3.2. Performance of Proposed ECG Acquisition Sensor
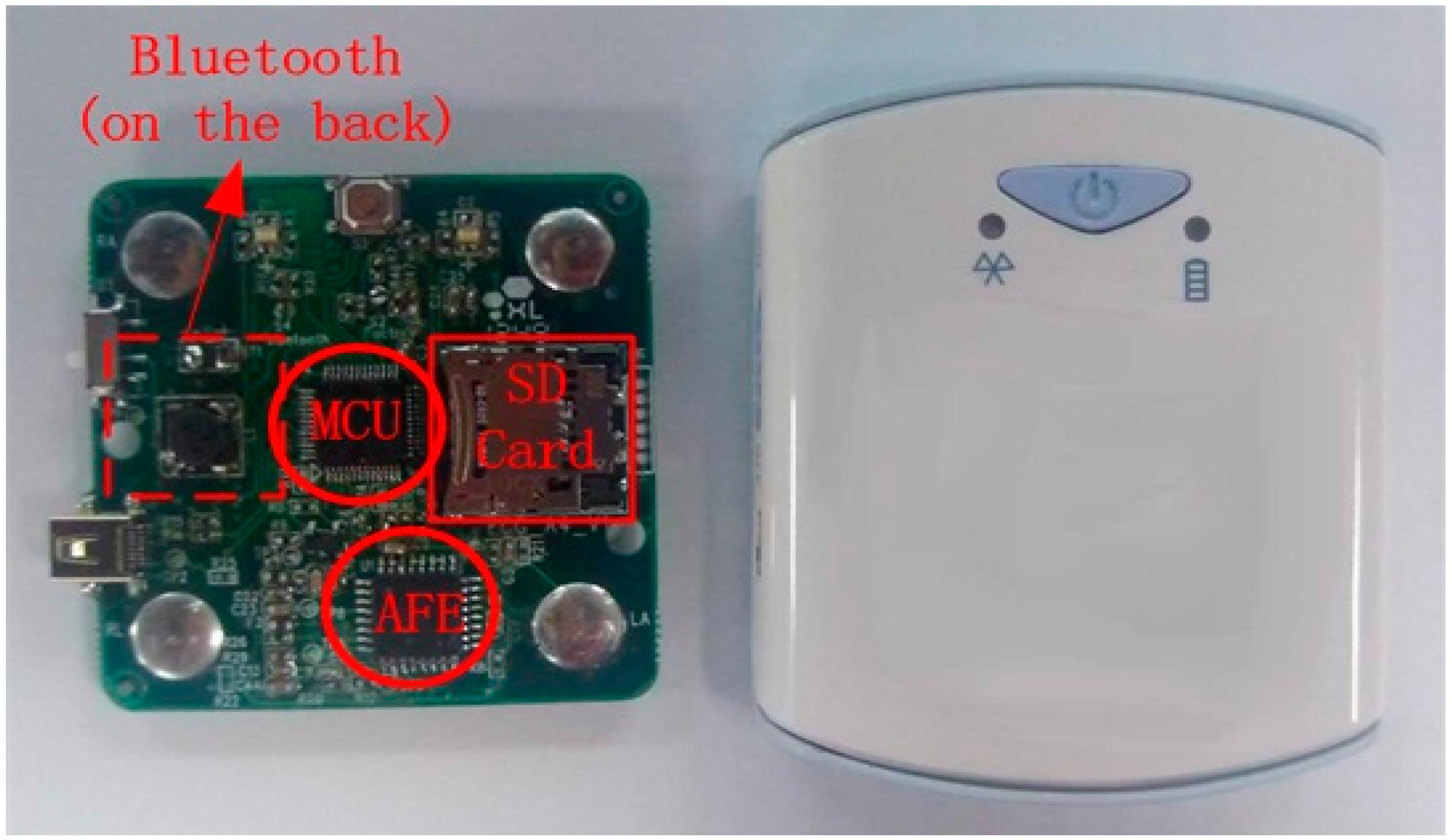
Figure 7 shows the photograph of proposed acquisition sensor at the left and its appearance of final package. The sensor is very small for wearable monitoring application with a size of only 58 × 50 × 10 mm and a weight of 20 g.
Figure 7.
Photograph of proposed ECG Acquisition device.
Figure 7.
Photograph of proposed ECG Acquisition device.
Figure 8.
ECG acquisition sensor hardware validation procedure.
Figure 8.
ECG acquisition sensor hardware validation procedure.
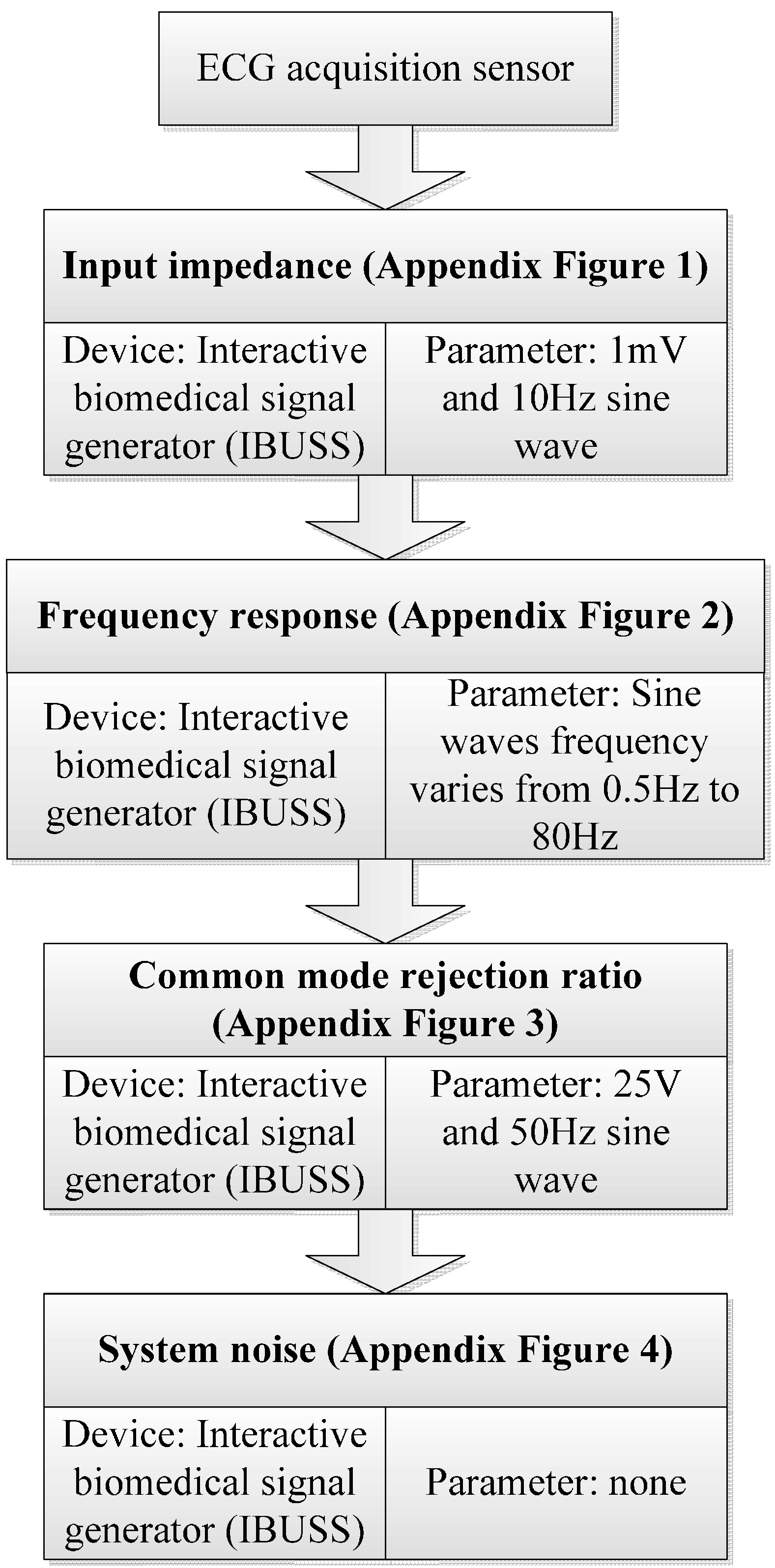
To validate the hardware performance of the proposed ECG sensor, we evaluated four main indexes including input impedance, frequency response, anti-jaming capability and system noise. The test procedure and corresponding device and setting parameters for all the indexes can be found in
Figure 8.
Table 1 gives a summary of the performance. The testbed for input impedance is presented in
appendix Figure 1. The skew rate of 1% has demonstrated the performance in input impedance with the input impedance larger than 5 MΩ, and thus is in accordance with YY1139-2000.
Appendix Figure 2 gives the testbed for frequency response. The sine waves with frequency varying from 0.5 Hz to 80Hz were inputted sequentially to verify the performance of frequency response. We evaluated the antijaming capability in terms of CMRR, which can be found in
appendix Figure 3. The screen height of 4.2 mm demonstrated the CMRR was larger than 85 dB, and thus complied with YY1139-2000 perfectly. The testbed for system noise is presented in
appendix Figure 4, a screen height of 0.4 mm showed the system noise was less than 15 μV, and also adhered to the rule in YY1139-2000.
Table 1.
Performance summary of the ECG sensor hardware.
Table 1.
Performance summary of the ECG sensor hardware.
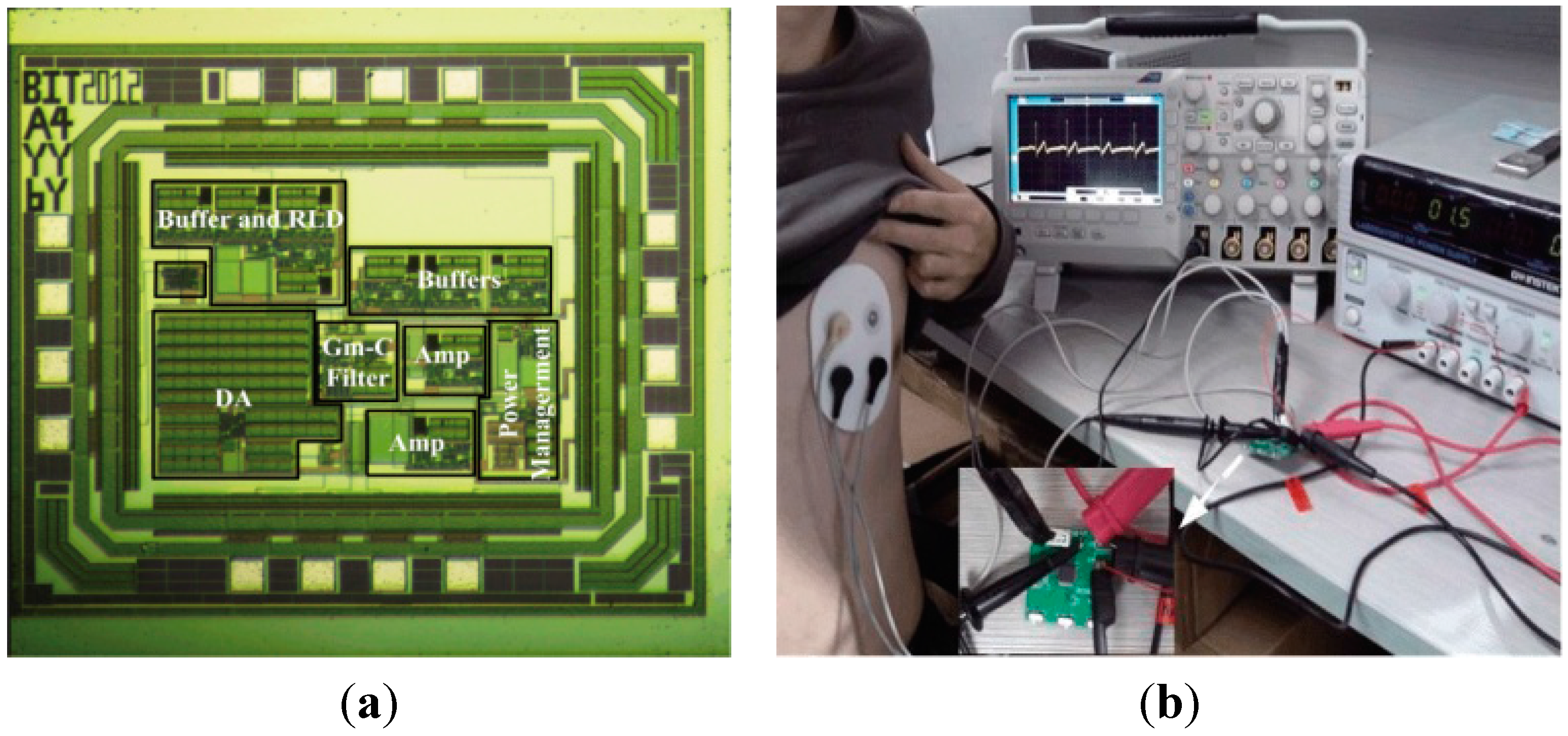
| Technology | CMOS 0.18 μm |
| Supply Voltage | 3 V |
| Chip Size | 1.3 mm × 1.1 mm |
| Input Impedance | >5 MΩ |
| Frequency Response | <20 Hz for 8 inputted frequency |
| CMRR | >85 dB |
| System Noise | <15 μV |
| Gain | 360 |
| Sampling Rate | 150 Hz, 250 Hz, 500 Hz |
| Data Bit-Width | 32 bit |
As the power consumption is a very important parameter for long-term continuously monitoring, we evaluated the total power consumption including AFE, MCU, SD card and other modules. The testbed for computing the power is demonstrated in
Figure 6b, in which a DC power supply (GPS-2303C) is used to generate the voltage and an oscilloscope to exhibit the output current. The power is computed by product of the voltage and the current under the voltage. The power consumption computation was performed on each module separately and then the total device from a 3 V supply. For example, with the power supply of 3 V, this AFE consumes around 100 µA typically and its shutdown current is less than 1 µA, and thus the power consumption is 0.3 mW. For the long term monitoring or home-based application scenario, we don’t need to view the real-time signal but transmit the data once a day. So the wireless module is off at most time and the power consumption can be ignored while discussing the total power dissipation of the system.
Table 2 summarizes the power consumption of the proposed acquisition device and each module separately. It can be seen that the presented device only consumes around 12.5 mW total power dissipation, and the proposed AFE only consumes 2.4% of total power consumption. The main part of power consumption focus on the SD card, due to the writing process. However, the process of writing the acquired ECG data to SD card only takes tens of milliseconds, in most of time it is inactive.
Table 2.
Power consumption of the proposed ECG acquisition device.
Table 2.
Power consumption of the proposed ECG acquisition device.
| | AFE | MCU | SD Card | Power Module and Other Circuits |
|---|
| Power Dissipation (mW) | 0.3 | 2.67 | 6 (on average) | 3.53 |
| Power Dissipation (%) | 2.4 | 21.36 | 48 | 28.24 |
| Total Power (mW) | 12.5 |
| Device Lifetime | 30 h (one 130 mAh AA battery) |
Table 3 summarizes the comparison of this work with other recent similar works and some commercial products in the market. In which the power consumption of other works are evaluated based on their data sheets. It can be seen that this work performs better than other works in those proposed aspects. In the future, the performance of higher CMRR, lower power consumption and lower noise, lower weight is our objective.
To validate the reliability of the proposed sensor on acquiring ECG data, we evaluated the sensor following the procedures presented in [
29]. The validation protocol is comprised of two phases: The first phase is a laboratory test for evaluating the performance of the proposed sensor using an ECG signal generator; the second phase is a real-life experiment on subjects while performing a standard procedure including sitting, sit-to-stand, standing, stand-to-sit using the BIOPAC MP150 multi-channel physiological instrument.
Table 3.
Performance comparison between our system and other recent similar works.
Table 3.
Performance comparison between our system and other recent similar works.
| | This Work | Sensors 2013[30] | ISITME 2011 | IEEE EMBC 2006 [31] | Holter ECG System (TLC4000) [32] | Holter Recording (DMS3004A) [33] |
|---|
| Channel | 1 | 1 | 1 | 3 | 12 | 12 |
| Size | 5.8 × 5.0 × 1.0 cm3 | 5.8 × 5.0 × 0.4 cm3 (Without Package) | 5.5 × 3.4 × 1.6 cm3 (Without Package) | N/A | N/A | 8.8 × 5.5 × 2.1 cm3 |
| Supply (V) | 3 | 3 | 3.3 | 3 | 3 | 1.5 |
| Power (mW) | 12.5 | 84.83 | 115 | 375 | 312.5 | 25 |
| Storage | SD Card | SD Card | N | SD Card | Build-in memory | Build-in memory |
| Weight (g) | 20 | 38 (exclude battery) | 20.7 (exclude battery) | N/A | N/A | 100 |
In the first phase, simulated ECG signals with six rates varying from 30 to 200 BPM and four amplitudes from 0.15 to 1 mV were generated by the ECG generator. Each signal was recorded firstly by attaching the BIOPAC to the ECG generator to acquire 50 ECG waveforms for each amplitude and frequency setting, then the same measurements were repeated using the proposed sensor. The testbed is presented in
appendix Figure 5a. We compared the two sets of signals in terms of cross-correlation coefficient of the signal and the QRS amplitude ratio, which can be seen in
Table 4 and
Table 5. From
Table 4 and
Table 5 we can see, the signals acquired from the proposed sensor are almost identical to those generated from the ECG generator. In the second phase, seven healthy subjects (five males and two females) were recruited to perform the following typical daily activities presented in
Table 6 sequentially for 3 times. The baseline characteristics of the experimental subjects are: age 24.4 ± 6.05 years, height 173.7 ± 5.3 cm, and body mass index 21.1 ± 2.3 kg/m
2. BIOPAC and the proposed sensor were used to collect the ECG signals simultaneously and the testbed is presented in
appendix Figure 5b. We compared the acquired ECG signals between the BIOPAC and the proposed sensor in terms of QRS detection error, QRS amplitude ratio, QRS cross correlation and QRS detection delay, which were defined in [
29]. The test results are presented in
Table 7. From
Table 7 we can see, the signals acquired from the proposed sensor are closely correlated to those collected from standard device in real-life settings.
Table 4.
Average signal cross correlation between ECG generator device and the proposed sensor.
Table 4.
Average signal cross correlation between ECG generator device and the proposed sensor.
| | Frequency (BPM) | 30 | 60 | 80 | 120 | 160 |
|---|
| Amplitudes (mV) | |
|---|
| 0.15 | 0.985 | 0.983 | 0.983 | 0.984 | 0.985 |
| 0.3 | 0.983 | 0.985 | 0.984 | 0.984 | 0.983 |
| 0.5 | 0.984 | 0.983 | 0.983 | 0.986 | 0.983 |
| 1 | 0.983 | 0.984 | 0.983 | 0.984 | 0.985 |
Table 5.
Average QRS amplitude ratio between ECG generator device and the proposed sensor.
Table 5.
Average QRS amplitude ratio between ECG generator device and the proposed sensor.
| | Frequency (BPM) | 30 | 60 | 80 | 120 | 160 |
|---|
| Amplitudes (mV) | |
|---|
| 0.15 | 1 | 1 | 1 | 1 | 1 |
| 0.3 | 1 | 1 | 1 | 1 | 1 |
| 0.5 | 1 | 1 | 1 | 1 | 1 |
| 1 | 1 | 1 | 1 | 1 | 1 |
Table 6.
Daily life activity.
Table 6.
Daily life activity.
| Activity | Time Duration |
|---|
| Sitting | 30 s |
| Sit-to-Stand | 5 s |
| Standing | 30 s |
| Stand-to-Sit | 5 s |
Table 7.
Performance comparison between the proposed sensor and BIOPAC in real-life setting.
Table 7.
Performance comparison between the proposed sensor and BIOPAC in real-life setting.
| | Performance | QRS Detection Error No. (Avg ± std) | QRS Amplitude Ratio (Avg ± std) | QRS Cross Correlation (Avg ± std) | QRS Detection Delay No. (Avg ± std) |
|---|
| Activity | |
|---|
| Sitting | 0.825 ± 0.836 | 0.987 ± 0.154 | 0.928 ± 0.137 | 0.687 ± 0.704 |
| Sit-to-Stand | 0.259 ± 0.117 | 1.082 ± 0.057 | 0.896± 0.106 | 0.524 ± 0.442 |
| Standing | 0.793 ± 0.689 | 1.061 ± 0.072 | 0.908 ± 0.174 | 0.712 ± 0.812 |
| Stand-to-Sit | 0.296 ± 0.124 | 0.899 ± 0.043 | 0.886 ± 0.157 | 0.465 ± 0.385 |
3.4. Performance of the Proposed Context-Aware ECG Monitoring System
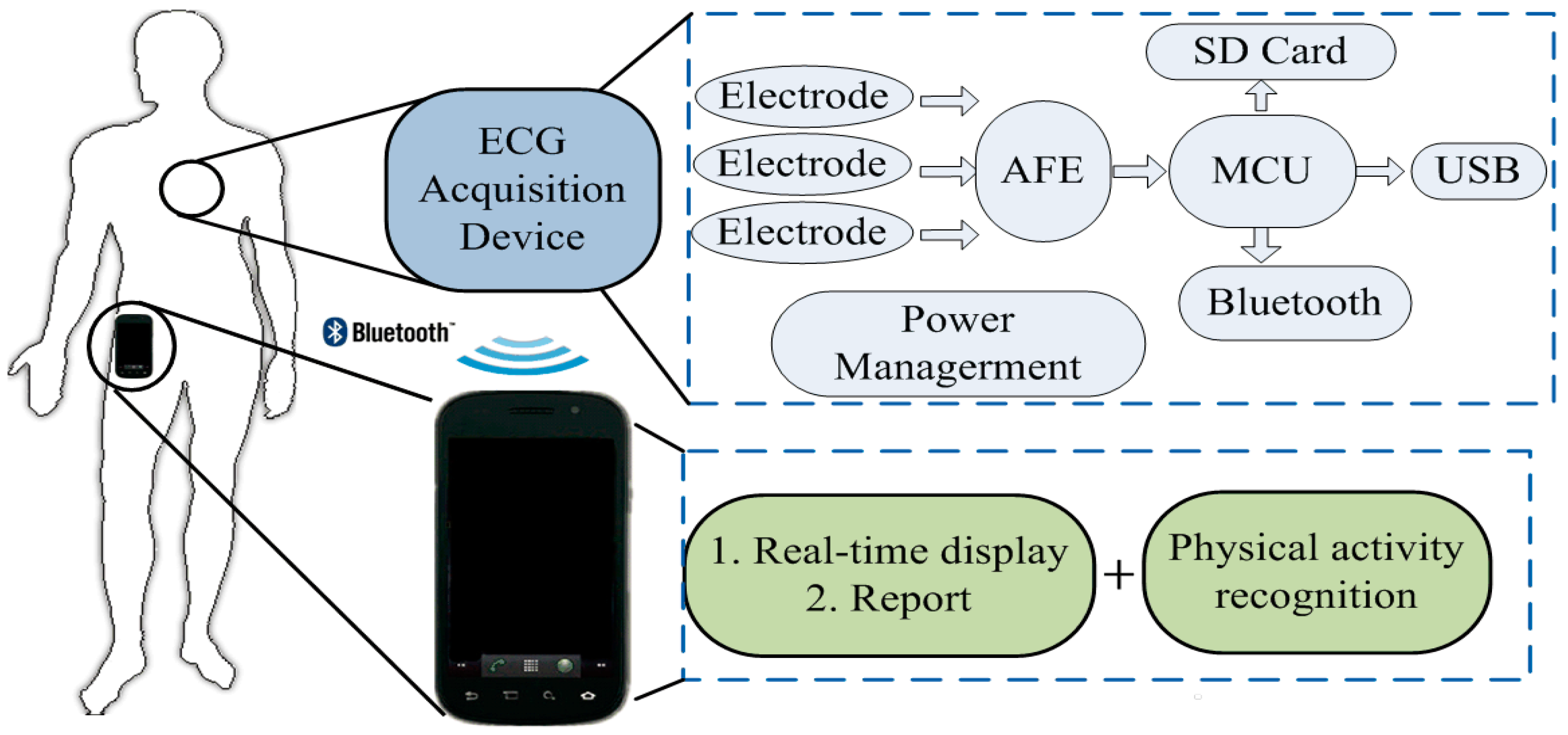
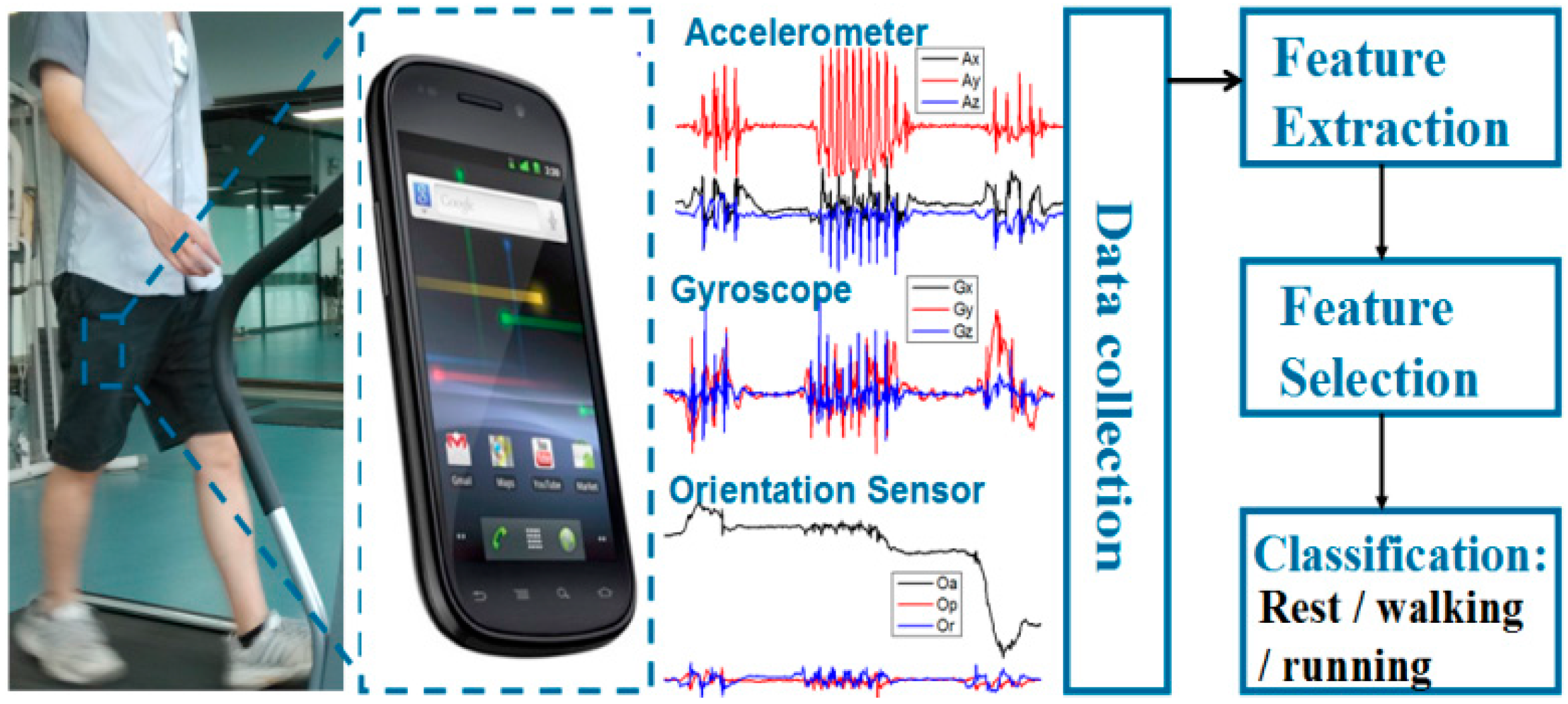
The ECG signal is amplified and filtered by the chip of AFE module, then the analog signal from AFE is converted to digital signal in MCU module. After processed with wavelet processing algorithm and feature extraction comparison algorithms, the generated digital signal are recorded in the memory cells or transmitted to the personal phone for data fusion and analysis.
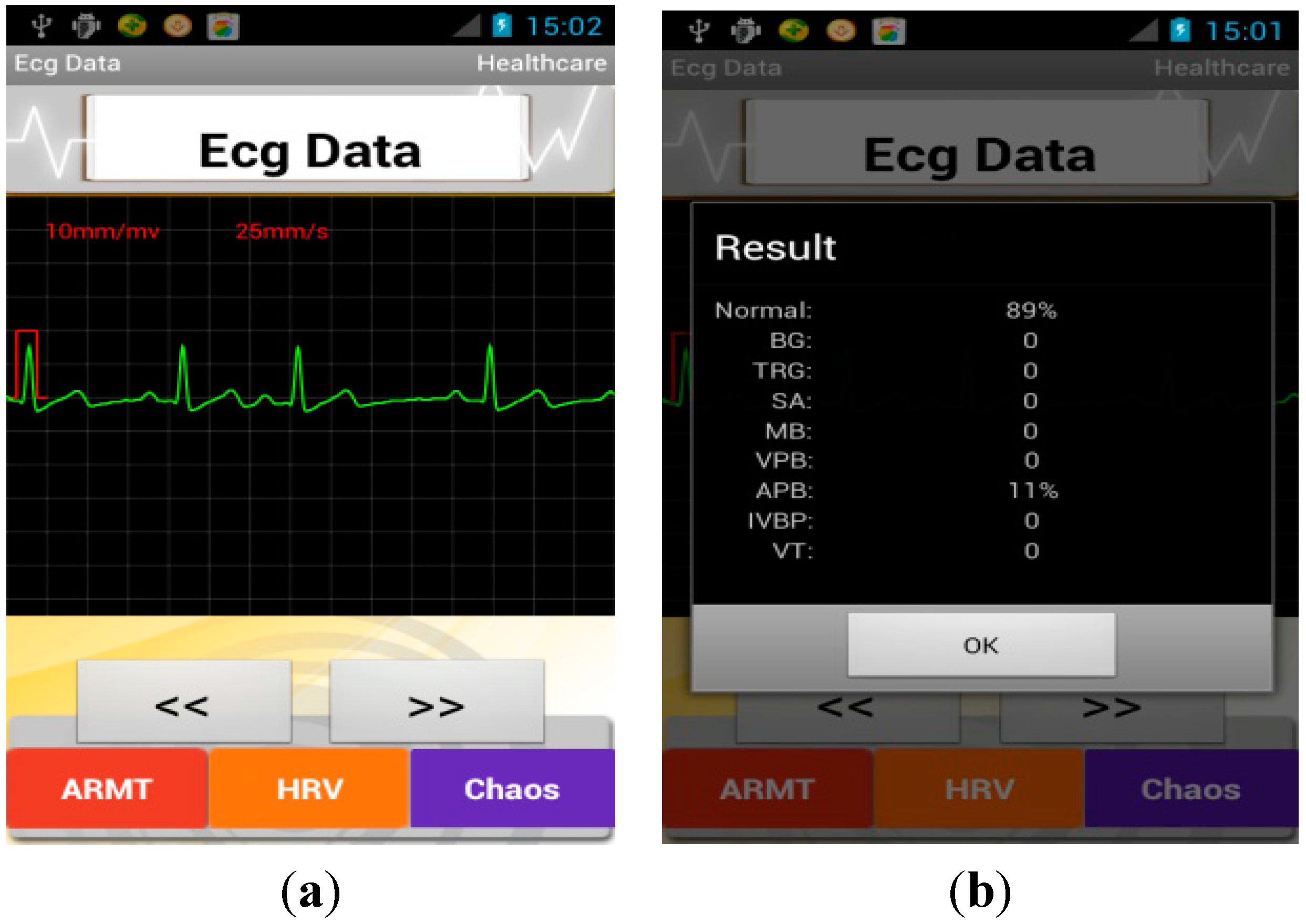
When the monitoring process completed, the features of subjects’ acquired ECG signal were extracted using WABS method and MLE method and according to these features a brief report aiming to detect 10-type arrhythmias and HRV analysis was given, as shown in
Figure 9. The full names of the abbreviations are given in
Table 9. The diagnostic capability was also validated using the muli-parameter simulator (MEDSIM 300B). The testbed is presented in
appendix Figure 6, in which the multi-parameter simulator was used to generate ECG signals with different arrhythmias types. We evaluated the discrimination ability of in terms of half total error rate (HTER), which equals to (false acceptance rate (FAR) + false rejection rate (FRR))/2. The technical report is demonstrated in
Table 10, from the
Table 10 we can see, the software on smartphone can realize a good discrimination performance in recognizing abnormal pattern with high reliability.
Figure 9.
Screenshot of smartphone (a) abnormal ECG signal; (b) the brief report.
Figure 9.
Screenshot of smartphone (a) abnormal ECG signal; (b) the brief report.
Table 9.
Abbreviations in the report.
Table 9.
Abbreviations in the report.
| Abbreviations | Full Name |
|---|
| BG | Bigeminy |
| TBG | Trigeminy |
| SA | Sinus arrhythmia |
| MB | Missed beat |
| VPB | Ventricular premature beats |
| APB | Atrial premature beats |
| IVBP | Interpolated ventricular premature beat |
| VT | Ventricular tachycardia |
| PB | Pause Beat |
Table 10.
Discrimination ability of the proposed software.
Table 10.
Discrimination ability of the proposed software.
| Items | True Positive | False Negative | True Negative | False Positive | Discrimination Ability (HTER) |
|---|
| Arrhythmias Type | BG | 444 | 3 | 2024 | 0 | 0.34% |
| TBG | 258 | 0 | 2213 | 0 | 0 |
| SA | 200 | 0 | 2271 | 0 | 0 |
| MB | 125 | 1 | 2345 | 0 | 0.345% |
| VPB | 149 | 3 | 2315 | 4 | 1.04% |
| APB | 247 | 1 | 2220 | 3 | 0.27% |
| PB | 49 | 1 | 2421 | 0 | 1% |
| VT | 287 | 3 | 2179 | 0 | 0.5% |
| Tachycardia | 200 | 0 | 2271 | 0 | 0 |
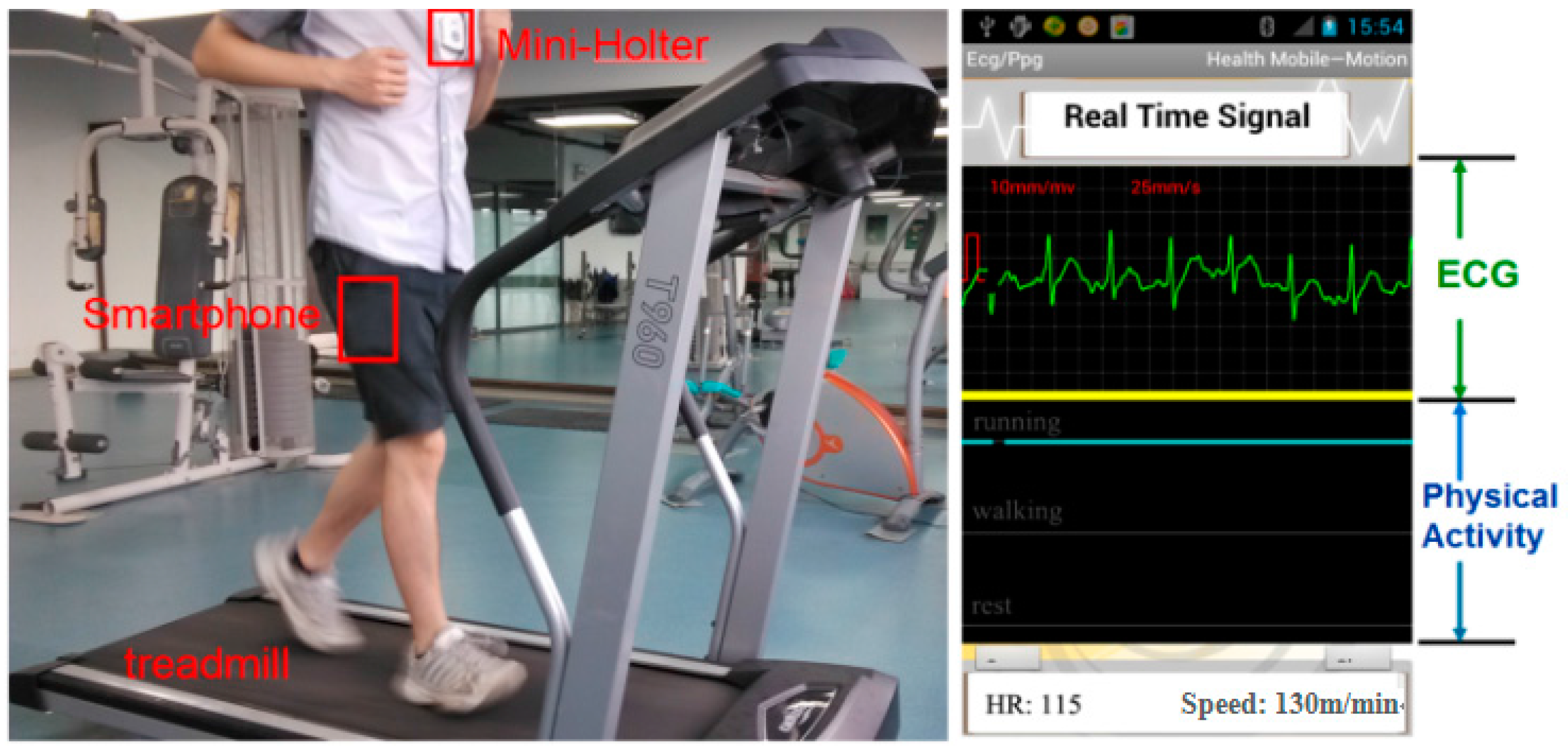
In the sensor fusion application, the subject wore the ECG acquisition sensor on the chest with the smartphone in any trousers pockets.
Figure 10 gives a visible presentation of our experiment with one subject as the example. On the treadmill, the subject was running at the speed of 8 km/h. Moreover, the screenshot of the smartphone was also displayed in
Figure 10. “HR” represents “Heart rate” in the figure, which indicates that the heart rate of the subject was 115 at this time. “Speed” represents the ambulation speed of the specific time duration, which can help to evaluate human efforts while performing the activity. The green line was the ECG signal at the real time, while the blue line indicated physical activity of the subject. When the blue line was located at the top, middle, bottom, it demonstrated that the subject was running, walking and resting at this moment, respectively.
Figure 10.
The experiment of ECG Acquisition system with physical activity recognition on a treadmill.
Figure 10.
The experiment of ECG Acquisition system with physical activity recognition on a treadmill.
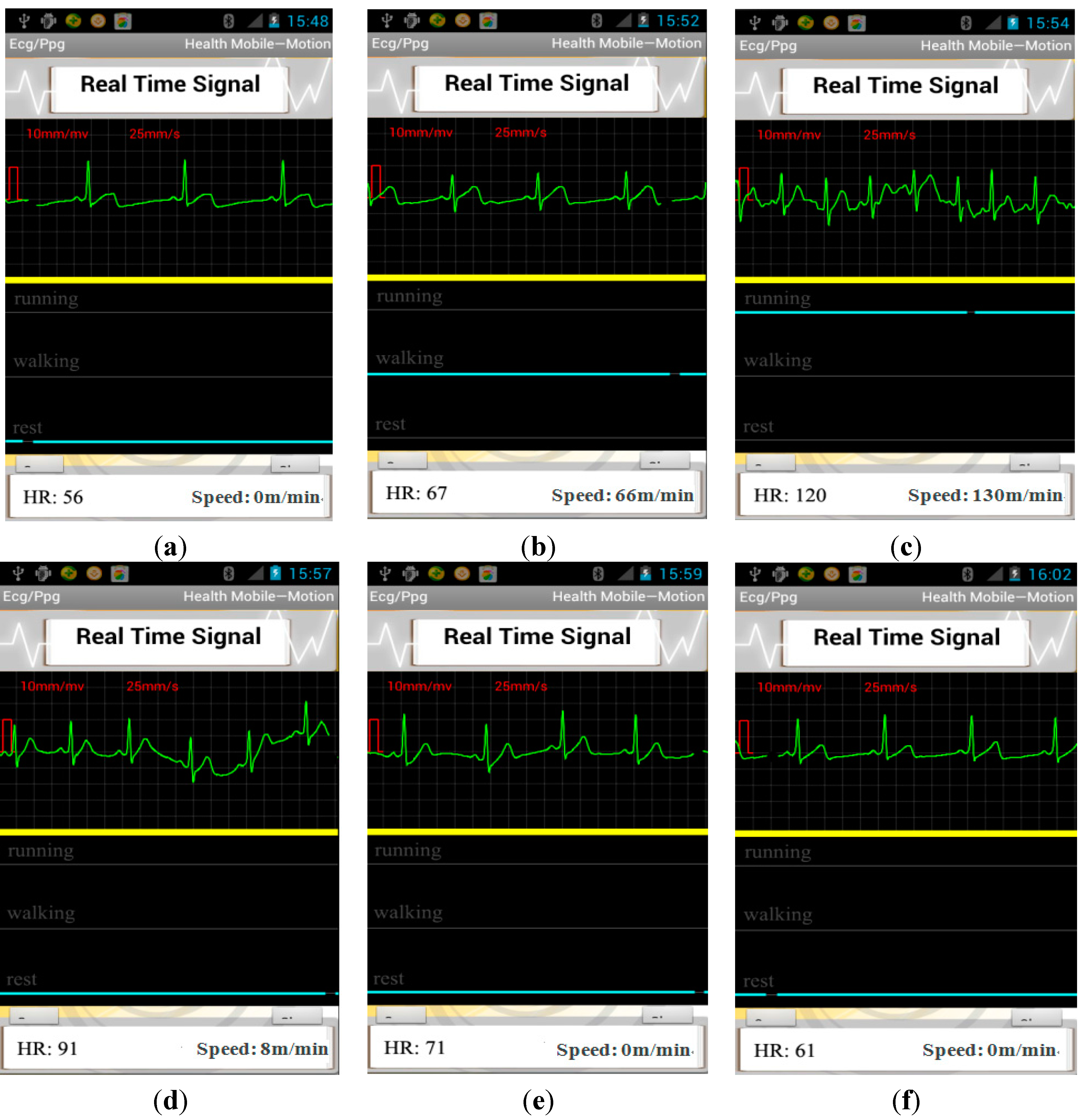
A case for continuously monitoring one subject’s context-aware ECG with the proposed system is presented in
Figure 11. From
Figure 11a we can see, the subject is with a heart rate of 56 while resting. When the subject changed his activity status from walking to running, there was a sharp increase in heart rate of the subject from 67 to 120. Then, after running, the subject rested 30 s with a heart rate of 91. When the subject was resting 300 s after running, heart rate of the subject recovered to the value before running. From the above report we can see, the context-aware system is necessary to evaluate the user’s real health condition. For example, a heart rate of 120 is usually deemed as tachycardia from professional experience. However, it is acceptable if the user is running or taking exercise, which can be reflected from the activity recognition solution. In addition, the monitoring on the variation of ECG with the physical activity provides a useful tool to evaluate one’s cardiac function on the adaption to the change of status.
To demonstrate the usefulness of context-aware ECG to recognize physical activity while monitoring ECG, we also performed a statistical analysis on the improvement on the diagnosis accuracy combined with physical activity.
Table 11 gives the abnormal patterns detected before and after combined with context information and the comparison with the actual patterns from the clinician’s diagnosis. The overall heartbeat number is 7100. VT is often classified as three or more beats on an ECG that are at a rate of more than 100 beats per minute in static status, however, when transferring from walking status to running status, the heart rate increased rapidly, perhaps in a range of 120–180. Therefore, VT can be defined as three or more beats are with a rate of more than 180 beats per minute in running status, as the volunteers are around 24 years old. In order to demonstrate the discrimination performance of the proposed context-aware ECG system, except for an intuitive presentation in
Table 11, we also compared the HTER between the single ECG sensor and the context-aware ECG system on recognizing abnormal patterns, which can be seen in
Table 12. From the table we can see, the discrimination ability was improved in a certain degree by combination of physical activity with a HTER of 2.6%, compared with 2.8% with the single ECG sensor, and thus demonstrated the effectiveness of the proposed context-aware ECG system in real-life application. In addition, the proposed system can identify the most frequent abnormal ECG patterns in different activities for each subject, and accordingly, we can provide helpful suggestions for him to be careful during this type of activity. For example, as our experiment is carried out on healthy subjects, the abnormal patterns have a very low rate; however, we also found that most abnormal patterns are occurring at running status. In another words, a lot of asymptomatic ECG patterns can be detected through monitoring context-aware ECG.
Figure 11.
The screenshot of smartphone (a) the subject was resting; (b) the subject was walking on the treadmill; (c) the subject was running on the treadmill; (d) the subject rested 30 s after running; (e) the subject rested 90 s after running; (f) the subject rested 300 s after running.
Figure 11.
The screenshot of smartphone (a) the subject was resting; (b) the subject was walking on the treadmill; (c) the subject was running on the treadmill; (d) the subject rested 30 s after running; (e) the subject rested 90 s after running; (f) the subject rested 300 s after running.
Table 11.
Statistical analysis on the performance of proposed context-aware ECG system.
Table 11.
Statistical analysis on the performance of proposed context-aware ECG system.
| Abnormal Patterns | Detected from ECG Sensor | Detected from Context-Aware ECG Sensor | Actual |
|---|
| BG | 0 | 0 | 0 |
| TBG | 0 | 0 | 0 |
| SA | 0 | 0 | 0 |
| MB | 0 | 0 | 0 |
| PB | 0 | 0 | 0 |
| VPB | 4 | 4 (3 in running, 1 in walking) | 4 |
| APB | 5 | 5 (3 in running, 1 in walking, 1 in rest) | 5 |
| IVBP | 0 | 0 | 0 |
| VT | 31 | 9 (8 in running, 1 in walking) | 10 |
| Tachycardia | 6 | 0 | 0 |
Table 12.
Discrimination ability comparison between the proposed context-aware ECG system and single ECG sensor. TP: true positive, FN: false negative, TN: true negative, FP: false positive.
Table 12.
Discrimination ability comparison between the proposed context-aware ECG system and single ECG sensor. TP: true positive, FN: false negative, TN: true negative, FP: false positive.
| | ECG Beat Number | Discrimination Ability (HTER) |
|---|
| TP | FN | TN | FP |
|---|
| Single ECG Sensor | 18 | 1 | 7054 | 27 | 2.8% |
| Context-Aware ECG System | 18 | 1 | 7081 | 0 | 2.6% |











{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}


