1. Introduction
Essential trace elements, also known as trace minerals, are micronutrients that are needed in very small amounts through diet but are critical for the prevention of acute and chronic diseases [
1,
2]. Furthermore, because each essential trace element is linked to multiple enzymes, deficiency of one of these elements can contribute to a variety of metabolic abnormalities and clinical conditions such as diabetes, metabolic syndrome, and cardiovascular diseases, among many others [
1,
2,
3,
4,
5,
6,
7]. Even though recent research has demonstrated the significance of the essential trace element in common diseases, nutritional advice has focused on deficiencies that can occur in both acute and chronic diseases and knowledge on the potential risk effects of increased dietary intakes or supplements still remains limited [
5,
6,
7,
8,
9,
10,
11,
12,
13]. Essential trace element classification varies slightly depending on the criteria considered [
1,
2,
3,
4]. The World Health Organization classified zinc (Zn), copper (Cu), selenium (Se), manganese (Mn), chromium (Cr), cobalt (Co), iodine (I), and molybdenum (Mo) as essential trace elements in 1973 [
2]. Other elements, such as iron (Fe) and boron (B), were later added to this classification (Frieden’s Classification in 1981) [
2]. In this study, we will focus on four essential trace elements that are frequently investigated for their relationship with cardiovascular risk factors (Zn, Cu, Se, and Mn). Having a significant function as dietary antioxidant micronutrients, these trace elements are cofactors in a large number of enzymes that participate in the antioxidant defense system and are related to changes in the body’s homeostatic mechanisms, especially inflammation and oxidative stress, which are vital for optimum health [
14,
15,
16,
17,
18].
In addition to foods, these trace elements can also be obtained from drinking water and environmental/occupational exposures [
19,
20,
21,
22,
23]. However, it has been estimated that in the general population, diet is the primary factor strongly influencing daily intake of these essential elements [
24,
25]. Meat and meat products have been reported as the main dietary source of Zn exposure in many countries [
20,
26,
27,
28,
29,
30]. Other items supplying greater Zn in Western diets include cereals, milk and dairy products, nuts, and seeds [
31,
32]. Cereals, followed by fresh fruits and vegetables, were considered to be the main sources of Cu in Mediterranean subjects [
32,
33,
34]. In other populations, fruits, nuts, and cereals, in addition to tap water have been informed as good sources of dietary Cu [
30,
35]. Cereals and meat are the leading sources of Se intake in Mediterranean and Western populations, followed by fish, seafood, organ meats, nuts, milk, and dairy products [
31,
32,
33,
34,
36]. Foods richest in Mn are nuts and seeds, cereals, seafood, legumes, fruits, chocolate, coffee, and tea [
34,
37,
38,
39]. However, in addition to the trace elements naturally present in foods, it has been reported that the use of multimineral supplements is the most significant dietary determinant of their intake in certain populations [
40,
41]. Due to public perceptions that the deficiency of certain minerals is linked to diseases, the usage of multivitamin/multimineral supplements has expanded over the past few decades [
42,
43]. The initial studies demonstrating the important antioxidant properties of the trace elements Zn, Cu, Se, and Mn [
44,
45,
46,
47,
48] as well as the links between deficiencies of these trace elements and several diseases [
49,
50,
51,
52,
53,
54], contributed to this perception.
However, high levels of these trace elements may have adverse effects, including toxicity [
55,
56,
57,
58]. Thus, caution is required when increasing their intakes given the harmful effects when present in quantities exceeding those physiologically necessary. Thus, Zn acts as a pro-oxidant at a range of concentrations [
59]. Zn excess as well as deficiency are pro-oxidant conditions. High concentrations of Zn have been linked to zinc inhibition of antioxidant enzymes, which result in increased reactive oxygen species formation. The thresholds determining the Zn concentrations that affect its function as a pro-antioxidant and a pro-oxidant have not been properly established [
60]. Excessive Cu exposure tends to result in the overproduction of reactive oxygen species, which can cause oxidative-stress-induced cellular damage [
61]. High blood selenium levels can lead to selenosis [
62]. High Mn levels have been associated with increased oxidative stress and induced neurodegeneration [
63,
64]. The ability of Mn to enhance oxidative stress is due to the transition of its oxidative state +2 to +3, which increases its pro-oxidant capacity [
65]. However, the current emphasis is on the chronic effect of moderately high concentrations of these elements, given the growing evidence of an increased risk of cardiometabolic diseases such as diabetes, hypertension, dyslipidemias, and some cardiovascular outcomes [
66,
67,
68,
69,
70,
71,
72,
73,
74,
75,
76,
77]. Despite the large number of studies [
66,
67,
68,
69,
70,
71,
72,
73,
74,
75,
76] that show a direct relationship between Se, Cu, Zn, or Mn and cardiovascular risk factors, there are other studies that show no associations or even an inverse relationship [
51,
78,
79,
80,
81,
82,
83,
84]. Many factors can contribute to the disparities in the findings of various studies. The most important are population characteristics (sex, age, geographical origin, diet, pathologies, or even genetic factors), as well as the measurement used to assess trace element levels. Several investigations have been conducted to assess the amount of trace elements provided by the diet [
3,
21,
27,
29,
30,
31,
32,
33,
34,
35,
36,
37,
38,
39,
71,
78,
81]. However, it is well known that the content of trace elements in food varies greatly depending on the composition of the soil, water, and the environment [
2]. As a result, it is preferable to use other, more objective measures of Zn, Cu, Se, and Mn status, such as analyzing their concentrations in biological samples [
85,
86,
87,
88,
89,
90,
91]. For each trace element, there are different types of biomarkers in blood, plasma, urine, hair, adipose tissue, and nails. Each has its own set of advantages and disadvantages [
86,
87,
88,
89,
90,
91,
92,
93,
94]. Plasma/serum concentrations are the most commonly used, though there may be differences between studies.
Therefore, in the new era of personalized nutrition, greater emphasis must be placed on the characteristics of the population analyzed as well as on the proper interpretation of the biomarkers used in each study [
95]. The majority of published studies have concentrated on trace element analyses separately. However, the significance of analyzing several combined trace elements in what is known as “mixture” analysis has been emphasized because the concentration of one element can influence the effects of the other [
96,
97,
98,
99,
100]. Accordingly, current recommendations insist on conducting these combined analyses using novel statistical methodologies [
101,
102,
103]. With this context in mind, our goals are as follows: (1) To investigate the single associations between trace element concentrations in plasma and the main cardiovascular risk factors in a general Mediterranean population. (2) To analyze these single associations in urine. (3) To conduct combined analyses of the associations between trace elements and cardiovascular risk factors in this population using three approaches—principal components analysis, quantile-based g-computation, and the calculation of so-called trace element risk scores (TERS).
4. Discussion
In this cross-sectional study conducted on a Spanish Mediterranean population aged between 18 and 80 years, statistically significant associations were identified between plasma and/or urine concentrations of essential trace elements (Zn, Cu, Se, and Mn) and highly prevalent cardiovascular risk factors. There is currently much controversy about the protective or risk role of these essential trace elements on cardiovascular risk factors and diseases. This is because studies conducted on this topic over the past few decades have yielded inconsistent results [
69,
70,
71,
72,
73,
74,
75,
76,
77,
78,
79,
80,
81,
82,
83,
84,
85,
86,
87,
88,
89,
90,
91,
92,
93,
94,
95,
96,
97,
98]. Numerous variables [
50,
55,
56,
57,
58,
59,
60] can impact the different results of studies in this field. Among these are the characteristics of the population, such as age, gender, the presence of various pathologies, and geographical origin. Additionally, genetic factors can be relevant. Our research was focused on four essential trace elements (Zn, Cu, Se, and Mn) mostly obtained from diet [
2]. When comparing the results of different investigations, it is also important to know if the population evaluated had high or low concentrations of the trace elements examined, because depending on these levels, the effects can be different [
79,
80,
81,
82,
83,
84,
85,
86,
87,
88,
89,
90,
91]. In our Mediterranean population, the presence of these essential trace elements is relatively high [
83,
97,
113]. Particularly significant is the methodology for evaluating exposure to trace elements from food or other sources [
114,
115,
116]. Considering that the geographical origin influences the trace element content of foods, various biomarkers in biological samples are preferred as more objective measures. However, there is controversy regarding the optimal biomarkers for each trace element [
87,
88,
89,
90,
91,
92,
93,
94]. We measured the concentrations of Zn, Cu, Se, and Mn in plasma and urine at the same time. This gives us an advantage over other studies that only look at one type of biomarker. Moreover, the majority of previous research has concentrated on the analysis of trace element associations in isolation. However, it is known that the effect of these trace elements can be joint, enhancing or inhibiting each other [
95,
96,
98,
99], which is why statistical analyses of association taking into account the combinations of these elements have recently been recommended [
101,
102]. Several methodological approaches have been proposed for this, and it is advised to utilize a combination of them because there is no consensus regarding the most successful [
99]. A number of more traditional investigations have employed principal component analysis [
110] for investigating the combined effect of trace elements. However, this approach has several limitations and is being superseded by alternative solutions employing more artificial intelligence algorithms and other methods including shrinkage methods (least absolute shrinkage and selection operator, elastic network model, adaptive elastic-net model), Bayesian kernel machine regression, WQS regression, and quantile-based g-computation [
97,
100,
102,
103,
111,
117,
118,
119,
120]. In our population, we analyzed the associations between trace elements and cardiovascular risk factors using both the single-trace-element approach and the combined-trace element approach. For the combined analysis, we used three approaches including principal component analysis, quantile-based g-computation, and a simple score method so-called TERS. Using quantile-based g-computation, our study is the first to apply the combined analysis of trace elements and their association with cardiovascular risk factors in a Mediterranean population.
Before discussing the obtained results in greater detail, it is necessary to comment on some descriptive aspects of the population’s characteristics and the concentrations of the studied biomarkers. In this Mediterranean population, the mean plasma Zn concentrations are comparable with those observed in a previous study conducted in southern Spain [
121] and higher [
122,
123,
124] or lower [
125] than those described in other studies. Cu values in this Mediterranean population are slightly higher than those reported in southern Spain [
126] and in other populations [
124,
127]. Mean plasma levels of Se are comparable to previous studies [
124,
126,
128,
129]. In the case of Mn, mean plasma values in this Mediterranean population are within the range provided by several authors [
130,
131,
132], higher than those described in some previous studies [
124,
126,
129], and lower than those observed by Shen et al. [
128].
In urine, mean Zn values for this population are lower than those reported in the EPIC study [
124] in Brazil and [
133], but slightly higher than those reported by [
134] in women in the United States and in a previous study in Spain [
97]. Cu concentrations in the urine of this Mediterranean population are higher than those reported by [
124], comparable with those observed by [
97], and lower than those found by [
133,
135,
136]. The mean values for urinary Se are higher than those reported by [
133,
135,
136] but lower than those reported by [
134]. Likewise, Mn concentrations in urine were lower than those reported by [
133,
136,
137] but comparable with those reported by [
134].
When comparing the results of different studies, it is also crucial to examine the demographic features of the population. In our sample, we looked at differences in trace element based on sex and age. In several of the biomarkers studied, we found statistically significant differences between the sexes, but the most relevant were the sex differences in plasma levels of Zn and Cu. These findings are consistent with previous studies [
121,
126,
138,
139,
140,
141]. Regarding urinary concentrations by sex, in our study, we observed that urinary excretion of Zn, Cu, and Se is higher in men. No sex-specific differences were noted for Mn. Once more, no consensus has been found in the literature. In a comprehensive review on urinary excretion of Se, it can be observed that there is a lack of agreement and that urinary Se in men and women shows great variation depending on the study characteristics and the geographical area and content in food [
124,
142]. Other authors did not observe significant differences in urinary excretion of Se between men and women [
143].
The analysis of differences in the plasma concentrations of the trace elements with age revealed that Zn and Cu do not vary significantly in the present study, whereas plasma Se increased and plasma Mn decreased with age. However, the information available in the literature on this subject is contradictory. Some authors reported increases in Zn with age [
138], while others report decreases [
121,
140,
141]. In the case of Cu, some authors report increases with age [
140,
141], similar to Se [
126,
138,
139,
140]; however, [
144] found very low Se levels in very elderly people. In the case of plasma Mn, our findings agree with those of some researchers [
124,
140], whereas other authors found increases with age [
144,
145] or no changes [
126]. Regarding changes in urinary content of the trace elements with age, in our case it was found that Zn, Cu, and Se decreased with age, with no significant variations for Mn. Although there is no total agreement on urinary changes of these elements with age, the trend for the excretion of Se to decrease with age has been described by other authors [
143] and has been linked to greater likelihood of the malnutrition and organic damage that come with age [
146]. However, in a study undertaken in Brazil, a negative correlation between serum concentrations of several minerals and age was reported, but no significant differences were observed in urine levels by age [
147]. Due to these potential differences by sex and age, we adjusted the models of the associations with cardiovascular risk factors for these two variables in subsequent statistical analyses to avoid a possible confounding effect.
Since plasma concentrations of Zn, Cu, Se, and Mn are the most widely used and accepted biomarkers for these trace elements [
86,
87,
88,
89,
90,
91,
92,
93], we began our investigation into the relationship between trace elements and cardiovascular risk factors by analyzing plasma levels of these elements. In this Mediterranean population, correlations between plasma concentrations and urine concentrations of these biomarkers were found to be quite weak. Depending on the biomarker utilized, these low correlations may account for the disparity in results across published studies [
48,
49,
50,
51,
52,
53,
54,
55,
56,
57,
58,
59,
60,
61,
62,
63,
64,
65,
66,
67,
68,
69,
70,
71,
72,
73,
74,
75,
76,
77,
78,
79,
80,
81,
82,
83,
84]. Although the majority of published studies analyzed plasma, serum, or blood concentrations, other studies used urine biomarkers [
97,
124,
127,
128,
129,
130,
131,
132,
133]. In the single-trace-element association analysis, we identified a number of statistically significant associations between cardiovascular risk factors and trace elements. Multivariable adjusted models revealed a statistically significant association between plasma Cu and plasma triglycerides, as well as plasma Cu and BMI or waist circumference. However, there was no statistically significant association between plasma Zn levels and the cardiovascular risk factors investigated. No significant associations were obtained for plasma Zn concentrations in the multivariable adjusted model despite the fact that some inverse associations were detected in the unadjusted model. There is currently no agreement on the plasma levels of these elements and their relationship with circulating lipids, blood pressure, fasting glucose, BMI, and/or cardiovascular disease. Rotter et al. [
148] positively correlated Zn with circulating triglycerides and Se with total cholesterol, LDL-cholesterol, and triglycerides. Other authors inversely related low circulating levels of Zn with systemic inflammatory activity [
80], and with dyslipidemia in the presence of hypertension and hypercholesterolemia [
149]. High Cu levels have been linked with hypertriglyceridemia in newborns [
150], cardiovascular risk [
77], and a positive correlation between Cu levels and total cholesterol and HDL-cholesterol has been described [
151]. However, other authors found no correlation between plasma Cu and Zn and lipid parameters [
125,
152]. Several studies demonstrate a positive correlation between elevated plasma zinc levels and diabetes or glucose at fasting [
153,
154]. However, in this Mediterranean population, no significant associations were found between plasma Zn levels and these parameters. Other authors found no association between diabetes and the levels of Zn or other trace elements [
148,
151], even an inverse association with glycated hemoglobin has been reported [
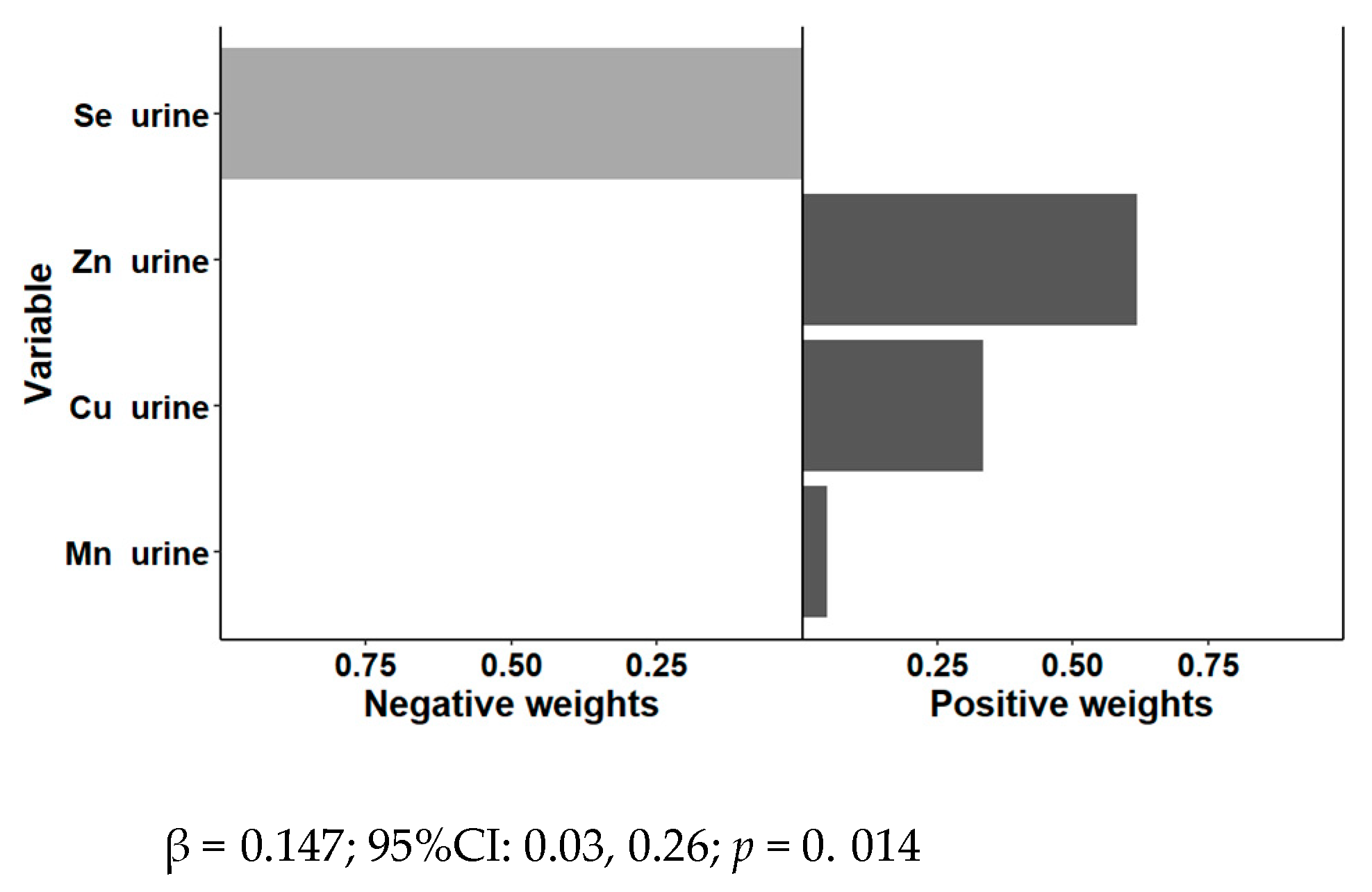
155]. Interestingly, despite not detecting statistically significant associations between plasma Zn concentrations and fasting glucose or diabetes risk, we identified a highly significant positive association between urine Zn concentrations and these parameters in our population. Many other studies have found a link between urinary Zn concentrations and glycemia/diabetes [
94,
155,
156,
157]. However, the mechanisms underlying this association between Zn concentrations in urine and fasting glucose, but not in plasma, remain unclear. It has been reported that individuals with insulin-dependent diabetes have approximately doubled urinary zinc excretion than controls [
158]. This is paradoxical because it has been reported that Zn may help reduce the onset or progression of type 2 diabetes through a variety of mechanisms involving both insulin secretion and peripheral tissue action [
159]. However, a suggested mechanism to explain the increased concentrations in urine is that high plasma glucose levels may interfere with the active transport of Zn in renal tubule cells, increasing Zn excretion from the body through urine [
160]. However, more research is needed. Additional prospective epidemiological and mechanistic studies should be conducted to better elucidate the associations of Zn plasma and urine levels with fasting glucose and type 2 diabetes risk [
161].
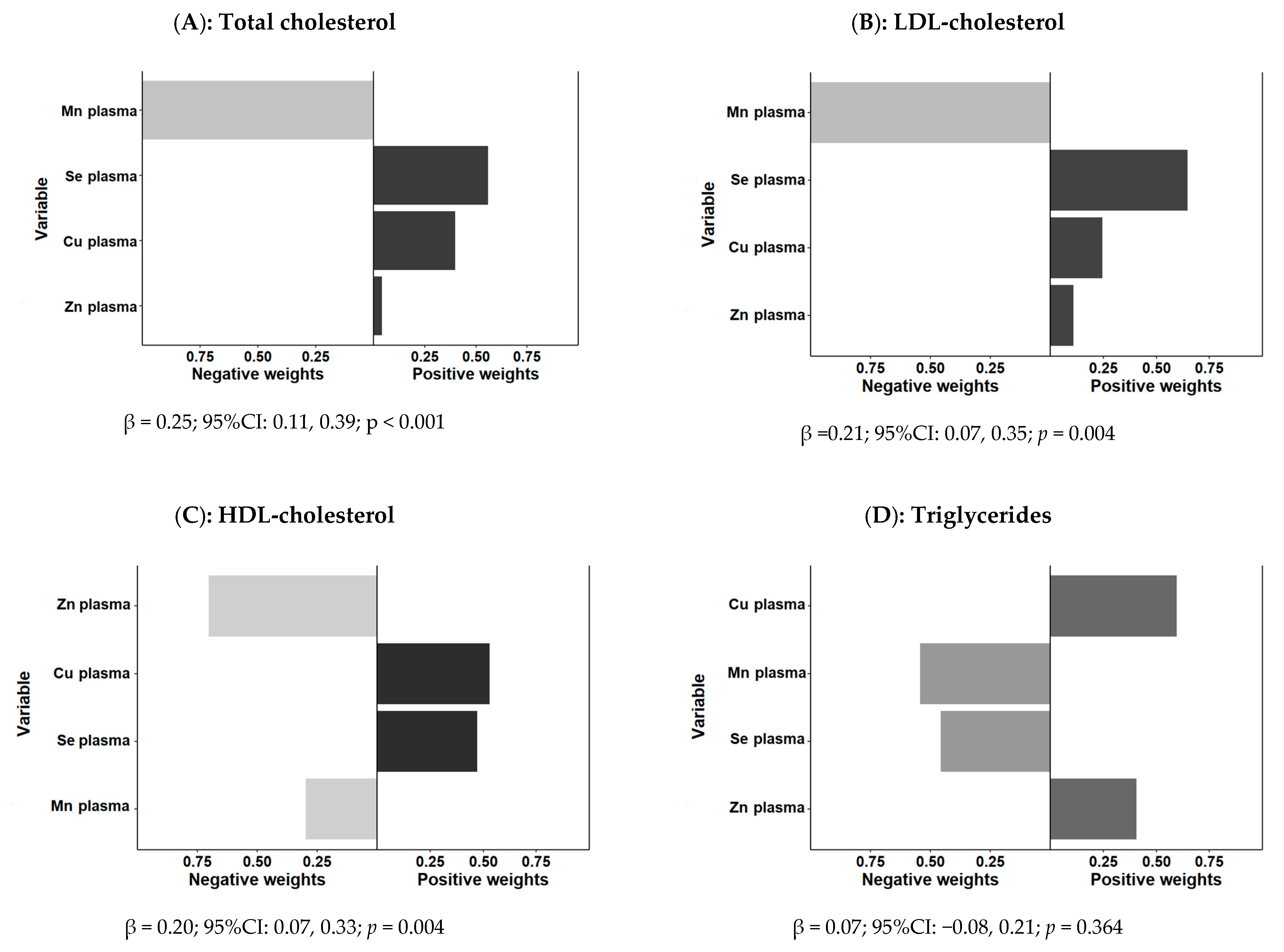
We found the most statistically significant and consistent associations between selenium in plasma and plasma lipid concentrations, primarily total cholesterol and LDL-cholesterol concentrations. Despite the fact that selenium was once assumed to be a potent cardiovascular-protective antioxidant with inverse associations with cardiovascular risk factors [
79], numerous studies published in populations from the United States, Europe, and even Asia have observed direct associations between higher plasma concentrations of selenium and increases in plasma concentrations of total cholesterol and LDL-cholesterol [
51,
66,
67,
68,
72,
82,
162]. Although our results are consistent with observational epidemiological research conducted in the so-called Se replete populations, the mechanism by which greater plasma Se concentrations are linked to hypercholesterolemia remains unclear. It is feasible that a U-shaped link exists between plasma Se concentrations and hypercholesterolemia, in that both low and high Se concentrations would have negative effects on plasma lipids [
163,
164]. A Se deficit may correlate to a decreased general synthesis of selenoproteins, and this may correspond to an increased oxidative stress and its repercussions in the lipid metabolism (alteration in redox balance, altered protein function, and abnormalities in cardiovascular relevant lipid signaling pathways, among others). Similarly, high plasma Se levels may be associated with the maximal activation of particular selenoproteins, resulting in a compensatory response towards the pro-oxidant effects of Se as well as unfavorable effects in some lipid signaling pathways [
164].
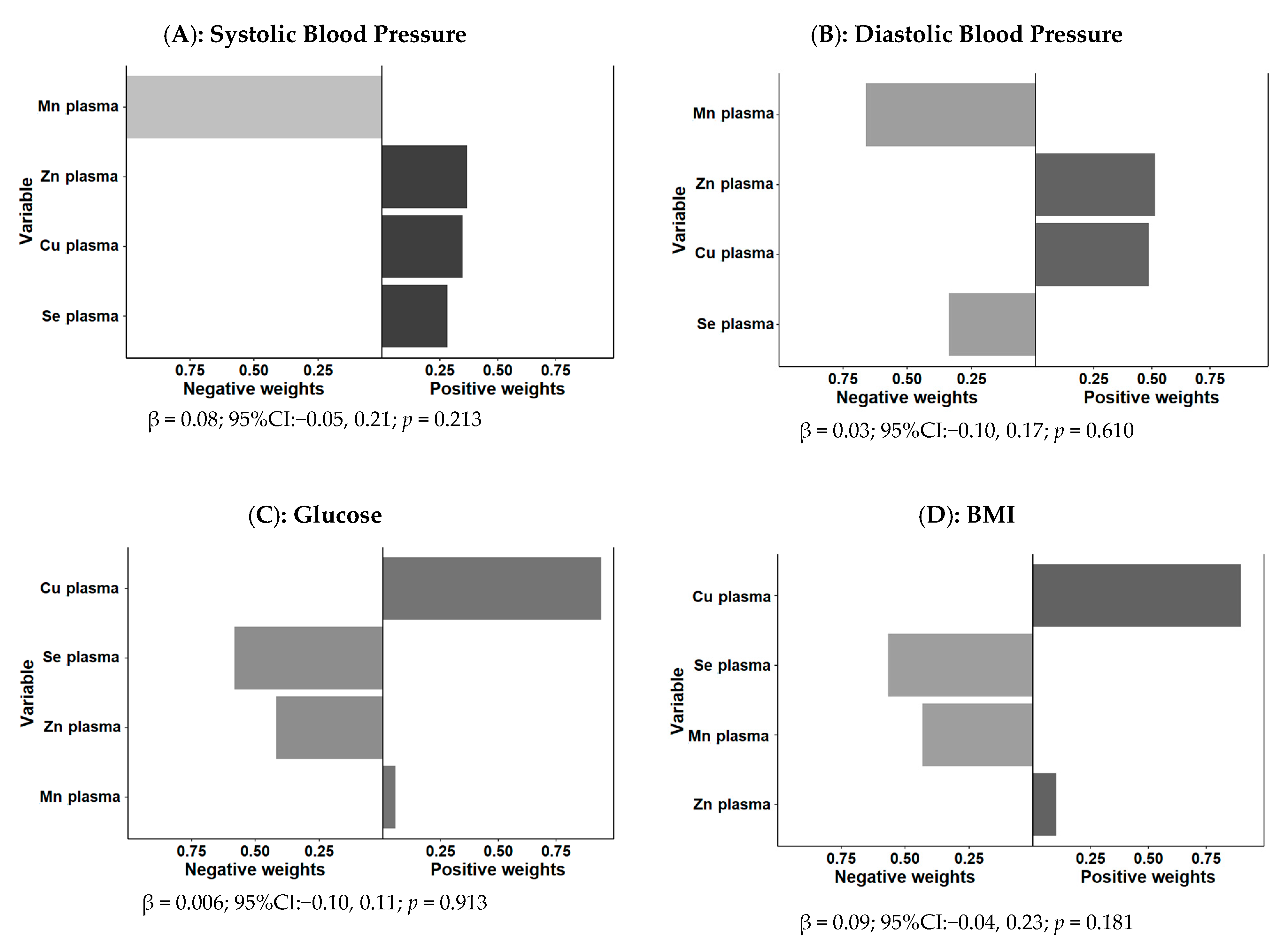
In addition to the strong associations between plasma Se and hypercholesterolemia, we detected a statistically significant association between plasma Se and SBP in our Mediterranean population. However, we did not detect significant associations with fasting glucose or diabetes. Other researchers have found associations between plasma Se and blood pressure or diabetes but the findings are inconsistent [
67,
70,
71,
79,
82]. In the single-trace-element study, plasma Mn was not significantly associated with any cardiovascular risk factor but presented inverse coefficients with many of them. It has been described that the highest Mn serum levels are associated with a lower presence of prediabetes and diabetes in elderly Chinese women but this correlation is found in men when Mn levels are moderate [
131].
Regarding BMI and waist circumference, we detected several statistically significant associations with plasma levels in the single-trace-element analysis. However, the associations were in opposite directions (direct associations for plasma Cu and inverse associations for Se). Published studies were also contradictory for plasma trace elements and anthropometric variables, reporting inverse, null, or direct relationships depending on the population [
121,
126,
148,
153,
154,
162,
165,
166,
167,
168].
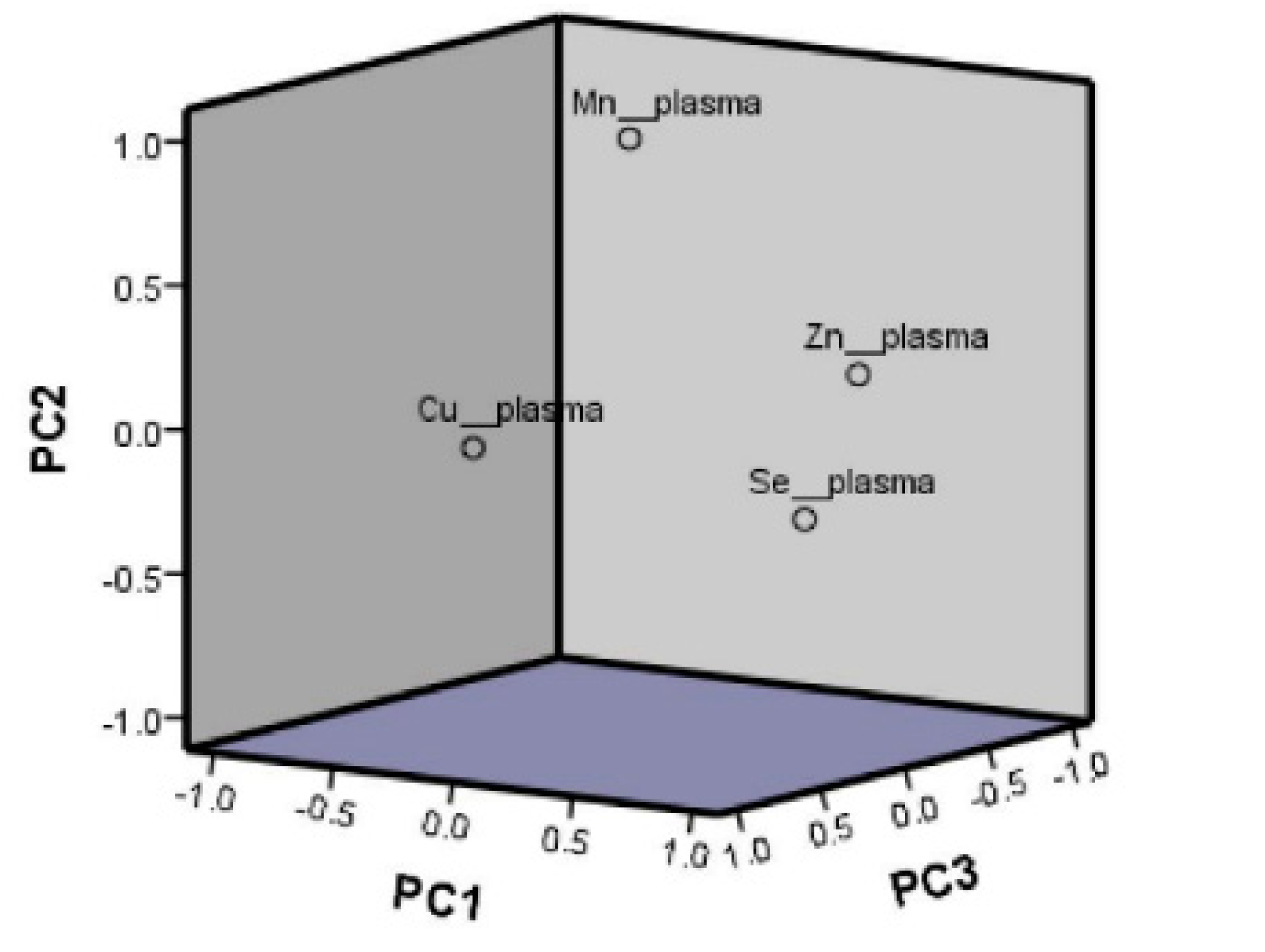
In the combined-trace-element analysis, we used three approaches: a principal component analysis, the quantile-based g-computation, and the construction of a simple score so-called TERS. We conducted the combined analysis with the three approaches separately for plasma and urine and compared the results. Finally, we used the quantile-based g-computation to jointly analyze plasma and urine biomarkers. Quantile-based g-computation is a novel method proposed to specifically address the inherent complexities of high-dimensional mixture data and to estimate the joint effect of the analyzed chemicals [
103]. It builds upon previous mixture-based regression models such as weighted quantile sum regression [
111]. However, quantile-based g-computation has more advantages, including that does not require a directional homogeneity assumption that all exposures have an effect in the same direction, as modeled in other approaches [
102]. Although in the last two years a number of studies employing this approach for the combined analysis of exposure to trace elements have been published [
98,
99,
100,
117,
118,
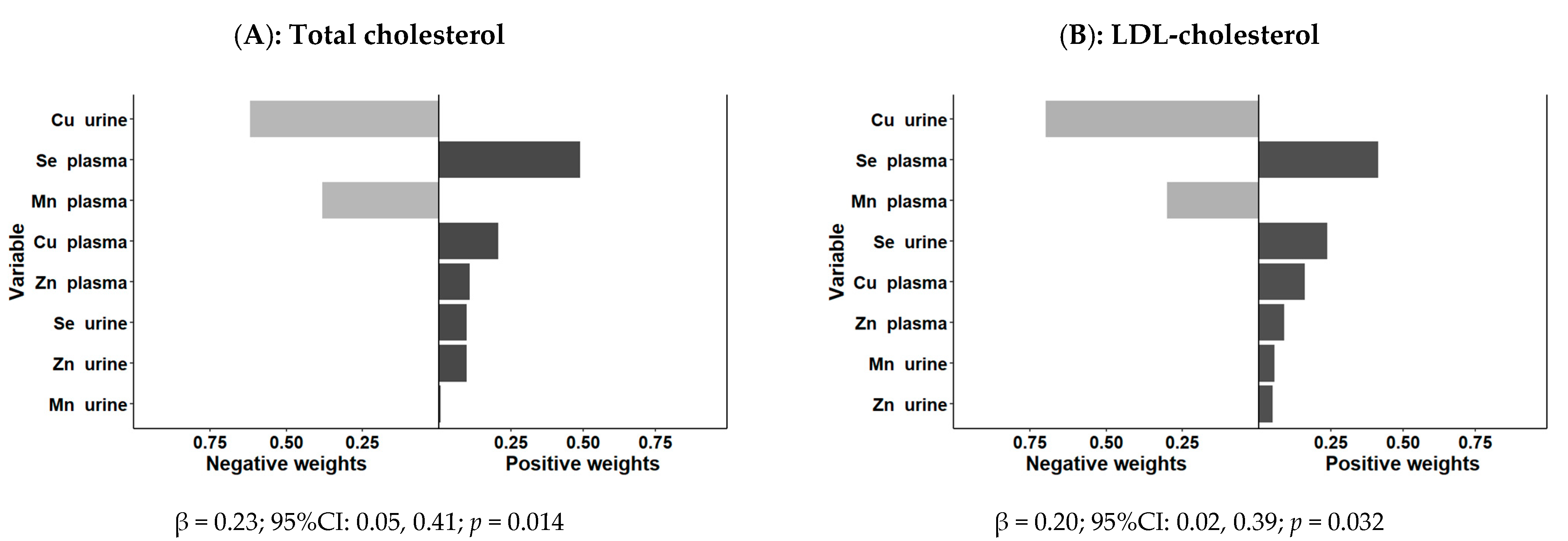
169], its use is still limited, and there are few published relationships with cardiovascular risk variables to which we can compare our findings. The results of our study’s combined analysis of trace element biomarkers in plasma using quantile-based g-computation were very enlightening. We were able to detect several statistically significant combined associations using this method. Among them is the joint association of the trace elements studied with total cholesterol and LDL-cholesterol concentrations. Perhaps most notably, it has made it possible to easily identify heterogeneity in the associations of different trace elements in combined analyses. We found that none of the cardiovascular risk factors investigated in the combined analysis had all of the trace elements acting in the same direction, increasing the risk. There are elements that, depending on the risk factor studied, have an inverse or direct influence. For example, in the case of total cholesterol, Se, Cu, and Zn all contribute to an increase in risk, whereas Mn decreases it. We were able to validate these findings by using TERS, a new method based on a score of tertiles of trace element concentrations in urine that we developed. In urine, the combined analysis using the quantile-based g-computation approach was very informative regarding the joint exposure effect and yielded statistically significant results for fasting glucose concentrations and diabetes. Again, heterogeneity among the trace elements was detected (Se inversely related and the others directly related). This significant association was also detected in our TERS approach. Finally, we explored the joint association between plasma and urine biomarkers with cardiovascular risk factors and observed statistically significant results for total cholesterol and LDL-cholesterol, revealing a strong association. Given the effects of these plasma lipids and fasting glucose on cardiovascular risk, a better understanding of the individual and combined effects of plasma and urine biomarkers is required for more personalized nutritional advice.
Our research has both strengths and limitations. Among the study’s strengths is that it was conducted on a well-defined general population, which included participants aged 18 to 80 years from a Mediterranean country. In addition, potential confounders have been accounted for in the statistical models. Moreover, we used both a single-trace-element statistical approach and a combined approach to capture the joint influence on the cardiovascular risk variables analyzed. Nonetheless, our study has a number of limitations. The first limitation is that it is a cross-sectional study, from which no causal inferences can be drawn. Similarly, because this is an epidemiological study, we do not analyze the potential mechanisms underlying the statistical relationships identified. Further mechanistic research is required to comprehend the potential mechanisms underlying each statistical association reported. Another limitation is the number of trace materials studied. We investigated Zn, Cu, Se, and Mn; however, it is well known that Fe is another essential trace element that plays a key role in oxidative-stress- and age-related diseases [
170,
171]. Fe is vital to numerous biological functions, and Fe deficiency or excess can result in a variety of medical conditions related to cardiovascular risk factors or diseases. However, more research is needed at the population level due to the mixed results [
172,
173,
174,
175]. It would have been highly interesting to add iron concentration analysis in this Mediterranean population, both for its research as a separate trace element and in the combined joint analysis; therefore, it will be evaluated for further research. Another limitation of the study is that oxidative stress biomarkers have not been determined. Currently, the so-called derivatives-reactive oxygen metabolites (d-ROMs) [
176,
177,
178] are an emerging biomarker of oxidative stress, and their measurement would have offered highly interesting information to relate it to the concentrations of trace elements and to the investigated cardiovascular risk factors. Finally, we did not analyze the genetic factors that may influence cardiovascular risk, which is still another limitation of our study. Several genetic polymorphisms are currently known to be associated with higher concentrations of plasma lipids (i.e., polymorphisms in the APOE gene determining LDL-c levels), blood glucose (i.e., polymorphisms in the TCF7L2 gene), body mass index (i.e., polymorphisms in the FTO gene), and other cardiovascular risk factors [
179,
180,
181,
182,
183]. More recently, associations of cardiovascular risk factors with microbiota-related polymorphisms have been reported [
184]. For all of these reasons, it would have been interesting to investigate if markers of higher or lower genetic risk can modulate the effect of the trace element concentrations on cardiovascular risk phenotypes. A bigger sample size is required for these gene–environment interaction investigations; therefore, we will continue to work in the future.

 ,
, 






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}