
A Glance at the Development and Patent Literature of Tecovirimat: The First-in-Class Therapy for Emerging Monkeypox Outbreak

 , , , , ,
, , , , ,  ,
,
Abstract
:1. Introduction
2. Tecovirimat
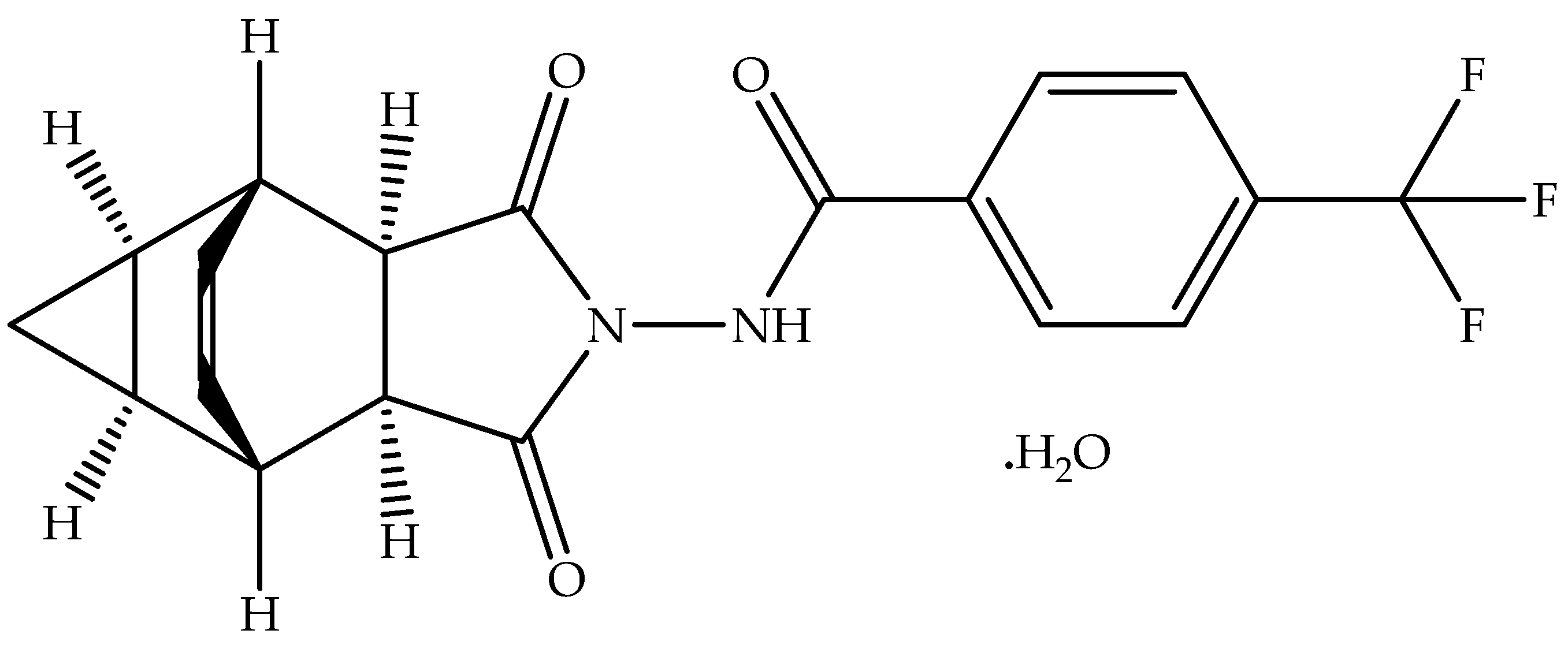
2.1. Chemistry
2.2. Worldwide Approval
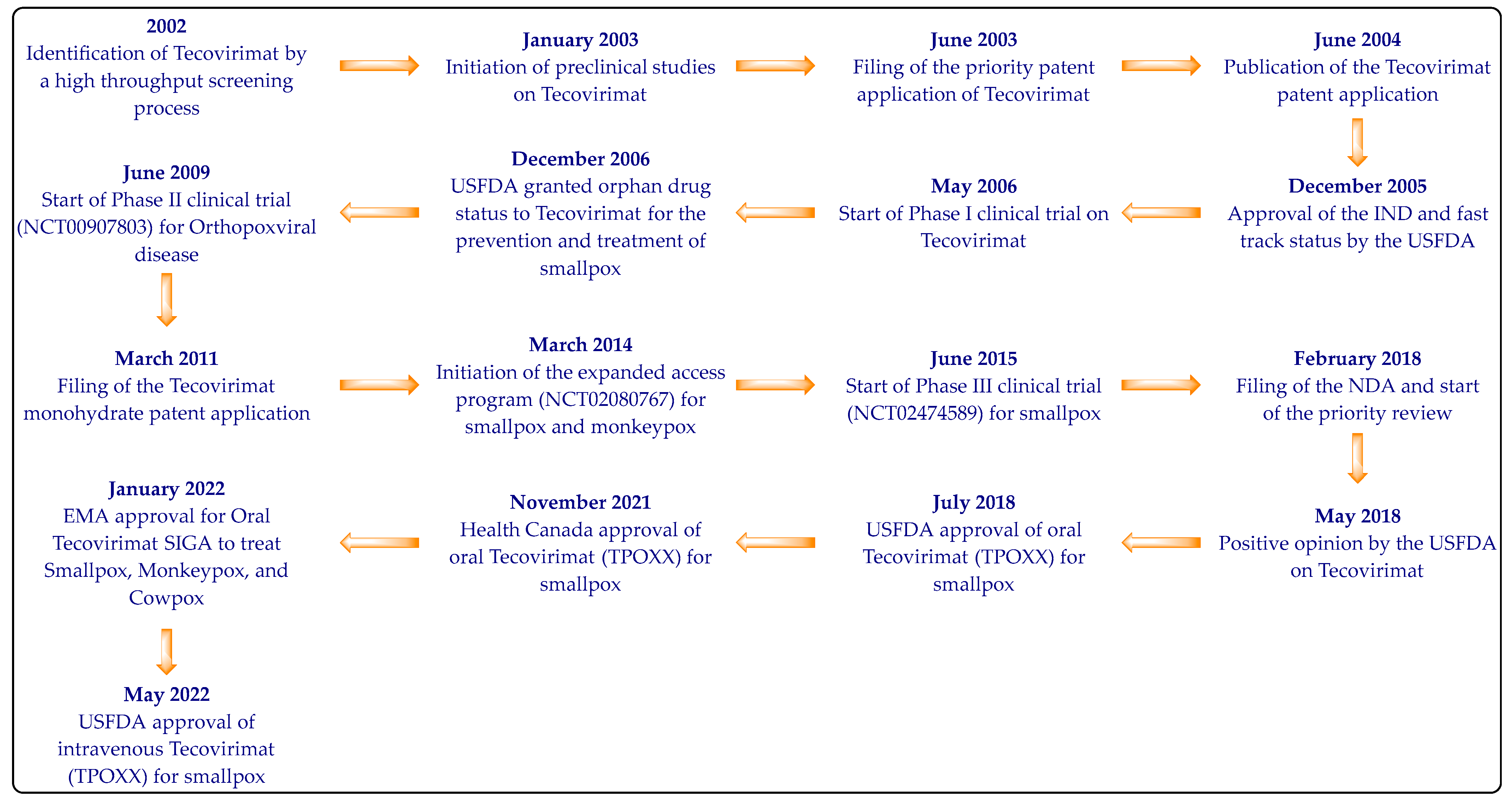
2.3. Development
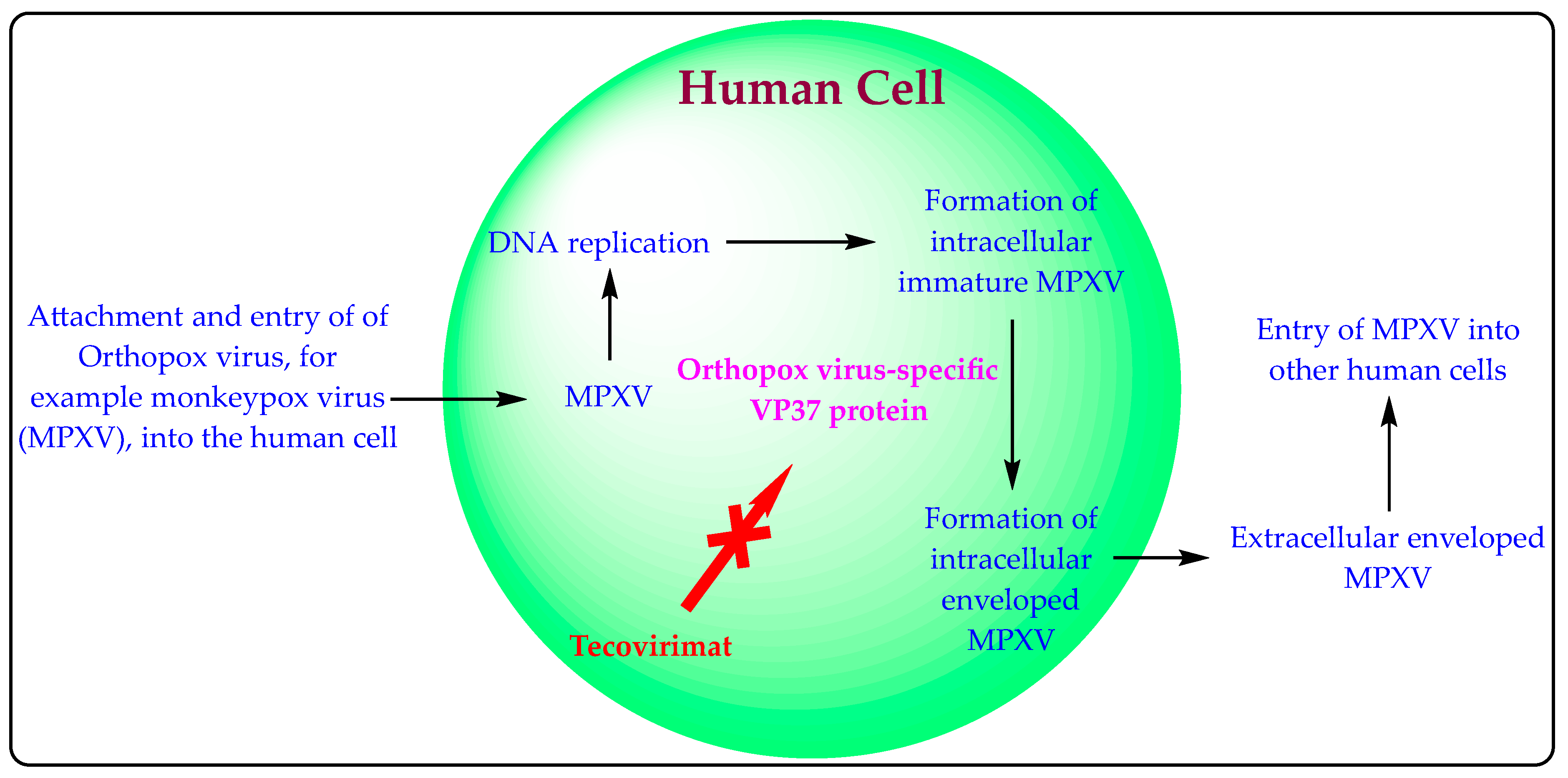
2.4. Pharmacology
3. Clinical Studies
4. Patent Searching and Summary
5. Discussion
6. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Memariani, M.; Memariani, H. Multinational monkeypox outbreak: What do we know and what should we do? Ir. J. Med. Sci. 2022, 1971, 1–2. [Google Scholar]
- Zhang, Y.; Zhang, J.Y.; Wang, F.S. Monkeypox outbreak: A novel threat after COVID-19? Mil. Med. Res. 2022, 9, 29. [Google Scholar] [CrossRef]
- Yoo, J.H. Once bitten, twice shy: Our attitude towards monkeypox. J. Korean Med. Sci. 2022, 37, e188. [Google Scholar] [CrossRef]
- Out, A.; Ebenso, B.; Walley, J.; Barceló, J.M.; Ochu, C.L. Global human monkeypox outbreak: Atypical presentation demanding urgent public health action. Lancet Microbe 2022, 3, e554–e555. [Google Scholar] [CrossRef]
- Sklenovská, N.; Van, R.M. Emergence of monkeypox as the most important orthopoxvirus infection in humans. Front. Public Health 2018, 6, 241. [Google Scholar] [CrossRef]
- Moore, M.; Zahra, F. Monkeypox. In StatPearls [Internet]. Treasure Island (FL); StatPearls Publishing: Tampa, FL, USA, 2022. [Google Scholar]
- World Health Organization. Monkeypox. Available online: https://www.who.int/emergencies/emergency-events/item/monkeypox (accessed on 11 July 2022).
- World Health Organization. Multi-Country Monkeypox Outbreak: Situation Update. Available online: https://www.who.int/emergencies/disease-outbreak-news/item/2022-DON392 (accessed on 11 July 2022).
- Adler, H.; Gould, S.; Hine, P.; Snell, L.B.; Wong, W.; Houlihan, C.F.; Osborne, J.C.; Rampling, T.; Beadsworth, M.B.; Duncan, C.J.; et al. NHS England High Consequence Infectious Diseases (Airborne) Network. Clinical features and management of human monkeypox: A retrospective observational study in the UK. Lancet Infect. Dis. 2022, 22, 1153–1162. [Google Scholar] [CrossRef]
- Kabuga, A.I.; El Zowalaty, M.E. A review of the monkeypox virus and a recent outbreak of skin rash disease in Nigeria. J. Med. Virol. 2019, 91, 533–540. [Google Scholar] [CrossRef]
- Centers for Disease Control and Prevention. Monkeypox Symptoms. Available online: https://www.cdc.gov/poxvirus/monkeypox/symptoms.html (accessed on 11 July 2022).
- World Health Organization. Monkeypox. Available online: https://www.who.int/news-room/fact-sheets/detail/monkeypox (accessed on 11 July 2022).
- Brown, K.; Leggat, P.A. Human monkeypox: Current state of knowledge and implications for the Future. Trop. Med. Infect. Dis. 2016, 1, 8. [Google Scholar] [CrossRef]
- Jain, N.; Lansiaux, E.; Simanis, R. The new face of monkeypox virus: An emerging global emergency. New Microbes New Infect. 2022, 47, 100989. [Google Scholar] [CrossRef]
- TPOXX. Available online: https://www.rxlist.com/tpoxx-drug.htm#clinpharm (accessed on 11 July 2022).
- European Medicines Agency. Tecovirimat SIGA. Available online: https://www.ema.europa.eu/en/medicines/human/EPAR/tecovirimat-siga (accessed on 11 July 2022).
- Hoy, S.M. Tecovirimat: First global approval. Drugs 2018, 78, 1377–1382. [Google Scholar] [CrossRef]
- European Medicines Agency. Assessment Report: Tecovirimat SIGA. Available online: https://www.ema.europa.eu/en/documents/assessment-report/tecovirimat-siga-epar-public-assessment-report_en.pdf (accessed on 11 July 2022).
- Center for Drug Evaluation and Research. Product Quality Review. Available online: https://www.accessdata.fda.gov/drugsatfda_docs/nda/2018/208627Orig1s000ChemR.pdf (accessed on 11 July 2022).
- SIGA Human BioArmor. TPOXX (Tecovirimat) Fact Sheet. Available online: https://www.siga.com/wp-content/uploads/2022/06/TPOXXFactSheet_2022.pdf (accessed on 11 July 2022).
- SIGA Human BioArmor. Smallpox. Available online: https://www.siga.com/wp-content/uploads/2022/06/CorporateBrochure_2022.pdf (accessed on 11 July 2022).
- Orange Book: Approved Drug Products with Therapeutic Equivalence Evaluations. Tecovirimat. Available online: https://www.accessdata.fda.gov/scripts/cder/ob/index.cfm (accessed on 11 July 2022).
- Product Monograph. TPOXX. Available online: https://pdf.hres.ca/dpd_pm/00063782.PDF (accessed on 11 July 2022).
- Government of Canada. Register of Innovative Drugs. Available online: https://www.canada.ca/en/health-canada/services/drugs-health-products/drug-products/applications-submissions/register-innovative-drugs.html (accessed on 11 July 2022).
- Grosenbach, D.W.; Jordan, R.; Hruby, D.E. Development of the small-molecule antiviral ST-246 as a smallpox therapeutic. Future Virol. 2011, 6, 653–671. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Jordan, R.; Leeds, J.M.; Tyavanagimatt, S.; Hruby, D.E. Development of ST-246 for treatment of poxvirus infections. Viruses 2010, 2, 2409–2435. [Google Scholar] [CrossRef] [PubMed]
- Jordan, R.; Bailey, T.R.; Rippin, S.R. Compounds, Compositions and Methods for Treatment and Prevention of Orthopoxvirus Infections and Associated Diseases. PCT Patent WO2,004,112,718A2, 29 December 2004. [Google Scholar]
- Tyavanagimatt, S.R.; Stone, M.A.C.L.; Weimers, W.C.; Nelson, D.; Bolken, T.C.; Hruby, D.E.; O’neill, M.H.; Sweetapple, G.; Mccloughan, K.A. Polymorphic Forms of ST-246 and Methods of Preparation. U.S. Patent 9,339,466B2, 17 May 2016. [Google Scholar]
- Jordan, R.; Goff, A.; Frimm, A.; Corrado, M.L.; Hensley, L.E.; Byrd, C.M.; Mucker, E.; Shamblin, J.; Bolken, T.C.; Wlazlowski, C.; et al. ST-246 antiviral efficacy in a non-human primate monkeypox model: Determination of the minimal effective dose and human dose justification. Antimicrob. Agents Chemother. 2009, 53, 1817–1822. [Google Scholar] [CrossRef] [PubMed]
- Highlights of Prescribing Information. TPOXX. Available online: https://www.accessdata.fda.gov/drugsatfda_docs/label/2018/208627s000lbl.pdf (accessed on 11 July 2022).
- Summary of Product Characteristics. Tecovirimat SIGA. Available online: https://www.ema.europa.eu/en/documents/product-information/tecovirimat-siga-epar-product-information_en.pdf (accessed on 11 July 2022).
- Grosenbach, D.W.; Honeychurch, K.; Rose, E.A.; Chinsangaram, J.; Frimm, A.; Maiti, B.; Lovejoy, C.; Meara, I.; Long, P.; Hruby, D.E. Oral tecovirimat for the treatment of smallpox. N. Engl. J. Med. 2018, 379, 44–53. [Google Scholar] [CrossRef] [PubMed]
- Yang, G.; Pevear, D.C.; Davies, M.H.; Collett, M.S.; Bailey, T.; Rippen, S.; Barone, L.; Burns, C.; Rhodes, G.; Tohan, S.; et al. An orally bioavailable antipoxvirus compound (ST-246) inhibits extracellular virus formation and protects mice from lethal orthopoxvirus Challenge. J. Virol. 2005, 79, 13139–13149. [Google Scholar] [CrossRef]
- Highlights of Prescribing Information. TPOXX. Available online: https://www.accessdata.fda.gov/drugsatfda_docs/label/2022/214518s000lbl.pdf (accessed on 11 July 2022).
- SIGA Technologies. FDA Advisory Committee Briefing Document: Tecovirimat for the Treatment of Smallpox Disease. Available online: https://www.fda.gov/media/112808/download (accessed on 11 July 2022).
- U.S. National Library of Medicines. ClinicalTrials Database. Available online: https://www.clinicaltrials.gov/ (accessed on 11 July 2022).
- Chinsangaram, J.; Honeychurch, K.M.; Tyavanagimatt, S.R.; Leeds, J.M.; Bolken, T.C.; Jones, K.F.; Jordan, R.; Marbury, T.; Ruckle, J.; Mee-Lee, D.; et al. Safety and pharmacokinetics of the anti-orthopoxvirus compound ST-246 following a single daily oral dose for 14 days in human volunteers. Antimicrob. Agents Chemother. 2012, 56, 4900–4905. [Google Scholar] [CrossRef]
- Chinsangaram, J.; Honeychurch, K.M.; Tyavanagimatt, S.R.; Bolken, T.C.; Jordan, R.; Jones, K.F.; Marbury, T.; Lichtenstein, I.; Pickens, M.; Corrado, M.; et al. Pharmacokinetic comparison of a single oral dose of polymorph form I versus form V capsules of the antiorthopoxvirus compound ST-246 in human volunteers. Antimicrob. Agents Chemother. 2012, 56, 3582–3586. [Google Scholar] [CrossRef]
- Jordan, R.; Chinsangaram, J.; Bolken, T.C.; Tyavanagimatt, S.R.; Tien, D.; Jones, K.F.; Frimm, A.; Corrado, M.L.; Pickens, M.; Landis, P.; et al. Safety and pharmacokinetics of the antiorthopoxvirus compound ST-246 following repeat oral dosing in healthy adult subjects. Antimicrob. Agents Chemother. 2010, 54, 2560–2566. [Google Scholar] [CrossRef]
- Jordan, R.; Tien, D.; Bolken, T.C.; Jones, K.F.; Tyavanagimatt, S.R.; Strasser, J.; Frimm, A.; Corrado, M.L.; Strome, P.G.; Hruby, D.E. Single-dose safety and pharmacokinetics of ST-246, a novel orthopoxvirus egress inhibitor. Antimicrob. Agents Chemother. 2008, 52, 1721–1727. [Google Scholar] [CrossRef]
- Leeds, J.M.; Fenneteau, F.; Gosselin, N.H.; Mouksassi, M.S.; Kassir, N.; Marier, J.F.; Chen, Y.; Grosenbach, D.; Frimm, A.E.; Honeychurch, K.M.; et al. Pharmacokinetic and pharmacodynamic modeling to determine the dose of ST-246 to protect against smallpox in humans. Antimicrob. Agents Chemother. 2013, 57, 1136–1143. [Google Scholar] [CrossRef]
- Espacenet. Patent Search. Available online: https://worldwide.espacenet.com/patent/search (accessed on 11 July 2022).
- WIPO IP Portal. Patentscope. Available online: https://patentscope.wipo.int/search/en/structuredSearch.jsf (accessed on 11 July 2022).
- Imran, M.; Alshrari, A.S.; Tauseef, M.; Khan, S.A.; Hudu, S.A.; Abida. Mucormycosis medications: A patent review. Expert Opin. Ther. Pat. 2021, 31, 1059–1074. [Google Scholar] [CrossRef] [PubMed]
- Imran, M.; Alshrari, A.S.; Thabet, H.K.; Abida; Bakht, M.A. Synthetic molecules as DprE1 inhibitors: A patent review. Expert Opin. Ther. Pat. 2021, 31, 759–772. [Google Scholar] [CrossRef] [PubMed]
- Imran, M.; Khan, S.A.; Abida; Alshrari, A.S.; Eltahir, M.M.M.; Alshammari, M.K.; Harshan, A.A.; Alshammari, N.A. Small molecules as kinetoplastid specific proteasome inhibitors for leishmaniasis: A patent review from 1998 to 2021. Expert Opin. Ther. Pat. 2022, 32, 591–604. [Google Scholar] [CrossRef] [PubMed]
- Imran, M.; Asdaq, S.M.B.; Khan, S.A.; Unnikrishnan, M.D.; Alamri, A.S.; Alsanie, W.F.; Alhomrani, M.; Mohzari, Y.; Alrashed, A.; AlMotairi, M.; et al. Innovations and patent trends in the development of USFDA approved protein kinase inhibitors in the last two decades. Pharmaceuticals 2021, 14, 710. [Google Scholar] [CrossRef] [PubMed]
- Ordan, R.; Bailey, T.R.; Rippin, S.R. Compounds, Compositions and Methods for Treatment and Prevention of Orthopoxvirus Infections and Associated Diseases. U.S. Patent 8,124,643B2, 28 February 2012. [Google Scholar]
- Jordan, R.; Bailey, T.R.; Rippin, S.R. Compounds, Compositions, and Methods for Treatment and Prevention of Orthopoxvirus Infections and Associated Diseases. U.S. Patent 7,737,168B2, 15 June 2010. [Google Scholar]
- Jordan, R.F.; Bailey, T.R.; Rippin, S.R.; Dai, D. Compounds, Compositions and Methods for Treatment and Prevention of Orthopoxvirus Infections and Associated Diseases. U.S. Patent 8,802,714B2, 12 August 2014. [Google Scholar]
- Jordan, R.; Bailey, T.R.; Rippin, S.R.; Dai, D. Compounds, Compositions and Methods for Treatment and Prevention of Orthopoxvirus Infections and Associated Diseases. U.S. Patent 8,530,509B2, 10 September 2013. [Google Scholar]
- Tyavanagimatt, S.R.; Anderson, M.A.C.L.S.; Weimers, W.; Kasi, G.K.; Samuel, N.K.P.; Bolken, T.C.; Hruby, D.E. ST-246 Liquid Formulations and Methods. U.S. Patent 10,576,165B2, 3 March 2020. [Google Scholar]
- Tyavanagimatt, S.R.; Stone, M.A.C.L.; Weimers, W.C.; Kasi, G.K.; Samuel, P.N.K.; Bolken, T.; Hruby, D.E. ST-246 Liquid Formulations. U.S. Patent 9,233,097B2, 12 January 2016. [Google Scholar]
- Tyavanagimatt, S.R.; Anderson, M.A.C.L.S.; Weimers, W.; Kasi, G.K.; Samuel, N.K.P.; Bolken, T.C.; Hruby, D.E. ST-246 Liquid Formulations and Methods. U.S. Patent 9,907,859B2, 6 March 2018. [Google Scholar]
- Jordan, R.F.; Bailey, T.R.; Rippin, S.R.; Dai, D. Chemicals, Compositions, and Methods for Treatment and Prevention of Orthopoxvirus Infections and Associated Diseases. U.S. Patent 8,039,504B2, 18 October 2011. [Google Scholar]
- Jordan, R.; Bailey, T.R.; Rippin, S.R. Compounds, Compositions and Methods for Treatment and Prevention of Orthopoxvirus Infections and Associated Diseases. U.S. Patent 7,956,197B2, 7 June 2011. [Google Scholar]
- Tyavanagimatt, S.R.; Anderson, M.A.C.L.S.; Weimers, W.C.; Nelson, D.; Bolken, T.C.; Hruby, D.E.; O’Neill, M.H.; Sweetapple, G.; McCloughan, K.A. Polymorphic Forms of ST-246 and Methods of Preparation. U.S. Patent 9,744,154B2, 29 August 2017. [Google Scholar]
- Tyavanagimatt, S.R.; Anderson, M.A.C.L.S.; Weimers, W.C.; Nelson, D.; Bolken, T.C.; Hruby, D.E.; O’Neill, M.H.; Sweetapple, G.; McCloughan, K.A. Polymorphic Forms of ST-246 and Methods of Preparation. U.S. Patent 10,045,964B2, 14 August 2018. [Google Scholar]
- Tyavanagimatt, S.R.; Anderson, M.A.C.L.S.; Weimers, W.C.; Nelson, D.; Bolken, T.C.; Hruby, D.E.; O’Neill, M.H.; Sweetapple, G.; McCloughan, K.A. Polymorphic Forms of ST-246 and Methods of Preparation. U.S. Patent 10,406,137B2, 10 September 2019. [Google Scholar]
- Tyavanagimatt, S.R.; Anderson, M.A.C.L.S.; Weimers, W.C.; Nelson, D.; Bolken, T.C.; Hruby, D.E.; O’Neill, M.H.; Sweetapple, G.; McCloughan, K.A. Polymorphic Forms of ST-246 and Methods of Preparation. U.S. Patent 10,933,050B2, 2 March 2021. [Google Scholar]
- Jordan, R.; Bailey, T.R.; Rippin, S.R.; Dai, D. Compounds, Compositions and Methods for Treatment and Prevention of Orthopoxvirus Infections and Associated Diseases. U.S. Patent 9,045,418B2, 2 June 2015. [Google Scholar]
- Tyavanagimatt, S.R.; Anderson, M.A.C.L.S.; Weimers, W.; Kasi, G.K.; Samuel, N.K.P.; Bolken, T.C.; Hruby, D.E. ST-246 Liquid Formulations and Methods. U.S. Patent 10,124,071B2, 13 November 2018. [Google Scholar]
- Tyavanagimatt, S.R.; Anderson, M.A.C.L.S.; Weimers, W.; Kasi, G.K.; Samuel, N.K.P.; Bolken, T.C.; Hruby, D.E. ST-246 Liquid Formulations and Methods. U.S. Patent 10,864,282B2, 15 December 2020. [Google Scholar]
- Tyavanagimatt, S.R.; Reeves, M.; Samuel, N.K.P.; Priebe, S.; Tan, Y.; Hruby, D.E. Rehydration of Micronized Tecovirimat Monohydrate. U.S. Patent 10,716,759B2, 21 July 2020. [Google Scholar]
- Tyavanagimatt, S.R.; Reeves, M.; Samuel, N.K.P.; Priebe, S.; Tan, Y.; Hruby, D.E. Rehydration of Micronized Tecovirimat monohydrate. U.S. Patent 10,406,103B2, 10 September 2019. [Google Scholar]
- Tyavanagimatt, S.R.; Samuel, N.K.P.; Paz, J.; Tan, Y.; Hruby, D.E. Amorphous Tecovirimat Preparation. U.S. Patent 9,670,158B2, 6 June 2017. [Google Scholar]
- Tyavanagimatt, S.R.; Samuel, N.K.P.; Paz, J.; Tan, Y.; Hruby, D.E. Amorphous Tecovirimat Preparation. U.S. Patent 9,889,119B2, 13 February 2018. [Google Scholar]
- Dai, D. Methods of Preparing Tecovirimat. U.S. Patent 10,155,723B2, 18 December 2018. [Google Scholar]
- Dai, D. Methods of Preparing Tecovirimat. U.S. Patent 10,662,155B2, 26 May 2020. [Google Scholar]
- Dai, D. Methods of Preparing Tecovirimat. U.S. Patent 9,546,137B2, 17 January 2017. [Google Scholar]
- Dai, D. Methods of Preparing Tecovirimat. U.S. Patent 9,862,683B2, 9 January 2018. [Google Scholar]
- Jordan, R.F.; Bailey, T.R.; Rippin, S.R.; Dai, D. Chemicals, Compositions, and Methods for Treatment and Prevention of Orthopoxvirus Infections and Associated Diseases. U.S. Patent 7,687,641B2, 30 March 2010. [Google Scholar]
- Dai, D.; Bailey, T.R.; Rippin, S.R.; Jordan, R. Chemicals, Compositions, and Methods for Treatment and Prevention of Orthopoxvirus Infections and Associated Diseases. Australian Patent 2,012,268,859B2, 5 May 2016. [Google Scholar]
- Tyavanagimatt, S.R.; Holt, K.; Tan, Y.; Anderson, M.A.C.L.S.; Hruby, D.E. ST-246 (Tecovirimat Monohydrate) Suspension Formulations. U.S. Patent 2,021,212,987A1, 15 July 2021. [Google Scholar]
- Zhong, W.; Yang, M.; Gong, W.; Wang, Y.; Gao, C.; Zhou, X.; Li, S. Injectable Pharmaceutical Composition of Tecovirimat and Preparation Method Thereof. U.S. Patent 11,369,587B2, 28 June 2022. [Google Scholar]
- Zhong, W.; Yang, M.; Gong, W.; Wang, Y.; Gao, C.; Zhou, X.; Li, S. Oral Pharmaceutical Composition of Tecovirimat and Preparation Method Thereof. U.S. Patent 11,318,115B2, 3 May 2022. [Google Scholar]
- Dai, Q.; Dong, M.; Yu, S.; Peng, B.; Wang, Y.; Zhu, M. Tecovirimat Dry Suspension and Preparation Method Thereof. Chinese Patent 102,406,617B, 28 August 2013. [Google Scholar]
- Almond, M.R.; Painter, G.R. Compounds, Compositions and Methods for the Treatment of Poxvirus Infections. U.S. Patent 8,642,577B2, 4 February 2014. [Google Scholar]
- Szalay, A.A.; Chen, N.; Yu, Y.A. Use of a Chemotherapeutic Agent in the Preparation of a Medicament for Treating or Ameliorating an Adverse Side Effect Associated with Oncolytic Viral Therapy. European Patent 2,202,297B1, 14 May 2014. [Google Scholar]
- Dai, Q.; Dong, M.; Hu, J. Compound ST-246 Containing a Crystal Water, crystal Thereof and Preparation Method Thereof. Chinese Patent 101,445,478B, 6 April 2011. [Google Scholar]
- Russo, A.T.; Grosenbach, D.W.; Chinsangaram, J.; Honeychurch, K.M.; Long, P.G.; Lovejoy, C.; Maiti, B.; Meara, I.; Hruby, D.E. An overview of tecovirimat for smallpox treatment and expanded anti-orthopoxvirus applications. Expert Rev. Anti-Infect. Ther. 2021, 19, 331–344. [Google Scholar] [CrossRef]
- Tran, M.T.; Grillo, J.A. Translation of drug interaction knowledge to actionable labeling. Clin. Pharmacol. Ther. 2019, 105, 1292–1295. [Google Scholar] [CrossRef]
- SIGA Human BioArmor. Press Releases. Available online: https://investor.siga.com/press-releases (accessed on 11 July 2022).
- Imran, M.; Fatima, W.; Alzahrani, A.K.; Suhail, N.; Alshammari, M.K.; Alghitran, A.A.; Alshammari, F.N.; Ghoneim, M.M.; Alshehri, S.; Shakeel, F. Development of therapeutic and prophylactic zinc compositions for use against COVID-19: A glimpse of the trends, inventions, and patents. Nutrients 2022, 14, 1227. [Google Scholar] [CrossRef]
- Imran, M.; Thabet, H.K.; Alaqel, S.I.; Alzahrani, A.R.; Abida; Alshammari, M.K.; Kamal, M.; Diwan, A.; Asdaq, S.M.B.; Alshehri, S. The therapeutic and prophylactic potential of quercetin against COVID-19: An outlook on the clinical studies, inventive compositions, and patent literature. Antioxidants 2022, 11, 876. [Google Scholar] [CrossRef]
- Imran, M.; Khan, S.A.; Abida; Alshammari, M.K.; Alkhaldi, S.M.; Alshammari, F.N.; Kamal, M.; Alam, O.; Asdaq, S.M.B.; Alzahrani, A.K.; et al. Nigella sativa L. and COVID-19: A glance at the anti-COVID-19 chemical constituents, clinical trials, inventions, and patent literature. Molecules 2022, 27, 2750. [Google Scholar]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Active Ingredient (Proprietary Name; Applicant) | Dosage Form (Route; Strength) | Approval Date (Marketing Status) | Exclusivity Code (Exclusivity Expiry Date) | Approved Indications |
|---|---|---|---|---|
| USFDA [22] | ||||
| Tecovirimat monohydrate (TPOXX; Siga Technologies Inc.) | Immediate-release capsule (Oral; 200 mg) | 13 July 2018 (Prescription) | New Chemical Entity (13 July 2023); Orphan Drug Exclusivity for capsule (13 July 2025) | Human smallpox disease caused by the variola virus in adults and pediatric patients weighing at least 13 Kg (capsule)/3 Kg (intravenous) |
| Solution (Intravenous; 10 mg/mL) | 18 May 2022 (Prescription) | |||
| EMA [16] | ||||
| Tecovirimat monohydrate (Tecovirimat SIGA; SIGA Technologies) | Immediate-release capsule (Oral; 200 mg) | 6 January 2022 (Prescription) | Exclusivity information is not available. However, ten years of marketing exclusivity is possible | Smallpox, monkeypox, cowpox, and complications due to replication of vaccinia virus following vaccination against smallpox |
| Health Canada [23,24] | ||||
| Tecovirimat monohydrate (TPOXX; Siga Technologies Inc.) | Immediate-release capsule (Oral; 200 mg) | 29 November 2021 (Prescription) | Marketing exclusivity expires on 29 November 2027 | Smallpox disease in adults and pediatric patients weighing at least 13 Kg |
| Parameter | Summary |
|---|---|
| Recommended dosage (Capsule 200 mg) | Adults: 600 mg two times a day; Pediatric patient (13 to <25 Kg): 200 mg two times a day; Pediatric patient (25 to <40 Kg): 400 mg two times a day; Pediatric patient (40 Kg or more): 600 mg two times a day; Treatment duration in all cases = 14 days; Capsule must be taken after half-hour of fatty meal which increases the absorption of the drug. The entire content present inside the capsule (recommended dose) can also be mixed carefully with milk (30 mL) or soft food (yogurt, applesauce, etc.) and administered to patients unable to swallow the capsule within 30 min [30,31]. |
| Recommended dosage (Intravenous) | Pediatric patient (3 to <35 Kg): 6 mg/Kg body weight two times a day over 6 h; Other patients (35 to <120 Kg): 200 mg two times a day over 6 h; Treatment duration in all cases = 14 days [34]. |
| Contraindications | None for capsule dosage form [30,31]. The intravenous injection should not be administered to individuals with serious renal impairments/injury [34]. |
| Warning / Precautions | Tecovirimat should be used cautiously in individuals with compromised immunity/renal/liver functions. Tecovirimat may be less efficacious in immunocompromised individuals [30,31,32]. |
| Adverse effects | Headache, dizziness, nausea, vomiting, diarrhea, and abdominal discomfort [30,31,32]. |
| Established drug interactions | Co-administration of Tecovirimat with repaglinide/midazolam may lead to hypoglycemia/reduced effect of midazolam [30,31,32]. |
| Absorption | Tmax = 4–6 h [25,30,31]; The drug absorption increases by 39% with fatty meal [25,30,31]. |
| Volume of distribution | After IV administration (200 mg) = 383 L; After oral administration (600 mg) = 1030 L; Blood to plasma ratio = 0.62–0.90; Protein binding = 77–82% [30,31,34]. |
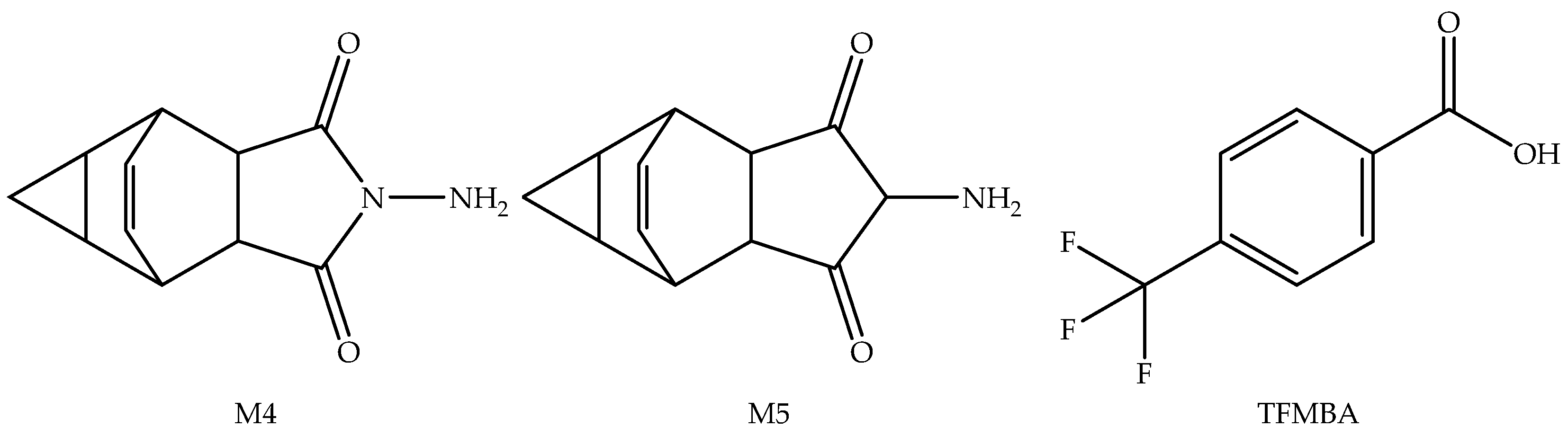
| Metabolism | Tecovirimat is a substrate of UGT1A4 and UGT1A1. Three important pharmacologically inactive metabolites, M4, M5, and TFMBA (Figure 4), have been identified. The glucuronide conjugates of Tecovirimat and M4 metabolite have been identified as the most abundant components in urine [31,34]. Tecovirimat and its M4 metabolites are inducers of CYP3A and CYP2B6. Therefore, the coadministration of Tecovirimat may reduce the therapeutic effect of drugs metabolized by CYP3A and CYP2B6 [31,34]. |
| Elimination | Urine (mainly as Tecovirimat conjugate) = 73%; Faeces (mainly unchanged) = 23% [30,31,34]. |
| Half-life | After IV administration (200 mg) = 21 h [34]; After oral administration (600 mg) = 19 h [30,31]. |
| Clearance | After oral administration (600 mg) of Tecovirimat = 31 L/h; After intravenous administration (200 mg) of Tecovirimat = 13 L/h [30,34]. |
| Overdose | LD50 (Single dose) = 2000 mg/Kg in mice/non-human primates [18,35]; No clinical overdose case reported [30,34]. The overdose cases must be monitored and handled based on signs and symptoms. Hemodialysis may not be an effective option for removing Tecovirimate from patients’ bodies [30,34]. |
| Study/Objective (Status; Condition; Intervention) | NCT Number (Sponsor & Collaborators; Location) | Clinical Phase (Study Type; Allocation; Numbers Enrolled; Comparison Group) | Primary Purpose (PP); Primary Outcome (PO); Study Starts Date (SSD); Study Completion Date (SCD); Last Update (LU); Results |
|---|---|---|---|
| Assessment of safety, tolerability, and pharmacokinetics of oral Tecovirimat (Completed; Orthopoxviral Disease; 400 mg and 600 mg Tecovirimat daily for 14 days) | NCT00907803 (SIGA Technologies and National Institutes of Health; United States) | 2 (Interventional; Randomized; 107; Matching Placebo capsules) | PP: Safety and tolerability of Tecovirimate; PO: Change in the pre-determined safety parameters; SSD: June 2009; SCD: January 2010 LU: 21 September 2010; Results: Available |
| Protocol to treat orthopoxvirus infection (Available; Monkeypox and smallpox; 600 mg daily dose of Tecovirimat) | NCT02080767 (U.S. Army Medical Research and Development Command; United States) | Not mentioned (Expanded Access; Not mentioned; Not mentioned; Not mentioned) | PP: Expanded Access; PO: Not mentioned; SSD: Not mentioned; SCD: Not mentioned; LU: 11 February 2021; Results: Not available |
| Animal Regulatory Rule-based study to evaluate the safety, tolerability, and pharmacokinetics of Tecovirimat (Completed; Smallpox; 600 mg of Tecovirimat two times a day for 45 days) | NCT02474589 (SIGA Technologies and BARDA; United States) | 3 (Interventional; Randomized; 449; Matching placebo capsule) | PP: Treatment; PO: Number of participants showing adverse effects; SSD: 19 June 2015; SCD: 24 August 2016; LU: 28 November 2017; Results: Available |
| Comparative safety and pharmacokinetic parameter evaluation of Form I and Form V of Tecovirimat (Completed; Monkeypox and smallpox; Administration of 400 mg of Form I and Form V of Tecovirimat for 13 days) | NCT00728689 (SIGA Technologies and National Institutes of Health; United States) | 1 (Interventional; Randomized; 12; Groups administered with crystalline Form I (1–3 days) and Form V (4–13 days) and vice versa) | PP: Treatment; PO: Pharmacokinetic parameters of Form I vs. Form V; SSD: August 2008; SCD: October 2008; LU: 29 June 2015; Results: Available |
| Treatment of orthopoxvirus infection with intravenous Tecovirimat (Available; orthopoxvirus infection; Intravenous Tecovirimat (10 mg/mL)) | NCT05380752 (U.S. Army Medical Research and Development Command and SIGA Technologies; United States) | Not mentioned (Expanded Access; Not mentioned; Not mentioned; Not mentioned) | PP: Treatment; PO: Not mentioned; SSD: Not mentioned; SCD: Not mentioned; LU: 19 May 2022; Results: Not available |
| Observational study on smallpox patients treated with Tecovirimat capsules (Enrolling by invitation; Smallpox; Tecovirimat (600 mg) two times a day for 14 days) | NCT03972111 (SIGA Technologies and BARDA; United States) | 4 (Observational; Observational; 100; Not mentioned) | PP: Safety and survival status of patients; PO: Patient survival status after 44 days post the first dose; SSD: 1 January 2020; SCD: 30 September 2024; LU: 14 February 2022; Results: Not available |
| Evaluation of the safety, tolerability, and pharmacokinetics of Tecovirimat (Completed; Healthy volunteers; Single oral dose (250 mg, 400 mg, or 800 mg) for 21 days in fed healthy volunteers) | NCT00431951 (SIGA Technologies and National Institute of Allergy and Infectious Diseases; United States) | 1 (Interventional; Randomized; 30; Matching placebo capsule) | PP: Treatment; PO: Changes in the pre-determined safety/tolerability parameters; SSD: February 2007; SCD: February 2008; LU: 27 July 2017; Results: Available |
| Animal Regulatory Rule-based evaluation of the safety, tolerability, and pharmacokinetics of Tecovirimat (Recruiting; Smallpox; Three capsules (3 × 200 mg) two times a day for 28 days) | NCT04971109 (SIGA Technologies and United States Department of Defense; United States) | 3 (Interventional; Randomized; 445; Matching placebo capsule) | PP: Treatment; PO: Laboratory / physical test, Heart / respiratory parameters, Cmax/Tmax; SSD: 29 March 2022; SCD: 30 June 2023; LU: 27 May 2022; Results: Not available |
| Drug interaction study of oral Tecovirimat in Healthy subjects (Not yet recruiting; Smallpox; Single oral dose (600 mg) of Tecovirimat co-administered with a single oral dose of sevelamer carbonate (1600 mg tablet), sucroferric oxyhydroxide (500 mg tablet), calcium acetate (1334 mg tablet), or lanthanum carbonate (500 mg tablet)) | NCT04485039 (SIGA Technologies, BARDA, and PPD; United States) | 4 (Interventional; Randomized; 44; Not mentioned) | PP: Drug interaction study; PO: Plasma parameters of Tecovirimat; SSD: 15 May 2022; SCD: 23 April 2023; LU: 14 January 2022; Results: Not available |
| Safety and pharmacokinetic parameter evaluation of oral Tecovirimat when administered for 28 days (Recruiting; Smallpox; Oral Tecovirimat (600 mg) two times a day for 28 days and a single subcutaneous dose (0.5 mL) of JYNNEOS vaccine on day one and day 29) | NCT04957485 (SIGA Technologies and United States Department of Defense; United States) | 2 (Interventional; Randomized; 445; Matching placebo of oral Tecovirimat and JYNNEOS vaccine) | PP: Treatment; PO: Geometric mean titer of vaccinia virus-neutralizing antibodies; SSD: 5 January 2022; SCD: 31 October 2022; LU: 27 May 2022; Results: Not available |
| Determination of the pharmacokinetic profile of Tecovirimat in individuals weighing > 120 Kg (Completed; Smallpox; Oral Tecovirimat capsule (200 × 3 = 600 mg) two times a day for seven days in subjects weighing > 120 Kg) | NCT04392739 (SIGA Technologies and BARDA; United States) | 4 (Interventional; Not mentioned; 34; Not mentioned) | PP: Dosing regimen for people > 120 Kg; PO: Pharmacokinetic parameters after days 1, 2, 6, 8, and 9; SSD: 19 July 2019; SCD: 5 December 2019; LU: 21 May 2020; Results: Available |
| Tecovirimat to treat smallpox (Withdrawn; Vaccinia; Protocol not provided) | NCT00303225 (National Institute of Allergy and Infectious Diseases and National Institutes of Health Clinical Center; United States) | 1 (Interventional; Not mentioned; Zero; Not mentioned) | PP: Treatment; PO: Not mentioned; SSD: 13 March 2006; SCD: 4 August 2006; LU: 2 July 2017; Results: Not available |
| S. No. | Patent/Application Number (Status) | Summary of the Claims |
|---|---|---|
| Patents/Patent Applications Filed by SIGA Technologies | ||
| 1 | US9339466B2 (Patented case) | This OB-listed patent claims a crystalline polymorphic Form I of Tecovirimat monohydrate, its pharmaceutical composition, and a method of preparing polymorphic Form I of Tecovirimat monohydrate [28]. |
| 2 | US8124643B2 (Patented case) | This OB-listed patent discloses Tecovirimat and claims a pharmaceutical composition containing a therapeutically effective amount of Tecovirimat and a pharmaceutically acceptable carrier [48]. |
| 3 | US7737168B2 (Patented case) | This OB listed patent claims a method of preventing/treating orthopoxvirus infection (monkeypox, smallpox, cowpox, vaccinia, buffalopox, camelpox, elephantpox, and rabbitpox) employing a therapeutically effective amount (0.125–250 mg/Kg/day) of Tecovirimat [49]. |
| 4 | US8802714B2 (Patented case) | This OB-listed patent claims a method of preventing/treating orthopoxvirus infection utilizing an adequate amount of a mixture of Tecovirimat (95% w/w or more) and one of its isomers (5% or less w/w) [50]. |
| 5 | US8530509B2 (Patented case) | This OB-listed patent claims a pharmaceutical composition comprising an adequate amount of a mixture of Tecovirimat (95% w/w or more) and one of its isomers (5% or less w/w) for preventing/treating orthopoxvirus infection [51]. |
| 6 | US10576165B2 (Patented case) | This OB-listed patent claims a unit liquid formulation containing Tecovirimat (2 to 20 mg/mL) and hydroxypropyl-β-cyclodextrin (125 to 400 mg/mL) [52]. |
| 7 | US9233097B2 (Patented case) | This OB-listed patent claims a liquid formulation comprising an adequate amount of Tecovirimat, hydroxypropyl-β-cyclodextrin, and sufobutyl-ether-β-cyclodextrin [53]. |
| 8 | US9907859B2 (Patented case) | This OB-listed patent claims to treat orthopoxvirus infection or eczema utilizing a liquid composition (injectable or topical) comprising Tecovirimat and hydroxypropyl-β-cyclodextrin, and sulfobutyl-ether-β-cyclodextrin [54]. |
| 9 | US8039504B2 (Patented case) | This OB-listed patent claims a pharmaceutical composition (capsule) containing Tecovirimat and additional ingredients. It also claims a unit pharmaceutical composition containing Tecovirimat (200 mg), lactose monohydrate, croscarmellose sodium, colloidal silicon dioxide, hydroxypropyl methylcellulose, sodium lauryl sulfate, magnesium stearate, and microcrystalline cellulose [55]. |
| 10 | US7956197B2 (Patented case) | A process for preparing Tecovirimat [56]. |
| 11 | US9744154B2 (Patented case) | A polymorphic Form II of Tecovirimat and its preparation method [57]. |
| 12 | US10045964B2 (Patented case) | A polymorphic Form III of Tecovirimat and a method to prepare it [58]. |
| 13 | US10406137B2 (Patented case) | A polymorphic Form IV of Tecovirimat [59]. |
| 14 | US10933050B2 (Patented case) | A polymorphic Form VI of Tecovirimat and a method of its preparation [60]. |
| 15 | US9045418B2 (Patented case) | A process for preparing Tecovirimat [61]. |
| 16 | US10124071B2 (Patented case) | A process for making a liquid formulation comprising Tecovirimat (including polymorphic Form I, Form II, Form III, Form IV, Form V, and Form VI) and cyclodextrin [62]. |
| 17 | US10864282B2 (Patented case) | A process for preparing water-soluble lyophilized formulation of Tecovirimat with cyclodextrin [63]. |
| 18 | US10716759B2 (Patented case) | A method of reducing the particle size of dehydrated Tecovirimat monohydrate (Form I) [64]. |
| 19 | US10406103B2 (Patented case) | A method of hydrating Tecovirimat monohydrate (Form I) [65]. |
| 20 | US9670158B2 (Patented case) | A method of preparing amorphous Tecovirimat [66]. |
| 21 | US9889119B2 (Patented case) | A method of preparing amorphous solid dispersion of Tecovirimat by the spray-drying process [67]. |
| 22 | US10155723B2 (Patented case) | A method of producing Tecovirimat [68]. |
| 23 | US10662155B2 (Patented case) | A method of producing Tecovirimat [69]. |
| 24 | US9546137B2 (Patented case) | A method of producing Tecovirimat [70]. |
| 25 | US9862683B2 (Patented case) | A method of producing Tecovirimat [71]. |
| 26 | US7687641B2 (Patented case) | A method of producing Tecovirimat [72]. |
| 27 | AU2012268859B2 (Patented case) | A method of producing Tecovirimat [73]. |
| 28 | US2021212987A1 (Notice of Allowance mailed) | A dry suspension of polymorphic Form I of Tecovirimat and simethicone and its use to treat orthopoxvirus infection [74]. |
| Important Patents/Patent Applications Filed by Other Applicants | ||
| 29 | US11369587B2 (Patented case) | This patent is assigned to the Institute of Pharmacology and Toxicology Academy of Military Medical Sciences, China. It claims an injectable composition comprising Tecovirimat, cyclodextrin, and meglumine [75]. |
| 30 | US11318115B2 (Patented case) | This patent is assigned to the Institute of Pharmacology and Toxicology Academy of Military Medical Sciences, China. It claims a composition comprising Tecovirimat, cyclodextrin, and meglumine [76]. |
| 31 | CN102406617B (Patented case) | This patent is assigned to the Institute of Bioengineering, The Academy of Military Medical Sciences, China. It claims a suspension composition comprising Tecovirimat, lactose, sodium carboxymethyl cellulose, dimethyl silicone oil, silica gel, and aspartame [77]. |
| 32 | US8642577B2 (Patented case) | This patent is filed by Almond et al. It claims a method of treating pox virus infection using cidofovir in combination with Tecovirimat [78]. |
| 33 | EP2202297B1 (Patented case) | This patent is assigned to Genelux Corporation. It claims to use Tecovirimat to treat an adverse side effect associated with cancer oncolytic pox virus therapy [79]. |
| 34 | CN101445478B (Patented case) | This patent is assigned to the Institute of Biological Engineering, Academy of Military Medical Sciences, China, and claims a process for making Tecovirimat monohydrate [80]. |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Almehmadi, M.; Allahyani, M.; Alsaiari, A.A.; Alshammari, M.K.; Alharbi, A.S.; Hussain, K.H.; Alsubaihi, L.I.; Kamal, M.; Alotaibi, S.S.; Alotaibi, A.N.; et al. A Glance at the Development and Patent Literature of Tecovirimat: The First-in-Class Therapy for Emerging Monkeypox Outbreak. Viruses 2022, 14, 1870. https://doi.org/10.3390/v14091870
Almehmadi M, Allahyani M, Alsaiari AA, Alshammari MK, Alharbi AS, Hussain KH, Alsubaihi LI, Kamal M, Alotaibi SS, Alotaibi AN, et al. A Glance at the Development and Patent Literature of Tecovirimat: The First-in-Class Therapy for Emerging Monkeypox Outbreak. Viruses. 2022; 14(9):1870. https://doi.org/10.3390/v14091870
Chicago/Turabian StyleAlmehmadi, Mazen, Mamdouh Allahyani, Ahad Amer Alsaiari, Mohammed Kanan Alshammari, Abrar Saleh Alharbi, Khansa Hamza Hussain, Lojain Ibrahim Alsubaihi, Mehnaz Kamal, Shahad Saleh Alotaibi, Atheer Nasser Alotaibi, and et al. 2022. "A Glance at the Development and Patent Literature of Tecovirimat: The First-in-Class Therapy for Emerging Monkeypox Outbreak" Viruses 14, no. 9: 1870. https://doi.org/10.3390/v14091870