
Vitamin D and Cardiovascular Disease: Current Evidence and Future Perspectives

 ,
,
Abstract
:1. Introduction
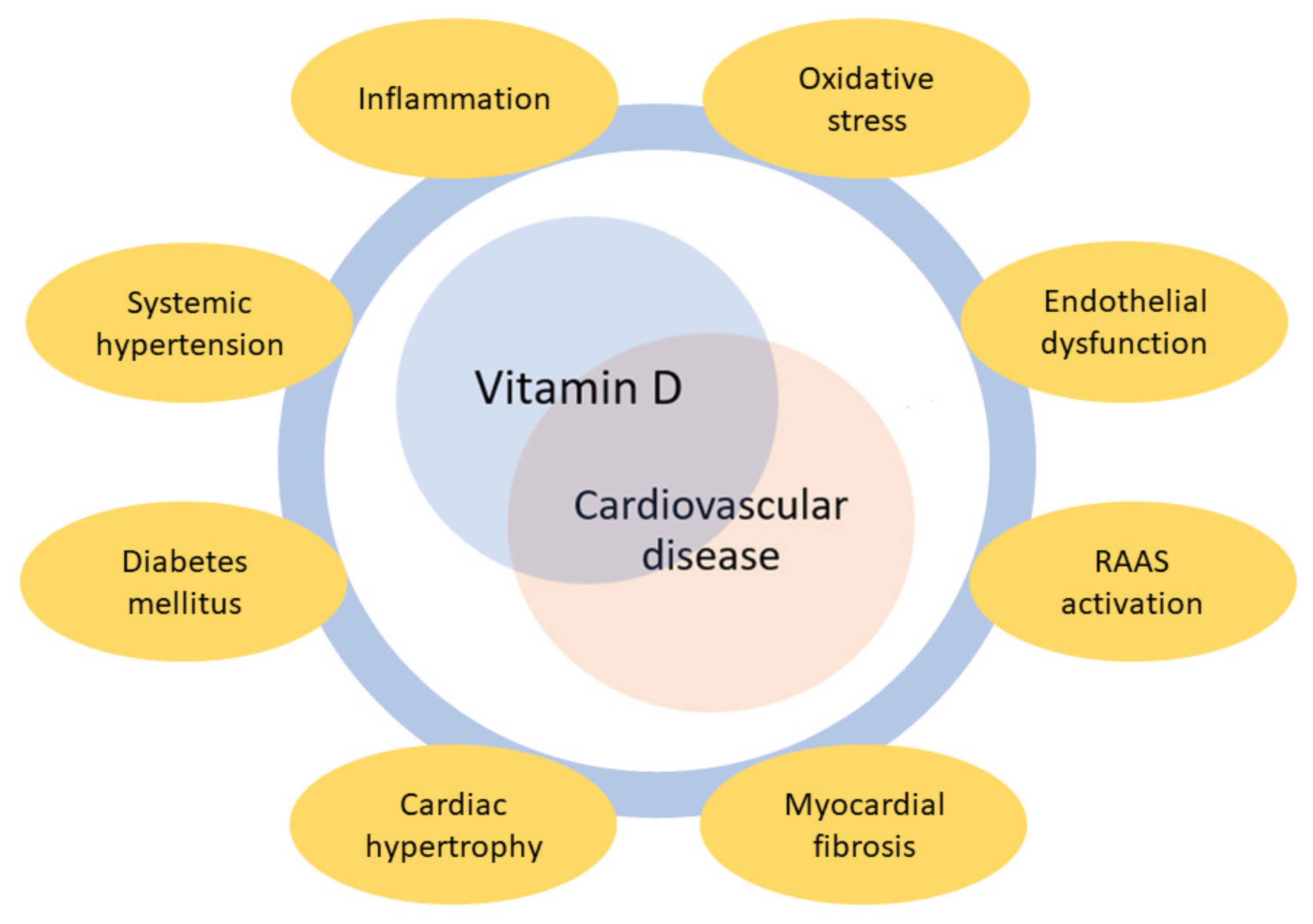
2. Vitamin D and the Cardiovascular System
3. Vitamin D and Coronary Artery Disease
4. Vitamin D and Heart Failure
5. Vitamin D and Atrial Fibrillation
6. Vitamin D and Interaction with Antiplatelet Drugs
7. Future Perspectives
8. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Mensah, G.A.; Wei, G.S.; Sorlie, P.D.; Fine, L.J.; Rosenberg, Y.; Kaufmann, P.G.; Mussolino, M.E.; Hsu, L.L.; Addou, E.; Engelgau, M.M.; et al. Decline in Cardiovascular Mortality: Possible Causes and Implications. Circ. Res. 2017, 120, 366–380. [Google Scholar] [CrossRef]
- US Preventive Services Task Force; Curry, S.J.; Krist, A.H.; Owens, D.K.; Barry, M.J.; Caughey, A.B.; Davidson, K.W.; Doubeni, C.A.; Epling, J.W., Jr.; Kemper, A.R.; et al. Risk Assessment for Cardiovascular Disease with Nontraditional Risk Factors: US Preventive Services Task Force Recommendation Statement. JAMA 2018, 320, 272–280. [Google Scholar]
- Norman, P.E.; Powell, J.T. Vitamin D and cardiovascular disease. Circ. Res. 2014, 114, 379–393. [Google Scholar] [CrossRef] [PubMed]
- Palacios, C.; Gonzalez, L. Is vitamin D deficiency a major global public health problem? J. Steroid Biochem. Mol. Biol. 2014, 144 Pt A, 138–145. [Google Scholar] [CrossRef] [Green Version]
- Amrein, K.; Scherkl, M.; Hoffmann, M.; Neuwersch-Sommeregger, S.; Köstenberger, M.; Tmava Berisha, A.; Martucci, G.; Pilz, S.; Malle, O. Vitamin D deficiency 2.0: An update on the current status worldwide. Eur. J. Clin. Nutr. 2020, 74, 1498–1513. [Google Scholar] [CrossRef]
- Vaidya, A.; Williams, J.S. The relationship between vitamin D and the renin-angiotensin system in the pathophysiology of hypertension, kidney disease, and diabetes. Metabolism 2012, 61, 450–458. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Nakashima, A.; Yokoyama, K.; Yokoo, T.; Urashima, M. Role of vitamin D in diabetes mellitus and chronic kidney disease. World J. Diabetes 2016, 7, 89–100. [Google Scholar] [CrossRef]
- Pike, J.W.; Meyer, M.B. The vitamin D receptor: New paradigms for the regulation of gene expression by 1,25-dihydroxyvitamin D(3). Endocrinol. Metab. Clin. N. Am. 2010, 39, 255–269. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ellison, T.I.; Dowd, D.R.; MacDonald, P.N. Calmodulin-dependent kinase IV stimulates vitamin D receptor-mediated transcription. Mol. Endocrinol. 2005, 19, 2309–2319. [Google Scholar] [CrossRef] [Green Version]
- Chen, S.; Law, C.S.; Grigsby, C.L.; Olsen, K.; Hong, T.T.; Zhang, Y.; Yeghiazarians, Y.; Gardner, D.G. Cardiomyocyte-specific deletion of the vitamin D receptor gene results in cardiac hypertrophy. Circulation 2011, 124, 1838–1847. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zittermann, A.; Trummer, C.; Theiler-Schwetz, V.; Lerchbaum, E.; März, W.; Pilz, S. Vitamin D and Cardiovascular Disease: An Updated Narrative Review. Int. J. Mol. Sci. 2021, 22, 2896. [Google Scholar] [CrossRef] [PubMed]
- Zittermann, A. Vitamin D Status, Supplementation and Cardiovascular Disease. Anticancer Res. 2018, 38, 1179–1186. [Google Scholar] [PubMed]
- Franczyk, A.; Stolarz-Skrzypek, K.; Wesołowska, A.; Czarnecka, D. Vitamin D and vitamin D receptor activators in treatment of hypertension and cardiovascular disease. Cardiovasc. Hematol. Disord. Drug Targets 2014, 14, 34–44. [Google Scholar] [CrossRef] [PubMed]
- Ni, W.; Watts, S.W.; Ng, M.; Chen, S.; Glenn, D.J.; Gardner, D.G. Elimination of vitamin D receptor in vascular endothelial cells alters vascular function. Hypertension 2014, 64, 1290–1298. [Google Scholar] [CrossRef] [Green Version]
- Khammissa, R.A.G.; Fourie, J.; Motswaledi, M.H.; Ballyram, R.; Lemmer, J.; Feller, L. The Biological Activities of Vitamin D and Its Receptor in Relation to Calcium and Bone Homeostasis, Cancer, Immune and Cardiovascular Systems, Skin Biology, and Oral Health. BioMed. Res. Int. 2018, 2018, 9276380. [Google Scholar] [CrossRef] [PubMed]
- Pilz, S.; Tomaschitz, A. Role of vitamin D in arterial hypertension. Expert Rev. Cardiovasc. Ther. 2010, 8, 1599–1608. [Google Scholar] [CrossRef] [PubMed]
- Hiemstra, T.; Lim, K.; Thadhani, R.; Manson, J.E. Vitamin D and Atherosclerotic Cardiovascular Disease. J. Clin. Endocrinol. Metab. 2019, 104, 4033–4050. [Google Scholar] [CrossRef]
- Freundlich, M.; Li, Y.C.; Quiroz, Y.; Bravo, Y.; Seeherunvong, W.; Faul, C.; Weisinger, J.R.; Rodriguez-Iturbe, B. Paricalcitol downregulates myocardial renin-angiotensin and fibroblast growth factor expression and attenuates cardiac hypertrophy in uremic rats. Am. J. Hypertens. 2014, 27, 720–726. [Google Scholar] [CrossRef] [Green Version]
- Cui, C.; Xu, P.; Li, G.; Qiao, Y.; Han, W.; Geng, C.; Liao, D.; Yang, M.; Chen, D.; Jiang, P. Vitamin D receptor activation regulates microglia polarization and oxidative stress in spontaneously hypertensive rats and angiotensin II-exposed microglial cells: Role of renin-angiotensin system. Redox Biol. 2019, 26, 101295. [Google Scholar] [CrossRef] [PubMed]
- Xu, J.; Yang, J.; Chen, J.; Luo, Q.; Zhang, Q.; Zhang, H. Vitamin D alleviates lipopolysaccharide-induced acute lung injury via regulation of the renin-angiotensin system. Mol. Med. Rep. 2017, 16, 7432–7438. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Oh, J.; Matkovich, S.J.; Riek, A.E.; Bindom, S.M.; Shao, J.S.; Head, R.D.; Barve, R.A.; Sands, M.S.; Carmeliet, G.; Osei-Owusu, P.; et al. Macrophage secretion of miR-106b-5p causes renin-dependent hypertension. Nat. Commun. 2020, 11, 4798. [Google Scholar] [CrossRef] [PubMed]
- Polly, P.; Tan, T.C. The role of vitamin D in skeletal and cardiac muscle function. Front. Physiol. 2014, 5, 145. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Roffe-Vazquez, D.N.; Huerta-Delgado, A.S.; Castillo, E.C.; Villarreal-Calderón, J.R.; Gonzalez-Gil, A.M.; Enriquez, C.; Garcia-Rivas, G.; Elizondo-Montemayor, L. Correlation of Vitamin D with Inflammatory Cytokines, Atherosclerotic Parameters, and Lifestyle Factors in the Setting of Heart Failure: A 12-Month Follow-Up Study. Int. J. Mol. Sci. 2019, 20, 5811. [Google Scholar] [CrossRef] [Green Version]
- Wöbke, T.K.; Sorg, B.L.; Steinhilber, D. Vitamin D in inflammatory diseases. Front. Physiol. 2014, 5, 244. [Google Scholar] [CrossRef] [Green Version]
- Siadat, Z.D.; Kiani, K.; Sadeghi, M.; Shariat, A.S.; Farajzadegan, Z.; Kheirmand, M. Association of vitamin D deficiency and coronary artery disease with cardiovascular risk factors. J. Res. Med. Sci. 2012, 17, 1052–1055. [Google Scholar]
- Raslan, E.; Soliman, S.S.A.; Nour, Z.A.; Ahmed, D.; Saad, N.E.S. Association of Vitamin D Deficiency with Chronic Stable Angina: A Case Control Study. High Blood Press. Cardiovasc. Prev. 2019, 26, 77–80. [Google Scholar] [CrossRef]
- Xu, R.; Li, Y.Y.; Ma, L.L.; Yang, H.N. Association of vitamin D status with coronary artery disease in postmenopausal women. Medicine 2020, 99, e19544. [Google Scholar] [CrossRef] [PubMed]
- Lund, B.; Badskjaer, J.; Lund, B.; Soerensen, O.H. Vitamin D and ischaemic heart disease. Horm. Metab. Res. 1978, 10, 553–556. [Google Scholar] [CrossRef]
- Scragg, R.; Jackson, R.; Holdaway, I.M.; Lim, T.; Beaglehole, R. Myocardial infarction is inversely associated with plasma 25-hydroxyvitamin D3 levels: A community-based study. Int. J. Epidemiol. 1990, 19, 559–563. [Google Scholar] [CrossRef]
- Lee, J.H.; Gadi, R.; Spertus, J.A.; Tang, F.; O’Keefe, J.H. Prevalence of vitamin D deficiency in patients with acute myocardial infarction. Am. J. Cardiol. 2011, 107, 1636–1638. [Google Scholar] [CrossRef] [Green Version]
- Brøndum-Jacobsen, P.; Benn, M.; Jensen, G.B.; Nordestgaard, B.G. 25-hydroxyvitamin d levels and risk of ischemic heart disease, myocardial infarction, and early death: Population-based study and meta-analyses of 18 and 17 studies. Arterioscler. Thromb. Vasc. Biol. 2012, 32, 2794–2802. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ng, L.L.; Sandhu, J.K.; Squire, I.B.; Davies, J.E.; Jones, D.J. Vitamin D and prognosis in acute myocardial infarction. Int. J. Cardiol. 2013, 168, 2341–2346. [Google Scholar] [CrossRef]
- Correia, L.C.; Sodré, F.; Garcia, G.; Sabino, M.; Brito, M.; Kalil, F.; Barreto, B.; Lima, J.C.; Noya-Rabelo, M.M. Relation of severe deficiency of vitamin D to cardiovascular mortality during acute coronary syndromes. Am. J. Cardiol. 2013, 111, 324–327. [Google Scholar] [CrossRef] [PubMed]
- De Metrio, M.; Milazzo, V.; Rubino, M.; Cabiati, A.; Moltrasio, M.; Marana, I.; Campodonico, J.; Cosentino, N.; Veglia, F.; Bonomi, A.; et al. Vitamin D plasma levels and in-hospital and 1-year outcomes in acute coronary syndromes: A prospective study. Medicine 2015, 94, e857. [Google Scholar] [CrossRef]
- Scragg, R.; Stewart, A.W.; Waayer, D.; Lawes, C.M.M.; Toop, L.; Sluyter, J.; Murphy, J.; Khaw, K.T.; Camargo, C.A., Jr. Effect of Monthly High-Dose Vitamin D Supplementation on Cardiovascular Disease in the Vitamin D Assessment Study: A Randomized Clinical Trial. JAMA Cardiol. 2017, 2, 608–616. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Giovannucci, E.; Liu, Y.; Hollis, B.W.; Rimm, E.B. 25-hydroxyvitamin D and risk of myocardial infarction in men: A prospective study. Arch. Int. Med. 2008, 168, 1174–1180. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wang, L.; Song, Y.; Manson, J.E.; Pilz, S.; März, W.; Michaëlsson, K.; Lundqvist, A.; Jassal, S.K.; Barrett-Connor, E.; Zhang, C.; et al. Circulating 25-hydroxy-vitamin D and risk of cardiovascular disease: A meta-analysis of prospective studies. Circ. Cardiovasc. Qual. Outcomes 2012, 5, 819–829. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Dziedzic, E.A.; Gąsior, J.S.; Pawłowski, M.; Wodejko-Kucharska, B.; Saniewski, T.; Marcisz, A.; Dąbrowski, M.J. Vitamin D level is associated with severity of coronary artery atherosclerosis and incidence of acute coronary syndromes in non-diabetic cardiac patients. Arch. Med. Sci. 2019, 15, 359–368. [Google Scholar] [CrossRef]
- Dziedzic, E.A.; Przychodzeń, S.; Dąbrowski, M. The effects of vitamin D on severity of coronary artery atherosclerosis and lipid profile of cardiac patients. Arch. Med. Sci. 2016, 12, 1199–1206. [Google Scholar] [CrossRef] [Green Version]
- Monraats, P.S.; Fang, Y.; Pons, D.; Pires, N.M.; Pols, H.A.; Zwinderman, A.H.; de Maat, M.P.; Doevendans, P.A.; DeWinter, R.J.; Tio, R.A.; et al. Vitamin D receptor: A new risk marker for clinical restenosis after percutaneous coronary intervention. Expert Opin. Ther. Targets 2010, 14, 243–251. [Google Scholar] [CrossRef]
- Chang, S.; Gao, L.; Yang, Y.; Tong, D.; Guo, B.; Liu, L.; Li, Z.; Song, T.; Huang, C. miR-145 mediates the antiproliferative and gene regulatory effects of vitamin D3 by directly targeting E2F3 in gastric cancer cells. Oncotarget 2015, 6, 7675–7685. [Google Scholar] [CrossRef] [Green Version]
- Liu, X.; Cheng, Y.; Yang, J.; Qin, S.; Chen, X.; Tang, X.; Zhou, X.; Krall, T.J.; Zhang, C. Flank sequences of miR-145/143 and their aberrant expression in vascular disease: Mechanism and therapeutic application. J. Am. Heart Assoc. 2013, 2, e000407. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Milazzo, V.; De Metrio, M.; Cosentino, N.; Marenzi, G.; Tremoli, E. Vitamin D and acute myocardial infarction. World J. Cardiol. 2017, 9, 14–20. [Google Scholar] [CrossRef]
- Padoan, L.; Beltrami, A.P.; Stenner, E.; Beleù, A.; Ruscio, M.; Sinagra, G.; Aleksova, A. Left ventricular adverse remodeling after myocardial infarction and its association with vitamin D levels. Int. J. Cardiol. 2019, 277, 159–165. [Google Scholar] [CrossRef]
- Bahrami, L.S.; Ranjbar, G.; Norouzy, A.; Arabi, S.M. Vitamin D supplementation effects on the clinical outcomes of patients with coronary artery disease: A systematic review and meta-analysis. Sci. Rep. 2020, 10, 12923. [Google Scholar] [CrossRef] [PubMed]
- Legarth, C.; Grimm, D.; Krüger, M.; Infanger, M.; Wehland, M. Potential beneficial Effects of vitamin D in coronary artery disease. Nutrients 2019, 12, 99. [Google Scholar] [CrossRef] [Green Version]
- De la Guía-Galipienso, F.; Martínez-Ferran, M.; Vallecillo, N.; Lavie, C.J.; Sanchis-Gomar, F.; Pareja-Galeano, H. Vitamin D and cardiovascular health. Clin. Nutr. 2021, 40, 2946–2957. [Google Scholar] [CrossRef] [PubMed]
- Donneyong, M.M.; Hornung, C.A.; Taylor, K.C.; Baumgartner, R.N.; Myers, J.A.; Eaton, C.B.; Gorodeski, E.Z.; Klein, L.; Martin, L.W.; Shikany, J.M.; et al. Risk of heart failure among postmenopausal women: A secondary analysis of the randomized trial of vitamin D plus calcium of the women’s health initiative. Circ. Heart Fail. 2015, 8, 49–56. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bischoff-Ferrari, H.A.; Vellas, B.; Rizzoli, R.; Kressig, R.W.; da Silva, J.A.P.; Blauth, M.; Felson, D.T.; McCloskey, E.V.; Watzl, B.; Hofbauer, L.C.; et al. DO-HEALTH Research Group. Effect of Vitamin D Supplementation, Omega-3 Fatty Acid Supplementation, or a Strength-Training Exercise Program on Clinical Outcomes in Older Adults: The DO-HEALTH Randomized Clinical Trial. JAMA 2020, 324, 1855–1868. [Google Scholar] [CrossRef]
- LeBoff, M.S.; Murata, E.M.; Cook, N.R.; Cawthon, P.; Chou, S.H.; Kotler, G.; Bubes, V.; Buring, J.E.; Manson, J.E. VITamin D and OmegA-3 TriaL (VITAL): Effects of Vitamin D Supplements on Risk of Falls in the US Population. J. Clin. Endocrinol. Metab. 2020, 105, 2929–2938. [Google Scholar] [CrossRef]
- Jessup, M.; Brozena, S. Heart failure. N. Engl. J. Med. 2003, 348, 2007–2018. [Google Scholar] [CrossRef] [PubMed]
- Zittermann, A.; Schleithoff, S.S.; Tenderich, G.; Berthold, H.K.; Körfer, R.; Stehle, P. Low vitamin D status: A contributing factor in the pathogenesis of congestive heart failure? J. Am. Coll. Cardiol. 2003, 41, 105–112. [Google Scholar] [CrossRef] [Green Version]
- Shane, E.; Mancini, D.; Aaronson, K.; Silverberg, S.J.; Seibel, M.J.; Addesso, V.; McMahon, D.J. Bone mass, vitamin D deficiency, and hyper-parathyroidism in congestive heart failure. Am. J. Med. 1997, 103, 197–207. [Google Scholar] [CrossRef]
- Anderson, J.L.; May, H.T.; Horne, B.D.; Bair, T.L.; Hall, N.L.; Carlquist, J.F.; Lappé, D.L.; Muhlestein, J.B. Intermountain Heart Collaborative (IHC) Study Group. Relation of vitamin D deficiency to cardiovascular risk factors, disease status, and incident events in a general healthcare population. Am. J. Cardiol. 2010, 106, 963–968. [Google Scholar] [CrossRef]
- Pilz, S.; März, W.; Wellnitz, B.; Seelhorst, U.; Fahrleitner-Pammer, A.; Dimai, H.P.; Boehm, B.O.; Dobnig, H. Association of vitamin D deficiency with heart failure and sudden cardiac death in a large cross-sectional study of patients referred for coronary angiography. J. Clin. Endocrinol. Metab. 2008, 93, 3927–3935. [Google Scholar] [CrossRef] [Green Version]
- Nolte, K.; Herrmann-Lingen, C.; Platschek, L.; Holzendorf, V.; Pilz, S.; Tomaschitz, A.; Düngen, H.D.; Angermann, C.E.; Hasenfuß, G.; Pieske, B.; et al. Vitamin D deficiency in patients with diastolic dysfunction or heart failure with preserved ejection fraction. ESC Heart Fail. 2019, 6, 262–270. [Google Scholar] [CrossRef]
- Kusunose, K.; Okushi, Y.; Okayama, Y.; Zheng, R.; Abe, M.; Nakai, M.; Sumita, Y.; Ise, T.; Tobiume, T.; Yamaguchi, K.; et al. Association between Vitamin D and heart failure mortality in 10,974 hospitalized individuals. Nutrients 2021, 13, 335. [Google Scholar] [CrossRef] [PubMed]
- Liu, L.C.; Voors, A.A.; van Veldhuisen, D.J.; van der Veer, E.; Belonje, A.M.; Szymanski, M.K.; Silljé, H.H.; van Gilst, W.H.; Jaarsma, T.; de Boer, R.A. Vitamin D status and outcomes in heart failure patients. Eur. J. Heart Fail. 2011, 13, 619–625. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kim, D.H.; Sabour, S.; Sagar, U.N.; Adams, S.; Whellan, D.J. Prevalence of hypovitaminosis D in cardiovascular diseases (from the National Health and Nutrition Examination Survey 2001 to 2004). Am. J. Cardiol. 2008, 102, 1540–1544. [Google Scholar] [CrossRef] [PubMed]
- Soh, V.; Tan, S.J.X.; Sehgal, R.; Shirke, M.M.; Ashry, A.; Harky, A. The Relationship Between Vitamin D Status and Cardiovascular Diseases. Curr. Probl. Cardiol. 2021, 46, 100836. [Google Scholar] [CrossRef] [PubMed]
- Gotsman, I.; Shauer, A.; Zwas, D.R.; Hellman, Y.; Keren, A.; Lotan, C.; Admon, D. Vitamin D deficiency is a predictor of reduced survival in patients with heart failure; vitamin D supplementation improves outcome. Eur. J. Heart Fail. 2012, 14, 357–366. [Google Scholar] [CrossRef] [PubMed]
- Gruson, D.; Ferracin, B.; Ahn, S.A.; Zierold, C.; Blocki, F.; Hawkins, D.M.; Bonelli, F.; Rousseau, M.F. 1,25-Dihydroxyvitamin D to PTH(1-84) Ratios Strongly Predict Cardiovascular Death in Heart Failure. PLoS ONE 2015, 10, e0135427. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Witte, K.K.; Byrom, R.; Gierula, J.; Paton, M.F.; Jamil, H.A.; Lowry, J.E.; Gillott, R.G.; Barnes, S.A.; Chumun, H.; Kearney, L.C.; et al. Effects of Vitamin D on Cardiac Function in Patients with Chronic HF: The VINDICATE Study. J. Am. Coll. Cardiol. 2016, 67, 2593–2603. [Google Scholar] [CrossRef] [Green Version]
- Zittermann, A.; Ernst, J.B.; Prokop, S.; Fuchs, U.; Dreier, J.; Kuhn, J.; Knabbe, C.; Birschmann, I.; Schulz, U.; Berthold, H.K.; et al. Effect of vitamin D on all-cause mortality in heart failure (EVITA): A 3-year randomized clinical trial with 4000 IU vitamin D daily. Eur. Heart J. 2017, 38, 2279–2286. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Schroten, N.F.; Ruifrok, W.P.; Kleijn, L.; Dokter, M.M.; Silljé, H.H.; Lambers Heerspink, H.J.; Bakker, S.J.; Kema, I.P.; van Gilst, W.H.; van Veldhuisen, D.J.; et al. Short-term vitamin D3 supplementation lowers plasma renin activity in patients with stable chronic heart failure: An open-label, blinded end point, randomized prospective trial (VitD-CHF trial). Am. Heart J. 2013, 166, 357–364. [Google Scholar] [CrossRef]
- Dalbeni, A.; Scaturro, G.; Degan, M.; Minuz, P.; Delva, P. Effects of six months of vitamin D supplementation in patients with heart failure: A randomized double-blind controlled trial. Nutr. Metab. Cardiovasc. Dis. 2014, 24, 861–868. [Google Scholar] [CrossRef]
- Jiang, W.L.; Gu, H.B.; Zhang, Y.F.; Xia, Q.Q.; Qi, J.; Chen, J.C. Vitamin D supplementation in the treatment of chronic heart failure: A meta-analysis of randomized controlled trials. Clin. Cardiol. 2016, 39, 56–61. [Google Scholar] [CrossRef] [Green Version]
- Wang, T.; Liu, Z.; Fu, J.; Min, Z. Meta-analysis of vitamin D supplementation in the treatment of chronic heart failure. Scand. Cardiovasc. J. 2019, 53, 110–116. [Google Scholar] [CrossRef] [PubMed]
- D’Amore, C.; Marsico, F.; Parente, A.; Paolillo, S.; De Martino, F.; Gargiulo, P.; Ferrazzano, F.; De Roberto, A.M.; La Mura, L.; Marciano, C.; et al. Vitamin D deficiency and clinical outcome in patients with chronic heart failure: A review. Nutr. Metab. Cardiovasc. Dis. 2017, 27, 837–849. [Google Scholar] [CrossRef] [PubMed]
- Morillo, C.A.; Banerjee, A.; Perel, P.; Wood, D.; Jouven, X. Atrial fibrillation: The current epidemic. J. Geriatr. Cardio. 2017, 14, 195–203. [Google Scholar]
- Freedman, B.; Hindricks, G.; Banerjee, A.; Baranchuk, A.; Ching, C.K.; Du, X.; Fitzsimons, D.; Healey, J.S.; Ikeda, T.; Lobban, T.C.A.; et al. World Heart Federation Roadmap on Atrial Fibrillation—A 2020 Update. Glob. Heart 2021, 16, 41. [Google Scholar] [CrossRef] [PubMed]
- Demir, M.; Uyan, U.; Melek, M. The effects of vitamin D deficiency on atrial fibrillation. Clin. Appl. Thromb. Hemost. 2014, 20, 98–103. [Google Scholar] [CrossRef]
- Huang, W.L.; Yang, J.; Yang, J.; Wang, H.B.; Yang, C.J.; Yang, Y. Vitamin D and new-onset atrial fibrillation: A meta-analysis of randomized controlled trials. Hellenic J. Cardiol. 2018, 59, 72–77. [Google Scholar] [CrossRef] [PubMed]
- Hu, Y.F.; Chen, Y.J.; Lin, Y.J.; Chen, S.A. Inflammation and the pathogenesis of atrial fibrillation. Nat. Rev. Cardiol. 2015, 12, 230–243. [Google Scholar] [CrossRef] [PubMed]
- Galea, R.; Cardillo, M.T.; Caroli, A.; Marini, M.G.; Sonnino, C.; Narducci, M.L.; Biasucci, L.M. Inflammation and C-reactive protein in atrial fibrillation: Cause or effect? Tex. Heart Inst. J. 2014, 41, 461–468. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Patel, D.; Druck, A.; Hoppensteadt, D.; Bansal, V.; Brailovsky, Y.; Syed, M.; Fareed, J. Relationship between 25-Hydroxyvitamin, D, Renin, and collagen remodeling biomarkers in atrial fibrillation. Clin. Appl. Thromb. Hemost. 2020, 26, 1076029619899702. [Google Scholar] [CrossRef] [Green Version]
- Zhang, Z.; Yang, Y.; Ng, C.Y.; Wang, D.; Wang, J.; Li, G.; Liu, T. Meta-analysis of Vitamin D Deficiency and Risk of Atrial Fibrillation. Clin. Cardiol. 2016, 39, 537–543. [Google Scholar] [CrossRef] [Green Version]
- Vitezova, A.; Cartolano, N.S.; Heeringa, J.; Zillikens, M.C.; Hofman, A.; Franco, O.H.; Kiefte-de Jong, J.C. Vitamin D and the risk of atrial fibrillation--the Rotterdam Study. PLoS ONE 2015, 10, e0125161. [Google Scholar] [CrossRef] [Green Version]
- Chen, W.R.; Liu, Z.Y.; Shi, Y.; Yin, D.W.; Wang, H.; Sha, Y.; Chen, Y.D. Relation of low vitamin D to nonvalvular persistent atrial fibrillation in Chinese patients. Ann. Noninvasive Electrocardiol. 2014, 19, 166–173. [Google Scholar] [CrossRef]
- Rienstra, M.; Cheng, S.; Larson, M.G.; McCabe, E.L.; Booth, S.L.; Jacques, P.F.; Lubitz, S.A.; Yin, X.; Levy, D.; Magnani, J.W.; et al. Vitamin D status is not related to development of atrial fibrillation in the community. Am. Heart J. 2011, 162, 538–541. [Google Scholar] [CrossRef] [Green Version]
- Alonso, A.; Misialek, J.R.; Michos, E.D.; Eckfeldt, J.; Selvin, E.; Soliman, E.Z.; Chen, L.Y.; Gross, M.D.; Lutsey, P.L. Serum 25-hydroxyvitamin D and the incidence of atrial fibrillation: The Atherosclerosis Risk in Communities (ARIC) study. Europace 2016, 18, 1143–1149. [Google Scholar] [CrossRef] [PubMed]
- Ozsin, K.K.; Sanri, U.S.; Toktas, F.; Kahraman, N.; Yavuz, S. Effect of plasma level of Vitamin D on postoperative atrial fibrillation in patients undergoing isolated coronary artery bypass grafting. Braz. J. Cardiovasc. Surg. 2018, 33, 217–223. [Google Scholar] [CrossRef] [PubMed]
- Gode, S.; Aksu, T.; Demirel, A.; Sunbul, M.; Gul, M.; Bakir, I.; Yeniterzi, M. Effect of vitamin D deficiency on the development of postoperative atrial fibrillation in coronary artery bypass patients. J. Cardiovasc. Thorac. Res. 2016, 8, 140–146. [Google Scholar] [CrossRef] [Green Version]
- Liu, X.; Wang, W.; Tan, Z.; Zhu, X.; Liu, M.; Wan, R.; Hong, K. The relationship between vitamin D and risk of atrial fibrillation: A dose-response analysis of observational studies. Nutr. J. 2019, 18, 73. [Google Scholar] [CrossRef] [PubMed]
- Cerit, L.; Özcem, B.; Cerit, Z.; Duygu, H. Preventive Effect of Preoperative Vitamin D Supplementation on Postoperative Atrial Fibrillation. Braz. J. Cardiovasc. Surg. 2018, 33, 347–352. [Google Scholar] [CrossRef] [PubMed]
- Belen, E.; Aykan, A.C.; Kalaycioglu, E.; Sungur, M.A.; Sungur, A.; Cetin, M. Low-Level Vitamin D Is Associated with Atrial Fibrillation in Patients with Chronic Heart Failure. Adv. Clin. Exp. Med. 2016, 25, 51–57. [Google Scholar] [CrossRef] [Green Version]
- Ozcan, O.U.; Gurlek, A.; Gursoy, E.; Gerede, D.M.; Erol, C. Relation of vitamin D deficiency and new-onset atrial fibrillation among hypertensive patients. J. Am. Soc. Hypertens. 2015, 9, 307–312. [Google Scholar] [CrossRef]
- Verdoia, M.; Pergolini, P.; Rolla, R.; Sartori, C.; Nardin, M.; Schaffer, A.; Barbieri, L.; Daffara, V.; Marino, P.; Bellomo, G.; et al. Novara Atherosclerosis Study Group (NAS). Vitamin D levels and high-residual platelet reactivity in patients receiving dual antiplatelet therapy with clopidogrel or ticagrelor. Platelets 2016, 27, 576–582. [Google Scholar] [CrossRef]
- Lu, B.C.; Shi, X.J.; Liang, L.; Dong, N.; Liu, Z.Z. Platelet surface CD62p and serum vitamin D levels are associated with clopidogrel resistance in chinese patients with ischemic stroke. J. Stroke Cerebrovasc. Dis. 2019, 28, 1323–1328. [Google Scholar] [CrossRef]
- Aihara, K.; Azuma, H.; Akaike, M.; Ikeda, Y.; Yamashita, M.; Sudo, T.; Hayashi, H.; Yamada, Y.; Endoh, F.; Fujimura, M.; et al. Disruption of nuclear vitamin D receptor gene causes enhanced thrombogenicity in mice. J. Biol. Chem. 2004, 279, 35798–35802. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Silvagno, F.; De Vivo, E.; Attanasio, A.; Gallo, V.; Mazzucco, G.; Pescarmona, G. Mitochondrial localization of vitamin D receptor in human platelets and differentiated megakaryocytes. PLoS ONE 2010, 5, e8670. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Borst, O.; Münzer, P.; Schmid, E.; Schmidt, E.M.; Russo, A.; Walker, B.; Yang, W.; Leibrock, C.; Szteyn, K.; Schmidt, S.; et al. 1,25(OH)2 vitamin D3-dependent inhibition of platelet Ca2+ signaling and thrombus formation in klotho-deficient mice. FASEB J. 2014, 28, 2108–2119. [Google Scholar] [CrossRef] [PubMed]
- Sultan, M.; Twito, O.; Tohami, T.; Ramati, E.; Neumark, E.; Rashid, G. Vitamin D diminishes the high platelet aggregation of type 2 diabetes mellitus patients. Platelets 2019, 30, 120–125. [Google Scholar] [CrossRef]
- Verdoia, M.; Pergolini, P.; Rolla, R.; Nardin, M.; Schaffer, A.; Barbieri, L.; Daffara, V.; Marino, P.; Bellomo, G.; Suryapranata, H.; et al. Novara Atherosclerosis Study Group (NAS). Impact of high-dose statins on vitamin D levels and platelet function in patients with coronary artery disease. Thromb. Res. 2017, 150, 90–95. [Google Scholar] [CrossRef] [PubMed]
- Drocourt, L.; Ourlin, J.C.; Pascussi, J.M.; Maurel, P.; Vilarem, M.J. Expression of CYP3A4, CYP2B6, and CYP2C9 is regulated by the vitamin D receptor pathway in primary human hepatocytes. J. Biol. Chem. 2002, 277, 25125–25132. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Fan, J.; Liu, S.; Du, Y.; Morrison, J.; Shipman, R.; Pang, K.S. Up-regulation of transporters and enzymes by the vitamin D receptor ligands, 1alpha,25-dihydroxyvitamin D3 and vitamin D analogs, in the Caco-2 cell monolayer. J. Pharmacol. Exp. Ther. 2009, 330, 389–402. [Google Scholar] [CrossRef] [Green Version]
- Schmiedlin-Ren, P.; Thummel, K.E.; Fisher, J.M.; Paine, M.F.; Lown, K.S.; Watkins, P.B. Expression of enzymatically active CYP3A4 by Caco-2 cells grown on extracellular matrix-coated permeable supports in the presence of 1alpha,25-dihydroxyvitamin D3. Mol. Pharmacol. 1997, 51, 741–754. [Google Scholar] [CrossRef] [Green Version]
- Daly, A.K. Significance of the minor cytochrome P450 3A isoforms. Clin. Pharmacokinet. 2006, 45, 13–31. [Google Scholar] [CrossRef]
- Webb, A.R.; Kline, L.; Holick, M.F. Influence of season and latitude on the cutaneous synthesis of vitamin D3: Exposure to winter sunlight in Boston and Edmonton will not promote vitamin D3 synthesis in human skin. J. Clin. Endocrinol. Metab. 1988, 67, 373–378. [Google Scholar] [CrossRef] [Green Version]
- Trummer, O.; Pilz, S.; Hoffmann, M.M.; Winkelmann, B.R.; Boehm, B.O.; März, W.; Pieber, T.R.; Obermayer-Pietsch, B.; Renner, W. Vitamin D and mortality: A Mendelian randomization study. Clin. Chem. 2013, 59, 793–797. [Google Scholar] [CrossRef] [Green Version]
- Manson, J.E.; Cook, N.R.; Lee, I.M.; Christen, W.; Bassuk, S.S.; Mora, S.; Gibson, H.; Gordon, D.; Copeland, T.; D’Agostino, D.; et al. VITAL Research Group. Vitamin D Supplements and Prevention of Cancer and Cardiovascular Disease. N. Engl. J. Med. 2019, 380, 33–44. [Google Scholar] [CrossRef] [PubMed]
- Tang, J.C.Y.; Nicholls, H.; Piec, I.; Washbourne, C.J.; Dutton, J.J.; Jackson, S.; Greeves, J.; Fraser, W.D. Reference intervals for serum 24,25-dihydroxyvitamin D and the ratio with 25-hydroxyvitamin D established using a newly developed LC-MS/MS method. J. Nutr. Biochem. 2017, 46, 21–29. [Google Scholar] [CrossRef] [PubMed] [Green Version]


{kind=link}
| Author | Country | Study Design/Type of Observation | Study Population | Patients (n) Age (yrs) Gender | Definition of Vit. D Deficiency (ng/mL) | Prevalence of Vit. D Deficiency | Major Findings |
|---|---|---|---|---|---|---|---|
| Raslan [26] | Egypt | Case–-control /prospective | CCS | n = 84 | - | - | Every 10-unit (ng/mL) increase in vitamin D level decreased the chance of having chronic stable angina by three times |
| Xu [27] | China | Case–control /prospective | Postmenopausal women | n = 93 67 ± 6 yrs | Deficiency: <10 | - | Vitamin D deficiency increased CAD risk (OR = 2.9) |
| Lee [30] | US | Retrospective | NSTEMI/STEMI | n = 219 58 ± 11 yrs 74% males | Insufficiency: 21–29 Deficiency: <20 | 75% insufficient; 21% deficient | - |
| Brøndum-Jacobsen [31] | Denmark | Population-based study /retrospective | General population | n = 10,170 57 yrs 44% males | - | - | Patients with low vitamin D levels had increased adjusted risks of CAD of 72%, of AMI of 99%, and of fatal CAD/AMI of 122% compared to those with higher vitamin D levels at 29-years FU |
| Ng [32] | England | Cohort study /prospective | NSTEMI/STEMI | n = 1259 66 ± 13 yrs 72% males | Deficiency: <20 | 74% deficient | A significant higher incidence of MACE in patients with vitamin D deficiency at 1.6-years FU |
| Correia [33] | Brazil | Retrospective | ACS | n = 20670 ± 12 yrs 50% males | Severe deficiency: <10 | 10% severely deficient | A significant higher incidence of in-hospital and long-term mortality (2-year FU) in patients with severe vitamin D deficiency |
| De Metrio [34] | Italy | Cohort study /prospective | NSTEMI/STEMI | n = 814 67 ± 12 yrs 72% males | Insufficiency: 21–29 Deficiency: <20 | 19% insufficient; 70% deficient | A higher incidence of in-hospital mortality, mechanical ventilation, and major bleeding in patients with the lowest quartile of vitamin D. A significant higher incidence of 1-year mortality and re-hospitalization for HF in patients with the lowest quartile of vitamin D |
| Scragg [35] | Mostly from New Zeland | RCT /prospective | Participants from the community; adults aged 50–84 years | n = 5108 66 ± 8 yrs 58% males | Oral vitamin D3 in an initial dose of 20,000 IU, followed a month later by monthly doses of 100,000 IU, or placebo for a median of 3.3 years | The primary outcome of CVD incidence and death occurred in 11.8% in the vitamin D group and in 11.5% in the placebo group (adjusted HR: 1.02 (95% CI, 0.87–1.20)). Similar results were seen for participants with baseline vitamin D deficiency and for secondary outcomes (angina, HF, hypertension, arrhythmias, arteriosclerosis, stroke, and venous thrombosis) | |
| Study #1 | Study #2 | Study #3 | Study #4 | |
|---|---|---|---|---|
| ClinicalTrials.gov Identifier | NCT03416361 | NCT02996721 | NCT03086746 | NCT02178410 |
| Study start | December 2021 | April 2017 | April 2018 | October 2012 |
| Study type | Interventional | Interventional | Observational | Interventional |
| Study design | RCT | RCT | Prospective | RCT |
| Status | Not yet recruiting | Recruiting | Recruiting | Recruiting |
| Clinical setting | Stable HF | AMI | STEMI | General population |
| Interventions | 4000 IU vitamin D3/day | Supplementation to maintain | 2000 IU vitamin D/day or | Vitamin D levels > 40 ng/mL |
| 1 gr omega-3/day | ||||
| Main outcomes | 2-year mortality and HF | 2-year death, AMI | 6-month 5% reduction in LVEF | 7-year AF |
| Hospitalization | HF hospitalization, CVA | 15% increase in LVESVi | ||
| Estimated enrollment (n) | 1253 | 890 | 800 | 25,871 |
| Author [Ref] | Country | Study Design/Type of Observation | Study Population | Patients (n) Age (yrs) Gender (Male) | Prevalence of Vitamin D Deficiency and Major Findings |
|---|---|---|---|---|---|
| Zitterman [52] | Germany | Case–control /prospective | NYHA ≥II | n = 53 60% males | Significant reduction of vitamin D levels in HF patients |
| Shane [53] | US | Cohort study /prospective | NYHA III–IV | n = 101 79% males | 17% of the study patients had vitamin D levels <9 pg/mL |
| Anderson [54] | US | Cohort study /prospective | General healthcare population | n = 41,504 | 97% of HF patients had vitamin D levels <30 ng/mL 1.31 HR for new HF development in patients with low and very low vitamin D |
| Liu [58] | Netherlands | Cohort study /prospective | NYHA II–IV | n = 548 74 years 61% males | 1.09 HR (95% CI 1.00–1.16) for all-cause mortality and re-hospitalization for HF at 18 months per 10 nmol/L decrease of vitamin D |
| Kim [59] | US | Retrospective | NHANES from 2001–2004 | n = 8351 | 89% of HF patients with CAD had vitamin D <30 ng/mL |
| Gotsman [61] | Israel | Case–control/retrospective | Age ≥45 years | n = 49,834 49% males | 1.52 HR (95% CI 1.21–1.92) for 1.6-year mortality in patients with vitamin D deficiency (<25 nmol/L). 0.68 HR (95% CI 0.54–0.85) for 1.6-year mortality in patients in therapy with vitamin D supplementation |
| Gruson [62] | Belgium | Cohort study /prospective | LVEF ≥35% | n = 1709 69 years 79% males | Vitamin D significantly predicted CV death and heart transplantation at 4.1 years |
| Witte [63] | Caucasian Non-Caucasian | RCT /prospective | LVEF ≤ 45% + NYHA II–III + vitamin D < 20 ng/mL | n = 229 69 ± 13 yrs 79% males | 1-year of high-dose vitamin D supplementation (4000 IU daily) did not improve 6-min walk distance at 1 year but was associated with a significant improvement in LVEF and a reversal of LV remodeling |
| Zitterman [64] | Germany | RCT /prospective | NYHA ≥ II + vit D ≤ 75 nmol/L | n = 40,054 55 years 83% males | 3-year mortality was not different in patients receiving vitamin D (4000 IU/day) or placebo with a HR of 1.09 (95% CI 0.69–1.71). Other secondary clinical endpoints were similar between groups (HF hospitalization, resuscitation, highly urgent listing for heart transplantation, heart transplantation, and hypercalcemia). |
| Author [Ref.] | Country | Study Design/Type of Observation | Study Population | Patients (n) | Age (yrs) | Gender (males) | Endpoint Considered | Major Findings |
|---|---|---|---|---|---|---|---|---|
| Chen [79] | China | Case–control /retrospective | - | 322 | 65 ± 5 | 45% | Incidence of AF | Vitamin D <20 ng/mL increased AF risk by two times |
| Gode [83] | Turkey | Case–control /prospective | CABG | 90 | 59 ± 6 | 33% | New-onset post-op AF | Vitamin D levels in AF patients: 9 ng/mL Vitamin D levels in non-AF patients: 15 ng/mL |
| Cerit [85] | Cyprus | Retrospective | On-pump CABG | 128 | 65 ± 9 | 86% | New-onset post-op AF | Vitamin D levels in AF patients: 20 ng/mL Vitamin D levels in non-AF patients: 26 ng/mL |
| Ozcan [87] | Turkey | Case–control /prospective | Hypertensive patients | 227 | - | - | new-onset AF | Vitamin D <20 ng/mL increased AF risk by 1.7 times |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Cosentino, N.; Campodonico, J.; Milazzo, V.; De Metrio, M.; Brambilla, M.; Camera, M.; Marenzi, G. Vitamin D and Cardiovascular Disease: Current Evidence and Future Perspectives. Nutrients 2021, 13, 3603. https://doi.org/10.3390/nu13103603
Cosentino N, Campodonico J, Milazzo V, De Metrio M, Brambilla M, Camera M, Marenzi G. Vitamin D and Cardiovascular Disease: Current Evidence and Future Perspectives. Nutrients. 2021; 13(10):3603. https://doi.org/10.3390/nu13103603
Chicago/Turabian StyleCosentino, Nicola, Jeness Campodonico, Valentina Milazzo, Monica De Metrio, Marta Brambilla, Marina Camera, and Giancarlo Marenzi. 2021. "Vitamin D and Cardiovascular Disease: Current Evidence and Future Perspectives" Nutrients 13, no. 10: 3603. https://doi.org/10.3390/nu13103603