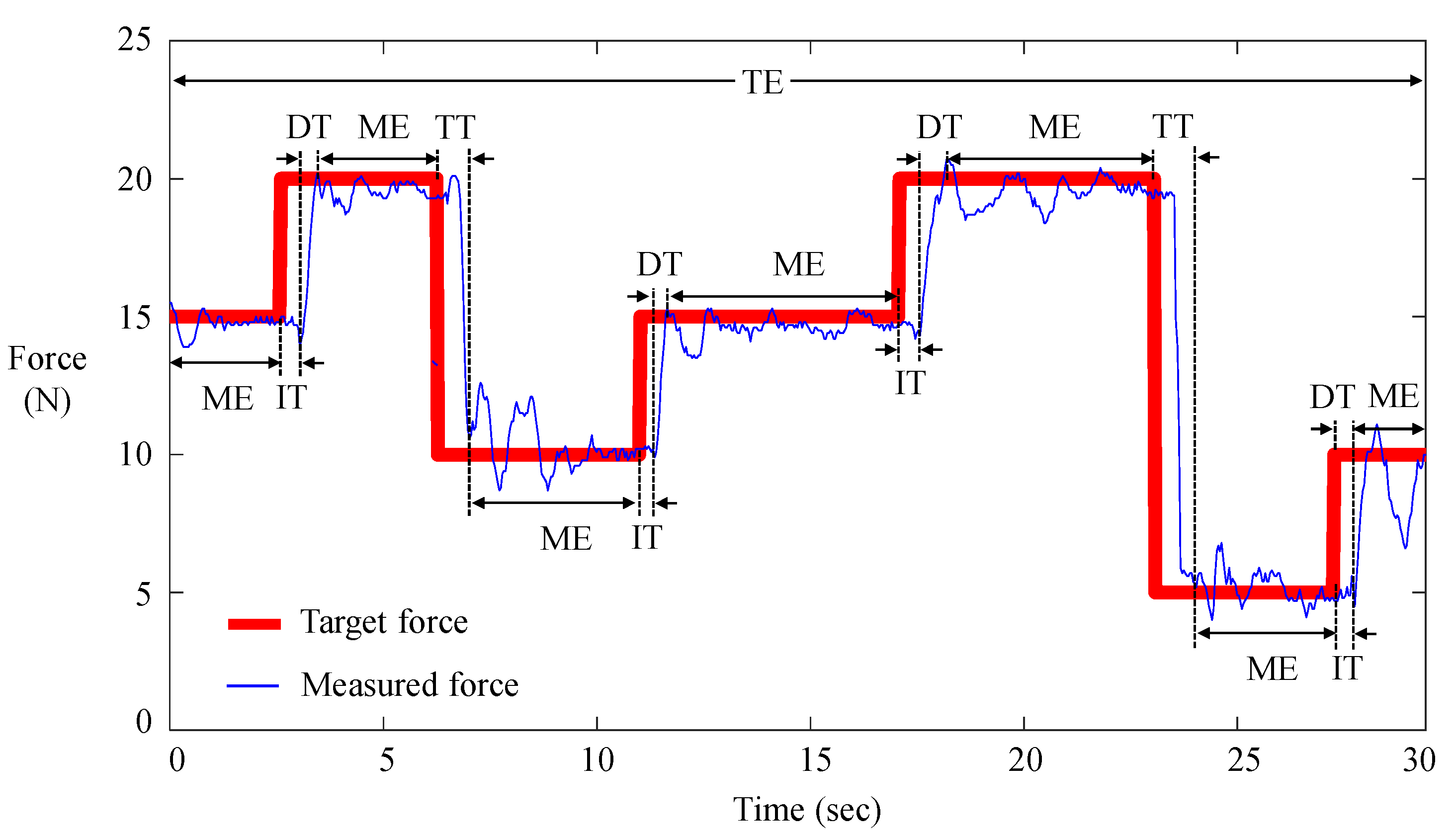
2.2. Quantification Protocol of Force Control Capabilities
2.3. System Configuration
3. Case Study
3.1. Participants
3.2. Experimental Design and Statistical Analysis
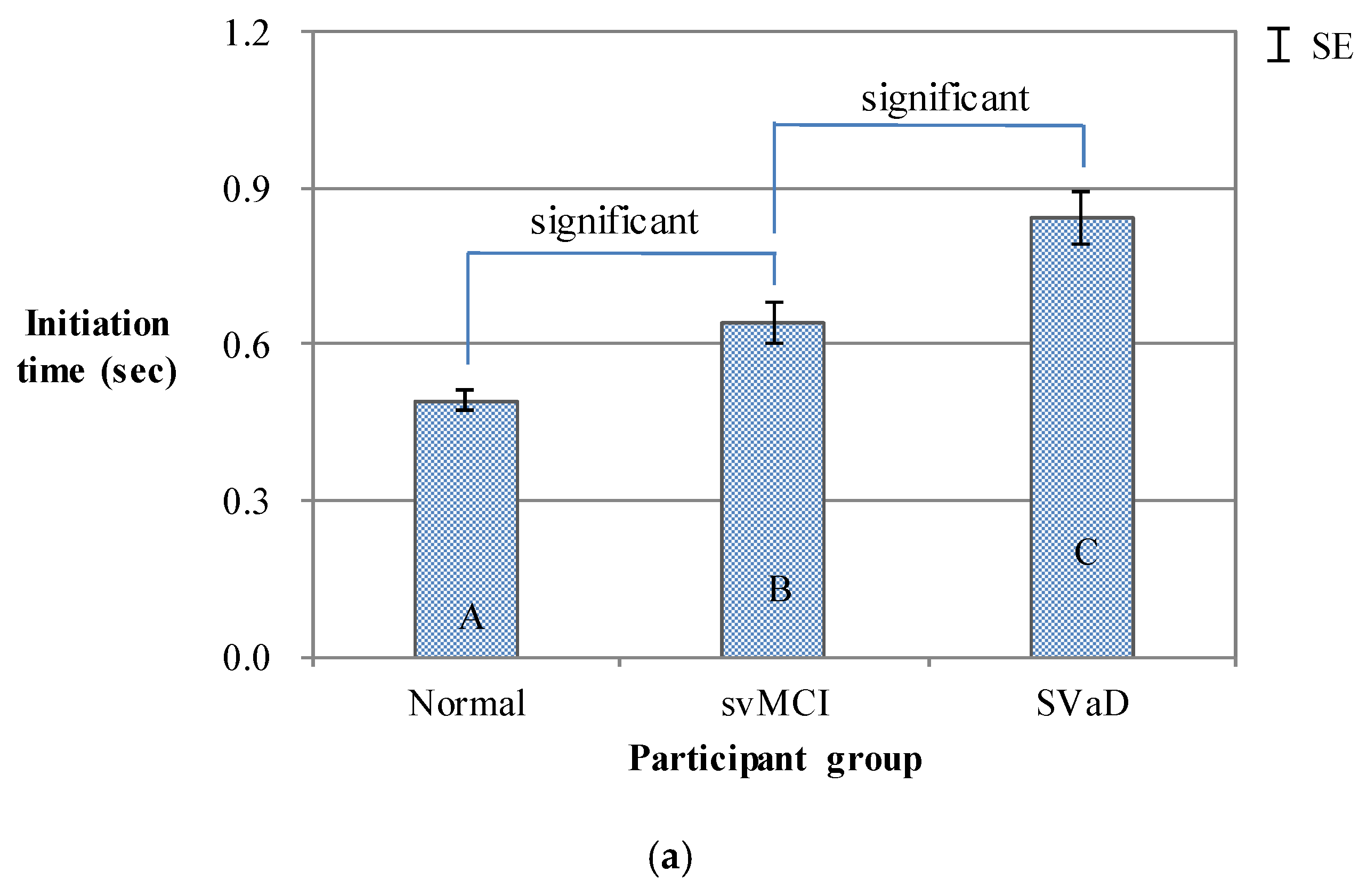
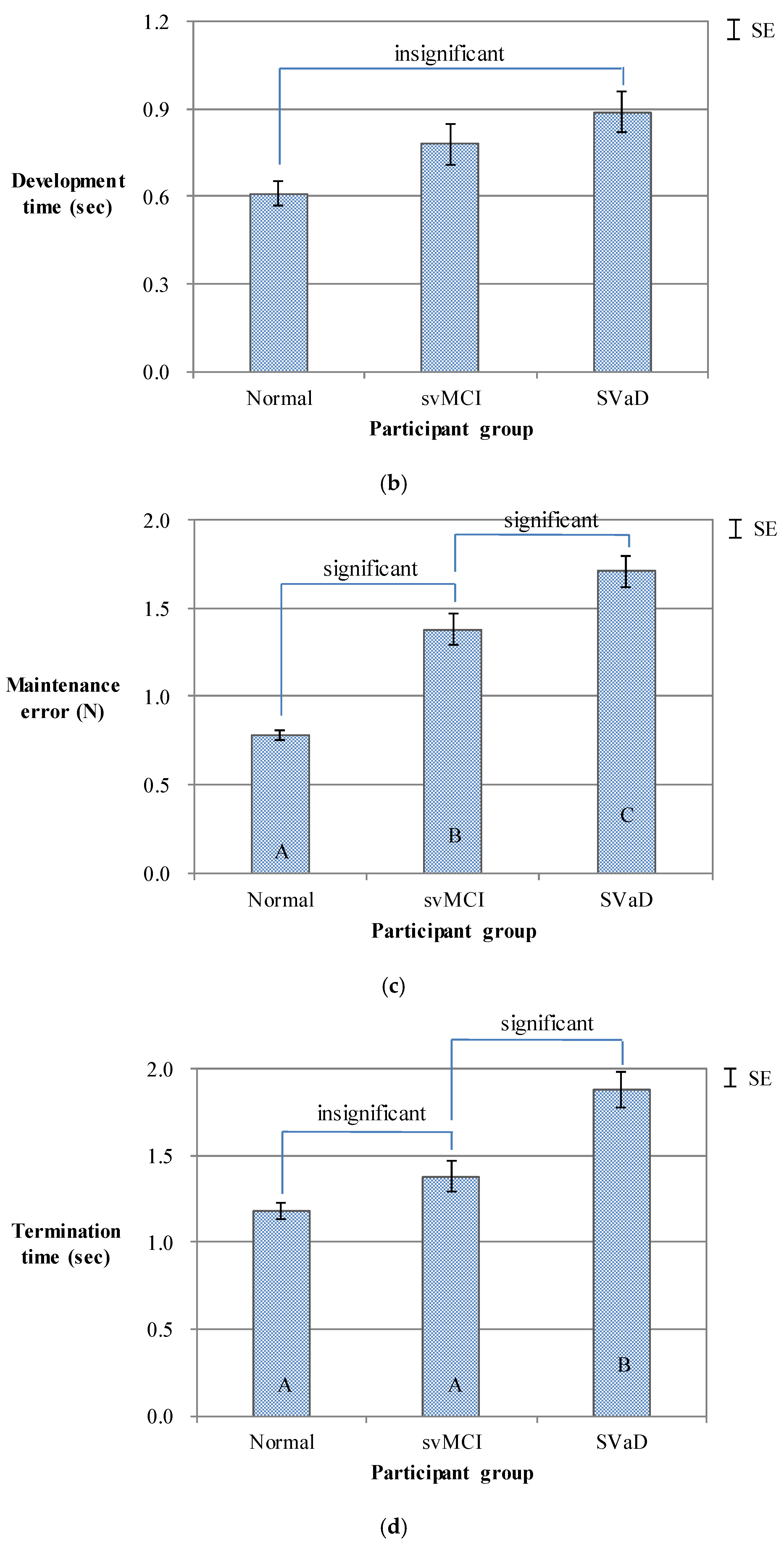
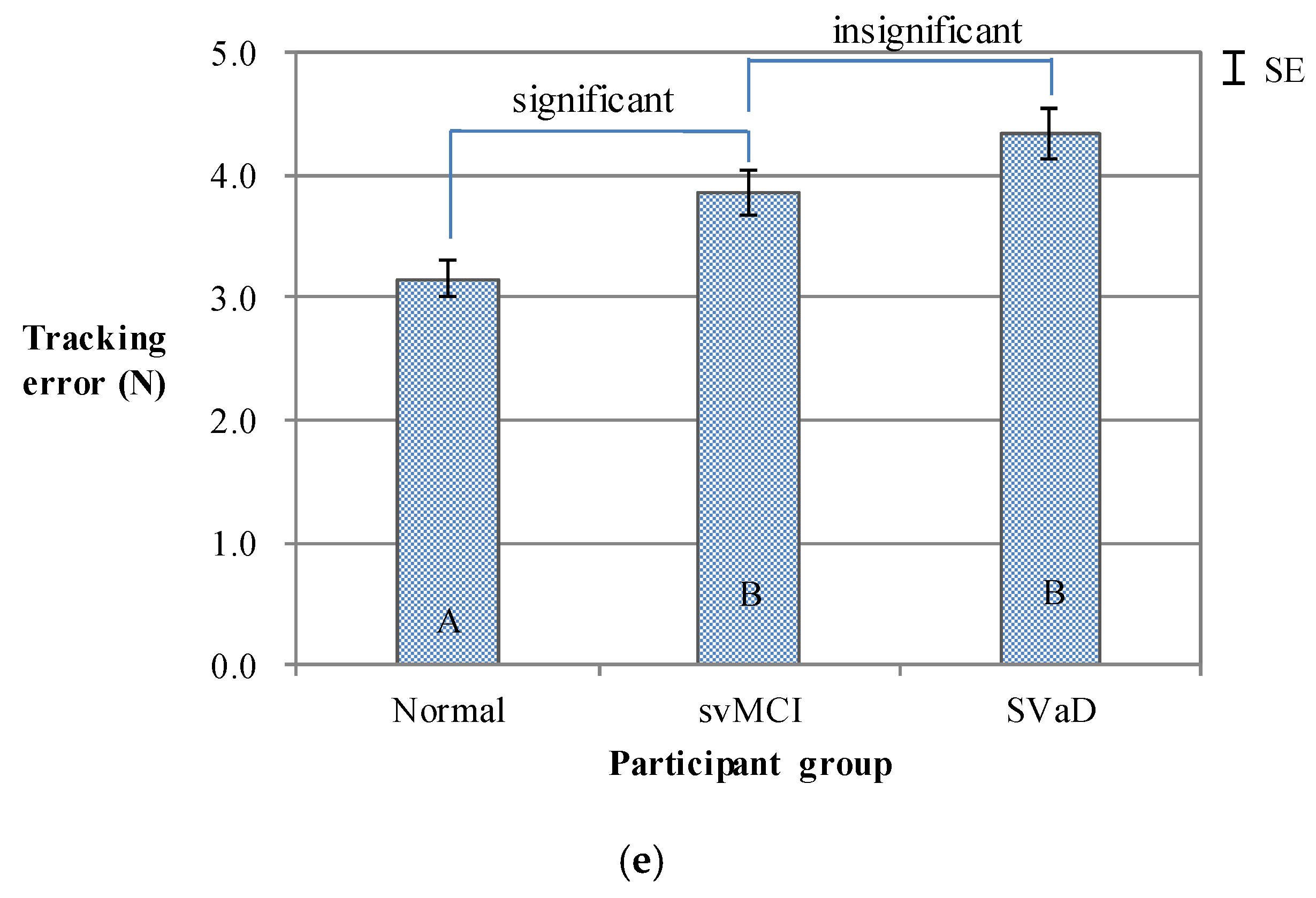
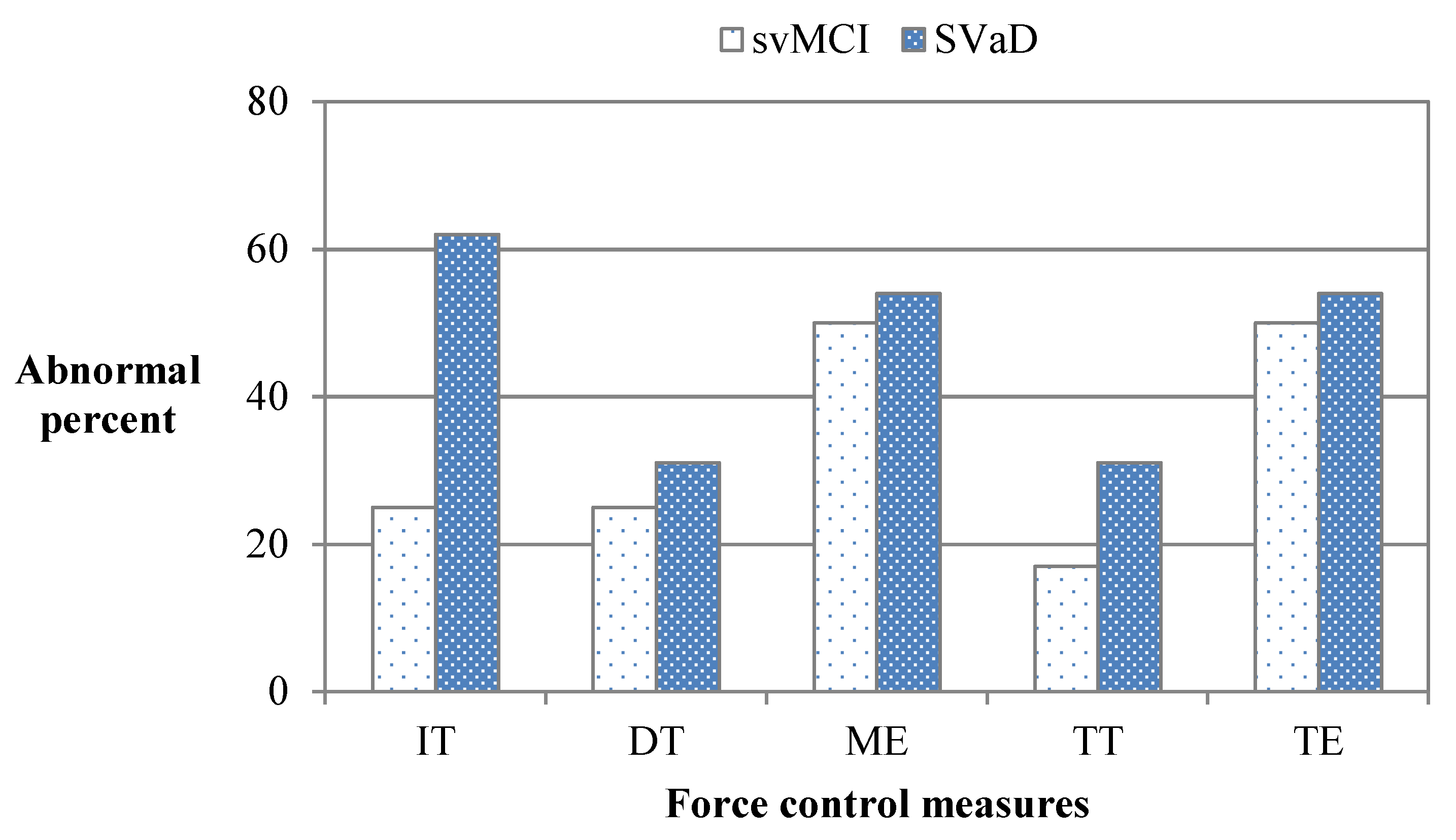
3.3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Heilman, K.M. Intentional neglect. Front. Biosci. 2004, 1, 694–705. [Google Scholar] [CrossRef] [PubMed]
- Heilman, K.M.; Watson, R.T.; Valenstein, E. Neglect and related disorders. In Clinical Neuropsychology; Heilman, K.M., Valenstein, E., Eds.; Oxford University Press: New York, NY, USA, 2012; pp. 296–348. [Google Scholar]
- Coslett, H.B.; Heilman, K.M. Hemihypokinesia after right hemisphere stroke. Brain Cogn. 1989, 9, 267–278. [Google Scholar] [CrossRef]
- Kertesz, A.; Nicholson, I.; Cancelliere, A.; Kassa, K.; Black, S.E. Motor impersistence: A right-hemisphere syndrome. Neurology 1985, 35, 662–666. [Google Scholar] [CrossRef] [PubMed]
- Crucian, G.P.; Heilman, K.M.; Junco, E.; Maraist, M.; Owens, W.E.; Foote, K.D.; Okun, M.S. The crossed response inhibition task in Parkinson’s disease: Disinhibition hyperkinesia. Neurocase 2007, 13, 158–164. [Google Scholar] [CrossRef] [PubMed]
- Buchanan, R.W.; Heinrichs, D.W. The Neurological Evaluation Scale (NES): A structured instrument for the assessment of neurological signs in schizophrenia. Psychiatry Res. 1989, 27, 335–350. [Google Scholar] [CrossRef]
- Chen, E.Y.H.; Shapleske, J.; Luque, R.; McKenna, P.J.; Hodges, J.R.; Calloway, S.P.; Hymas, N.F.; Dening, T.R.; Berrios, G.E. The Cambridge Neurological Inventory: A clinical instrument for assessment of soft neurological signs in psychiatric patients. Psychiatry Res. 1995, 56, 183–204. [Google Scholar] [CrossRef]
- Luria, A.R. L.S. Vygotsky and the problem of localization of functions. Neuropsychologia 1965, 3, 387–392. [Google Scholar] [CrossRef]
- Lee, B.; Park, H.; Jung, K.; Lee, B.H.; Na, D.L.; You, H. The effects of age, gender, and hand on finger force control capabilities. Hum. Factors 2015, 57, 1248–1358. [Google Scholar] [CrossRef] [PubMed]
- Seo, S.W.; Jung, K.; You, H.; Lee, B.H.; Kim, G.; Chung, C.; Lee, K.H.; Na, D.L. Motor-intentional disorders in right hemisphere stroke. Cogn. Behav. Neurol. 2009, 22, 242–248. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Yoon, D.S.; Jung, K.; Kim, G.H.; Kim, S.H.; Lee, B.H.; Seo, S.W.; You, H.; Na, D.L. Motor intentional disorders in vascular mild cognitive impairment and vascular dementia of subcortical type. Neurocase 2014, 20, 53–60. [Google Scholar] [CrossRef]
- Kim, S.H.; Seo, S.W.; Go, S.M.; Chin, J.; Lee, B.H.; Lee, J.H.; Han, S.H.; Na, D.L. Pyramidal and extrapyramidal scale (PEPS): A new scale for the assessment of motor impairment in vascular cognitive impairment associated with small vessel disease. Clin. Neurol. Neurosurg. 2011, 113, 181–187. [Google Scholar] [CrossRef] [PubMed]
- Seo, S.W.; Jung, K.; You, H.; Kim, E.J.; Lee, B.H.; Adair, J.C.; Na, D.L. Dominant limb motor impersistence associated with callosal disconnection. Am. Acad. Neurol. 2007, 68, 862–864. [Google Scholar] [CrossRef]
- Seo, S.W.; Ahn, J.; Yoon, U.; Im, K.; Lee, J.M.; Tae, K.S.; Ahn, H.J.; Chin, J.; Jeong, Y.; Na, D.L. Cortical thinning in vascular mild cognitive impairment and vascular dementia of subcortical type. J. Neuroimaging 2009, 20, 37–45. [Google Scholar] [CrossRef]
- Kim, G.H.; Seo, S.W.; Jung, K.; Kwon, O.; Kwon, H.; Kim, J.H.; Roh, J.H.; Kim, M.; Lee, B.H.; Yoon, D.S.; et al. The neural correlates of motor intentional disorders in patients with subcortical vascular cognitive impairment. J. Neurol. 2016, 263, 89–99. [Google Scholar] [CrossRef] [PubMed]
- Petersen, R.C.; Smith, G.E.; Waring, S.C.; Ivnik, R.J.; Tangalos, E.G.; Kokmen, E. Mild cognitive impairment: Clinical characterization and outcome. Arch. Neurol. 1999, 56, 303–308. [Google Scholar] [CrossRef] [PubMed]
- Erkinjuntti, T.; Inzitari, D.; Pantoni, L.; Wallin, A.; Scheltens, P.; Rockwood, K.; Roman, G.C.; Chui, H.; Desmond, D.W. Research criteria for subcortical vascular dementia in clinical trials. J. Neural Transm. Suppl. 2000, 59, 23–30. [Google Scholar]
- Hubner, L.; Godde, B.; Voelcker-Rehage, C. Older adults reveal enhanced task-related beta power decreases during a force modulation task. Behav. Brain Res. 2018, 345, 104–113. [Google Scholar] [CrossRef] [PubMed]
- Liu, C.; Li, C.; Yang, J.; Gui, L.; Zhao, L.; Evans, A.C.; Yin, X.; Wang, J. Characterizing brain iron deposition in subcortical ischemic vascular dementia using susceptibility-weighted imaging: An in vivo MR study. Behav. Brain Res. 2015, 288, 33–38. [Google Scholar] [CrossRef] [PubMed]
- Li, C.; Liu, C.; Yin, X.; Yang, J.; Gui, L.; Wei, L.; Wang, J. Frequency-dependent changes in the amplitude of low-frequency fluctuations in subcortical ischemic vascular disease (SIVD): A resting-state fMRI study. Behav. Brain Res. 2014, 274, 205–210. [Google Scholar] [CrossRef] [PubMed]
- Frisoni, G.B.; Galluzzi, S.; Bresciani, L.; Zanetti, O.; Geroldi, C. Mild cognitive impairment with subcortical vascular features: Clinical characteristics and outcome. J. Neurol. 2002, 249, 1423–1432. [Google Scholar] [CrossRef] [PubMed]
- Sun, Y.; Qin, L.; Zhou, Y.; Xu, Q.; Qian, L.; Tao, J.; Xu, J. Abnormal functional connectivity in patients with vascular cognitive impairment, no dementia: A resting-state functional magnetic resonance imaging study. Behav. Brain Res. 2011, 223, 388–394. [Google Scholar] [CrossRef] [PubMed]
- Kramer, A.F.; Colcombe, S. Fitness effects on the cognitive function of older adults: A meta-analytic study-revisited. Perspect. Psychol. Sci. 2018, 13, 213–217. [Google Scholar] [CrossRef] [PubMed] [Green Version]







{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Group | Gender | Age | |||
|---|---|---|---|---|---|
| Male | Female | Percentage of Male | Mean | SD | |
| Normal | 4 | 8 | 33% | 71.6 | 7.3 |
| svMCI | 6 | 5 | 55% | 74.5 | 5.6 |
| SVaD | 5 | 8 | 39% | 75.8 | 4.7 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Jung, K.; Lee, B.H.; Seo, S.W.; Yoon, D.S.; Lee, B.; Na, D.L.; You, H. Quantitative Assessment Method of Force Tracking Capabilities for Detection of Motor Intentional Disorders. Appl. Sci. 2021, 11, 3244. https://doi.org/10.3390/app11073244
Jung K, Lee BH, Seo SW, Yoon DS, Lee B, Na DL, You H. Quantitative Assessment Method of Force Tracking Capabilities for Detection of Motor Intentional Disorders. Applied Sciences. 2021; 11(7):3244. https://doi.org/10.3390/app11073244
Chicago/Turabian StyleJung, Kihyo, Byung Hwa Lee, Sang Won Seo, Doo Sang Yoon, Baekhee Lee, Duk L. Na, and Heecheon You. 2021. "Quantitative Assessment Method of Force Tracking Capabilities for Detection of Motor Intentional Disorders" Applied Sciences 11, no. 7: 3244. https://doi.org/10.3390/app11073244