
Hepatitis B Vaccination in Senegalese Children: Coverage, Timeliness, and Sociodemographic Determinants of Non-Adherence to Immunisation Schedules (ANRS 12356 AmBASS Survey)

 , , , , and
, , , , and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Setting and Design
2.2. Data Collection
2.2.1. HBV Vaccination Status
2.2.2. Socioeconomic Questionnaires
2.3. Ethical Consideration
2.4. Study Population
2.5. Study Outcome
2.6. Explanatory Variables
- Children’s sociodemographic characteristics: sex (male/female); season of birth (wet season [July–October]/dry season ([November–June]); place of birth (healthcare facility [i.e., healthcare post, healthcare centre, hospital, etc.]/home); birth order (1/≥2);
- Children’s living conditions: type of village (semi-urban/rural); distance to the nearest healthcare post (≤3 km/>3 km); household living conditions index (1st/2nd/3rd/4th quartile); household agricultural resources index (1st/2nd/3rd/4th quartile or 1st quartile/2nd–4th quartiles). The latter two indexes were built using a multiple correspondence analysis of information on durable goods, agricultural/farming resources, and housing characteristics at the household level;
- Parents’ sociodemographic characteristics: mother’s age at childbirth (≤19/20–29/≥30 years); prenatal consultation during the mother’s most recent pregnancy (yes/no); mother’s marital status (married/not married [single, widowed, divorced]); mother’s educational level (no schooling/primary school/secondary school and higher); father’s educational level (no schooling/primary school/secondary school and higher).
2.7. Statistical Analyses
2.7.1. Data Weighting and Calibration
2.7.2. Descriptive Analyses
2.7.3. Regression Models
2.7.4. Sensitivity Analyses
3. Results
3.1. Sociodemographic Characteristics of Children
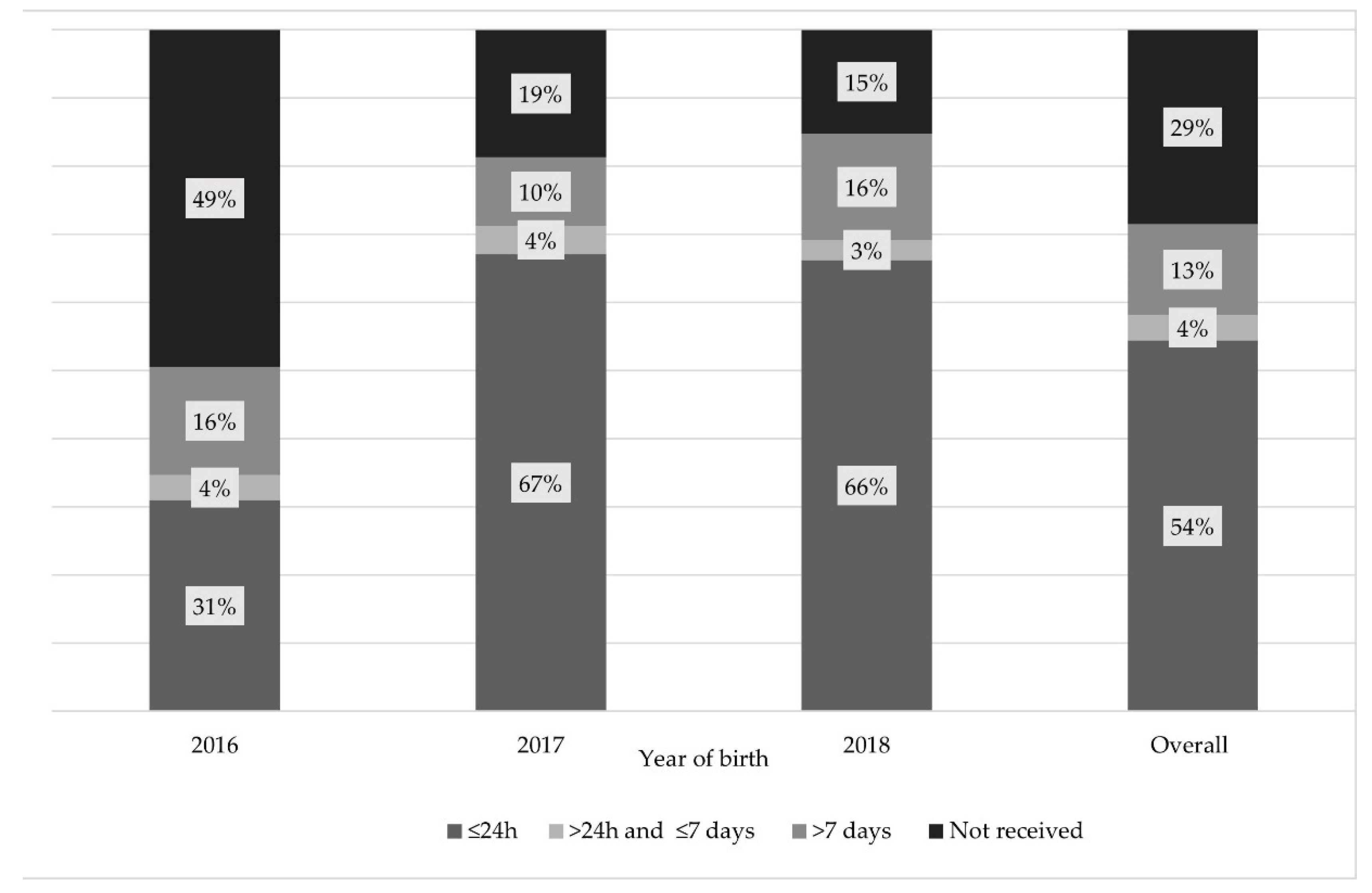
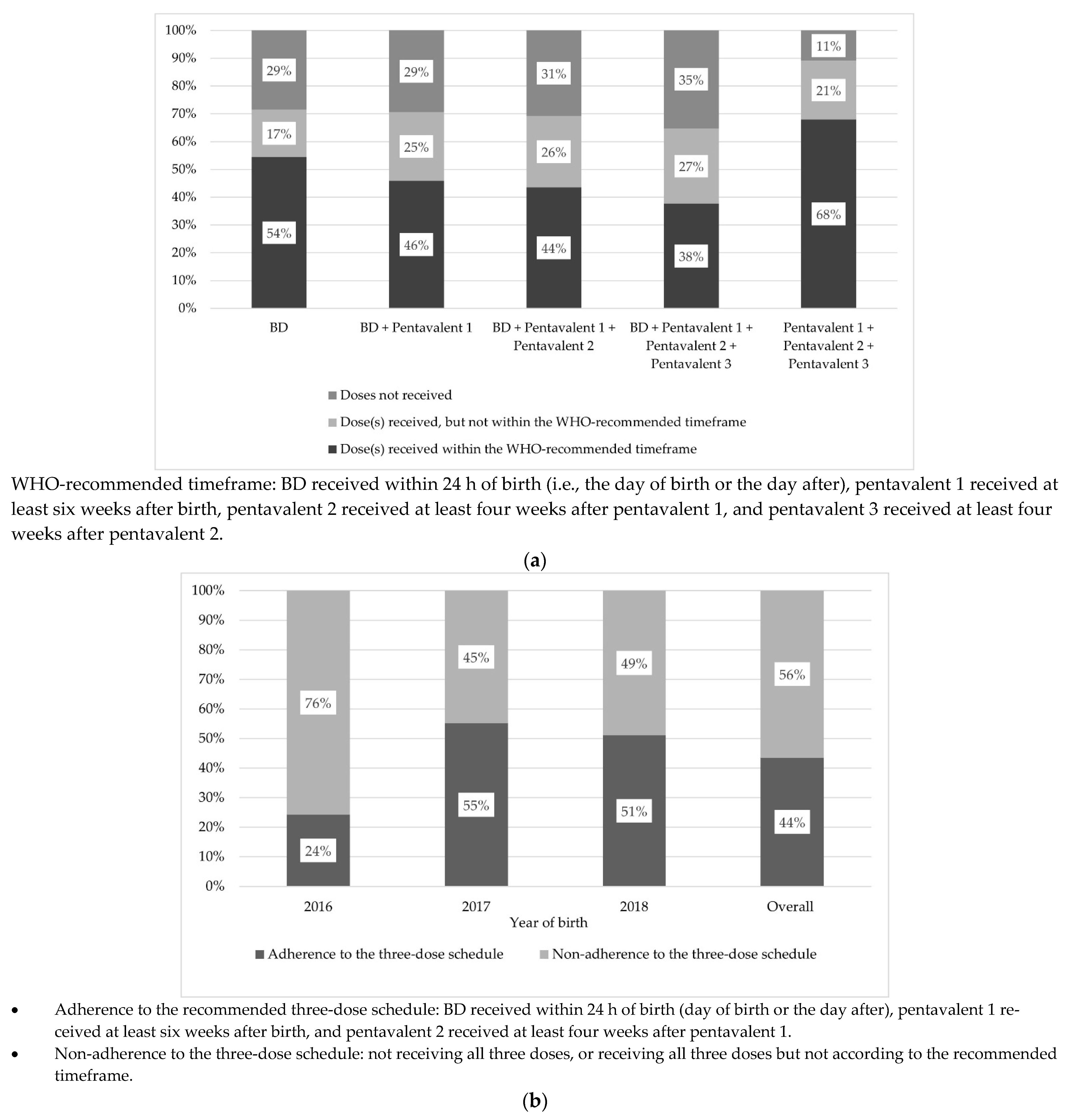
3.2. Vaccination Coverage and Timeliness
3.3. Factors Associated with Non-Adherence to WHO-Recommended Schedules
3.3.1. Non-Adherence to the BD Schedule
3.3.2. Non-Adherence to the Three-Dose Schedule
3.3.3. Sensitivity Analyses
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Razavi-Shearer, D.; Gamkrelidze, I.; Nguyen, M.H.; Chen, D.-S.; Van Damme, P.; Abbas, Z.; Abdulla, M.; Rached, A.A.; Adda, D.; Aho, I.; et al. The Polaris Observatory Collaborators Global prevalence, treatment, and prevention of hepatitis B virus infection in 2016: A modelling study. Lancet Gastroenterol. Hepatol. 2018, 3, 383–403. [Google Scholar] [CrossRef]
- Global Burden of Disease Collaborative Network. Global Burden of Disease Study 2019 (GBD 2019) Results; Institute for Health Metrics and Evaluation (IHME): Seattle, WA, USA, 2020. [Google Scholar]
- WHO. Global Health Sector Strategy on Viral Hepatitis 2016–2021; WHO: Geneva, Switzerland, 2016. [Google Scholar]
- Spearman, C.W.; Afihene, M.; Ally, R.; Apica, B.; Awuku, Y.; Cunha, L.; Dusheiko, G.; Gogela, N.; Kassianides, C.; Kew, M.; et al. Hepatitis B in sub-Saharan Africa: Strategies to achieve the 2030 elimination targets. Lancet Gastroenterol. Hepatol. 2017, 2, 900–909. [Google Scholar] [CrossRef] [Green Version]
- Edmunds, W.J.; Medley, G.F.; Nokes, D.J.; O’Callaghan, C.J.; Whittle, H.C.; Hall, A.J. Epidemiological patterns of hepatitis B virus (HBV) in highly endemic areas. Epidemiol. Infect. 1996, 313–325. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Martinson, F.E.A.; Weigle, K.A.; Royce, R.A.; Weber, D.J.; Suchindran, C.M.; Lemon, S.M. Risk Factors for Horizontal Transmission of Hepatitis B Virus in a Rural District in Ghana. Am. J. Epidemiol. 1998, 147, 478–487. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Edmunds, W.J.; Medley, G.F.; Nokes, D.J.; Hall, A.J.; Whittle, H.C. The influence of age on the development of the hepatitis B carrier state. Proc. R. Soc. Lond. B Biol. Sci. 1993, 253, 197–201. [Google Scholar]
- Shimakawa, Y.; Yan, H.-J.; Tsuchiya, N.; Bottomley, C.; Hall, A.J. Association of Early Age at Establishment of Chronic Hepatitis B Infection with Persistent Viral Replication, Liver Cirrhosis and Hepatocellular Carcinoma: A Systematic Review. PLoS ONE 2013, 8, e69430. [Google Scholar] [CrossRef] [PubMed]
- WHO. Hepatitis B vaccines: WHO position paper-July. WHO Wkly. Epidemiol. Rec. 2017, 92, 369–392. [Google Scholar]
- Nayagam, S.; Thursz, M.; Sicuri, E.; Conteh, L.; Wiktor, S.; Low-Beer, D.; Hallett, T.B. Requirements for global elimination of hepatitis B: A modelling study. Lancet Infect. Dis. 2016, 16, 1399–1408. [Google Scholar] [CrossRef] [Green Version]
- Mbengue, M.A.S.; Sarr, M.; Faye, A.; Badiane, O.; Camara, F.B.N.; Mboup, S.; Dieye, T.N. Determinants of complete immunization among senegalese children aged 12–23 months: Evidence from the demographic and health survey. BMC Public Health 2017, 17, 630. [Google Scholar] [CrossRef] [PubMed]
- Peretti-Watel, P.; Cortaredona, S.; Ly, E.Y.; Seror, V.; Ndiaye, S.; Gaye, I.; Fall, M. Determinants of childhood immunizations in Senegal: Adding previous shots to sociodemographic background. Hum. Vaccines Immunother. 2020, 16, 363–370. [Google Scholar] [CrossRef]
- WHO; UNICEF. Senegal: WHO and UNICEF Estimates of Immunization Coverage: 2019 Revision. 2020. Available online: https://www.who.int/immunization/monitoring_surveillance/data/sen.pdf (accessed on 7 May 2021).
- Agence Nationale de la Statistique et de la Démographie (ANSD) [Sénégal]. Sénégal: Enquête Démographique et de Santé Continue (EDS-Continue 2019); ANSD and ICF: Rockville, MA, USA, 2020. (In French) [Google Scholar]
- Kroger, A.; Bahta, L.; Hunter, P. General Best Practice Guidelines for Immunization. Best Practice Guidance of the Advisory Committee on Immunization Practices (ACIP). Available online: https://www.cdc.gov/vaccines/hcp/acip-recs/general-recs/downloads/general-recs.pdf (accessed on 7 May 2021).
- Guerra, F.A. Delays in Immunization Have Potentially Serious Health Consequences. Pediatr Drugs 2007, 6, 143–148. [Google Scholar] [CrossRef]
- Soares-Weisner, K. Ompitmizing the Hepatitis B Vaccinaiton Schedules: Systematic Review Of Safety and Efficacy of Childhood Schedules Using Hepatitis B Containing Vaccines. Available online: https://www.who.int/immunization/sage/meetings/2016/october/4_Systematic_review_of_safety_efficacy_hep_b.pdf?ua=1 (accessed on 6 April 2021).
- Delaunay, V.; Douillot, L.; Diallo, A.; Dione, D.; Trape, J.-F.; Medianikov, O.; Raoult, D.; Sokhna, C. Profile: The Niakhar Health and Demographic Surveillance System. Int. J. Epidemiol. 2013, 42, 1002–1011. [Google Scholar] [CrossRef] [PubMed]
- Coste, M.; De Sèze, M.; Diallo, A.; Carrieri, M.P.; Marcellin, F.; Boyer, S. Burden and impacts of chronic hepatitis B infection in rural Senegal: Study protocol of a cross-sectional survey in the area of Niakhar (AmBASS ANRS 12356). BMJ Open 2019, 9, e030211. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Programme National de Lutte Contre les Hépatites. Strategic Plan against Viral Hepatitis in Senegal (2019–2023): Policy Brief; Ministère de la Santé et de l’Action Sociale and Programme National de Lutte Contre les Hépatites: Dakar, Senegal, 2019. [Google Scholar]
- Voxco—The Insights platform for Changemakers. Available online: https://www.voxco.com/ (accessed on 17 March 2021).
- Miyahara, R.; Jasseh, M.; Gomez, P.; Shimakawa, Y.; Greenwood, B.; Keita, K.; Ceesay, S.; D’Alessandro, U.; Roca, A. Barriers to timely administration of birth dose vaccines in The Gambia, West Africa. Vaccine 2016, 34, 3335–3341. [Google Scholar] [CrossRef] [Green Version]
- Sarker, A.R.; Akram, R.; Ali, N.; Chowdhury, Z.I.; Sultana, M. Coverage and Determinants of Full Immunization: Vaccination Coverage among Senegalese Children. Medicina 2019, 55, 480. [Google Scholar] [CrossRef] [Green Version]
- Schoeps, A.; Ouédraogo, N.; Kagoné, M.; Sié, A.; Müller, O.; Becher, H. Socio-demographic determinants of timely adherence to BCG, Penta3, measles, and complete vaccination schedule in Burkina Faso. Vaccine 2013, 32, 96–102. [Google Scholar] [CrossRef]
- Dionne-Odom, J.; Westfall, A.O.; Nzuobontane, D.; Vinikoor, M.J.; Halle-Ekane, G.; Welty, T.; Tita, A.T.N. Predictors of Infant Hepatitis B Immunization in Cameroon: Data to Inform Implementation of a Hepatitis B Birth Dose. Pediatr. Infect. Dis. J. 2018, 37, 103–107. [Google Scholar] [CrossRef] [PubMed]
- Van de Ven, W.P.M.M.; Van Pragg, B.M.S. The demand for deductibles in private health insurance: A probit model with sample selection. J. Econom. 1981, 17, 229–252. [Google Scholar] [CrossRef]
- Bassoum, O.; Kimura, M.; Tal Dia, A.; Lemoine, M.; Shimakawa, Y. Coverage and Timeliness of Birth Dose Vaccination in Sub-Saharan Africa: A Systematic Review and Meta-Analysis. Vaccines 2020, 8, 301. [Google Scholar] [CrossRef] [PubMed]
- Agence Nationale de la Statistique et de la Démographie (ANSD) [Sénégal]. Sénégal: Enquête Démographique et de Santé Continue (EDS-Continue 2018); ANSD and ICF: Rockville, MA, USA, 2019. (In French) [Google Scholar]
- Gibson, D.G.; Ochieng, B.; Kagucia, E.W.; Obor, D.; Odhiambo, F.; O’Brien, K.L.; Feikin, D.R. Individual level determinants for not receiving immunization, receiving immunization with delay, and being severely underimmunized among rural western Kenyan children. Vaccine 2015, 33, 6778–6785. [Google Scholar] [CrossRef] [Green Version]
- Adetifa, I.M.O.; Karia, B.; Mutuku, A.; Bwanaali, T.; Makumi, A.; Wafula, J.; Chome, M.; Mwatsuma, P.; Bauni, E.; Hammitt, L.L.; et al. Coverage and timeliness of vaccination and the validity of routine estimates: Insights from a vaccine registry in Kenya. Vaccine 2018, 36, 7965–7974. [Google Scholar] [CrossRef]
- Gram, L.; Soremekun, S.; ten Asbroek, A.; Manu, A.; O’Leary, M.; Hill, Z.; Danso, S.; Amenga-Etego, S.; Owusu-Agyei, S.; Kirkwood, B.R. Socio-economic determinants and inequities in coverage and timeliness of early childhood immunisation in rural Ghana. Trop. Med. Int. Health 2014, 19, 802–811. [Google Scholar] [CrossRef] [Green Version]
- Marefiaw, T.A.; Yenesew, M.A.; Mihirete, K.M. Age-appropriate vaccination coverage and its associated factors for pentavalent 1-3 and measles vaccine doses, in northeast Ethiopia: A community-based cross-sectional study. PLOS ONE 2019, 14, e0218470. [Google Scholar] [CrossRef] [Green Version]
- Schweitzer, A.; Akmatov, M.K.; Krause, G. Hepatitis B vaccination timing: Results from demographic health surveys in 47 countries. Bull. World Health Organ. 2017, 95, 199G–209G. [Google Scholar] [CrossRef]
- Djaogol, T.; Coste, M.; Marcellin, F.; Jaquet, A.; Chabrol, F.; Giles-Vernick, T.; Diallo, A.; Carrieri, M.P.; Boyer, S. Prevention and care of hepatitis B in the rural region of Fatick in Senegal: A healthcare workers’ perspective using a mixed methods approach. BMC Health Serv. Res. 2019, 19, 627. [Google Scholar] [CrossRef] [Green Version]
- Okwaraji, Y.B.; Mulholland, K.; Schellenberg, J.; Andarge, G.; Admassu, M.; Edmond, K.M. The association between travel time to health facilities and childhood vaccine coverage in rural Ethiopia. A community based cross sectional study. BMC Public Health 2012, 12, 476. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Masters, N.B.; Wagner, A.L.; Boulton, M.L. Vaccination timeliness and delay in low- and middle-income countries: A systematic review of the literature, 2007–2017. Hum. Vaccines Immunother. 2019, 15, 2790–2805. [Google Scholar] [CrossRef] [PubMed]
- Gibson, D.G.; Ochieng, B.; Kagucia, E.W.; Were, J.; Hayford, K.; Moulton, L.H.; Levine, O.S.; Odhiambo, F.; O’Brien, K.L.; Feikin, D.R. Mobile phone-delivered reminders and incentives to improve childhood immunisation coverage and timeliness in Kenya (M-SIMU): A cluster randomised controlled trial. Lancet Glob. Health 2017, 5, e428–e438. [Google Scholar] [CrossRef] [Green Version]
- Oyo-Ita, A.; Wiysonge, C.S.; Oringanje, C.; Nwachukwu, C.E.; Oduwole, O.; Meremikwu, M.M. Interventions for improving coverage of childhood immunisation in low- and middle-income countries. Cochrane Database Syst. Rev. 2016, 7, CD008145. [Google Scholar] [CrossRef] [Green Version]
- Rainey, J.J.; Watkins, M.; Ryman, T.K.; Sandhu, P.; Bo, A.; Banerjee, K. Reasons related to non-vaccination and under-vaccination of children in low and middle income countries: Findings from a systematic review of the published literature, 1999–2009. Vaccine 2011, 29, 8215–8221. [Google Scholar] [CrossRef]
- Phillips, D.E.; Dieleman, J.L.; Lim, S.S.; Shearer, J. Determinants of effective vaccine coverage in low and middle-income countries: A systematic review and interpretive synthesis. BMC Health Serv. Res. 2017, 17, 681. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| Characteristics (% of Missing Data) | Overall (n = 272) % | Available Vaccination Data (n = 241) % | Missing Vaccination Data (n = 31) % | Pearson Chi2 p Value |
|---|---|---|---|---|
| Sex (0.0) | ||||
| Male | 47.3 | 45.5 | 61.1 | 0.122 |
| Female | 52.7 | 54.5 | 38.9 | |
| Season of birth (0.0) | ||||
| Wet season | 35.8 | 38.0 | 19.7 | 0.058 |
| Dry season | 64.2 | 62.0 | 80.3 | |
| Place of birth (0.0) | ||||
| Healthcare facility | 77.6 | 79.5 | 63.2 | 0.155 |
| Home | 22.4 | 20.5 | 36.8 | |
| Birth order (0.6) | ||||
| 1 | 19.9 | 18.5 | 30.5 | 0.132 |
| ≥2 | 80.1 | 81.5 | 69.5 | |
| Type of village (0.0) | ||||
| Semi-urban | 57.7 | 58.7 | 50.0 | 0.475 |
| Rural | 42.3 | 41.3 | 50.0 | |
| Distance to closest healthcare post (0.6) | ||||
| ≤3 km | 69.6 | 71.0 | 60.0 | 0.268 |
| >3 km | 30.4 | 29.0 | 40.0 | |
| Mother’s age at child’s birth (years) (5.7) | ||||
| ≤19 | 6.9 | 6.1 | 15.3 | 0.119 |
| 20–29 | 46.0 | 48.1 | 22.9 | |
| ≥30 | 47.1 | 45.8 | 61.8 | |
| Prenatal consultation during the mother’s most recent pregnancy (14.2) | ||||
| Yes | 96.2 | 95.9 | 100.0 | 0.444 |
| No | 3.8 | 4.1 | 0.0 | |
| Mother’s marital status (11.2) | ||||
| Married | 97.1 | 96.9 | 100.0 | 0.439 |
| Not married (single, widowed, divorced) | 2.9 | 3.1 | 0.0 | |
| Mother’s educational level (6.9) | ||||
| No schooling | 66.5 | 68.0 | 49.6 | |
| Primary school | 20.1 | 18.7 | 35.6 | 0.394 |
| Secondary school and higher | 13.4 | 13.3 | 14.8 | |
| Father’s educational level (25.4) | ||||
| No schooling | 57.3 | 57.9 | 50.8 | |
| Primary school | 26.6 | 24.9 | 44.5 | 0.263 |
| Secondary school and higher | 16.1 | 17.2 | 4.7 | |
| Household living conditions index1 (0.0) | ||||
| 1st quartile | 13.7 | 13.1 | 18.0 | |
| 2nd quartile | 22.6 | 21.6 | 29.6 | 0.354 |
| 3rd quartile | 26.0 | 27.7 | 13.2 | |
| 4th quartile | 37.7 | 37.6 | 39.2 | |
| Household agricultural wealth index1 (0.0) | ||||
| 1st quartile | 24.1 | 21.4 | 44.2 | 0.118 |
| 2nd quartile | 18.7 | 19.1 | 15.8 | |
| 3rd quartile | 24.3 | 25.6 | 14.3 | |
| 4th quartile | 32.9 | 33.9 | 25.7 | |
| Born in 2016 (0.0) | ||||
| Yes | 39.3 | 34.5 | 74.1 | 0.006 |
| No (2017–2018) | 60.7 | 65.5 | 25.9 |
| Characteristics (% of Missing Data) | Non-Adherence to the BD Schedule (n = 112) % | Adherence to the BD Schedule (n = 129) % | Univariable Analysis | Multivariable Analysis | ||
|---|---|---|---|---|---|---|
| OR [95% CI] | p Value | aOR [95% CI] | p Value | |||
| Sex (0.0) | ||||||
| Male (ref.) | 40.1 | 49.9 | 1 | 0.200 | ||
| Female | 59.9 | 50.1 | 1.49 [0.78–2.84] | |||
| Season of birth (0.0) | ||||||
| Wet season (ref.) | 31.3 | 43.6 | 1 | 0.102 | 1 | 0.054 |
| Dry season | 68.7 | 56.4 | 1.70 [0.88–3.27] | 1.97 [0.99–3.95] | ||
| Place of birth (0.0) | ||||||
| Healthcare facility (ref.) | 74.4 | 83.8 | 1 | 0.108 | 1 | 0.077 |
| Home | 25.6 | 16.2 | 1.78 [0.86–3.72] | 2.02 [0.91–4.47] | ||
| Birth order (0.7) | ||||||
| 1 | 23.4 | 14.4 | 1.81 [0.81–4.06] | |||
| ≥2 (ref.) | 76.6 | 85.6 | 1 | 0.131 | ||
| Type of village (0.0) | ||||||
| Semi-urban (ref.) | 58.3 | 59.0 | 1 | 0.922 | ||
| Rural | 41.7 | 41.0 | 1.03 [0.53–2.01] | |||
| Distance to closest healthcare post (0.7) | ||||||
| ≤3 km (ref.) | 68.9 | 72.7 | 1 | 0.554 | ||
| >3 km | 31.1 | 27.3 | 1.20 [0.61–2.38] | |||
| Mother’s age at child’s birth (years) (1.5) | ||||||
| ≤19 | 8.4 | 4.1 | 2.47 [0.48–12.73] | |||
| 20–29 | 50.4 | 46.1 | 1.32 [0.70–2.49] | 0.461 | ||
| ≥30 (ref.) | 41.2 | 49.8 | 1 | |||
| Prenatal consultation during the mother’s most recent pregnancy (9.9) | ||||||
| Yes (ref.) | 95.4 | 96.3 | 1 | 0.801 | ||
| No | 4.6 | 3.7 | 1.25 [0.18–8.40] | |||
| Mother’s marital status (11.2) | ||||||
| Married (ref.) | 95.5 | 98.0 | 1 | 0.341 | ||
| Not married (single, widowed, divorced) | 4.5 | 2.0 | 2.34 [0.35–15.82] | |||
| Mother’s educational level (2.9) | ||||||
| No schooling (ref.) | 62.7 | 72.3 | 1 | |||
| Primary school | 23.2 | 15.0 | 1.78 [0.76–4.17] | 0.363 | ||
| Secondary school and higher | 14.1 | 12.7 | 1.28 [0.54–3.06] | |||
| Father’s educational level (22.6) | ||||||
| No schooling (ref.) | 59.7 | 56.4 | 1 | |||
| Primary school | 27.2 | 23.0 | 1.12 [0.56–2.32] | 0.598 | ||
| Secondary school and higher | 13.1 | 20.6 | 0.60 [0.16–2.30] | |||
| Household living conditions index1 (0.0) | ||||||
| 1st quartile | 16.8 | 10.0 | 2.20 [0.90–5.38] | 0.424 | ||
| 2nd quartile | 21.7 | 21.5 | 1.31 [0.48–3.63] | |||
| 3rd quartile | 29.2 | 26.5 | 1.44 [0.67–3.09] | |||
| 4th quartile (ref.) | 32.3 | 42.0 | 1 | |||
| Household agricultural wealth index1 (0.0) | ||||||
| 1st quartile | 25.0 | 18.4 | 1.63 [0.64–4.17] | 0.558 | ||
| 2nd quartile | 21.3 | 17.2 | 1.48 [0.60–3.65] | |||
| 3rd quartile | 23.1 | 27.7 | 1.00 [0.47–2.14] | |||
| 4th quartile (ref.) | 30.6 | 36.7 | 1 | |||
| Born in 2016 (0.0) | ||||||
| Yes (ref.) | 52.3 | 19.6 | 4.48 [1.99–10.08] | 0.002 | 4.94 [2.14–11.40] | 0.002 |
| No (2017–2018) | 47.7 | 80.4 | 1 | 1 | ||
| Characteristics (% of Missing Data) | Non-Adherence to the Three-Dose Schedule (n = 138) | Adherence to the Three-Dose Schedule (n = 103) | Univariable Analysis | Multivariable Analysis | ||
|---|---|---|---|---|---|---|
| OR [95% CI] | p Value | aOR [95% CI] | p Value | |||
| Sex (0.0) | ||||||
| Male (ref.) | 43.6 | 47.8 | 1 | 0.596 | ||
| Female | 56.4 | 52.2 | 1.19 [0.59–2.38] | |||
| Season of birth (0.0) | ||||||
| Wet season (ref.) | 30.5 | 47.7 | 1 | 0.034 | 1 | 0.010 |
| Dry season | 69.5 | 52.3 | 2.08 [1.07–4.02] | 2.70 [1.35–5.39] | ||
| Place of birth (0.0) | ||||||
| Healthcare facility (ref.) | 75.3 | 85.0 | 1 | 0.114 | 1 | 0.047 |
| Home | 24.7 | 15.0 | 1.86 [0.83–4.16] | 2.38 [1.02–5.56] | ||
| Birth order (0.7) | ||||||
| 1 | 23.6 | 12.0 | 2.27 [0.98–5.24] | 0.054 | 2.07 [0.97–4.40] | 0.057 |
| ≥2 (ref.) | 76.4 | 88.0 | 1 | 1 | ||
| Type of village (0.0) | ||||||
| Semi-urban (ref.) | 60.4 | 56.6 | 1 | 0.608 | ||
| Rural | 39.6 | 43.4 | 0.86 [0.44–1.66] | |||
| Distance to closest healthcare post (0.7) | ||||||
| ≤3 km (ref.) | 67.3 | 75.8 | 1 | 0.030 | 1 | 0.058 |
| >3 km | 32.7 | 24.2 | 1.52 [0.81–2.85] | 2.04 [0.97–4.27] | ||
| Mother’s age at child’s birth (years) (1.5) | ||||||
| ≤19 | 8.6 | 2.9 | 3.64 [0.62–21.3] | |||
| 20–29 | 49.6 | 46.1 | 1.32 [0.70–2.47] | 0.321 | ||
| ≥30 (ref.) | 41.8 | 51.0 | 1 | |||
| Prenatal consultation during the mother’s most recent pregnancy (8.3) | ||||||
| Yes (ref.) | 96.3 | 95.4 | 1 | 0.778 | ||
| No | 3.7 | 4.6 | 0.78 [0.12–5.13] | |||
| Mother’s marital status (11.2) | ||||||
| Married (ref.) | 96.3 | 97.5 | 1 | 0.650 | ||
| Not married (single, widowed, divorced) | 3.7 | 2.5 | 1.49 [0.22–10.01] | |||
| Mother’s educational level (2.9) | ||||||
| No schooling (ref.) | 66.9 | 69.5 | 1 | |||
| Primary school | 20.0 | 17.0 | 1.23 [0.49–3.06] | 0.894 | ||
| Secondary school and higher | 13.1 | 13.5 | 1.01 [0.43–2.27] | |||
| Father’s educational level (22.6) | ||||||
| No schooling (ref.) | 62.1 | 52.4 | 1 | |||
| Primary school | 25.1 | 27.4 | 0.85 [0.39–1.88] | 0.541 | ||
| Secondary school and higher | 12.8 | 22.9 | 0.47 [0.12–1.90] | |||
| Household living conditions index1 (0.0) | ||||||
| 1st quartile | 17.4 | 7.6 | 2.50 [0.99–6.32] | 0.324 | ||
| 2nd quartile | 19.2 | 24.7 | 0.85 [0.31–2.36] | |||
| 3rd quartile | 27.3 | 28.3 | 1.05 [0.53–2.08] | |||
| 4th quartile (ref.) | 36.1 | 39.4 | 1 | |||
| Household agricultural wealth index1 (0.0) | ||||||
| 1st quartile | 26.3 | 15.1 | 2.00 [0.95–4.22] | 0.064 | 3.18 [1.33–7.61] | 0.015 |
| 2nd–4th quartile (ref.) | 73.7 | 84.9 | 1 | 1 | ||
| Born in 2016 (0.0) | ||||||
| Yes (ref.) | 46.3 | 19.2 | 3.61 [1.68–7.75] | 0.004 | 3.93 [1.74–8.89] | 0.004 |
| No (2017–2018) | 53.7 | 80.8 | 1 | 1 | ||
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Périères, L.; Marcellin, F.; Lo, G.; Protopopescu, C.; Ba, E.H.; Coste, M.; Touré Kane, C.; Maradan, G.; Diallo, A.; Sokhna, C.; et al. Hepatitis B Vaccination in Senegalese Children: Coverage, Timeliness, and Sociodemographic Determinants of Non-Adherence to Immunisation Schedules (ANRS 12356 AmBASS Survey). Vaccines 2021, 9, 510. https://doi.org/10.3390/vaccines9050510
Périères L, Marcellin F, Lo G, Protopopescu C, Ba EH, Coste M, Touré Kane C, Maradan G, Diallo A, Sokhna C, et al. Hepatitis B Vaccination in Senegalese Children: Coverage, Timeliness, and Sociodemographic Determinants of Non-Adherence to Immunisation Schedules (ANRS 12356 AmBASS Survey). Vaccines. 2021; 9(5):510. https://doi.org/10.3390/vaccines9050510
Chicago/Turabian StylePérières, Lauren, Fabienne Marcellin, Gora Lo, Camelia Protopopescu, El Hadji Ba, Marion Coste, Coumba Touré Kane, Gwenaëlle Maradan, Aldiouma Diallo, Cheikh Sokhna, and et al. 2021. "Hepatitis B Vaccination in Senegalese Children: Coverage, Timeliness, and Sociodemographic Determinants of Non-Adherence to Immunisation Schedules (ANRS 12356 AmBASS Survey)" Vaccines 9, no. 5: 510. https://doi.org/10.3390/vaccines9050510