
Influence of Semiquantitative [18F]FDG PET and Hematological Parameters on Survival in HNSCC Patients Using Neural Network Analysis

 , , , , ,
, , , , ,
Abstract
:1. Introduction
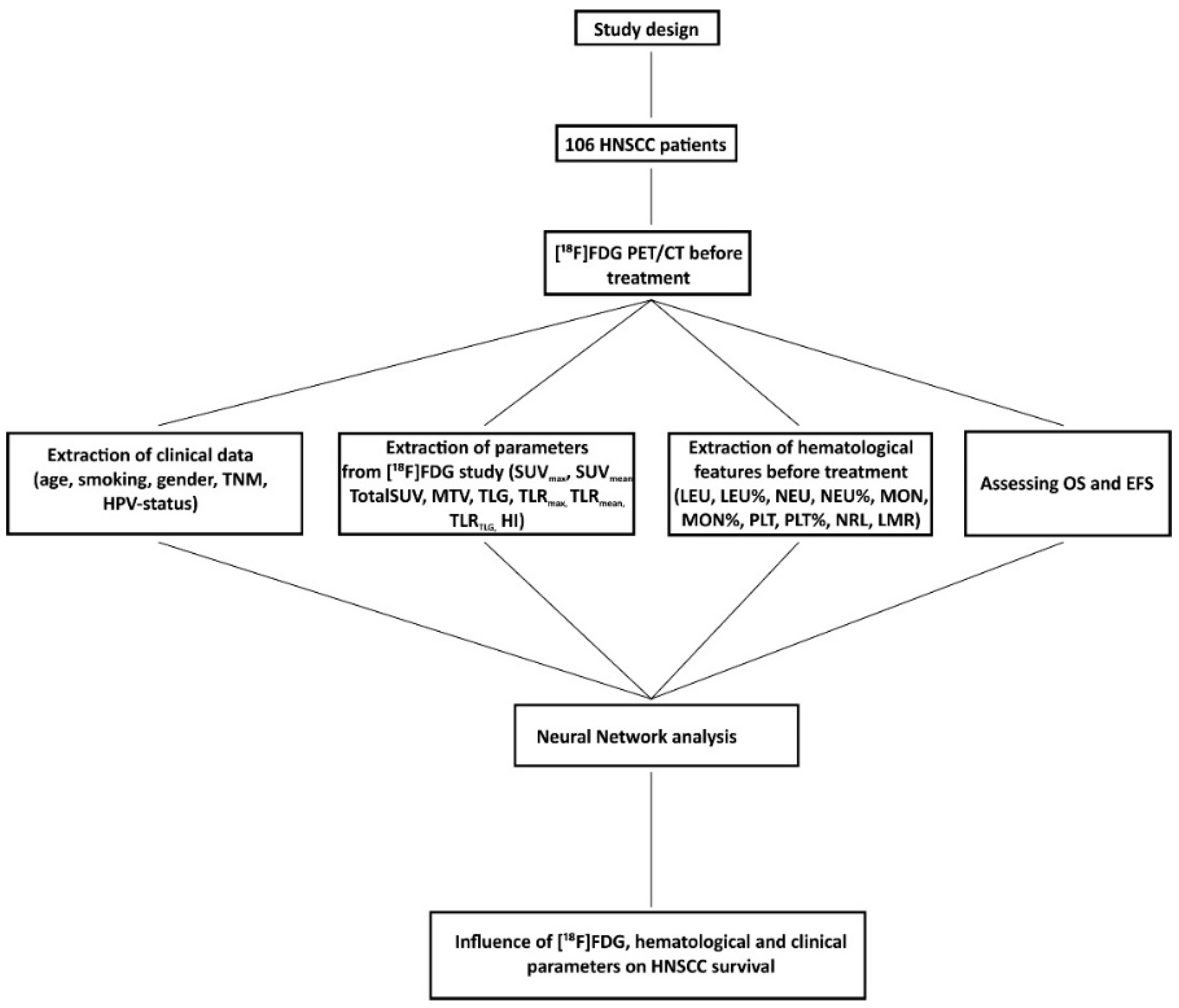
2. Materials and Methods
2.1. Patient Characteristics
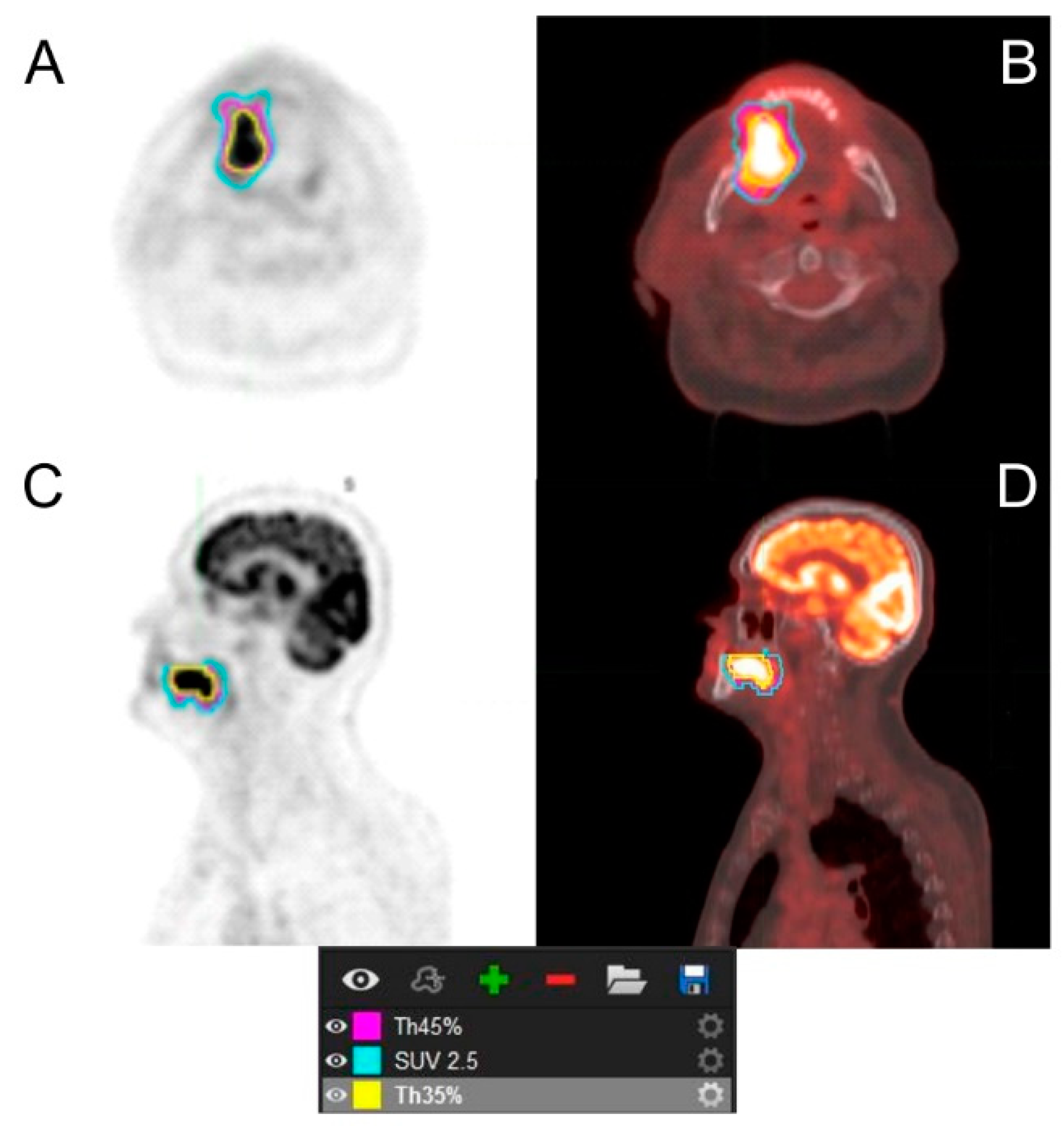
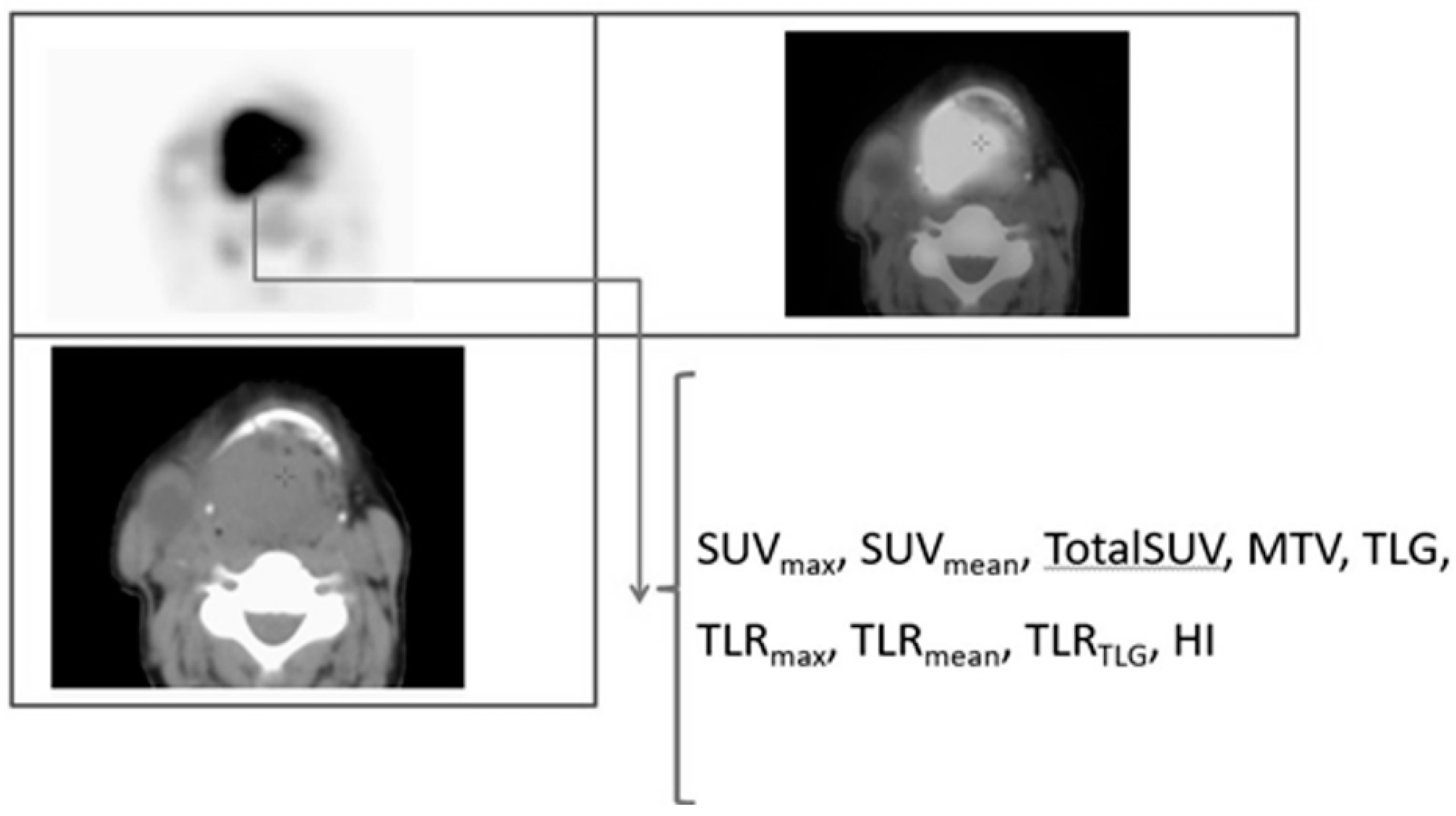
2.2. [18F]FDG PET/CT Analysis
2.3. Hematological Parameters Analysis
2.4. Neural Network Analysis
3. Results
3.1. Differences in [18F]FDG Parameters
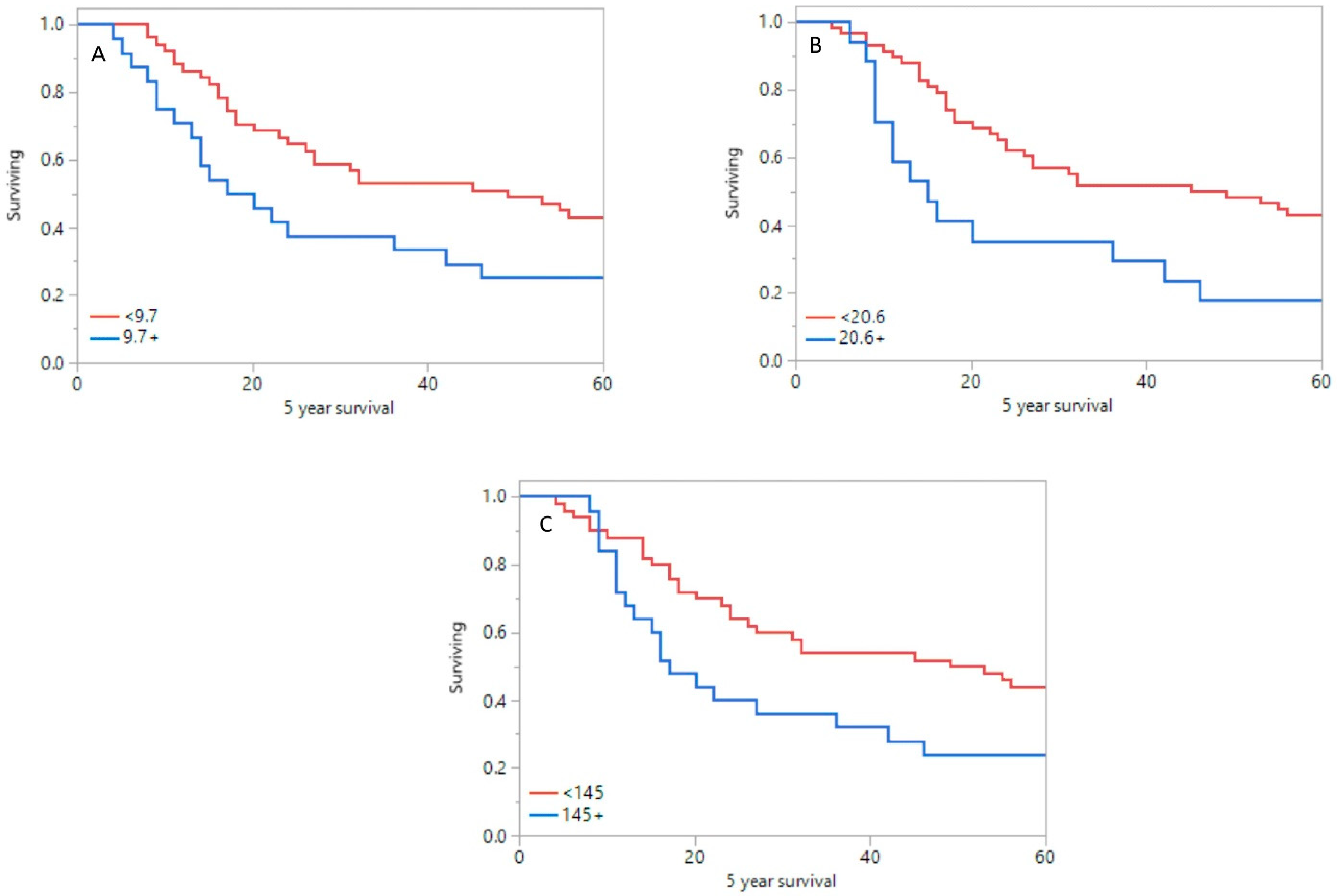
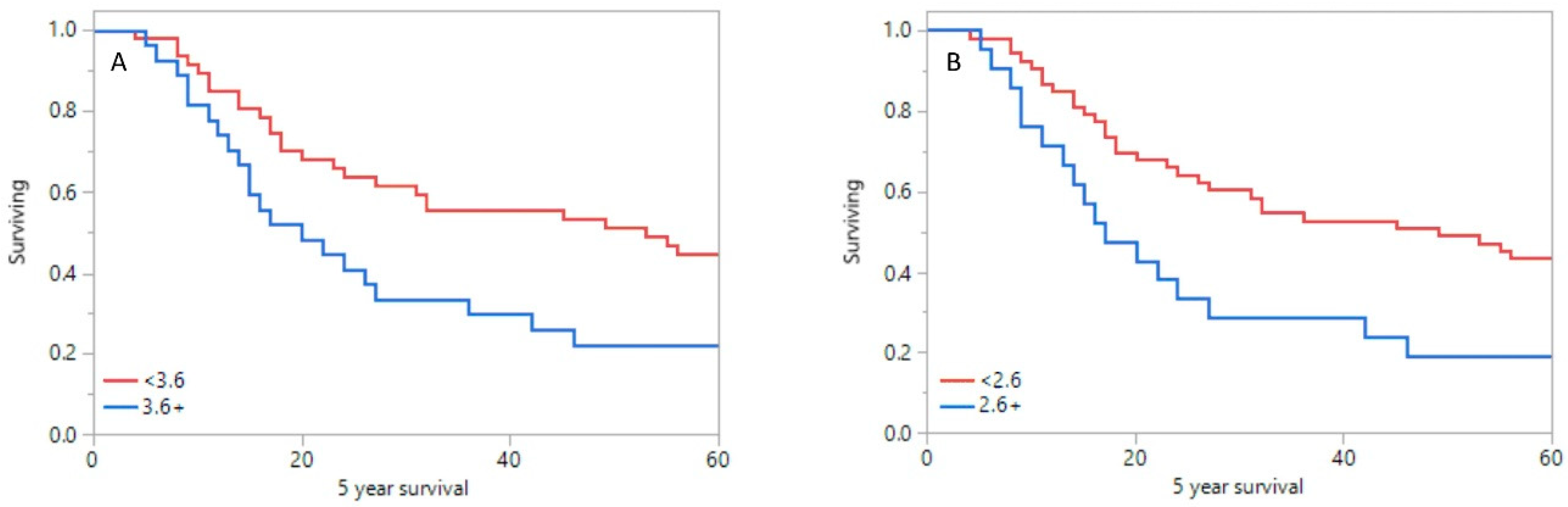
3.2. Overall Survival Analysis
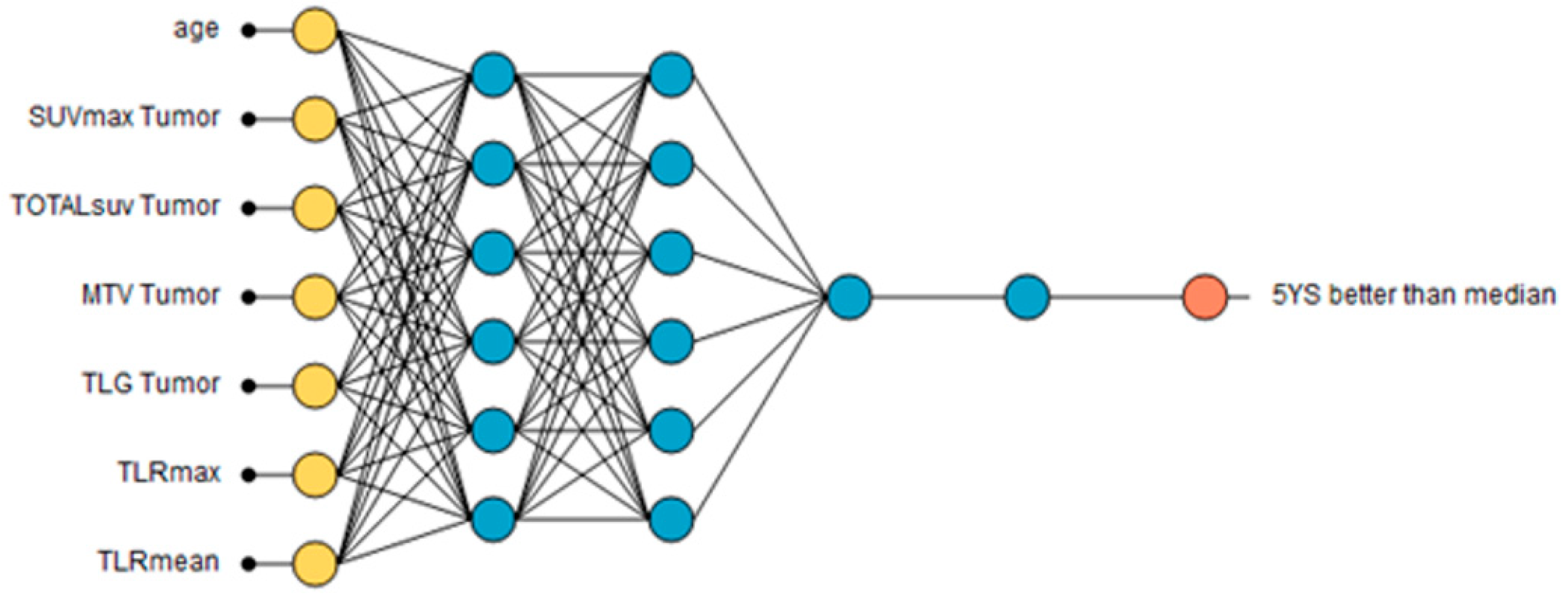
3.3. Neural Network Analysis
- Age 60+ years;
- SUVmax tumor over 9.7;
- TotalSUV tumor over 2255;
- MTV tumor over 20.6;
- TLG tumor over 145;
- TLRmax over 3.6;
- TLRmean over 2.6.
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Bray, F.; Ferlay, J.; Soerjomataram, I.; Siegel, R.L.; Torre, L.A.; Jemal, A. Global cancer statistics 2018: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries. CA Cancer J. Clin. 2018, 68, 394–424. [Google Scholar] [CrossRef] [Green Version]
- Johnson, D.E.; Burtness, B.; Leemans, C.R.; Lui, V.W.Y.; Bauman, J.E.; Grandis, J.R. Head and neck squamous cell carcinoma. Nat. Rev. Dis. Primers 2020, 6, 92. [Google Scholar] [CrossRef] [PubMed]
- Machczyński, P.; Majchrzak, E.; Niewinski, P.; Marchlewska, J.; Golusiński, W. A review of the 8th edition of the AJCC staging system for oropharyngeal cancer according to HPV status. Eur. Arch. Otorhinolaryngol. 2020, 277, 2407–2412. [Google Scholar] [CrossRef] [PubMed]
- Leclere, J.-C.; Delcroix, O.; Rousset, J.; Valette, G.; Robin, P.; Guezennec, C.; Le Pennec, R.; Gujral, D.M.; Abgral, M.; Ollivier, L.; et al. Integration of 18-FDG PET/CT in the Initial Work-Up to Stage Head and Neck Cancer: Prognostic Significance and Impact on Therapeutic Decision Making. Front. Med. 2020, 7, 273. [Google Scholar] [CrossRef] [PubMed]
- Cheng, G.; Huang, H. Prognostic Value of (18F)-Fluorodeoxyglucose PET/Computed Tomography in Non–Small-Cell Lung Cancer. PET Clin. 2018, 13, 59–72. [Google Scholar] [CrossRef]
- Paidpally, V.; Chirindel, A.; Chung, C.H.; Richmon, J.; Koch, W.; Quon, H.; Subramaniam, R.M. FDG volumetric parameters and survival outcomes after definitive chemoradio-therapy in patients with recurrent head and neck squamous cell carcinoma. AJR Am. J. Roentgenol. 2014, 203, W139–W145. [Google Scholar] [CrossRef] [Green Version]
- Huang, J.; Huang, L.; Zhou, J.; Duan, Y.; Zhang, Z.; Wang, X.; Huang, P.; Tan, S.; Yinghua, D.; Wang, J.; et al. Elevated tumor-to-liver uptake ratio (TLR) from 18F–FDG-PET/CT predicts poor prognosis in stage IIA colorectal cancer following curative resection. Eur. J. Nucl. Med. Mol. Imaging 2017, 44, 1958–1968. [Google Scholar] [CrossRef] [Green Version]
- Li, M.-X.; Liu, X.-M.; Zhang, X.-F.; Zhang, J.-F.; Wang, W.-L.; Zhu, Y.; Dong, J.; Cheng, J.-W.; Liu, Z.-W.; Ma, L.; et al. Prognostic role of neutrophil-to-lymphocyte ratio in colorectal cancer: A systematic review and meta-analysis. Int. J. Cancer 2013, 134, 2403–2413. [Google Scholar] [CrossRef]
- Chen, J.; Deng, Q.; Pan, Y.; He, B.; Ying, H.; Sun, H.; Liu, X.; Wang, S. Prognostic value of neutrophil-to-lymphocyte ratio in breast cancer. FEBS Open Bio 2015, 5, 502–507. [Google Scholar] [CrossRef] [Green Version]
- Ozyurek, B.A.; Ozdemirel, T.S.; Ozden, S.B.; Erdogan, Y.; Kaplan, B.; Kaplan, T. Prognostic value of the neutrophil to lymphocyte ratio (NLR) in lung cancer cases. Asian Pac. J. Cancer Prev. 2017, 18, 1417–1421. [Google Scholar]
- Cao, J.; Zhu, X.; Zhao, X.; Zhao, X.; Li, X.F.; Xu, R. Neutrophil-to-lymphocyte ratio predicts PSA response and prognosis in prostate cancer: A systematic review and meta-analysis. PLoS ONE 2016, 11, e015877. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Xiang, J.; Zhou, L.; Li, X.; Bao, W.; Chen, T.; Xi, X.; He, Y.; Wan, X. Preoperative Monocyte-to-Lymphocyte Ratio in Peripheral Blood Predicts Stages, Metastasis, and Histological Grades in Patients with Ovarian Cancer. Transl. Oncol. 2016, 10, 33–39. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mascarella, M.A.; Mannard, E.; Silva, S.D.; Zeitouni, A. Neutrophil-to-lymphocyte ratio in head and neck cancer prognosis: A systematic review and meta-analysis. Head Neck 2018, 40, 1091–1100. [Google Scholar] [CrossRef]
- Lu, A.; Li, H.; Zheng, Y.; Tang, M.; Li, J.; Wu, H.; Zhong, W.; Gao, J.; Ou, N.; Cai, Y. Prognostic Significance of Neutrophil to Lymphocyte Ratio, Lymphocyte to Monocyte Ratio, and Platelet to Lymphocyte Ratio in Patients with Nasopharyngeal Carcinoma. BioMed Res. Int. 2017, 2017, 3047802. [Google Scholar] [CrossRef]
- Li, W.; Liu, H.; Cheng, F.; Li, Y.; Li, S.; Yan, J. Artificial intelligence applications for oncological positron emission tomography imaging. Eur. J. Radiol. 2020, 134, 109448. [Google Scholar] [CrossRef]
- Haider, S.P.; Burtness, B.; Yarbrough, W.G.; Payabvash, S. Applications of radiomics in precision diagnosis, prognostication and treatment planning of head and neck squamous cell carcinomas. Cancers Head Neck 2021, 5, 6. [Google Scholar] [CrossRef]
- Moe, Y.M.; Groendahl, A.R.; Tomic, O.; Dale, E.; Malinen, E.; Futsaether, C.M. Deep learning-based auto-delineation of gross tumour volumes and involved nodes in PET/CT images of head and neck cancer patients. Eur. J. Nucl. Med. Mol. Imaging 2021, 48, 2782–2792. [Google Scholar] [CrossRef]
- Boellaard, R.; Delgado-Bolton, R.; Oyen, W.J.G.; Giammarile, F.; Tatsch, K.; Eschner, W.; Verzijlbergen, F.J.; Barrington, S.F.; Pike, L.C.; Weber, W.A.; et al. FDG PET/CT: EANM procedure guidelines for tumour imaging: Version 2.0. Eur. J. Nucl. Med. Mol. Imaging 2015, 42, 328–354. [Google Scholar] [CrossRef]
- Cegła, P.; Burchardt, E.; Wierzchosławska, E.; Roszak, A.; Cholewiński, W. The effect of different segmentation methods on primary tumour metabolic volume assessed in 18F-FDG-PET/CT in patients with cervical cancer, for radiotherapy planning. Contemp. Oncol. 2019, 23, 183–186. [Google Scholar] [CrossRef]
- Yang, Z.; Shi, Q.; Zhang, Y.; Pan, H.; Yao, Z.; Hu, S.; Shi, W.; Zhu, B.; Zhang, Y.; Hu, C.; et al. Pretreatment (18)F-FDG uptake heterogeneity can predict survival in patients with locally ad-vanced nasopharyngeal carcinoma—A retrospective study. Radiat. Oncol. 2015, 10, 4. [Google Scholar] [CrossRef] [Green Version]
- Currie, G.M. Intelligent Imaging: Developing a Machine Learning Project. J. Nucl. Med. Technol. 2021, 49, 44–48. [Google Scholar] [CrossRef] [PubMed]
- Currie, G.; Hawk, K.E.; Rohren, E.; Vial, A.; Klein, R. Machine Learning and Deep Learning in Medical Imaging: Intelligent Imaging. J. Med. Imaging Radiat. Sci. 2019, 50, 477–487. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Currie, G.M. Intelligent Imaging: Anatomy of Machine Learning and Deep Learning. J. Nucl. Med. Technol. 2019, 47, 273–281. [Google Scholar] [CrossRef] [PubMed]
- Rohde, M.; Nielsen, A.L.; Pareek, M.; Johansen, J.; Sørensen, J.A.; Diaz, A.; Nielsen, M.K.; Christiansen, J.M.; Asmussen, J.T.; Nguyen, N.; et al. PET/CT Versus Standard Imaging for Prediction of Survival in Patients with Recurrent Head and Neck Squamous Cell Carcinoma. J. Nucl. Med. 2019, 60, 592–599. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Halfpenny, W.; Hain, S.F.; Biassoni, L.; Maisey, M.N.; A Sherman, J.; McGurk, M. FDG–PET. A possible prognostic factor in head and neck cancer. Br. J. Cancer 2002, 86, 512–516. [Google Scholar] [CrossRef]
- Allal, A.S.; Dulguerov, P.; Allaoua, M.G.; Haenggeli, C.A.; El-Ghazi, E.A.; Lehmann, W.; Slosman, D.O. Standardized uptake value of 2-[18F]fluoro-2-deoxy-D-glucose in predicting out-come in head and neck carcinomas treated by radiotherapy with or without chemotherapy. J. Clin. Oncol. 2002, 20, 1398-404. [Google Scholar] [CrossRef]
- Querellou, S.; Abgral, R.; Le Roux, P.-Y.; Nowak, E.; Valette, G.; Potard, G.; Le Duc-Pennec, A.; Cavarec, M.-B.; Marianovski, R.; Salaün, P. Prognostic value of fluorine-18 fluorodeoxyglucose positron-emission tomography imaging in patients with head and neck squamous cell carcinoma. Head Neck 2012, 34, 462–468. [Google Scholar] [CrossRef]
- Minn, H.; Lapela, M.; Klemi, P.J.; Grénman, R.; Leskinen, S.; Lindholm, P.; Bergman, J.; Eronen, E.; Haaparanta, M.; Joensuu, H. Prediction of survival with fluorine-18-fluoro-deoxyglucose and PET in head and neck cancer. J. Nucl. Med. 1997, 38, 1907–1911. [Google Scholar]
- Paidpally, V.; Chirindel, A.; Lam, S.; Agrawal, N.; Quon, H.; Subramaniam, R.M. FDG-PET/CT imaging biomarkers in head and neck squamous cell carcinoma. Imaging Med. 2012, 4, 633–647. [Google Scholar] [CrossRef] [Green Version]
- Torizuka, T.; Tanizaki, Y.; Kanno, T.; Futatsubashi, M.; Naitou, K.; Ueda, Y.; Ouchi, Y. Prognostic value of 18F-FDG PET in patients with head and neck squamous cell cancer. AJR Am. J. Roentgenol. 2009, 192, W156–W160. [Google Scholar] [CrossRef]
- Scott, S.; Byrd, J.K.; Figueroa, R.; Williams, H.; Chen, J.; Lee, J.; Pucar, D. 18F-fluorodeoxyglucose positron emission tomography/computed tomography in predict-ing overall survival of oral cavity squamous cell carcinoma: Ongoing controversy. World J. Nucl. Med. 2020, 17, 111–117. [Google Scholar]
- Zhu, D.; Ma, T.; Niu, Z.; Zheng, J.; Han, A.; Zhao, S.; Yu, J. Prognostic significance of metabolic parameters measured by (18)F-fluorodeoxyglucose positron emission tomography/computed tomography in patients with small cell lung cancer. Lung Cancer 2001, 73, 332–337. [Google Scholar] [CrossRef] [PubMed]
- Hyun, S.H.; Choi, J.Y.; Shim, Y.M.; Kim, K.; Lee, S.J.; Cho, Y.S.; Kim, B.T.; Lee, J.Y.; Lee, K. Prognostic value of metabolic tumor volume measured by 18F-fluorodeoxyglucose posi-tron emission tomography in patients with oesophageal carcinoma. Ann. Surg. Oncol. 2010, 17, 115–122. [Google Scholar] [CrossRef] [PubMed]
- Chung, H.H.; Kwon, H.W.; Kang, K.W.; Park, N.-H.; Song, Y.-S.; Chung, J.-K.; Kang, S.-B.; Kim, J.W. Prognostic Value of Preoperative Metabolic Tumor Volume and Total Lesion Glycolysis in Patients with Epithelial Ovarian Cancer. Ann. Surg. Oncol. 2012, 19, 1966–1972. [Google Scholar] [CrossRef] [PubMed]
- Abgral, R.; Keromnes, N.; Robin, P.; Le Roux, P.-Y.; Bourhis, D.; Palard, X.; Rousset, J.; Valette, G.; Marianowski, R.; Salaun, P.-Y. Prognostic value of volumetric parameters measured by 18F-FDG PET/CT in patients with head and neck squamous cell carcinoma. Eur. J. Nucl. Med. Mol. Imaging 2014, 41, 659–667. [Google Scholar] [CrossRef]
- La, T.H.; Filion, E.J.; Turnbull, B.B.; Chu, J.N.; Lee, P.; Nguyen, K.; Maxim, P.; Quon, A.; Graves, E.E.; Loo, B.W.; et al. Metabolic Tumor Volume Predicts for Recurrence and Death in Head-and-Neck Cancer. Int. J. Radiat. Oncol. Biol. Phys. 2009, 74, 1335–1341. [Google Scholar] [CrossRef] [Green Version]
- Tang, C.; Murphy, J.D.; Khong, B.; La, T.H.; Kong, C.; Fischbein, N.J.; Colevas, A.D.; Iagaru, A.H.; Graves, E.E.; Loo, B.W.; et al. Validation that Metabolic Tumor Volume Predicts Outcome in Head-and-Neck Cancer. Int. J. Radiat. Oncol. Biol. Phys. 2012, 83, 1514–1520. [Google Scholar] [CrossRef] [Green Version]
- Moon, S.H.; Sun, J.M.; Ahn, J.S.; Park, K.; Kim, B.T.; Lee, K.H.; Choi, J.Y.; Ahn, M.-J. Predictive and Prognostic Value of 18F-fluorodeoxyglucose Uptake Combined with Thymi-dylate Synthase Expression in Patients with Advanced Non-Small Cell Lung Cancer. Sci. Rep. 2019, 9, 12215. [Google Scholar] [CrossRef] [Green Version]
- Wen, W.; Xuan, D.; Hu, Y.; Li, X.; Liu, L.; Xu, D. Prognostic value of maximum standard uptake value, metabolic tumor volume, and total lesion glycolysis of positron emission tomography/computed tomography in patients with breast cancer: A systematic review and meta-analysis. PLoS ONE 2019, 14, e0225959. [Google Scholar] [CrossRef]
- Lim, Y.; Bang, J.-I.; Han, S.-W.; Paeng, J.C.; Lee, K.-H.; Kim, J.H.; Kang, G.H.; Jeong, S.-Y.; Park, K.J.; Kim, T.-Y. Total lesion glycolysis (TLG) as an imaging biomarker in metastatic colorectal cancer patients treated with regorafenib. Eur. J. Nucl. Med. Mol. Imaging 2017, 44, 757–764. [Google Scholar] [CrossRef]
- Cheng, N.-M.; Chang, J.T.-C.; Huang, C.-G.; Tsan, D.-L.; Ng, S.-H.; Wang, H.-M.; Liao, C.-T.; Lin, C.-Y.; Hsu, C.-L.; Yen, T.-C. Prognostic value of pretreatment (18)F-FDG PET/CT and human papillomavirus type 16 testing in locally advanced oropharyngeal squamous cell carcinoma. Eur. J. Nucl. Med. Mol. Imaging 2012, 39, 1673–1684. [Google Scholar] [CrossRef] [PubMed]
- Moon, S.H.; Choi, J.Y.; Lee, H.J.; Son, Y.-I.; Baek, C.-H.; Ahn, Y.C.; Park, K.; Lee, K.-H.; Kim, B.-T. Prognostic value of18F-FDG PET/CT in patients with squamous cell carcinoma of the tonsil: Comparisons of volume-based metabolic parameters. Head Neck 2013, 35, 15–22. [Google Scholar] [CrossRef] [PubMed]
- Park, H.L.; Yoo, I.R.; Boo, S.H.; Park, S.Y.; Park, J.K.; Sung, S.W.; Moon, S.W. Does FDG PET/CT have a role in determining adjuvant chemotherapy in surgical mar-gin-negative stage IA non-small cell lung cancer patients? J. Cancer Res. Clin. Oncol. 2019, 145, 1021–1026. [Google Scholar] [CrossRef] [PubMed]
- Annunziata, S.; Cuccaro, A.; Calcagni, M.L.; Hohaus, S.; Giordano, A.; Rufini, V. Interim FDG-PET/CT in Hodgkin lymphoma: The prognostic role of the ratio between target lesion and liver SUVmax (rPET). Ann. Nucl. Med. 2016, 30, 588–592. [Google Scholar] [CrossRef]
- Choi, K.H.; Song, J.H.; Park, E.Y.; Hong, J.H.; Yoo, I.R.; Lee, Y.S.; Kim, Y.S.; Sun, D.-I.; Kim, M.-S. Analysis of PET parameters as prognosticators of survival and tumor extent in Oro-pharyngeal Cancer treated with surgery and postoperative radiotherapy. BMC Cancer 2021, 21, 317. [Google Scholar] [CrossRef]
- Roxburgh, C.S.; McMillan, D.C. Role of systemic inflammatory response in predicting survival in patients with primary operable cancer. Future Oncol. 2010, 6, 149–163. [Google Scholar] [CrossRef]
- McMillan, D.C. Systemic inflammation, nutritional status and survival in patients with cancer. Curr. Opin. Clin. Nutr. Metab. Care 2009, 12, 223–226. [Google Scholar] [CrossRef] [Green Version]
- Ohashi, T.; Terasawa, K.; Aoki, M.; Akazawa, T.; Shibata, H.; Kuze, B.; Asano, T.; Kato, H.; Miyazaki, T.; Matsuo, M.; et al. The importance of FDG-PET/CT parameters for the assessment of the immune status in advanced HNSCC. Auris Nasus Larynx 2020, 47, 658–667. [Google Scholar] [CrossRef]
- Guo, D.; Jin, F.; Jing, W.; Li, M.; Chen, D.; Zou, B.; Yue, J.; Jiang, G.; Fu, L.; Zhu, H.; et al. Incorporation of the SUVmax Measured From FDG PET and Neutrophil-to-lymphocyte Ratio Im-proves Prediction of Clinical Outcomes in Patients with Locally Advanced Non-small-cell Lung Cancer. Clin. Lung Cancer 2019, 20, 412–419. [Google Scholar] [CrossRef]







{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| T Stage | TX | T1 | T2 | T3 | T4 | P |
|---|---|---|---|---|---|---|
| Patient details | ||||||
| Proportion of studies (%) | 16 (13.5) | 18 (16.4) | 18 (16.4) | 19 (18.3) | 35 (35.6) | - |
| Mean age (years) | 63.4 | 53.8 | 55.8 | 59.0 | 56.7 | 0.098 |
| Male (%) | 78.6 | 76.5 | 64.7 | 68.4 | 70.3 | 0.901 |
| Smoker (%) | 64.3 | 52.9 | 70.6 | 68.4 | 64.9 | 0.696 |
| Mean packs/year | 13.1 | 12.8 | 17.7 | 17.1 | 16.9 | 0.871 |
| Mean overall survival (months) | 14.4 | 62.7 | 18.0 | 22.6 | 25.1 | 0.003 |
| Mean event free survival (months) | 31.0 | 68.6 | 62.4 | 48.5 | 66.3 | 0.156 |
| HPV+ (%) | 0 | 58.8 | 47.1 | 31.6 | 10.8 | <0.001 |
| Tumor localization % | ||||||
| Hypopharynx/larynx | 0 | 5.9 | 29.4 | 15.8 | 37.8 | <0.001 |
| Nasopharynx | 0 | 0 | 0 | 0 | 2.7 | |
| Oropharynx | 0 | 88.2 | 52.9 | 68.4 | 35.1 | |
| Oral cavity | 0 | 5.9 | 17.7 | 10.3 | 21.6 | |
| CUP | 100 | 0 | 0 | 0 | 0 | |
| Differentiation | ||||||
| G1 | 0 | 5.9 | 5.9 | 0 | 5.4 | 0.006 |
| G2 | 7.1 | 58.8 | 64.7 | 68.4 | 67.6 | |
| G3 | 35.7 | 17.7 | 17.7 | 26.3 | 16.2 | |
| N staging | ||||||
| 0 | 0 | 12.5 | 25.0 | 26.3 | 13.9 | 0.004 |
| 1 | 0 | 18.8 | 12.5 | 0 | 8.3 | |
| 2 | 50 | 56.3 | 56.3 | 63.2 | 75 | |
| 3 | 50 | 12.5 | 6.3 | 10.5 | 2.8 | |
| M0 stage (%) | 15.6 | 19.5 | 19.5 | 23.4 | 22.1 | 0.271 |
| Treatment | ||||||
| Surgery | 0 | 0 | 11.8 | 0 | 0 | 0.001 |
| Chemotherapy | 7.1 | 0 | 0 | 0 | 0 | |
| RT | 21.4 | 0 | 11.8 | 26.3 | 8.1 | |
| Surgery/Chemo | 14.3 | 5.9 | 5.9 | 0 | 0 | |
| Surgery/RT | 42.9 | 35.3 | 11.8 | 5.3 | 8.1 | |
| Surgery/Chemo/RT | 7.1 | 35.3 | 29.4 | 31.6 | 24.3 | |
| RTCH | 7.1 | 23.5 | 29.4 | 36.8 | 59.5 | |
| Parameter | CUP | T1 | T2 | T3 | T4 |
|---|---|---|---|---|---|
| TotalSUV | 6984.1 | 307.5 | 850.1 | 1396.2 | 1519.8 |
| MTV (cm3) | 47.1 | 6.0 | 12.0 | 17.0 | 18.1 |
| TLG | 447.0 | 20.8 | 54.4 | 86.7 | 98.7 |
| TLRTLG | 13.3 | 0.7 | 2.1 | 2.6 | 3.8 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Cegla, P.; Currie, G.; Wróblewska, J.P.; Cholewiński, W.; Kaźmierska, J.; Marszałek, A.; Kubiak, A.; Golusinski, P.; Golusiński, W.; Majchrzak, E. Influence of Semiquantitative [18F]FDG PET and Hematological Parameters on Survival in HNSCC Patients Using Neural Network Analysis. Pharmaceuticals 2022, 15, 224. https://doi.org/10.3390/ph15020224
Cegla P, Currie G, Wróblewska JP, Cholewiński W, Kaźmierska J, Marszałek A, Kubiak A, Golusinski P, Golusiński W, Majchrzak E. Influence of Semiquantitative [18F]FDG PET and Hematological Parameters on Survival in HNSCC Patients Using Neural Network Analysis. Pharmaceuticals. 2022; 15(2):224. https://doi.org/10.3390/ph15020224
Chicago/Turabian StyleCegla, Paulina, Geoffrey Currie, Joanna P. Wróblewska, Witold Cholewiński, Joanna Kaźmierska, Andrzej Marszałek, Anna Kubiak, Pawel Golusinski, Wojciech Golusiński, and Ewa Majchrzak. 2022. "Influence of Semiquantitative [18F]FDG PET and Hematological Parameters on Survival in HNSCC Patients Using Neural Network Analysis" Pharmaceuticals 15, no. 2: 224. https://doi.org/10.3390/ph15020224