
Interventions for Improving Long COVID-19 Symptomatology: A Systematic Review

 , , , , , , , ,
, , , , , , , ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Protocol Registration
2.2. Research Question
2.3. Information Sources and Search Strategies
2.4. Eligibility Criteria
2.5. Study Selection
2.6. Data Extraction
2.7. Risk of Bias Assessment
2.8. Data Synthesis
3. Results
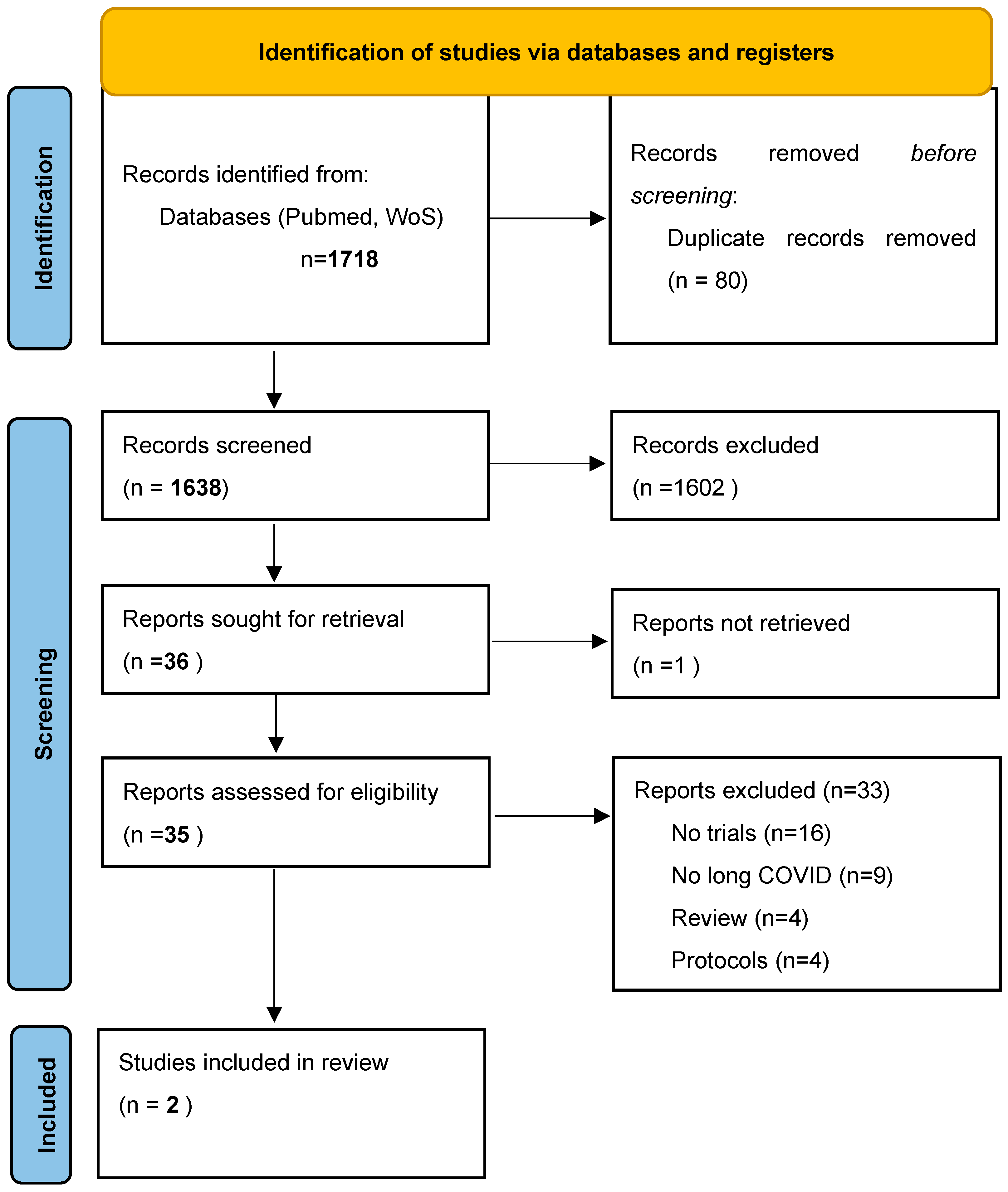
3.1. Literature Search
3.2. Descriptive Characteristics and Risk of Bias
3.3. Main Findings
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Acknowledgments
Conflicts of Interest
References
- Callard, F.; Perego, E. How and why patients made Long Covid. Soc. Sci. Med. 2021, 268, 113426. [Google Scholar] [CrossRef]
- Lopez-Leon, S.; Wegman-Ostrosky, T.; Perelman, C.; Sepulveda, R.; Rebolledo, P.A.; Cuapio, A.; Villapol, S. More than 50 long-term effects of COVID-19: A systematic review and meta-analysis. Sci. Rep. 2021, 11, 16144. [Google Scholar] [CrossRef] [PubMed]
- Di Gennaro, F.; Petrosillo, N. New endemic and pandemic pathologies with interhuman airborne transmission through ear, nose and throat anatomical sites. Acta Otorhinolaryngol. Ital. 2022, 42 (Suppl. 1), S5–S13. [Google Scholar] [CrossRef] [PubMed]
- Lennon, P.; Crotty, M.; Fenton, J.E. Infectious mononucleosis. BMJ 2015, 350, h1825. [Google Scholar] [CrossRef] [PubMed]
- Lee, S.H.; Shin, H.-S.; Park, H.Y.; Kim, J.L.; Lee, J.J.; Lee, H.; Won, S.D.; Han, W. Depression as a mediator of chronic fatigue and post-traumatic stress symptoms in Middle East respiratory syndrome survivors. Psychiatry Investig. 2019, 16, 59. [Google Scholar] [CrossRef]
- Dennis, A.; Wamil, M.; Alberts, J.; Oben, J.; Cuthbertson, D.J.; Wootton, D.; Crooks, M.; Gabbay, M.; Brady, M.; Hishmeh, L.; et al. Multiorgan impairment in low-risk individuals with post-COVID-19 syndrome: A prospective, community-based study. BMJ Open 2021, 11, e048391. [Google Scholar]
- Townsend, L.; Dowds, J.; O’Brien, K.; Sheill, G.; Dyer, A.H.; O’Kelly, B.; Hynes, J.P.; Mooney, A.; Dunne, J.; Cheallaigh, C.N.; et al. Persistent poor health after COVID-19 is not associated with respiratory complications or initial disease severity. Ann. Am. Thorac. Soc. 2021, 18, 997–1003. [Google Scholar] [CrossRef]
- Zimmermann, P.; Pittet, L.F.; Curtis, N. How common is long COVID in children and adolescents? Pediatric Infect. Dis. J. 2021, 40, e482. [Google Scholar] [CrossRef]
- Cares-Marambio, K.; Montenegro-Jiménez, Y.; Torres-Castro, R.; Vera-Uribe, R.; Torralba, Y.; Alsina-Restoy, X.; Vasconcello-Castillo, L.; Villaro, J. Prevalence of potential respiratory symptoms in survivors of hospital admission after coronavirus disease 2019 (COVID-19): A systematic review and meta-analysis. Chronic Respir. Dis. 2021, 18, 14799731211002240. [Google Scholar] [CrossRef]
- Aiyegbusi, O.L.; Hughes, S.E.; Turner, G.; Rivera, S.C.; McMullan, C.; Chandan, J.S.; Shamil, H.; Gary, P.; Haf, D.E.; Krishnarajar, N.; et al. Symptoms, complications and management of long COVID: A review. J. R. Soc. Med. 2021, 114, 428–442. [Google Scholar] [CrossRef]
- Higgins, V.; Sohaei, D.; Diamandis, E.P.; Prassas, I. COVID-19: From an acute to chronic disease? Potential long-term health consequences. Crit. Rev. Clin. Lab. Sci. 2021, 58, 297–310. [Google Scholar] [CrossRef] [PubMed]
- Higgins, J.P.; Thomas, J.; Chandler, J.; Cumpston, M.; Li, T.; Page, M.J.; Welch, V. Cochrane Handbook for Systematic Reviews of Interventions; John Wiley & Sons: Hoboken, NJ, USA, 2019. [Google Scholar]
- Sarkis-Onofre, R.; Catalá-López, F.; Aromataris, E.; Lockwood, C. How to properly use the PRISMA Statement. Syst. Rev. 2021, 10, 117. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization (WHO). A Clinical Case Definition of Post COVID-19 Condition by a Delphi Consensus, 6 October 2021; World Health Organization: Geneva, Switzerland, 2021.
- Hawkins, J.; Hires, C.; Keenan, L.; Dunne, E. Aromatherapy blend of thyme, orange, clove bud, and frankincense boosts energy levels in post-COVID-19 female patients: A randomized, double-blinded, placebo controlled clinical trial. Complement. Ther. Med. 2022, 67, 102823. [Google Scholar] [CrossRef] [PubMed]
- D’Ascanio, L.; Vitelli, F.; Cingolani, C.; Maranzano, M.; Brenner, M.; Di Stadio, A. Randomized clinical trial “olfactory dysfunction after COVID-19: Olfactory rehabilitation therapy vs. intervention treatment with Palmitoylethanolamide and Luteolin”: Preliminary results. Eur. Rev. Med. Pharmacol. Sci. 2021, 25, 4156–4162. [Google Scholar]
- Zahra, S.A.; Iddawela, S.; Pillai, K.; Choudhury, R.Y.; Harky, A. Can symptoms of anosmia and dysgeusia be diagnostic for COVID-19? Brain Behav. 2020, 10, e01839. [Google Scholar] [CrossRef] [PubMed]
- Hummel, T.; Sekinger, B.; Wolf, S.R.; Pauli, E.; Kobal, G. ‘Sniffin’ sticks’: Olfactory performance assessed by the combined testing of odor identification, odor discrimination and olfactory threshold. Chem. Senses 1997, 22, 39–52. [Google Scholar] [CrossRef]
- Butowt, R.; von Bartheld, C.S. Anosmia in COVID-19: Underlying mechanisms and assessment of an olfactory route to brain infection. Neuroscientist 2021, 27, 582–603. [Google Scholar] [CrossRef]
- Philpott, C.; Dixon, J.; Boak, D. Qualitative Olfactory Disorders: Patient experiences and self-management. Allergy Rhinol. 2021, 12, 21526567211004251. [Google Scholar] [CrossRef]
- Parker, J.K.; Kelly, C.E.; Smith, B.C.; Kirkwood, A.F.; Hopkins, C.; Gane, S. Patients’ perspectives on qualitative olfactory dysfunction: Thematic analysis of social media posts. JMIR Form. Res. 2021, 5, e29086. [Google Scholar] [CrossRef]
- Kwon, C.Y.; Lee, B. Complementary and integrative medicines for behavioral and psychological symptoms of dementia: Overview of systematic reviews. Explore 2022. [Google Scholar] [CrossRef]
- Bested, A.C.; Marshall, L.M. Review of Myalgic Encephalomyelitis/Chronic Fatigue Syndrome: An evidence-based approach to diagnosis and management by clinicians. Rev. Environ. Health 2015, 30, 223–249. [Google Scholar] [CrossRef] [PubMed]
- Leow, M.K.S.; Kwek, D.S.K.; Ng, A.W.K.; Ong, K.C.; Kaw, G.J.L.; Lee, L.S.U. Hypocortisolism in survivors of severe acute respiratory syndrome (SARS). Clin. Endocrinol. 2005, 63, 197–202. [Google Scholar] [CrossRef] [PubMed]
- Philip, K.E.J.; Owles, H.; McVey, S.; Pagnuco, T.; Bruce, K.; Brunjes, H.; Banya, W.; Mollica, J.; Lound, A.; Zumpe, S.; et al. An online breathing and wellbeing programme (ENO Breathe) for people with persistent symptoms following COVID-19: A parallel-group, single-blind, randomised controlled trial. Lancet Respir. Med. 2022. [Google Scholar] [CrossRef]
- Al-Aly, Z.; Bowe, B.; Xie, Y. Long COVID after breakthrough SARS-CoV-2 infection. Nat. Med. 2022, 28, 1461–1467. [Google Scholar] [CrossRef]
- Varnai, R.; Molnar, T.; Zavori, L.; Tőkés-Füzesi, M.; Illes, Z.; Kanizsai, A.; Csecsei, P. Serum Level of Anti-Nucleocapsid, but Not Anti-Spike Antibody, Is Associated with Improvement of Long COVID Symptoms. Vaccines 2022, 10, 165. [Google Scholar] [CrossRef]
- Di Gennaro, F.; Marotta, C.; Locantore, P.; Pizzol, D.; Putoto, G. Malaria and COVID-19: Common and Different Findings. Trop. Med. Infect. Dis. 2020, 5, 141. [Google Scholar] [CrossRef]
- Baronti, A.; Gentile, F.; Manetti, A.C.; Scatena, A.; Pellegrini, S.; Pucci, A.; Franzini, M.; Castiglione, V.; Maiese, A.; Giannoni, A.; et al. Myocardial Infarction Following COVID-19 Vaccine Administration: Post Hoc, Ergo Propter Hoc? Viruses 2022, 14, 1644. [Google Scholar] [CrossRef]
- Segala, F.V.; Bavaro, D.F.; Di Gennaro, F.; Salvati, F.; Marotta, C.; Saracino, A.; Murri, R.; Fantoni, M. Impact of SARS-CoV-2 Epidemic on Antimicrobial Resistance: A Literature Review. Viruses 2021, 13, 2110. [Google Scholar] [CrossRef]
- Maiese, A.; Baronti, A.; Manetti, A.C.; Di Paolo, M.; Turillazzi, E.; Frati, P.; Fineschi, V. Death after the Administration of COVID-19 Vaccines Approved by EMA: Has a Causal Relationship Been Demonstrated? Vaccines 2022, 10, 308. [Google Scholar] [CrossRef]
- Crook, H.; Raza, S.; Nowell, J.; Young, M.; Edison, P. Long covid—Mechanisms, risk factors, and management. BMJ 2021, 374, n1648. [Google Scholar] [CrossRef]
- Peluso, M.J.; Deeks, S.G. Early clues regarding the pathogenesis of long-COVID. Trends Immunol. 2022, 43, 268–270. [Google Scholar] [CrossRef] [PubMed]
- Veronese, N.; Smith, L.; Di Gennaro, F.; Bruyère, O.; Yang, L.; Demurtas, J.; Maggi, S.; Sabico, S.; Al-Daghri, N.M.; Barbagallo, M.; et al. Influenza Vaccination and COVID-19 Outcomes in People Older than 50 Years: Data from the Observational Longitudinal SHARE Study. Vaccines 2022, 10, 899. [Google Scholar] [CrossRef] [PubMed]
- Di Gennaro, F.; Veronese, N.; Marotta, C.; Shin, J.I.; Koyanagi, A.; Silenzi, A.; Antunes, M.; Saracino, A.; Bavaro, D.F.; Soysal, P.; et al. Human Monkeypox: A Comprehensive Narrative Review and Analysis of the Public Health Implications. Microorganisms 2022, 10, 1633. [Google Scholar] [CrossRef]
- Cochrane COVID-19 Study Register. Available online: https://covid19.cochrane.org/?q=k(Long%20and%20covid).k(%22long%20covid%22).c(study-types/interventional:Interventional).c(intervention-assignments/randomised:Randomised)&pn=1 (accessed on 15 May 2022).


{kind=link}
| Author | Year | Country | Sample Size | Definition of Long COVID-19 | Sign or Symptom Investigated | Methods for COVID19 Diagnosis | Age | % Females | Follow-Up (Months) | Type of Intervention | Outcome | Descriptive Results |
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| D’Ascanio | 2021 | Italy | 12 | A condition that occurs in individuals with a history of probable or confirmed SARS-CoV-2 infection, usually 3 months from the onset of COVID-19 with symptoms that last for at least 2 months and cannot be explained by an alternative diagnosis | anosmia/hyposmia persisting ≥ 90 days after negative COVID-19 nasopharyngeal swab | nasopharyngeal swab | 42.2 (14.1) | 67% | 1 | olfactory training/stimulation through Sniffin Sticks, administered twice every day (10-min session) for 30 days plus daily treatment with PEA/Luteolin oral supplement | Sniffin scores | Patients taking supplement had greater improvement in Sniffin score than controls (mean change in Sniffin score = 2 for CG and 4 for TG; KW: p = 0.01) |
| Hawkins | 2022 | US | 44 | fatigue not prior to COVID-19 infection and recovered at least 5 months before | fatigue | nasopharyngeal swab | 19–49 | 100% | 0.5 | aromatherapy | Multidimensional Fatigue Symptom Inventory, Short Form | Individuals who inhaled the essential oil blend for 2 weeks had significantly lower fatigue scores. Significant results were found on the subscales of global, behavioral, general, and mental fatigue, as well as vigor. |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Veronese, N.; Bonica, R.; Cotugno, S.; Tulone, O.; Camporeale, M.; Smith, L.; Trott, M.; Bruyere, O.; Mirarchi, L.; Rizzo, G.; et al. Interventions for Improving Long COVID-19 Symptomatology: A Systematic Review. Viruses 2022, 14, 1863. https://doi.org/10.3390/v14091863
Veronese N, Bonica R, Cotugno S, Tulone O, Camporeale M, Smith L, Trott M, Bruyere O, Mirarchi L, Rizzo G, et al. Interventions for Improving Long COVID-19 Symptomatology: A Systematic Review. Viruses. 2022; 14(9):1863. https://doi.org/10.3390/v14091863
Chicago/Turabian StyleVeronese, Nicola, Roberta Bonica, Sergio Cotugno, Ottavia Tulone, Michele Camporeale, Lee Smith, Mike Trott, Olivier Bruyere, Luigi Mirarchi, Giuseppina Rizzo, and et al. 2022. "Interventions for Improving Long COVID-19 Symptomatology: A Systematic Review" Viruses 14, no. 9: 1863. https://doi.org/10.3390/v14091863