LCA of Hospital Solid Waste Treatment Alternatives in a Developing Country: The Case of District Swat, Pakistan

 , ,
, ,  and
and
Abstract
:1. Introduction
2. Materials and Methods
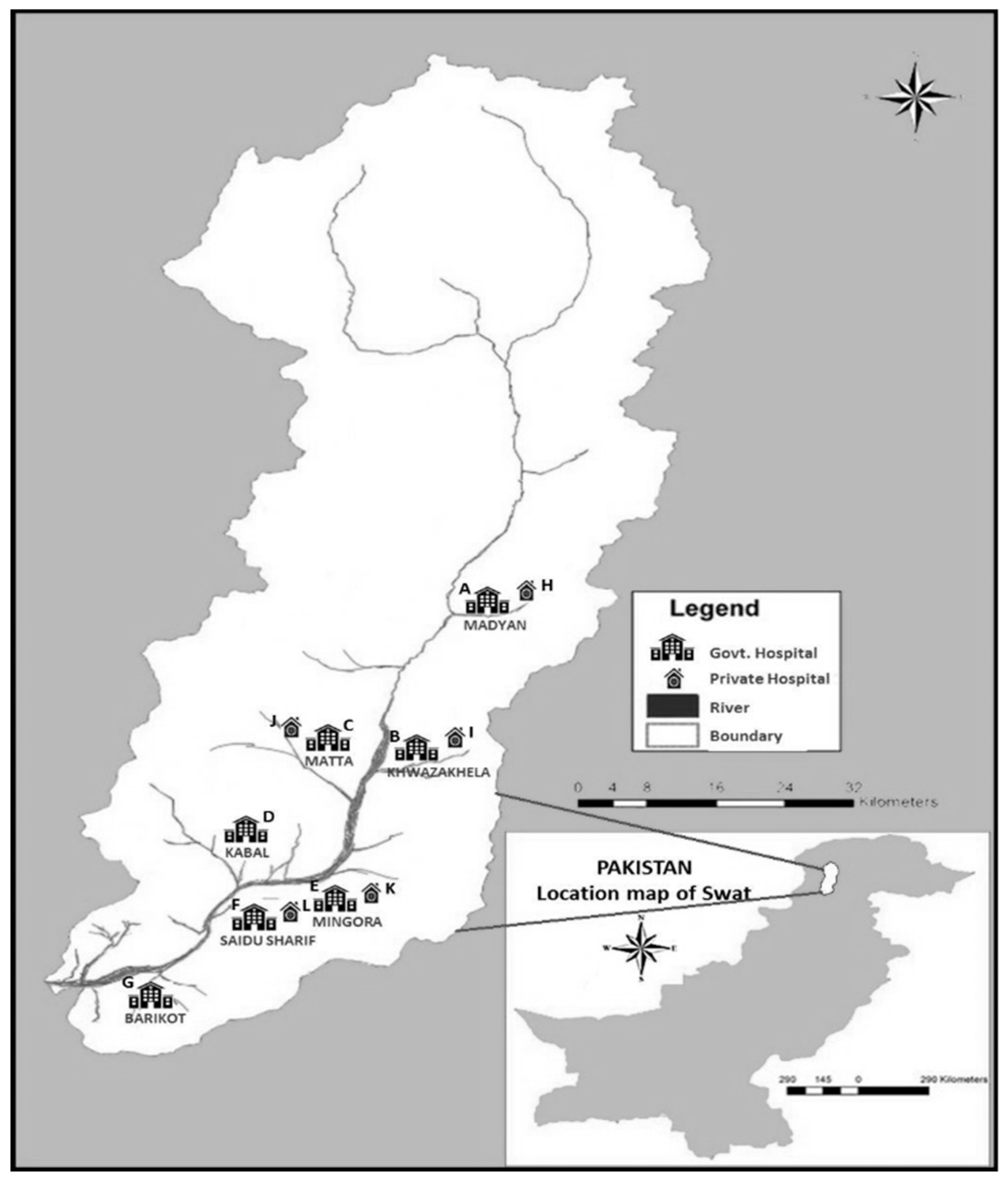
2.1. Geographical Boundaries of the Study
2.1.1. Government-Owned Hospitals
2.1.2. Private-Owned Hospitals
2.1.3. Field Data Collection
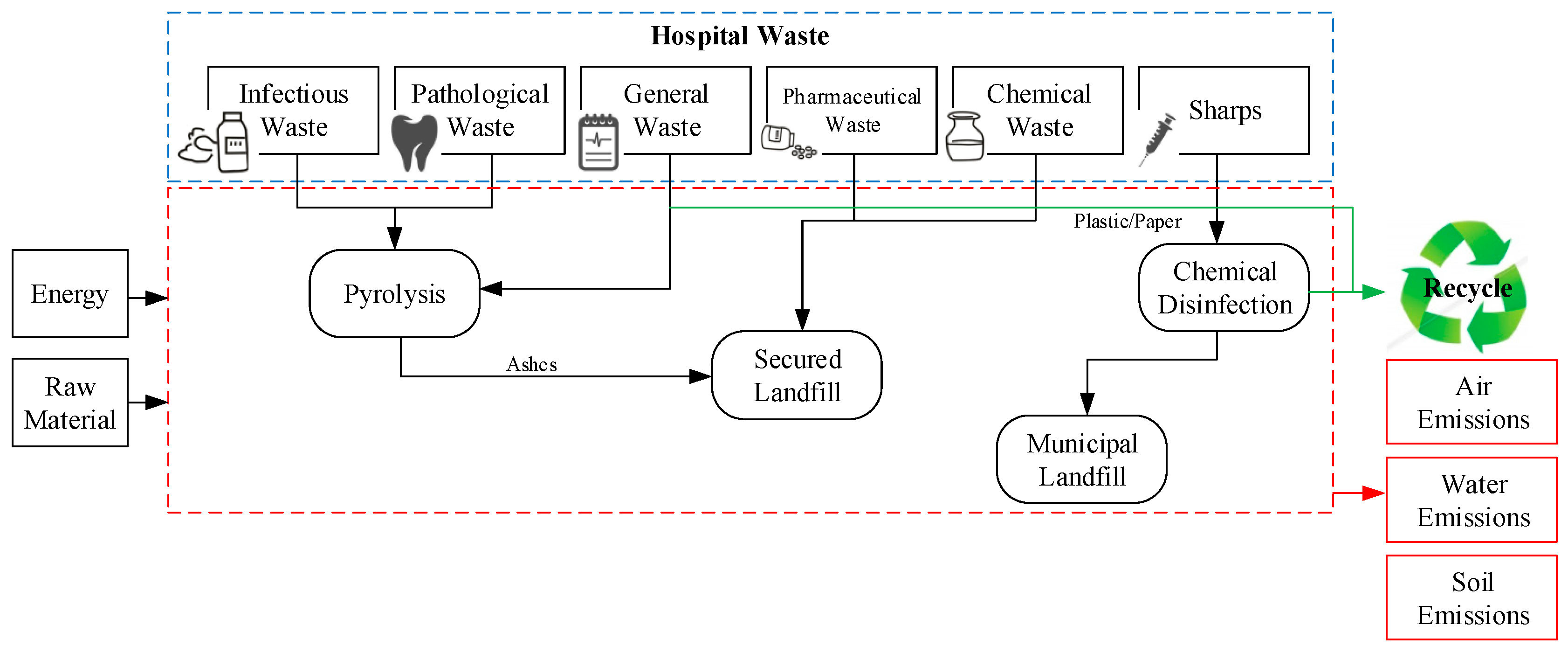
2.2. Medical Waste Classification and Optimal Treatment Options
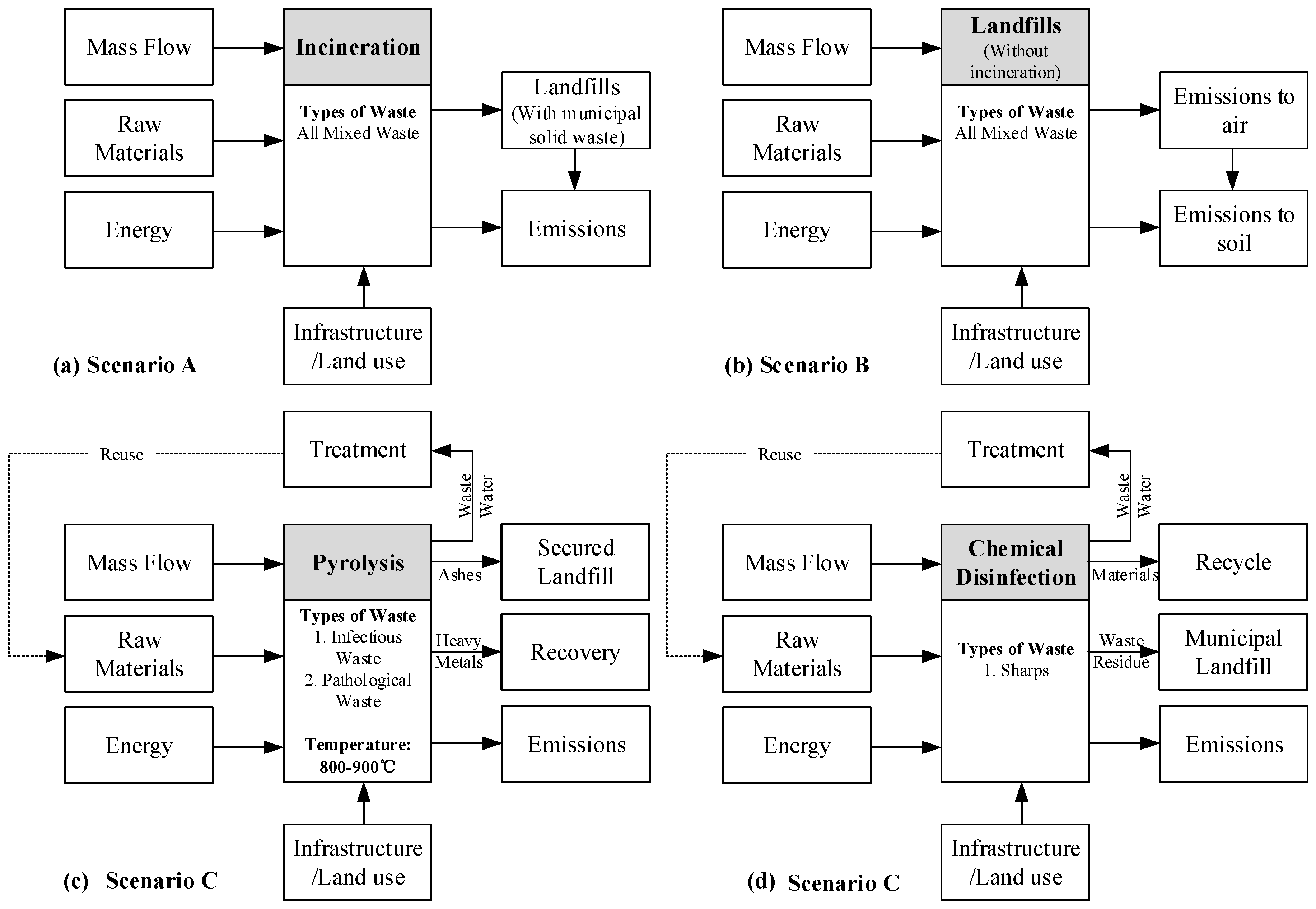
2.3. Considered Scenarios
2.3.1. Scenario A: Incineration and Landfilling
2.3.2. Scenario B: Direct Landfilling
2.3.3. Scenario C: Up-to-Date Treatment Technologies
Waste Combustion through Pyrolysis
Waste Chemical Disinfection
2.4. Chosen Scenarios
2.5. Life-Cycle Assessment (LCA) and Functional Unit Definition
3. Results
3.1. Quantitative Analysis of Waste in Concern Hospitals
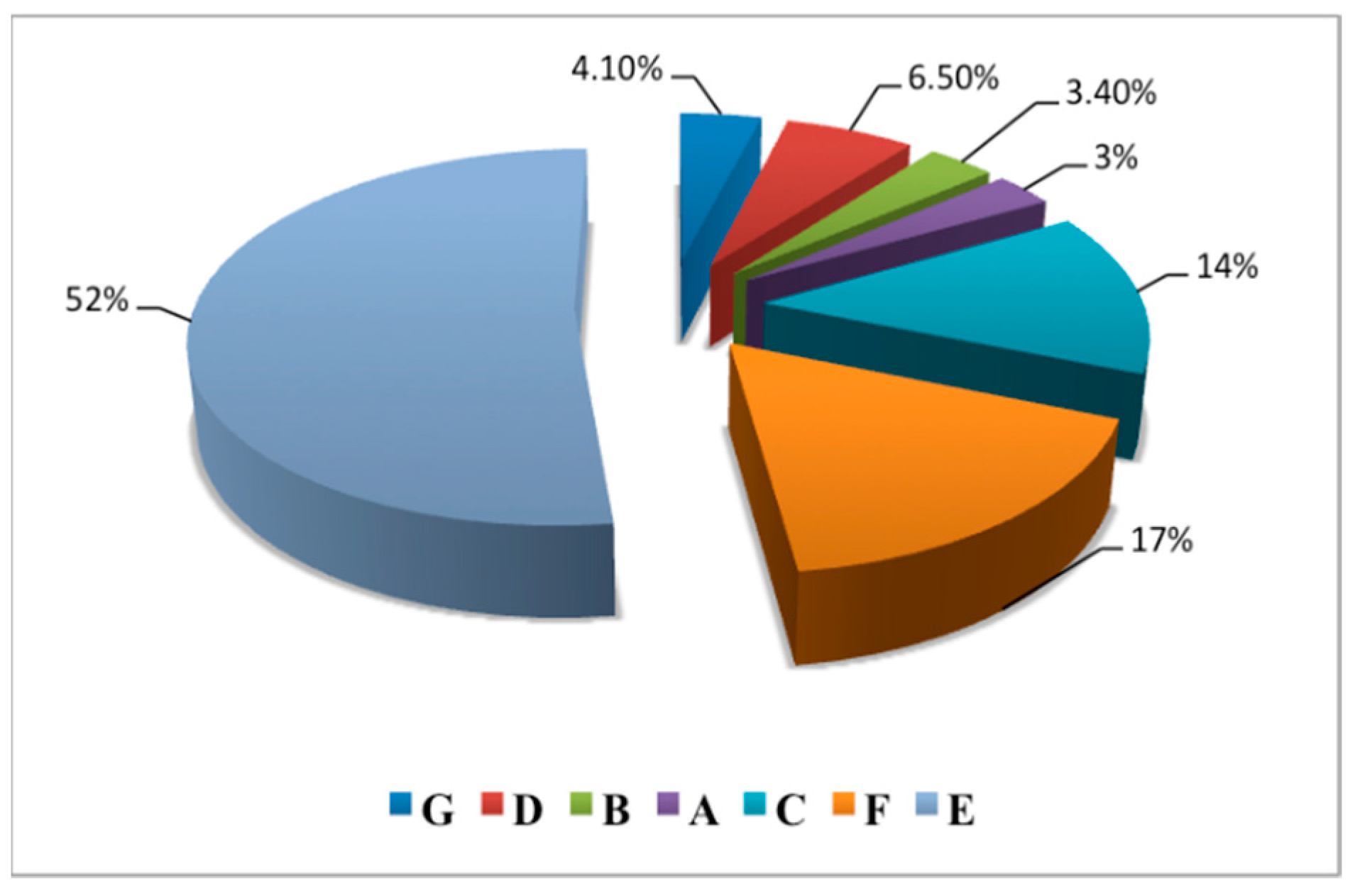
3.1.1. Hospital Solid Waste Production Rate
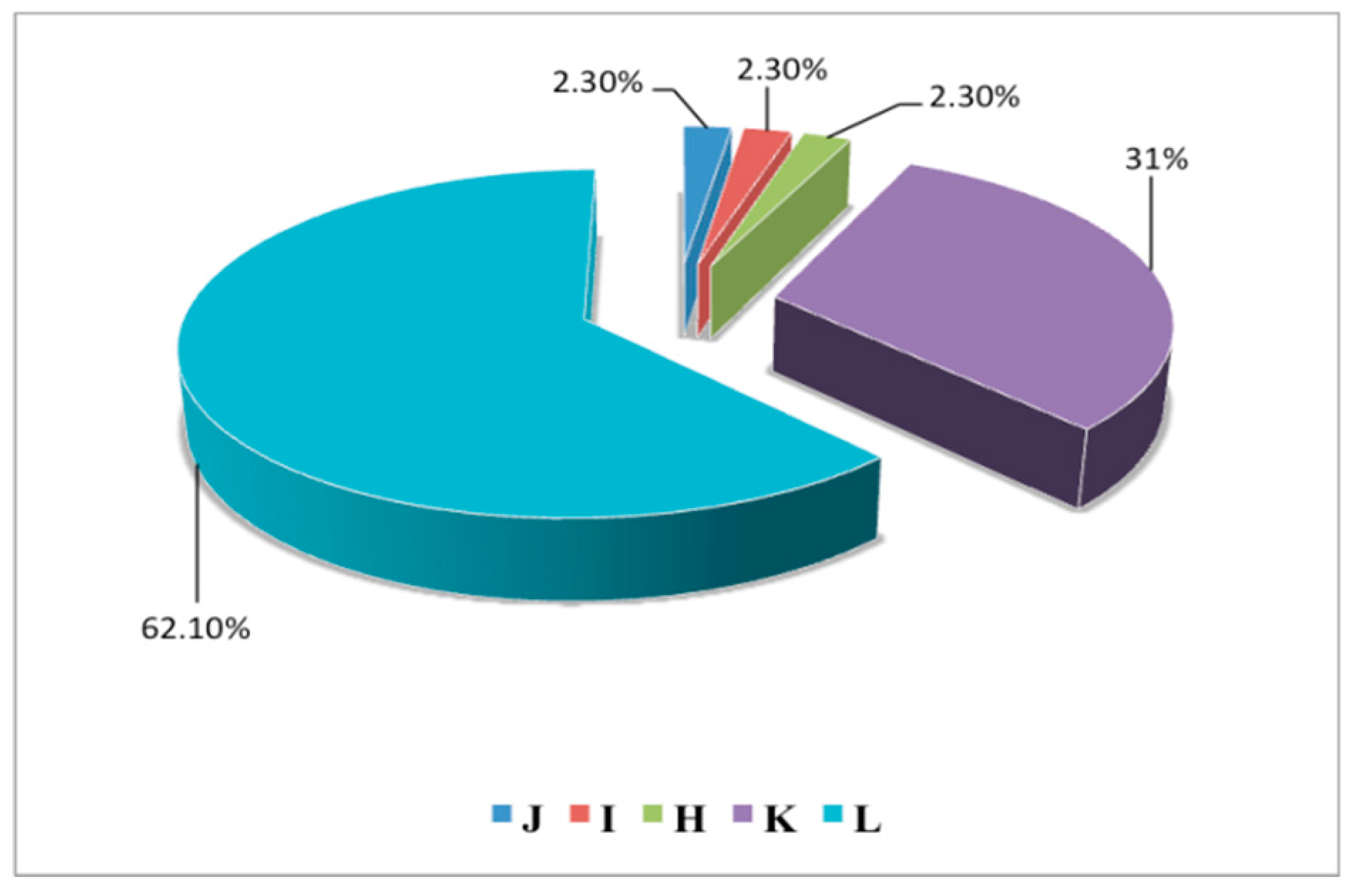
3.1.2. Waste Production Percentages
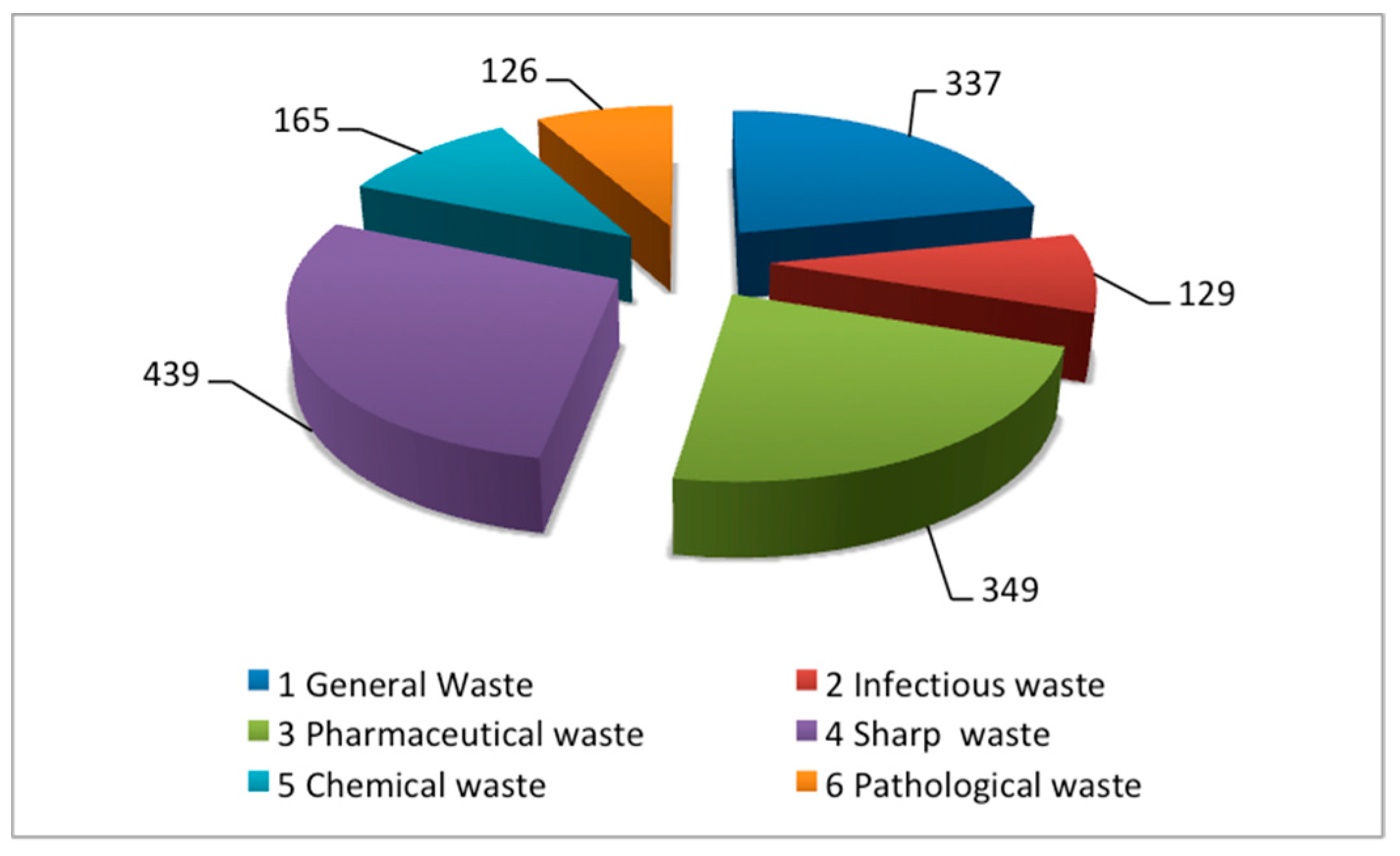
3.1.3. Waste Composition
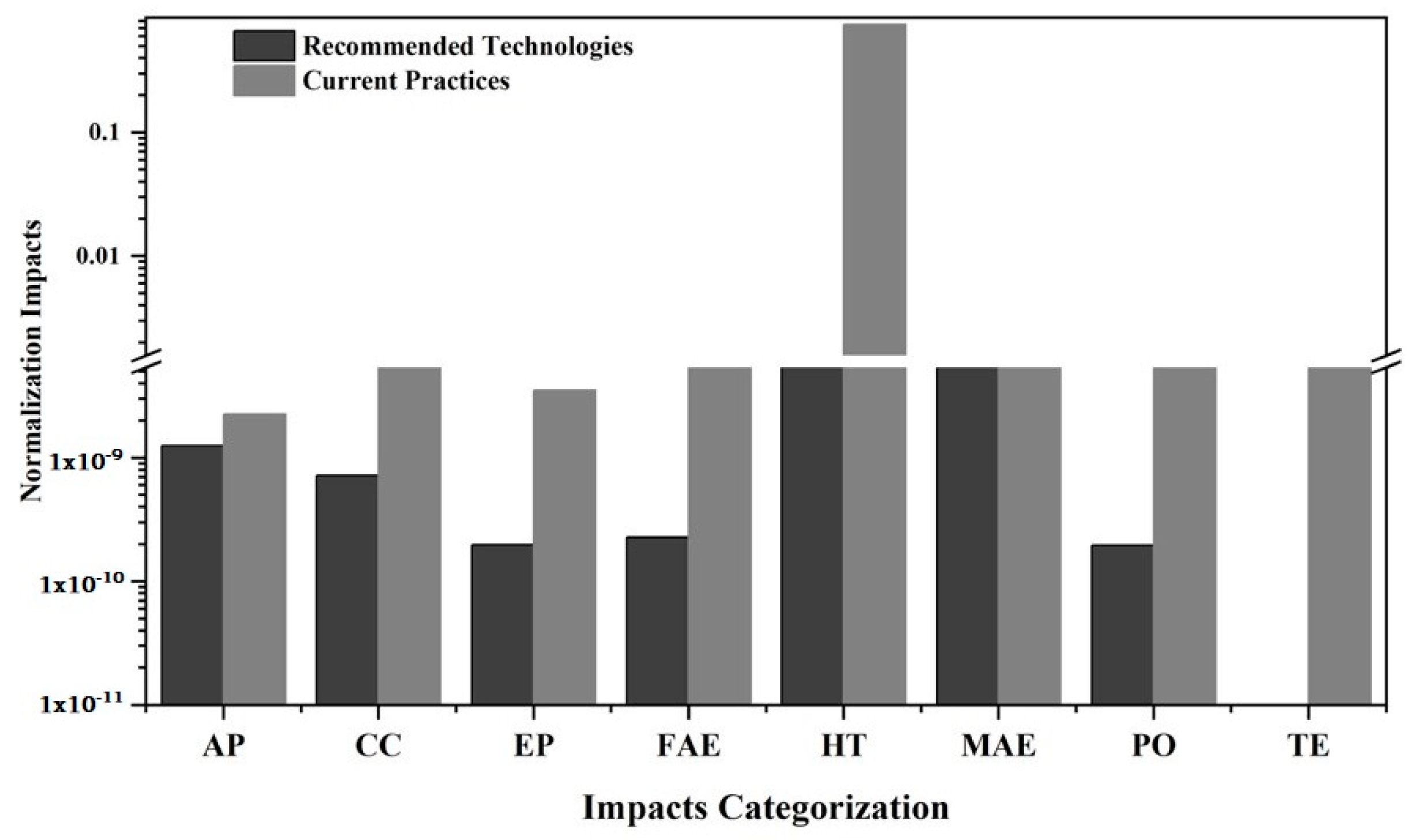
3.2. Life-Cycle Impact Assessment
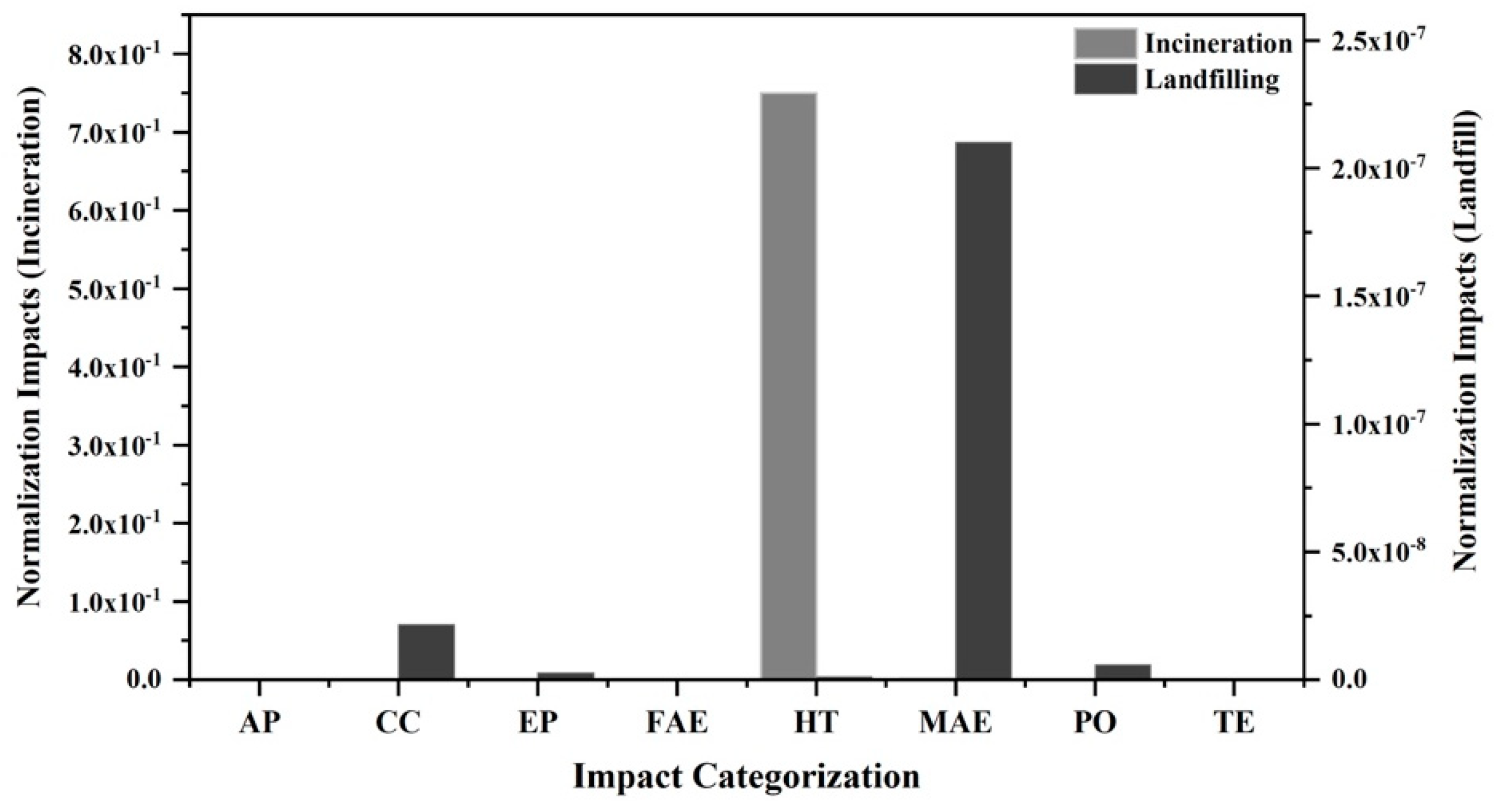
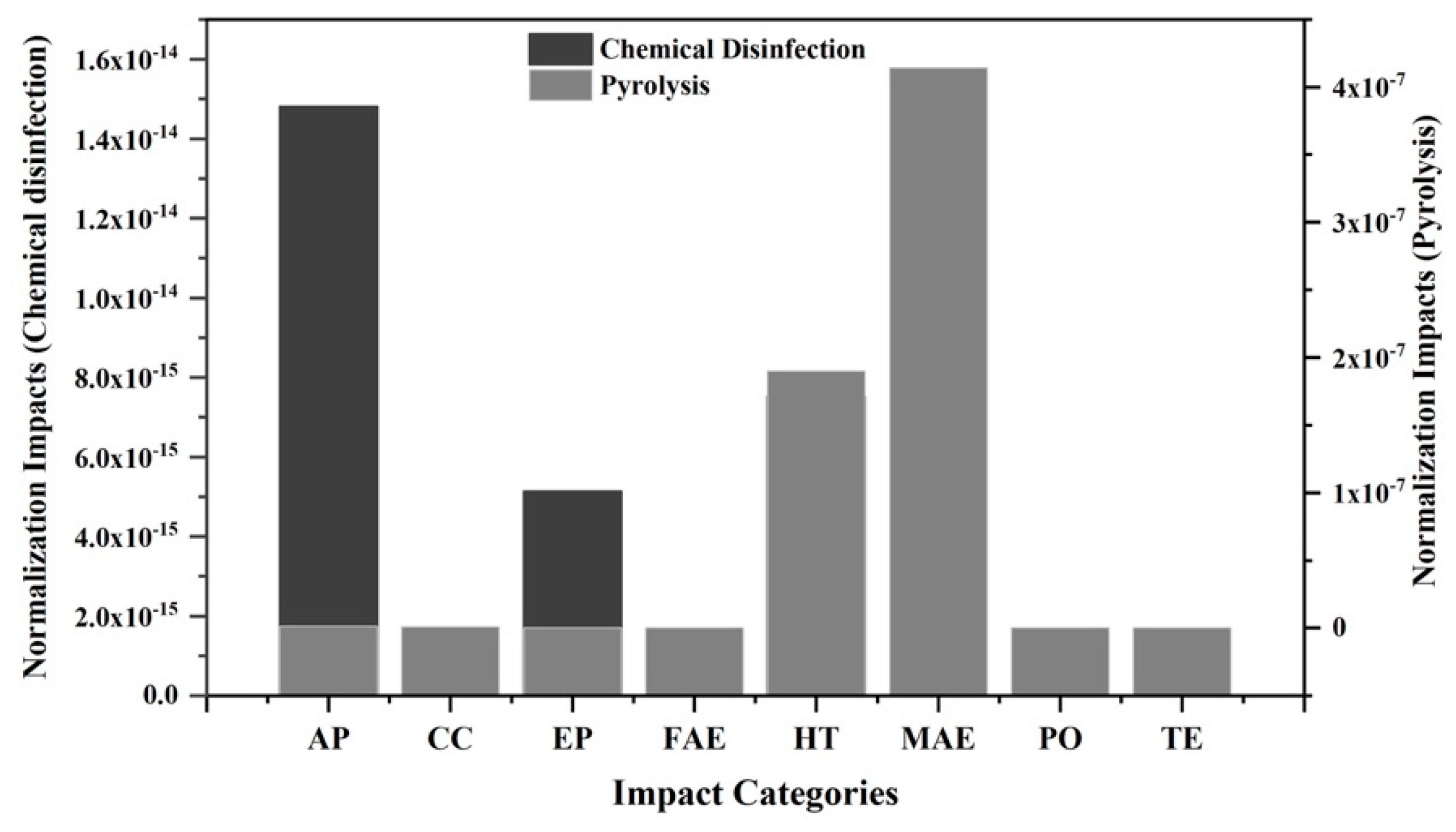
Impact Estimation and Quantification
4. Discussion
4.1. Comparative Analysis of Cumulative Impacts
4.2. Comparison with Previous Literature Results
4.3. Consequences for Hospital Solid Waste (HSW) Treatment Management in Swat District
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Conflicts of Interest
References
- El-Salam, M.M.A. Hospital waste management in El-Beheira Governorate, Egypt. J. Environ. Manag. 2010, 91, 618–629. [Google Scholar] [CrossRef] [PubMed]
- Rushbrook, P. Starting Health Care Waste Management in Medical Institutions. In OMS Health Care Waste Practical Information Series (Volume 1). 2000. Available online: www.searo.who.int/srilanka/documents/safe_management_of_wastes_from_healthcare_activities.pdf?ua=1 (accessed on 22 April 2019).
- Anwar, O.; Malik, N.; Asim, M. Evaluation of Hospital Waste Management in Public and Private Sector Hospitals of Faisalabad City, Pakistan. Acad. J. Interdiscip. Stud. 2013, 2, 161–164. [Google Scholar] [CrossRef]
- Bokhoree, C.; Beeharry, Y.; Makoondlall-Chadee, T.; Doobah, T.; Soomary, N. Assessment of environmental and health risks associated with the management of medical waste in Mauritius. APCBEE Procedia 2014, 9, 36–41. [Google Scholar] [CrossRef]
- Oli, A.N.; Ekejindu, C.C.; Ejiofor, O.S.; Oli, A.H.; Ezeobi, I.; Ibeh, C.C. The knowledge of and attitude to hospital-acquired infections among public and private healthcare workers in south-east Nigeria. Br. J. Med. Med. Res. 2016, 11, 1–13. [Google Scholar] [CrossRef]
- Awodele, O.; Adewoye, A.A.; Oparah, A.C. Assessment of medical waste management in seven hospitals in Lagos, Nigeria. BMC Public Health 2016, 16, 269–273. [Google Scholar] [CrossRef] [PubMed]
- Nemathaga, F.; Maringa, S.; Chimuka, L. Hospital solid waste management practices in Limpopo Province, South Africa: A case study of two hospitals. Waste Manag. 2008, 28, 1236–1245. [Google Scholar] [CrossRef] [PubMed]
- Caniato, M.; Tudor, T.; Vaccari, M. International governance structures for health-care waste management: A systematic review of scientific literature. J. Environ. Manag. 2015, 153, 93–107. [Google Scholar] [CrossRef]
- Tudor, T.L.; Noonan, C.L.; Jenkin, L.E.T. Health care waste management: A case study from the National Health Service in Cornwall, United Kingdom. Waste Manag. 2005, 25, 606–615. [Google Scholar] [CrossRef]
- Shinee, E.; Gombojav, E.; Nishimura, A.; Hamajima, N.; Ito, K. Healthcare waste management in the capital city of Mongolia. Waste Manag. 2008, 28, 435–441. [Google Scholar] [CrossRef]
- Da Silva, C.E.; Hoppe, A.E.; Ravanello, M.M.; Mello, N. Medical wastes management in the south of Brazil. Waste Manag. 2005, 25, 600–605. [Google Scholar] [CrossRef]
- Pant, D. Waste management in small hospitals: Trouble for environment. Env. Monit. Assess. 2011, 1, 1–13. [Google Scholar] [CrossRef] [PubMed]
- Blenkharn, J.I. Standards of clinical waste management in UK hospitals. J. Hosp. Infect. 2006, 62, 300–303. [Google Scholar] [CrossRef] [PubMed]
- Yves Chartier, J.E.; Pieper, U.; Prüss, A.; Rushbrook, P.; Stringer, R.; Townend, W.; Wilburn, S.; Zghondi, R. Safe Management of Wastes from Health Care Activities, 2nd ed.; World Health Organization: Geneva, Switzerland, 2013. [Google Scholar]
- Ozkan, A. Evaluation of healthcare waste treatment/disposal alternatives by using multi-criteria decision-making techniques. Waste Manag. Res. 2013, 31, 141–149. [Google Scholar] [CrossRef] [PubMed]
- Coulter, W.A.; Chew-Graham, C.A.; Cheung, S.W.; Burke, F.J.T. Autoclave performance and operator knowledge of autoclave use in primary care: A survey of UK practices. J. Hosp. Infect. 2001, 48, 180–185. [Google Scholar] [CrossRef] [PubMed]
- Chen, Y.; Liu, L.Y.; Feng, Q.Z.; Chen, G. Key Issues Study on the Operation Management of Medical Waste Incineration Disposal Facilities. In Seventh International Conference on Waste Management and Technology; Jinhui, L., Hualong, H., Eds.; Elsevier Science: Amsterdam, The Netherlands, 2012; pp. 208–213. [Google Scholar]
- Zhao, W.; van der Voet, E.; Huppes, G.; Zhang, Y. Comparative life cycle assessments of incineration and non-incineration treatments for medical waste. Int. J. Life Cycle Assess. 2009, 14, 114–121. [Google Scholar] [CrossRef]
- Unger, S.; Landis, A. Assessing the environmental, human health, and economic impacts of reprocessed medical devices in a Phoenix hospital’s supply chain. J. Clean. Prod. 2016, 112, 1995–2003. [Google Scholar] [CrossRef]
- Dempsey, C.R.; Oppelt, E.T. Incineration of hazardous waste: A critical review update. Air Waste 1993, 43, 25–73. [Google Scholar] [CrossRef]
- Tozlu, A.; Ozahi, E.; Abuşoğlu, A. Waste to energy technologies for municipal solid waste management in Gaziantep. Renew. Sustain. Energy Rev. 2016, 54, 809–815. [Google Scholar] [CrossRef]
- Zhang, Y.F.; Deng, N.; Ling, J.H.; Xu, C.Z. A new pyrolysis technology and equipment for treatment of municipal household garbage and hospital waste. Renew. Energy 2003, 28, 2383–2393. [Google Scholar]
- Lee, C.C. Environmental Engineering Dictionary; Government Institutes Inc.: Rockville, MD, USA, 1988.
- Tudor, T.L.; Townend, W.K.; Cheeseman, C.R.; Edgar, J.E. An overview of arisings and large-scale treatment technologies for healthcare waste in the United Kingdom. Waste Manag. Res. 2009, 27, 374–383. [Google Scholar] [CrossRef] [PubMed]
- Yang, C.; Peijun, L.; Lupi, C.; Yangzhao, S.; Diandou, X.; Qian, F.; Shasha, F. Sustainable management measures for healthcare waste in China. Waste Manag. 2009, 29, 1996–2004. [Google Scholar] [CrossRef] [PubMed]
- Tonuci, L.R.S.; Paschoalatto, C.F.P.R.; Pisani, R., Jr. Microwave inactivation of Escherichia coli in healthcare waste. Waste Manag. 2008, 28, 840–848. [Google Scholar] [CrossRef] [PubMed]
- Avery, L.M.; Prysor Williams, A.; Killham, K.; Jones, D.L. Heat and lime- treatment as effective control methods for E. coli O157:H7 in organic wastes. Bioresour. Technol. 2009, 100, 2692–2698. [Google Scholar] [CrossRef] [PubMed]
- Karagiannidis, A.; Papageorgiou, A.; Perkoulidis, G.; Sanida, G.; Samaras, P. A multi-criteria assessment of scenarios on thermal processing of infectious hospital wastes: A case study for Central Macedonia. Waste Manag. 2010, 30, 251–262. [Google Scholar] [CrossRef] [PubMed]
- Lee, B.K.; Ellenbecker, M.J.; Moure-Eraso, R. Analyses of the recycling potential of medical plastic wastes. Waste Manag. 2002, 22, 461–470. [Google Scholar] [CrossRef]
- Hong, J.; Zhan, S.; Yu, Z.; Hong, J.; Qi, C. Life-cycle environmental and economic assessment of medical waste treatment. J. Clean. Prod. 2018, 174, 65–73. [Google Scholar] [CrossRef]
- Eriksson, O.; Carlsson, R.M.; Frostell, B.; Björklund, A.; Assefa, G.; Sundqvist, J.O.; Granath, J.; Baky, A.; Thyselius, L. Municipal solid waste management from a system perspective. J. Clean Prod. 2005, 13, 241–252. [Google Scholar] [CrossRef]
- Ali, M.; Wang, W.; Chaudhry, N. Application of life cycle assessment for hospital solid waste management: A case study. J. Air Waste Manag. Assoc. 2016, 66, 1012–1018. [Google Scholar] [CrossRef] [Green Version]
- Merrild, H.; Damgaard, A.; Christensen, T.H. Recycling of paper: Accounting of greenhouse gases and global warming contributions. Waste Manag. Res. 2009, 27, 746–753. [Google Scholar] [CrossRef]
- Kumar, R.; Shaikh, B.T.; Somrongthong, R.; Chapman, R.S. Practices and challenges of infectious waste management: A qualitative descriptive study from tertiary care hospitals in Pakistan. Pak. J. Med. Sci. 2015, 31, 795–798. [Google Scholar] [CrossRef]
- Longe, E.O.; Williams, A. A preliminary study of medical waste management in Lagos metropolis, Nigeria. J. Environ. Health Sci. Eng. 2006, 3, 133–139. [Google Scholar]
- Huffman, G.L. Medical waste management/incineration. J. Hazard. Mater. 1996, 1, 1–30. [Google Scholar]
- Rao, M.N.; Sultana, R.; Kota, S.H.; Shah, A.; Davergave, N. Solid and Hazardous Waste Management: Science and Engineering; Butterworth-Heinemann: Oxford, UK, 2016. [Google Scholar]
- Rabl, A.; Spadaro, J.V.; Zoughaib, A. Environmental impacts and costs of solid waste: A comparison of landfill and incineration. Waste Manag. Res. 2008, 26, 147–162. [Google Scholar] [CrossRef] [PubMed]
- Mendes, M.R.; Aramaki, T.; Hanaki, K. Comparison of the environmental impact of incineration and landfilling in São Paulo City as determined by LCA. Resour. Conserv. Recycl. 2004, 41, 47–63. [Google Scholar] [CrossRef]
- Assamoi, B.; Lawryshyn, Y. The environmental comparison of landfilling vs. incineration of MSW accounting for waste diversion. Waste Manag. 2012, 32, 1019–1030. [Google Scholar] [CrossRef] [PubMed]
- Environment Canada. National Inventory Report 1990–2007: Greenhouse Gas Sources and Sinks in Canada; Canadian Environmental Assessment Agency: Ottawa, ON, Canada, 2009. [Google Scholar]
- Hickman, H.L. Principles of Integrated Municipal Solid Waste Management; American Academy of Environmental Engineers: New York, NY, USA, 1999. [Google Scholar]
- Sabbas, T.; Polettini, A.; Pomi, R.; Astrup, T.; Hjelmar, O.; Mostbauer, P.; Lechner, P. Management of municipal solid waste incineration residues. Waste Manag. 2003, 23, 61–88. [Google Scholar] [CrossRef]
- Quina, M.J.; Bordado, J.C.M.; Quinta-Ferreira, R.M. Chemical stabilization of air pollution control residues from municipal solid waste incineration. J. Hazard. Waste Mater. 2010, 179, 382–392. [Google Scholar] [CrossRef]
- Nielsen, P.H.; Hauschild, M. Product specific emissions from municipal solid waste landfills. Int. J. Life Cycle Assess. 1998, 3, 158–168. [Google Scholar] [CrossRef]
- Dalemo, M.; Sonesson, U.; Björklund, A.; Mingarini, K.; Frostell, B.; Jönsson, H.; Nybrant, T.; Sundqvist, J.O.; Thyselius, L. ORWARE—A simulation model for organic waste handling systems. Part 1: Model description. Resour. Conserv. Recycl. 1997, 21, 17–37. [Google Scholar] [CrossRef]
- Jones-Lee, A.; Lee, G.F. Appropriate Use of MSW Leachate Recycling in Municipal Solid Waste Landfilling. 2000. Available online: http://www.gfredlee.com/leachatepapsli.pdf (accessed on 16 June 2019).
- Doka, G. Life Cycle Inventories of Waste Treatment Services; Ecoinvent report No. 13; Swiss Centre for Life Cycle Inventories: Dübendorf, Switzerland, 2003. [Google Scholar]
- Program for Appropriate Technology in Health (PATH). Treatment Alternatives for Medical Waste Disposal; Program for Appropriate Technology in Health: Seattle, WA, USA, 2005. [Google Scholar]
- Li, A.M.; Li, X.D.; Li, S.Q.; Ren, Y.; Shang, N.; Chi, Y.; Yan, J.H.; Cen, K.F. Experimental studies on municipal solid waste pyrolysis in a laboratory-scale rotary kiln. Energy 1999, 24, 209–218. [Google Scholar] [CrossRef]
- Kaye, G.I.; Weber, P.B.; Evans, A.; Venezia, R.A. Efficacy of alkaline hydrolysis as an alternative method for treatment and disposal of infectious animal waste. J. Am. Assoc. Lab. Anim. Sci. 1998, 37, 43–46. [Google Scholar]
- Graikos, A.; Voudrias, E.; Papazachariou, A.; Iosifidis, N.; Kalpakidou, M. Composition and production rate of medical waste from a small producer in Greece. Waste Manag. 2010, 30, 1683–1689. [Google Scholar] [CrossRef] [PubMed]
- Health Care without Harm Europe. Non-Incineration Medical Waste Treatment Technologies in Europe; Health Care without Harm Europe: Prague, Czech Republic, 2003. [Google Scholar]
- Arena, U.; Mastellone, M.L.; Perugini, F. The environmental performance of alternative solid waste management options: A life cycle assessment study. Chem. Eng. J. 2003, 96, 207–222. [Google Scholar] [CrossRef]
- Obersteiner, G.; Binner, E.; Mosterbauer, P.; Salhofer, S. Landfilling modelling in LCA—A contribution based on empirical data. Waste Manag. 2007, 27, 58–74. [Google Scholar] [CrossRef] [PubMed]
- Cleary, J. Life cycle assessments of municipal solid waste management systems: A comparative analysis of selected peer-reviewed literature. Environ. Int. 2009, 35, 1256–1266. [Google Scholar] [CrossRef] [PubMed]
- Beylot, A.; Villeneuve, J. Environmental impacts of residual Municipal Solid Waste incineration: A comparison of 110 French incinerators using a life cycle approach. Waste Manag. 2013, 33, 2781–2788. [Google Scholar] [CrossRef] [PubMed]
- Habib, K.; Schmidt, J.H.; Christensen, P. A historical perspective of global warming potential from municipal solid waste management. Waste Manag. 2013, 33, 1926–1933. [Google Scholar] [CrossRef]
- Zhao, W.; Huppes, G.; Voet, E.V.D. Eco-efficiency for greenhouse gas emissions mitigation of municipal solid waste management: A case study of Tianjin. China. Waste Manag. 2011, 31, 1407–1415. [Google Scholar] [CrossRef]
- De Feo, G.; Malvano, C. The use of LCA in selecting the best MSW management system. Waste Manag. 2009, 29, 1901–1915. [Google Scholar] [CrossRef]
- Wittmaier, M.; Langer, S.; Sawilla, B. Possibilities and limitations of life cycle assessment (LCA) in the development of waste utilization systems—Applied examples for a region in Northern Germany. Waste Manag. 2009, 29, 1732–1738. [Google Scholar] [CrossRef]
- Campion, N.; Thiel, C.L.; DeBlois, J.; Woods, N.C.; Landis, A.E.; Bilec, M.M. Life cycle assessment perspectives on delivering an infant in the US. Sci. Total Environ. 2012, 425, 191–198. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Eckelman, M.J.; Mauter, M.S.; Isaacs, J.A.; Elimelech, M. New perspectives on nanomaterial aquatic ecotoxicity: Production impacts exceed direct exposure impacts for carbon nanotubes. Environ. Sci. Technol. 2012, 46, 2902–2910. [Google Scholar] [CrossRef] [PubMed]
- Sørensen, B.L.; Wenzel, H. Life cycle assessment of alternative bedpans—A case of comparing disposable and reusable devices. J. Clean. Prod. 2014, 83, 70–79. [Google Scholar] [CrossRef]
- Thiel, C.L.; Eckelman, M.; Guido, R.; Huddleston, M.; Landis, A.E.; Sherman, J.; Shrake, S.O.; Copley-Woods, N.; Bilec, M.M. Environmental impacts of surgical procedures: Life cycle assessment of hysterectomy in the United States. Environ. Sci. Technol. 2015, 49, 1779–1786. [Google Scholar] [CrossRef] [PubMed]
- Rebitzer, G.; Ekvall, T.; Frischknecht, R.; Hunkeler, D.; Norris, G.; Rydberg, T.; Schmidt, W.P.; Suh, S.; Weidema, B.P.; Pennington, D.W. Life cycle assessment: Part 1: Framework, goal and scope definition, inventory analysis, and applications. Environ. Int. 2004, 30, 701–720. [Google Scholar] [CrossRef] [PubMed]
- Soares, S.R.; Finotti, A.R.; da Silva, V.P.; Alvarenga, R.A. Applications of life cycle assessment and cost analysis in health care waste management. Waste Manag. 2013, 33, 175–183. [Google Scholar] [CrossRef] [PubMed]
- Hong, J.; Hong, J.; Otaki, M.; Jolliet, O. Environmental and economic life cycle assessment for sewage sludge treatment processes in Japan. Waste Manag. 2009, 29, 696–703. [Google Scholar] [CrossRef]
- Dong, J.; Tang, Y.; Nzihou, A.; Chi, Y.; Weiss-Hortala, E.; Ni, M. Life cycle assessment of pyrolysis, gasification and incineration waste-to-energy technologies: Theoretical analysis and case study of commercial plants. Sci. Total Environ. 2018, 626, 744–753. [Google Scholar] [CrossRef]
- Hong, J.; Han, X.; Chen, Y.; Ye, L.; Qi, C.; Li, X. Life cycle environmental assessment of industrial hazardous waste incineration and landfilling in China. Int. J. Life Cycle Assess. 2017, 22, 1054–1064. [Google Scholar] [CrossRef]
- Al-Khatib, I.A.; Sato, C. Solid health care waste management status at health care centers in the West Bank–Palestinian Territory. Waste Manag. 2009, 29, 2398–2403. [Google Scholar] [CrossRef]
- Jang, Y.C.; Lee, C.; Yoon, O.S.; Kim, H. Medical waste management in Korea. J. Environ. Manag. 2006, 80, 107–115. [Google Scholar] [CrossRef] [PubMed]
- Lee, B.K.; Ellenbecker, M.J.; Rafael, M.E. Alternatives for treatment and disposal cost reduction of regulated medical wastes. Waste Manag. 2004, 24, 143–151. [Google Scholar] [CrossRef] [PubMed]
- Prüss-Üstün, A. Safe Management of Wastes from Health-Care Activities; World Health Organization: Geneva, Switzerland, 1999. [Google Scholar]
- Environmenatal Protection Agency USA (EPA). Guidelines for Ecological Risk Assessment; Federal Register 63; USA Environmental Protection Agency: Washington, DC, USA, 1998; pp. 26846–26924.
- Marrack, D.; Meyers, D. PP/PE Medical Syringe Recycling System: Sharps Away. In Proceedings of the 87th Annual Meeting and Exhibition, Air & Waste Management Association, Paper No. 94-RP-123B.01, Cincinnati, OH, USA, 19–24 June 1994. [Google Scholar]
- Lee, B.K.; Ellenbecker, M.J. A Study of Disposal and Recycling of Hospital and Medical Wastes. In Center for Environmentally Appropriate Materials (CEAM) Final Report; University of Massachusetts: Massachusetts, MA, USA, 1995. [Google Scholar]
- EU Commission. Taking Sustainable Use of Resources Forward: A Thematic Strategy on the Prevention and Recycling of Waste; Communication from the Commission of the European Communities: Brussels, Belgium, 2005; p. 666. [Google Scholar]
- Lazarevic, D.; Aoustin, E.; Buclet, N.; Brandt, N. Plastic waste management in the context of a European recycling society: Comparing results and uncertainties in a life cycle perspective. Resour. Conserv. Recycl. 2010, 55, 246–259. [Google Scholar] [CrossRef]
- DEFRA UK. Review of Environmental and Health Effects of Waste Management: Municipal Solid Waste and Similar Wastes; Defra Publications: London, UK, 2004. [Google Scholar]
- Jaffery, S. Medical Waste Illegally Sold Off from Pakistan Hospital. 2013. Available online: www.bbc.com/news/world-asia-22130292 (accessed on 22 November 2018).










{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Waste Category | Treatment | Disposal |
|---|---|---|
| General | - | Municipal landfill/recycling |
| Infectious | Incineration | Deep burial |
| Pharmaceutical | - | Secured landfill |
| Sharp | Disinfection | Recycling |
| Chemical | - | Secured landfill |
| Pathological | Incineration | Deep burial |
| Incineration ashes | No treatment | Secured landfill |
| Scenario A (Currently Applied) | Scenario B (Currently Applied) | Scenario C (Alternative) |
|---|---|---|
| Incineration and landfilling | Landfilling | Incineration (pyrolysis), disinfection and landfilling |
| Impact Category | Process | |||
|---|---|---|---|---|
| Incineration | Landfilling | Pyrolysis | Chemical Disinfection | |
| AP | 2.16 × 10−9 | 8.58 × 10−11 | 1.26 × 10−9 | 1.48 × 10−14 |
| CC | 2.06 × 10−8 | 2.15 × 10−8 | 7.17 × 10−10 | 0 |
| EP | 8.46 × 10−10 | 2.69 × 10−9 | 1.97 × 10−10 | 5.13 × 10−15 |
| FAE | 9.00 × 104 | 1.96 × 10−12 | 2.29 × 10−10 | 0 |
| HT | 7.50 × 10−1 | 1.13 × 10−9 | 1.90 × 10−7 | 7.52 × 10−15 |
| MAE | 1.53 × 103 | 2.10 × 10−7 | 4.14 × 10−7 | 0 |
| PO | 7.83 × 10−10 | 5.84 × 10−9 | 1.96 × 10−10 | 0 |
| TE | 1.10 × 10−5 | 2.70 × 10−15 | 2.75 × 10−12 | 0 |
| Category | Value | Process |
|---|---|---|
| HT | 7.50 × 10−1 | Incineration |
| MAE | 1.53 × 10−3 | Incineration |
| FAE | 9.00 × 10−4 | Incineration |
| TE | 1.10 × 10−5 | Incineration |
| MAE | 4.14 × 10−7 | Pyrolysis |
| MAE | 2.10 × 10−7 | Landfilling |
| HT | 1.90 × 10−7 | Pyrolysis |
| CC | 2.15 × 10−8 | Landfilling |
| CC | 2.06 × 10−8 | Incineration |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Ahmad, R.; Liu, G.; Santagata, R.; Casazza, M.; Xue, J.; Khan, K.; Nawab, J.; Ulgiati, S.; Lega, M. LCA of Hospital Solid Waste Treatment Alternatives in a Developing Country: The Case of District Swat, Pakistan. Sustainability 2019, 11, 3501. https://doi.org/10.3390/su11133501
Ahmad R, Liu G, Santagata R, Casazza M, Xue J, Khan K, Nawab J, Ulgiati S, Lega M. LCA of Hospital Solid Waste Treatment Alternatives in a Developing Country: The Case of District Swat, Pakistan. Sustainability. 2019; 11(13):3501. https://doi.org/10.3390/su11133501
Chicago/Turabian StyleAhmad, Riaz, Gengyuan Liu, Remo Santagata, Marco Casazza, Jingyan Xue, Kifayatullah Khan, Javed Nawab, Sergio Ulgiati, and Massimiliano Lega. 2019. "LCA of Hospital Solid Waste Treatment Alternatives in a Developing Country: The Case of District Swat, Pakistan" Sustainability 11, no. 13: 3501. https://doi.org/10.3390/su11133501