1. Introduction
Hyaluronan (HA) is synthesized in all animals and some microorganisms. In vivo, it is present in all connective tissues and organs, including the skin, joint fluid, blood vessels, serum, the brain, cartilage, heart valves, and the umbilical cord. The skin is the largest organ of the body, accounting for 50% of the total body mass [
1].
Under the impact of various factors (e.g., aging, ultraviolet light, and dryness, etc.), the content of HA in the skin becomes low and the water content of the horny layer is decreased, leading to the formation of wrinkles and skin aging [
2,
3]. A study reported that the amount of HA contained in the skin gradually decreases with aging. More specifically, the content of HA in the skin of individuals aged 75 years is less than a quarter of that measured in persons aged 19 years [
4].
Surgical techniques (e.g., injection of HA fillers), topical agents, cosmetics, and health functional foods are currently utilized for the anti-aging treatment of the skin and improvement of dry skin. Surgical techniques offer immediate results; however, they are expensive and associated with a risk of pain and swelling [
5]. Various laser and light treatments were also proposed to prevent and treat facial aging and dry skin, with variable results [
6,
7]. Topical drugs and cosmetic creams are relatively inexpensive treatment options. Nevertheless, they exert limited effects on the site of application and are occasionally linked to the occurrence of skin inflammation due to irritation caused by the preservatives and perfumes contained in the products [
8]. Although health functional foods do not have an immediate effect, they are inexpensive; moreover, continuous intake of such foods can offer lasting benefits without unwanted side effects.
It was reported that food components (e.g., collagen peptide, placenta, and HA) function to maintain normal skin conditions, such as stratum corneum water content. However, evidence from randomized, placebo-controlled trials investigating anti-wrinkle therapy did not clearly demonstrate significant improvement in wrinkles by food materials other than HA [
9,
10,
11]. Thus far, multiple skin-moisturizing or anti-wrinkle functions of oral HA ingestion have been reported. Sato et al. investigated 39 Japanese women (aged 37–59 years) with skin dryness, sagging, and wrinkles around the eyes who received HA (120 mg/day) for 6 weeks. After 3 weeks of treatment, the HA group had significantly improved corneal water content compared with the placebo group (
p < 0.05) [
12]. Oe et al. reported that the administration of HA (120 mg/day) for 12 weeks in 50 Japanese men and women (aged 22–59 years) with wrinkles around their eyes resulted in a significant reduction in wrinkle volume ratio after 8 weeks of consumption versus the placebo (
p < 0.05) [
13]. Nevertheless, thus far, no human study has comprehensively evaluated the impacts of HA ingestion on the skin, including skin hydration, skin barrier function, skin elasticity, skin structure, and facial photography. Therefore, we conducted a double-blind, randomized, placebo-controlled, parallel-group trial involving Asian men and women aged 35–64 years to evaluate the impacts of HA consumption on the skin, with a particular emphasis on multifaceted skin assessment.
2. Materials and Methods
2.1. Study Samples
The subjects received 120 mg/capsule/day of HA (Hyabest®(S)LF-P; Kewpie Corporation, Tokyo, Japan) or the placebo (dextrin; Matsutani Chemical Industry Co., Ltd., Hyogo, Japan), taken orally, for 12 consecutive weeks. The HA had 95% purity according to a high-performance liquid chromatography analysis.
2.2. Study Design and Ethical Aspects
The study followed a randomized, double-blind, and placebo-controlled design. It was conducted in compliance with the Good Clinical Practice guidelines and the applicable regulatory requirements [
14]. Written informed consent was provided by all subjects. The study was registered with the UMIN Clinical Trials Registry (UMIN000043750). In addition, the study was approved by the institutional review board of Antai Medical Care Cooperation Antai Tian-Sheng Memorial Hospital (TSMHIRB 19-021-A) and was conducted in accordance with its rules and regulations. The study protocol conformed to the principles of the Declaration of Helsinki for the use of human subjects in experimental research. The present study was conducted from May to August 2019 in Taichung, Taiwan.
Prior to testing, the volunteers were examined by a cosmetic expert for any serious skin disease or damage, particularly on the cheeks and forearms. Before the study, every volunteer was provided with a volunteer protocol. This protocol, stating the terms and conditions of the testing, was individually signed by each volunteer.
2.3. Study Participants
In total, 41 subjects were enrolled into the trial; one subject withdrew from the study for personal reasons. All subjects were aged 35–64 years and met all inclusion criteria. The inclusion criteria were as follows:
- (1)
Taiwanese male and female subjects aged 30–65 years;
- (2)
Not currently taking any HA or any other health, nutritional, herbal supplement for skin;
- (3)
Not currently under-going any medical treatment (including laser treatment, face-lift, or skin-peel);
- (4)
Not using any topical application cream for skin treatment prescribed by doctors or dermatologists (commonly used facial cleanser, toner, and moisturizer were acceptable).
The subjects were randomly assigned to either the HA or placebo group. They were instructed to maintain their habitual patterns of physical activity throughout the entire study period. All measurements were carried out in a temperature- and relative humidity-controlled room (20 ± 2 °C and 50 ± 5%, respectively).
2.4. Study Schedule
The study was conducted over a period of 12 weeks. All parameters were assessed at four observation time points: weeks 0 (baseline), 4, 8, and 12.
2.5. Skin Hydration and Barrier Function
Skin hydration was evaluated using a capacitance method (Corneometer® CM 825, Courage+Khazaka Electronic, GmbH, Cologne, Germany). The barrier function was evaluated by measuring transepidermal water loss (TEWL) using the Tewameter® TM300 (Courage+Khazaka Electronic, GmbH). At each time point, measurements were performed at three sites on the face and two sites on the body (i.e., arm and waist). Three recordings were obtained for each of these different areas and the average was calculated.
2.6. Skin Elasticity
Skin elasticity was analyzed using the Cutometer® MPA580 (Courage+Khazaka Electronic, GmbH). Skin viscoelastic properties were evaluated by suction and measurements of the consequent skin deformation. This approach measures the elasticity of the upper skin layer using negative pressure, which mechanically deforms the skin. The measurements were performed on the forehead, arm, and waist. For the assessment of body skin elasticity, the Reviscometer® RVM 600 (Courage+Khazaka Electronic, GmbH) was used on the waist. The route resonance of an acoustic wave resonance running time was analyzed, and measurements were conducted at 0°, 90°, 180°, and 360° angles on the arm and waist.
2.7. Skin Structure
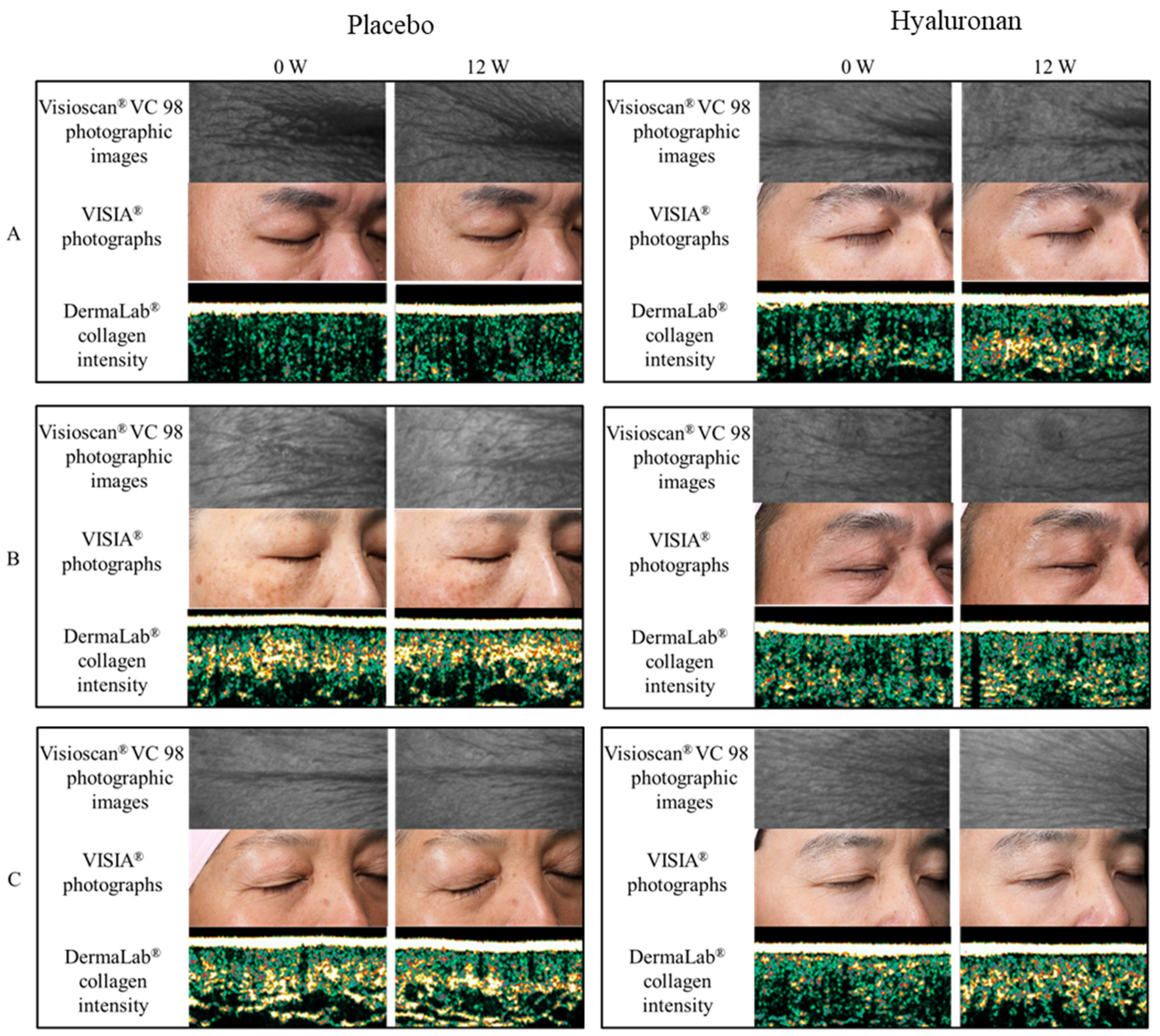
Ultrasound analysis was used to determine the thickness of the epidermis and dermis, as well as the collagen intensity score. The dermal thickness was measured using a DermaLab® (Cortex Technology, Hadsund, Denmark) ultrasound probe. Measurements were performed at the temple and waist. The skin surface analysis was carried out using the Visioscan VC98 (Courage+Khazaka Electronic, GmbH). A small area of the facial skin (at the crow feet region) was illuminated using non-harmful ultraviolet A light, and a high-resolution image was captured. The image was digitally analyzed using the surface evaluation of living skin method, which provides quantitative measurements of four parameters: roughness (SEr), scaling (SEsc), smoothness (SEsm), and wrinkling (SEw). This system also allows for the evaluation of five additional parameters, namely energy, entropy, homogeneity, variance, and contrast.
2.8. Facial Photography
Facial skin was digitally photographed, and the degree of wrinkling on the face was quantitatively analyzed using the VISIA® Evolution ver. 7.0.1 complexion analysis system (Canfield Scientific, Inc., Parsippany, NJ, USA).
2.9. Statistical Analysis
It was expected that an evaluable sample of 40 subjects would provide >80% power and an alpha of 0.05 to detect a difference between treatments in the primary outcome variable. The data were expressed as means ± standard deviation. Repeated measures analysis of variance and Dunnett’s test were used to compare the baseline value with that obtained at each measurement time point. After confirming the normal distribution of data using Levene’s test, the independent t-test was used to compare the placebo and HA groups. Statistical tests were performed with a significance level of 5%. SPSS statistics version 25.0 (IBM Corp., Armonk, NY, USA) software was used for the statistical calculations.
4. Discussion
This study revealed that oral ingestion of HA for 12 weeks significantly improved multiple parameters (e.g., skin moisturization and wrinkles) compared to the placebo. Moreover, there were no adverse events attributable to the consumption of HA. The epidermal turnover was 28 days [
15]. Therefore, it was anticipated that the efficacy could be confirmed after 4 weeks of ingestion. However, significant differences were observed between the HA and placebo groups only after 8 weeks of ingestion. In addition to the stratum corneum, dermal fibroblasts also synthesize collagen fibers, elastin fibers, and HA. In vitro, HA stimulates the proliferation of dermal fibroblasts, and HA stimulates in fibroblasts [
16,
17]. Therefore, it was assumed that 8–12 weeks of ingestion (i.e., a longer period than the epidermal turnover) was required to obtain a statistically significant anti-senescence effect.
This study was conducted on Asian men and women. However, evidence shows that there are no major differences in skin function between sexes or races. Previous studies have reported that there are no significant differences between men and women in stratum corneum water content, TEWL, or skin elasticity, which are key indicators of skin condition [
18,
19,
20,
21,
22]. Moreover, according to previous studies, there were no significant differences reported in stratum corneum water content between races [
23,
24,
25,
26]. Furthermore, investigations did not reveal significant differences in TEWL between black, white, and Hispanic subjects residing in Northern California, USA [
27]. Reportedly, there is also no difference in TEWL between Japanese and German individuals [
28]. Corneal lipid and ceramide levels were also reported to be similar in Thai and British individuals [
29]. In addition, it was shown that the size of corneocytes does not differ greatly between races [
30]. In a German study, ingestion of HA significantly improved stratum corneum moisture, elasticity, skin roughness, and wrinkle depth compared with the baseline [
31]. Collectively, these studies demonstrate that there are no differences in the effects of HA consumption across races. Therefore, it is inferred that the results of the present study can also be extrapolated in men and women of other races.
Ingested HA is degraded to 4–6 sugars by the gut microbiota and absorbed into the body to reach the skin [
32]. Enterobacteriaceae (e.g., Prevotella), which produce hyaluronidases, are widespread in the gut of Asians and Caucasians [
33,
34,
35]. Since there is a constant number of bacteria with HA-degrading capacity in the gut microbiota regardless of race, there is also no major racial difference in the absorption of HA.
The epidermis is composed of the stratum corneum, the granular layer, the stratum spinosum, and the basal layer. HA, which is required in the epidermis, is synthesized in keratinocytes of the basal layer [
36,
37]. It binds to receptors (CD44) present on the surface of keratinocytes, and normalizes skin function by signaling [
38]. It also possesses a high water retention capacity [
39]. Furthermore, owing to its skin normalization function and high water retention capacity, it is thought that HA suppresses wrinkle formation in the epidermis. In addition, it is speculated that multiple factors associated with the in vivo functions of HA are involved in the suppression of wrinkle formation. These mechanisms may have led to the improved efficacy and skin condition against wrinkles demonstrated in this study. This study has potential limitations. It was a relatively small sample size study with some indicators, such as SEms, that were not consistent with trends in other indicator results. Further studies, including mechanisms and large-scale clinical studies, are desirable. Skin condition is associated with various components, including diet, sleep, exercise, aging, hormonal balance, ultraviolet radiation, and seasonal variation. It is desirable to review HA intake and lifestyle habits as a whole for maintaining healthy skin. In the future, further investigation on the synergistic anti-aging effect of HA intake and lifestyle habits is warranted.


 ,
, 

{kind=link}