
Adherence to Ketogenic and Mediterranean Study Diets in a Crossover Trial: The Keto–Med Randomized Trial

 ,
,  ,
, 
 , and
, and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Description of the Keto–Med Trial
2.2. Modifications to the Study Design Due to COVID-19
2.3. Participants
2.4. Randomization
2.5. Dietary Intervention
2.6. Collection of Dietary Intake
2.7. Food Delivery
2.8. Measure of Adherence to Well Formulated Ketogenic Diet (WFKD) and Mediterranean-Plus Diet (Med-Plus)
2.9. Measurement of Ketone Levels
2.10. Measurement of Satisfaction and Preparedness to Follow Study Diets
2.10.1. Food Satisfaction
2.10.2. Diet Satisfaction
2.10.3. Qualitative Comments about Study Diets
2.11. Assessment of COVID-19 Related Alterations
2.12. Data Management
2.13. Statistical Analysis
3. Results
3.1. Demographics
3.2. Description of Food Delivery Meals
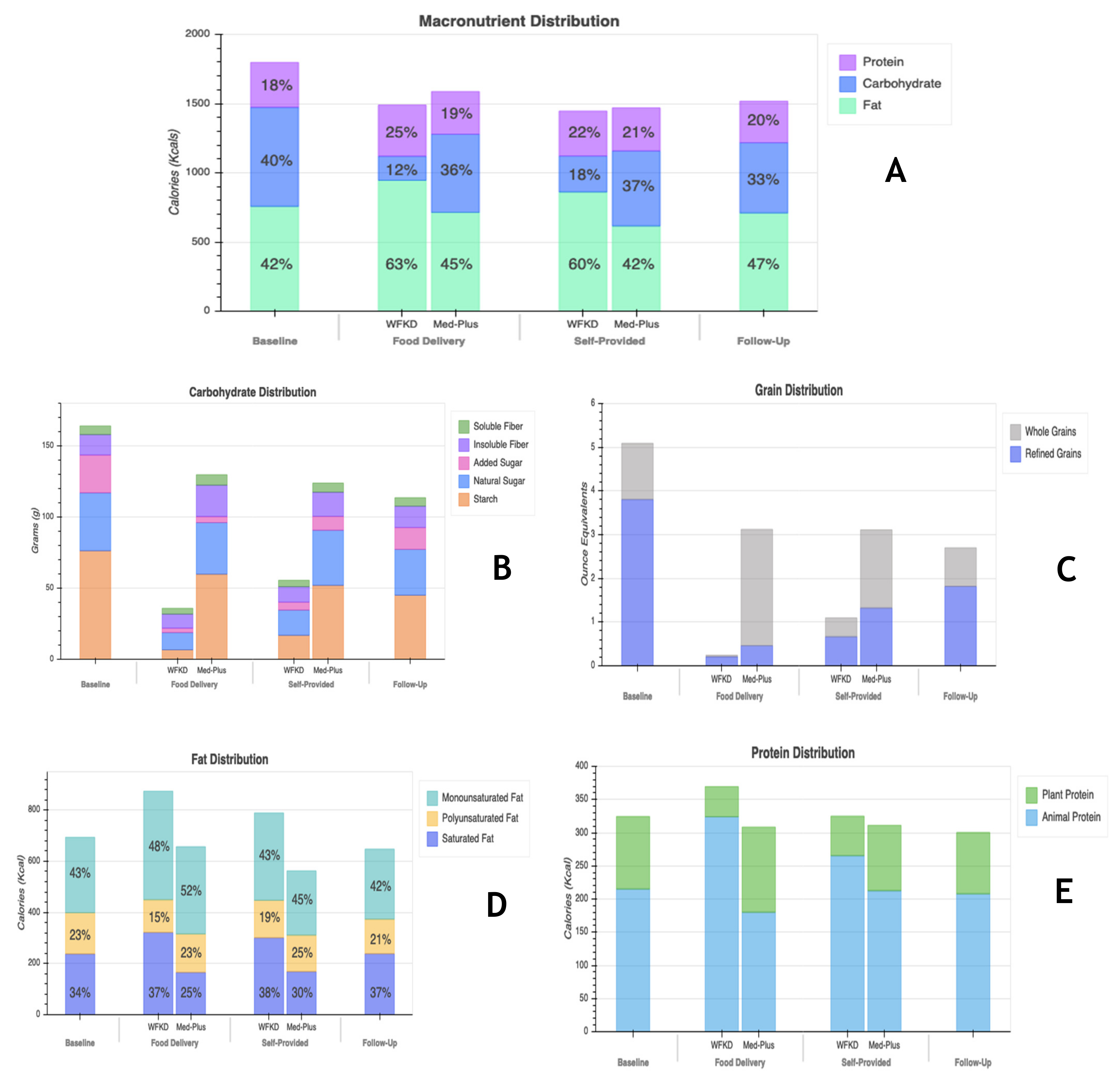
3.3. Description of Diet Composition
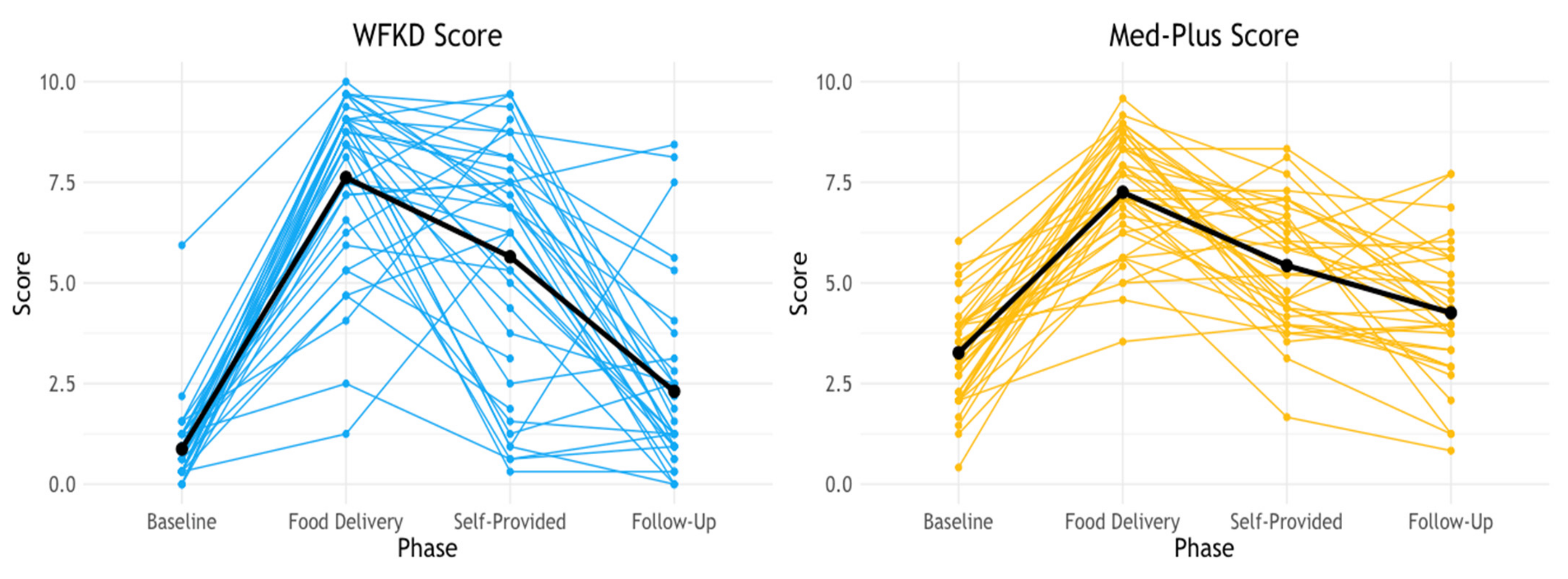
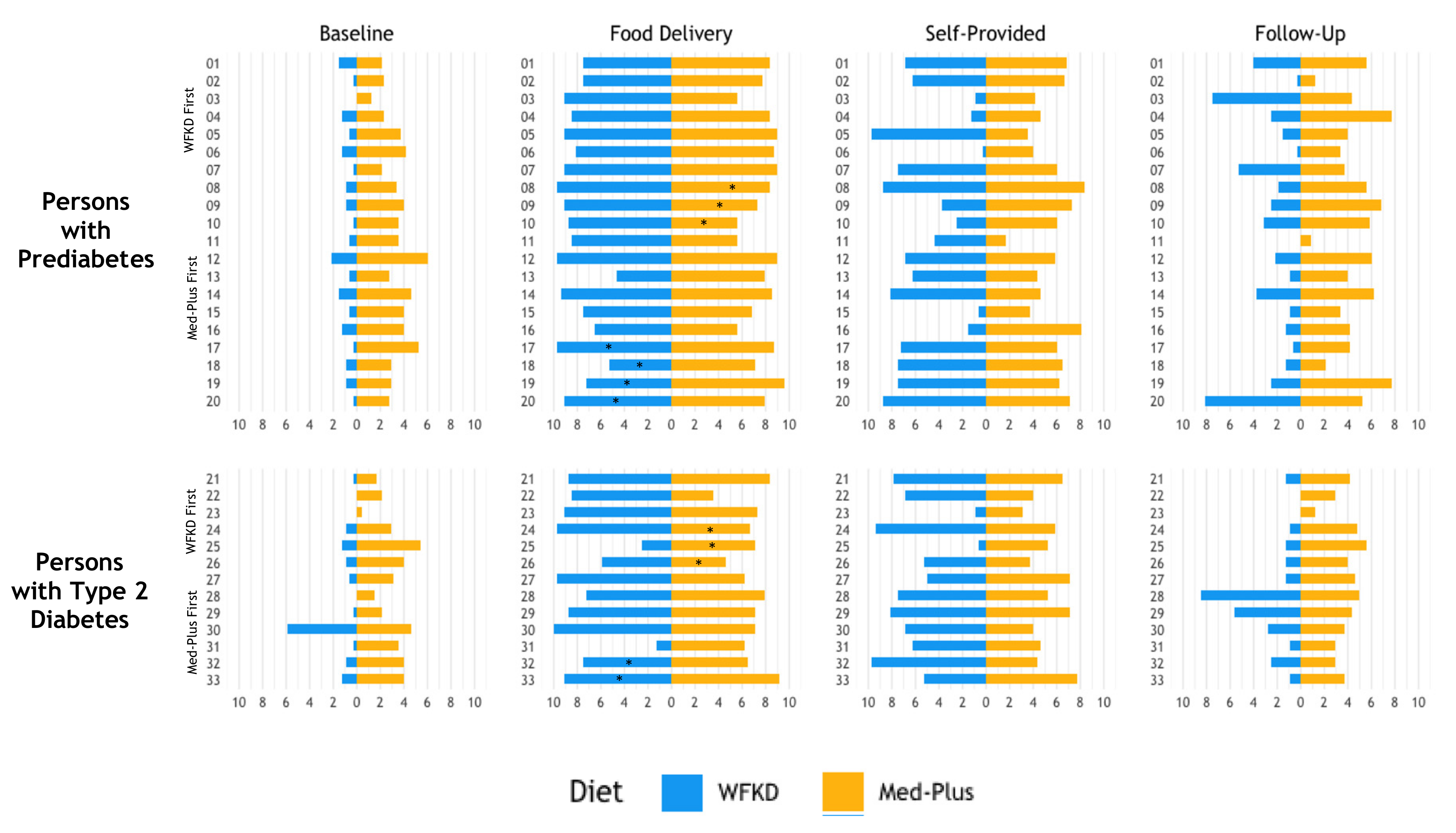
3.4. Adherence to Study Diets
3.5. Ketone Blood Levels
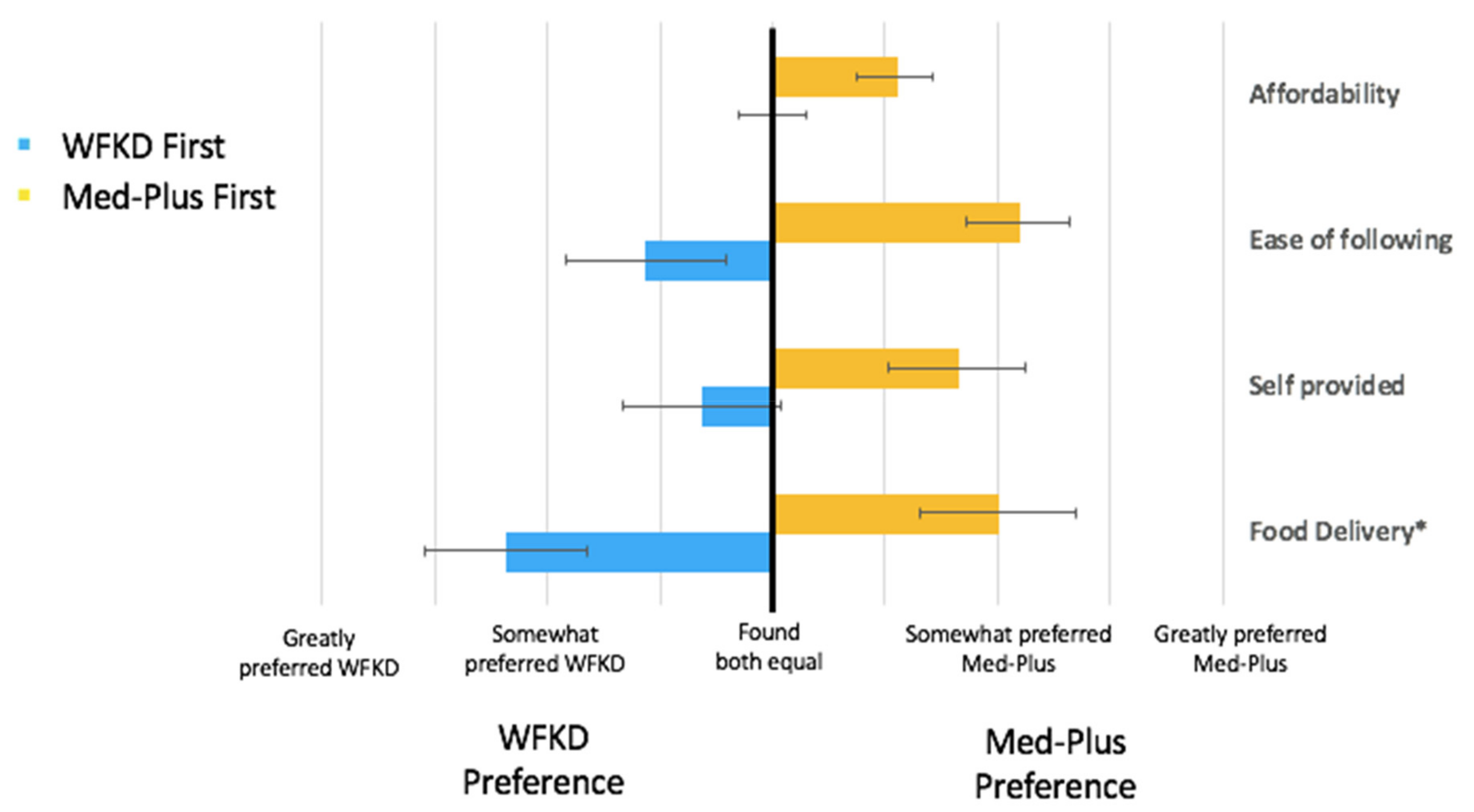
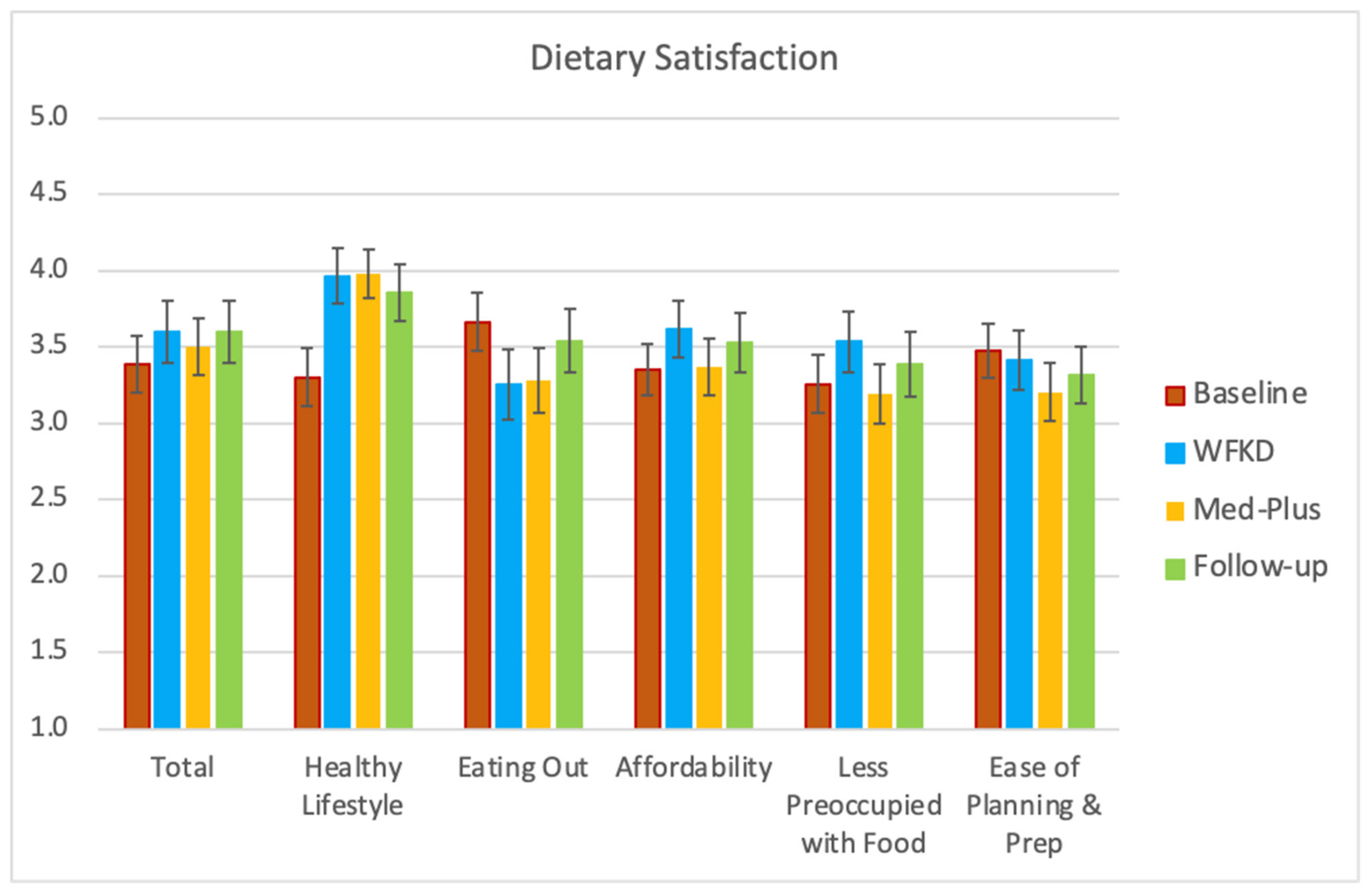
3.6. Satisfaction with Study Diets
3.7. Qualitative Comments about Study Diets
3.8. Assessment of COVID-19 Related Alterations
3.9. Adverse Events
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Centers for Disease Control and Prevention. National Diabetes Statistics Report, 2020; Centers for Disease Control and Prevention, U.S. Department of Health and Human Services: Atlanta, GA, USA, 2020. [Google Scholar]
- Evert, A.B.; Dennison, M.; Gardner, C.D.; Garvey, W.T.; Lau, K.H.K.; MacLeod, J.; Mitri, J.; Pereira, R.F.; Rawlings, K.; Robinson, S. Nutrition therapy for adults with diabetes or prediabetes: A consensus report. Diabetes Care 2019, 42, 731–754. [Google Scholar] [CrossRef] [Green Version]
- Stanley, K. Position of the Academy of Nutrition and Dietetics: The role of medical nutrition theorapy and registered dietitian nutritionists in the prevention and treatment of prediabetes and type 2 diabetes. J. Acad. Nutr. Diet 2018, 118, 343–353. [Google Scholar]
- Bantle, J.P.; Wylie-Rosett, J.; Albright, A.L.; Apovian, C.M.; Clark, N.G.; Franz, M.J.; Hoogwerf, B.J.; Lichtenstein, A.H.; Mayer-Davis, E.; Mooradian, A.D. Nutrition recommendations and interventions for diabetes: A position statement of the American Diabetes Association. Diabetes Care 2006, 29, 2140–2157. [Google Scholar] [CrossRef] [Green Version]
- Spritzler, F. A low-carbohydrate, whole-foods approach to managing diabetes and prediabetes. Diabetes Spectr. 2012, 25, 238–243. [Google Scholar] [CrossRef] [Green Version]
- Hite, A.H.; Berkowitz, V.G.; Berkowitz, K. Low-carbohydrate diet review: Shifting the paradigm. Nutr. Clin. Pract. 2011, 26, 300–308. [Google Scholar] [CrossRef] [Green Version]
- Estruch, R.; Ros, E.; Salas-Salvadó, J.; Covas, M.-I.; Corella, D.; Arós, F.; Gómez-Gracia, E.; Ruiz-Gutiérrez, V.; Fiol, M.; Lapetra, J. Primary prevention of cardiovascular disease with a Mediterranean diet. N. Engl. J. Med. 2013, 368, 1279–1290. [Google Scholar] [CrossRef] [Green Version]
- Davis, C.; Bryan, J.; Hodgson, J.; Murphy, K. Definition of the Mediterranean diet; a literature review. Nutrients 2015, 7, 9139–9153. [Google Scholar] [CrossRef]
- Kirkpatrick, C.F.; Bolick, J.P.; Kris-Etherton, P.M.; Sikand, G.; Aspry, K.E.; Soffer, D.E.; Willard, K.-E.; Maki, K.C. Review of current evidence and clinical recommendations on the effects of low-carbohydrate and very-low-carbohydrate (including ketogenic) diets for the management of body weight and other cardiometabolic risk factors: A scientific statement from the National Lipid Association Nutrition and Lifestyle Task Force. J. Clin. Lipidol. 2019, 13, 689–711. [Google Scholar] [CrossRef] [Green Version]
- Martín-Peláez, S.; Fito, M.; Castaner, O. Mediterranean Diet Effects on Type 2 Diabetes Prevention, Disease Progression, and Related Mechanisms. A Review. Nutrients 2020, 12, 2236. [Google Scholar] [CrossRef]
- Sleiman, D.; Al-Badri, M.R.; Azar, S.T. Effect of mediterranean diet in diabetes control and cardiovascular risk modification: A systematic review. Front. Public Health 2015, 3, 69. [Google Scholar] [CrossRef] [Green Version]
- Georgoulis, M.; Kontogianni, M.D.; Yiannakouris, N. Mediterranean diet and diabetes: Prevention and treatment. Nutrients 2014, 6, 1406–1423. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Westman, E.C.; Tondt, J.; Maguire, E.; Yancy, W.S., Jr. Implementing a low-carbohydrate, ketogenic diet to manage type 2 diabetes mellitus. Expert Rev. Endocrinol. Metab. 2018, 13, 263–272. [Google Scholar] [CrossRef]
- Bolla, A.M.; Caretto, A.; Laurenzi, A.; Scavini, M.; Piemonti, L. Low-carb and ketogenic diets in type 1 and type 2 diabetes. Nutrients 2019, 11, 962. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Pagoto, S.L.; Appelhans, B.M. A call for an end to the diet debates. JAMA 2013, 310, 687–688. [Google Scholar] [CrossRef] [PubMed]
- Middleton, K.R.; Anton, S.D.; Perri, M.G. Long-term adherence to health behavior change. Am. J. Lifestyle Med. 2013, 7, 395–404. [Google Scholar] [CrossRef] [Green Version]
- Gardner, C.D.; Crimarco, A.; Landry, M.J.; Fielding-Singh, P. Nutrition Study Design Issues—Important Issues for Interpretation. Am. J. Health Promot. 2020, 34, 951–954. [Google Scholar] [CrossRef]
- Gibson, A.A.; Sainsbury, A. Strategies to improve adherence to dietary weight loss interventions in research and real-world settings. Behav. Sci. 2017, 7, 44. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Alhassan, S.; Kim, S.; Bersamin, A.; King, A.; Gardner, C. Dietary adherence and weight loss success among overweight women: Results from the A TO Z weight loss study. Int. J. Obes. 2008, 32, 985–991. [Google Scholar] [CrossRef] [Green Version]
- Williamson, D.A.; Anton, S.D.; Han, H.; Champagne, C.M.; Allen, R.; LeBlanc, E.; Ryan, D.H.; McManus, K.; Laranjo, N.; Carey, V.J. Adherence is a multi-dimensional construct in the POUNDS LOST trial. J. Behav. Med. 2009, 33, 35–46. [Google Scholar] [CrossRef]
- Association, A.D. Classification and diagnosis of diabetes: Standards of Medical Care in Diabetes—2020. Diabetes Care 2020, 43, S14–S31. [Google Scholar] [CrossRef] [Green Version]
- Volek, J.S.; Phinney, S.D. The Art and Science of Low Carbohydrate Performance; Beyond Obesity LLC: Miami, FL, USA, 2012. [Google Scholar]
- Willett, W.C.; Sacks, F.; Trichopoulou, A.; Drescher, G.; Ferro-Luzzi, A.; Helsing, E.; Trichopoulos, D. Mediterranean diet pyramid: A cultural model for healthy eating. Am. J. Clin. Nutr. 1995, 61, 1402S–1406S. [Google Scholar] [CrossRef] [PubMed]
- Feskanich, D.; Sielaff, B.H.; Chong, K.; Buzzard, I.M. Computerized Collection and Analysis of Dietary Intake Information. Comput. Methods Programs Biomed. 1989, 30, 47–57. [Google Scholar] [CrossRef]
- James, B.; Loken, E.; Roe, L.; Myrissa, K.; Lawton, C.; Dye, L.; Rolls, B. Validation of the Diet Satisfaction Questionnaire: A new measure of satisfaction with diets for weight management. Obes. Sci. Pr. 2018, 4, 506–514. [Google Scholar] [CrossRef]
- Harris, P.A.; Taylor, R.; Thielke, R.; Payne, J.; Gonzalez, N.; Conde, J.G. Research electronic data capture (REDCap)—A metadata-driven methodology and workflow process for providing translational research informatics support. J. Biomed. Inform. 2009, 42, 377–381. [Google Scholar] [CrossRef] [Green Version]
- Harris, P.A.; Taylor, R.; Minor, B.L.; Elliott, V.; Fernandez, M.; O’Neal, L.; McLeod, L.; Delacqua, G.; Delacqua, F.; Kirby, J. The REDCap consortium: Building an international community of software platform partners. J. Biomed. Inform. 2019, 95, 103208. [Google Scholar] [CrossRef]
- Trichopoulou, A.; Kouris-Blazos, A.; Wahlqvist, M.L.; Gnardellis, C.; Lagiou, P.; Polychronopoulos, E.; Vassilakou, T.; Lipworth, L.; Trichopoulos, D. Diet and overall survival in elderly people. BMJ 1995, 311, 1457–1460. [Google Scholar] [CrossRef] [Green Version]
- Tobias, D.K.; Hu, F.B.; Chavarro, J.; Rosner, B.; Mozaffarian, D.; Zhang, C. Healthful dietary patterns and type 2 diabetes mellitus risk among women with a history of gestational diabetes mellitus. Arch. Intern. Med. 2012, 172, 1566–1572. [Google Scholar] [CrossRef] [Green Version]
- Stefler, D.; Malyutina, S.; Kubinova, R.; Pajak, A.; Peasey, A.; Pikhart, H.; Brunner, E.J.; Bobak, M. Mediterranean diet score and total and cardiovascular mortality in Eastern Europe: The HAPIEE study. Eur. J. Nutr. 2015, 56, 421–429. [Google Scholar] [CrossRef] [Green Version]
- Shan, Z.; Li, Y.; Baden, M.Y.; Bhupathiraju, S.N.; Wang, D.D.; Sun, Q.; Rexrode, K.M.; Rimm, E.B.; Qi, L.; Willett, W.C. Association between healthy eating patterns and risk of cardiovascular disease. JAMA Intern. Med. 2020, 180, 1090. [Google Scholar] [CrossRef] [PubMed]
- Bach, A.; Serra-Majem, L.; Carrasco, J.L.; Roman, B.; Ngo, J.; Bertomeu, I.; Obrador, B. The use of indexes evaluating the adherence to the Mediterranean diet in epidemiological studies: A review. Public Health Nutr. 2006, 9, 132–146. [Google Scholar] [CrossRef]
- Sotos-Prieto, M.; Moreno-Franco, B.; Ordovás, J.M.; León, M.; Casasnovas, J.A.; Peñalvo, J.L. Design and development of an instrument to measure overall lifestyle habits for epidemiological research: The Mediterranean Lifestyle (MEDLIFE) index. Public Health Nutr. 2014, 18, 959–967. [Google Scholar] [CrossRef] [PubMed]
- Retterstøl, K.; Svendsen, M.; Narverud, I.; Holven, K.B. Effect of low carbohydrate high fat diet on LDL cholesterol and gene expression in normal-weight, young adults: A randomized controlled study. Atherosclerosis 2018, 279, 52–61. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- McKenzie, A.L.; Hallberg, S.J.; Creighton, B.C.; Volk, B.M.; Link, T.M.; Abner, M.K.; Glon, R.M.; McCarter, J.P.; Volek, J.S.; Phinney, S.D. A novel intervention including individualized nutritional recommendations reduces hemoglobin A1c level, medication use, and weight in type 2 diabetes. JMIR Diabetes 2017, 2, e5. [Google Scholar] [CrossRef]
- Brinkworth, G.D.; Noakes, M.; Buckley, J.D.; Keogh, J.B.; Clifton, P.M. Long-term effects of a very-low-carbohydrate weight loss diet compared with an isocaloric low-fat diet after 12 mo. Am. J. Clin. Nutr. 2009, 90, 23–32. [Google Scholar] [CrossRef] [Green Version]
- Brehm, B.J.; Seeley, R.J.; Daniels, S.R.; D’Alessio, D.A. A randomized trial comparing a very low carbohydrate diet and a calorie-restricted low fat diet on body weight and cardiovascular risk factors in healthy women. J. Clin. Endocrinol. Metab. 2003, 88, 1617–1623. [Google Scholar] [CrossRef] [Green Version]
- Albanese, A.; Prevedello, L.; Markovich, M.; Busetto, L.; Vettor, R.; Foletto, M. Pre-operative very low calorie ketogenic diet (VLCKD) vs. very low calorie diet (VLCD): Surgical impact. Obes. Surg. 2018, 29, 292–296. [Google Scholar] [CrossRef] [PubMed]
- Dashti, H.M.; Mathew, T.C.; Khadada, M.; Al-Mousawi, M.; Talib, H.; Asfar, S.K.; Behbahani, A.I.; Al-Zaid, N.S. Beneficial effects of ketogenic diet in obese diabetic subjects. Mol. Cell. Biochem. 2007, 302, 249–256. [Google Scholar] [CrossRef]
- Hussain, T.A.; Mathew, T.C.; Dashti, A.A.; Asfar, S.; Al-Zaid, N.; Dashti, H.M. Effect of low-calorie versus low-carbohydrate ketogenic diet in type 2 diabetes. Nutrition 2012, 28, 1016–1021. [Google Scholar] [CrossRef]
- Hallberg, S.J.; McKenzie, A.L.; Williams, P.T.; Bhanpuri, N.H.; Peters, A.L.; Campbell, W.W.; Hazbun, T.L.; Volk, B.M.; McCarter, J.P.; Phinney, S.D. Effectiveness and safety of a novel care model for the management of type 2 diabetes at 1 year: An open-label, non-randomized, controlled study. Diabetes Ther. 2018, 9, 583–612. [Google Scholar] [CrossRef] [Green Version]
- De Lorgeril, M.; Renaud, S.; Salen, P.; Monjaud, I.; Mamelle, N.; Martin, J.; Guidollet, J.; Touboul, P.; Delaye, J. Mediterranean alpha-linolenic acid-rich diet in secondary prevention of coronary heart disease. Lancet 1994, 343, 1454–1459. [Google Scholar] [CrossRef]
- de Lorgeril, M.; Salen, P.; Martin, J.-L.; Monjaud, I.; Delaye, J.; Mamelle, N. Mediterranean diet, traditional risk factors, and the rate of cardiovascular complications after myocardial infarction: Final report of the Lyon Diet Heart Study. Circulation 1999, 99, 779–785. [Google Scholar] [CrossRef]
- Salas-Salvadó, J.; Bulló, M.; Estruch, R.; Ros, E.; Covas, M.-I.; Ibarrola-Jurado, N.; Corella, D.; Arós, F.; Gómez-Gracia, E.; Ruiz-Gutiérrez, V. Prevention of diabetes with Mediterranean diets: A subgroup analysis of a randomized trial. Ann. Intern. Med. 2014, 160, 1–10. [Google Scholar] [CrossRef] [Green Version]
- Estruch, R.; Ros, E.; Salas-Salvadó, J.; Covas, M.-I.; Corella, D.; Arós, F.; Gómez-Gracia, E.; Ruiz-Gutiérrez, V.; Fiol, M.; Lapetra, J. Primary prevention of cardiovascular disease with a Mediterranean diet supplemented with extra-virgin olive oil or nuts. N. Engl. J. Med. 2018, 378, e34. [Google Scholar] [CrossRef] [PubMed]
- Yubero-Serrano, E.M.; Fernandez-Gandara, C.; Garcia-Rios, A.; Rangel-Zuñiga, O.A.; Gutierrez-Mariscal, F.M.; Torres-Peña, J.D.; Marin, C.; Lopez-Moreno, J.; Castaño, J.P.; Delgado-Lista, J. Mediterranean diet and endothelial function in patients with coronary heart disease: An analysis of the CORDIOPREV randomized controlled trial. PLoS Med. 2020, 17, e1003282. [Google Scholar] [CrossRef]
- Saslow, L.R.; Mason, A.E.; Kim, S.; Goldman, V.; Ploutz-Snyder, R.; Bayandorian, H.; Daubenmier, J.; Hecht, F.M.; Moskowitz, J.T. An online intervention comparing a very low-carbohydrate ketogenic diet and lifestyle recommendations versus a plate method diet in overweight individuals with type 2 diabetes: A randomized controlled trial. J. Med. Internet Res. 2017, 19, e36. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Saslow, L.R.; Kim, S.; Daubenmier, J.J.; Moskowitz, J.T.; Phinney, S.D.; Goldman, V.; Murphy, E.J.; Cox, R.M.; Moran, P.; Hecht, F.M. A randomized pilot trial of a moderate carbohydrate diet compared to a very low carbohydrate diet in overweight or obese individuals with type 2 diabetes mellitus or prediabetes. PLoS ONE 2014, 9, e91027. [Google Scholar] [CrossRef] [Green Version]
- Tay, J.; Luscombe-Marsh, N.D.; Thompson, C.H.; Noakes, M.; Buckley, J.D.; Wittert, G.A.; Yancy, W.S., Jr.; Brinkworth, G.D. Comparison of low-and high-carbohydrate diets for type 2 diabetes management: A randomized trial. Am. J. Clin. Nutr. 2015, 102, 780–790. [Google Scholar] [CrossRef] [PubMed]
- Westman, E.C.; Yancy, W.S.; Mavropoulos, J.C.; Marquart, M.; McDuffie, J.R. The effect of a low-carbohydrate, ketogenic diet versus a low-glycemic index diet on glycemic control in type 2 diabetes mellitus. Nutr. Metab. 2008, 5, 36. [Google Scholar] [CrossRef] [Green Version]
- Shai, I.; Schwarzfuchs, D.; Henkin, Y.; Shahar, D.R.; Witkow, S.; Greenberg, I.; Golan, R.; Fraser, D.; Bolotin, A.; Vardi, H. Weight loss with a low-carbohydrate, Mediterranean, or low-fat diet. N. Engl. J. Med. 2008, 359, 229–241. [Google Scholar] [CrossRef] [Green Version]
- Greenberg, I.; Stampfer, M.J.; Schwarzfuchs, D.; Shai, I.; Group, D. Adherence and success in long-term weight loss diets: The dietary intervention randomized controlled trial (DIRECT). J. Am. Coll. Nutr. 2009, 28, 159–168. [Google Scholar] [CrossRef]
- Hall, K.D.; Ayuketah, A.; Brychta, R.; Cai, H.; Cassimatis, T.; Chen, K.Y.; Chung, S.T.; Costa, E.; Courville, A.; Darcey, V. Ultra-processed diets cause excess calorie intake and weight gain: An inpatient randomized controlled trial of ad libitum food intake. Cell Metab. 2019, 30, 67–77.e63. [Google Scholar] [CrossRef] [Green Version]
- Hall, K.D.; Chen, K.Y.; Guo, J.; Lam, Y.Y.; Leibel, R.L.; Mayer, L.E.; Reitman, M.L.; Rosenbaum, M.; Smith, S.R.; Walsh, B.T. Energy expenditure and body composition changes after an isocaloric ketogenic diet in overweight and obese men. Am. J. Clin. Nutr. 2016, 104, 324–333. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hall, K.D.; Guo, J.; Courville, A.B.; Boring, J.; Brychta, R.; Chen, K.Y.; Darcey, V.; Forde, C.G.; Gharib, A.M.; Gallagher, I. Effect of a plant-based, low-fat diet versus an animal-based, ketogenic diet on ad libitum energy intake. Nat. Med. 2021, 27, 344–353. [Google Scholar] [CrossRef]
- Perez-Cueto, F.J. An umbrella review of systematic reviews on food choice and nutrition published between 2017 and-2019. Nutrients 2019, 11, 2398. [Google Scholar] [CrossRef] [Green Version]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Carbohydrate Sources | Keto | Med |
|---|---|---|
| Similar | ||
| Added sugars | Avoid | Avoid |
| Refined grains | Avoid | Avoid |
| Nonstarchy vegetables | Include | Include |
| Different | ||
| Legumes | Avoid | Include |
| Fruits | Avoid | Include |
| Whole grains | Avoid | Include |
| Keto–Med (n = 20) | Med–Keto (n = 20) | All (n = 40) | |
|---|---|---|---|
| Gender, n | |||
| Male | 9 | 9 | 18 |
| Female | 11 | 11 | 22 |
| Diagnosis, n | |||
| Prediabetes | 10 | 11 | 21 |
| Type 2 Diabetes Mellitus | 10 | 9 | 19 |
| Age, year | 57.8 ± 9.2 | 59.6 ± 8.8 | 58.7 ± 9.1 |
| Highest level of education achieved, n | |||
| High school graduate | 1 | 2 | 3 |
| Some college | 2 | 2 | 4 |
| College degree | 6 | 6 | 12 |
| Some postgraduate school | 3 | 2 | 5 |
| Postgraduate degree | 8 | 8 | 16 |
| Race/ethnicity, n | |||
| Non-Hispanic White | 11 | 8 | 19 |
| Hispanic/Latinx | 2 | 5 | 7 |
| Asian | 6 | 5 | 11 |
| Black/African American | 0 | 1 | 1 |
| Native Hawaiian/Pacific Islander | 1 | 1 | 2 |
| Weight, kg | |||
| Male | 87.3 ± 12.1 | 88.5 ± 17.4 | 87.9 ± 14.1 |
| Female | 92.8 ± 13.3 | 85.0 ± 16.6 | 88.9 ± 14.8 |
| Both sexes | 90.3 ± 12.7 | 86.6 ± 16.6 | 88.4 ± 14.5 |
| Body Mass Index (kg/m2) | |||
| Male | 28.1 ± 3.5 | 29.6 ± 4.6 | 28.9 ± 3.9 |
| Female | 33.7 ± 3.5 | 32.2 ± 5.6 | 33.0 ± 3.5 |
| Both sexes | 31.2 ± 4.4 | 31.1 ± 5.2 | 31.1 ± 4.7 |
| Blood pressure, mmHg | |||
| Systolic | 122.6 ± 11.3 | 123.1 ± 13.9 | 122.8 ± 12.4 |
| Diastolic | 76.0 ± 10.0 | 74.5 ± 8.3 | 75.2 ± 9.0 |
| Blood lipids, mg/dL | |||
| HDL cholesterol | 48 ± 11 | 46 ± 10 | 47 ± 10 |
| LDL cholesterol | 100 ± 31 | 107 ± 34 | 104 ± 32 |
| Triglycerides | 150 ± 97 | 132 ± 65 | 141 ± 81 |
| Fasting glucose, mg/dL | |||
| Persons with prediabetes | 111.2 ± 6.4 | 103.4 ± 12.0 | 107.1 ± 10.5 |
| Persons with Type 2 Diabetes Mellitus | 138.4 ± 26.1 | 143.8 ± 31.3 | 140.9 ± 28.8 |
| Fasting insulin, µIU/mL | |||
| Persons with prediabetes | 21.6 ± 14.4 | 21.5 ± 14.5 | 21.6 ± 14.4 |
| Persons with Type 2 Diabetes Mellitus | 20.9 ± 9.3 | 12.4 ± 4.4 | 16.9 ± 8.5 |
| HbA1c levels, % | |||
| Persons with prediabetes | 5.8 ± 0.3 | 5.8 ± 0.3 | 5.8 ± 0.3 |
| Persons with Type 2 Diabetes Mellitus | 7.0 ± 0.7 | 6.9 ± 0.8 | 6.9 ± 0.8 |
| Alanine aminotransferase (ALT), IU/L | 29 ± 13 | 27 ± 12 | 28 ± 12 |
| Kcals | % Fat | % Carbohydrates | % Protein | % Alcohol | |
|---|---|---|---|---|---|
| As Designed1 | |||||
| WFKD | 2796 | 69 | 7 | 24 | -- |
| Med-Plus | 2784 | 48 | 36 | 16 | -- |
| As Delivered2 | |||||
| WFKD | 2816 | 66 | 5 | 29 | -- |
| Med-Plus | 2952 | 46 | 38 | 16 | -- |
| As Consumed3 | |||||
| WFKD | 1479 ± 420 | 63 ± 7.5 | 10 ± 4.5 | 25 ± 6.5 | 2 ± 3.1 |
| Med-Plus | 1562 ± 399 | 45 ± 6.9 | 34 ± 8.8 | 19 ± 6.3 | 2 ± 3.5 |
| Timepoint | Well Formulated Ketogenic Diet | Mediterranean Plus | Between Diet p-Value 1 | ||
|---|---|---|---|---|---|
| Mean ± SD | Range | Mean ± SD | Range | ||
| Food Delivery | 7.6 ± 2.1 | 1.2–10.0 | 7.3 ± 1.5 | 3.5–9.6 | 0.333 |
| Self-Provided Food | 5.7 ± 3.0 | 0.3–9.7 | 5.4 ± 1.5 | 1.7–8.3 | 0.641 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Landry, M.J.; Crimarco, A.; Perelman, D.; Durand, L.R.; Petlura, C.; Aronica, L.; Robinson, J.L.; Kim, S.H.; Gardner, C.D. Adherence to Ketogenic and Mediterranean Study Diets in a Crossover Trial: The Keto–Med Randomized Trial. Nutrients 2021, 13, 967. https://doi.org/10.3390/nu13030967
Landry MJ, Crimarco A, Perelman D, Durand LR, Petlura C, Aronica L, Robinson JL, Kim SH, Gardner CD. Adherence to Ketogenic and Mediterranean Study Diets in a Crossover Trial: The Keto–Med Randomized Trial. Nutrients. 2021; 13(3):967. https://doi.org/10.3390/nu13030967
Chicago/Turabian StyleLandry, Matthew J., Anthony Crimarco, Dalia Perelman, Lindsay R. Durand, Christina Petlura, Lucia Aronica, Jennifer L. Robinson, Sun H. Kim, and Christopher D. Gardner. 2021. "Adherence to Ketogenic and Mediterranean Study Diets in a Crossover Trial: The Keto–Med Randomized Trial" Nutrients 13, no. 3: 967. https://doi.org/10.3390/nu13030967