Calorie-Restricted Mediterranean and Low-Fat Diets Affect Fatty Acid Status in Individuals with Nonalcoholic Fatty Liver Disease

 , ,
, ,
Abstract
:1. Introduction
2. Materials and Methods
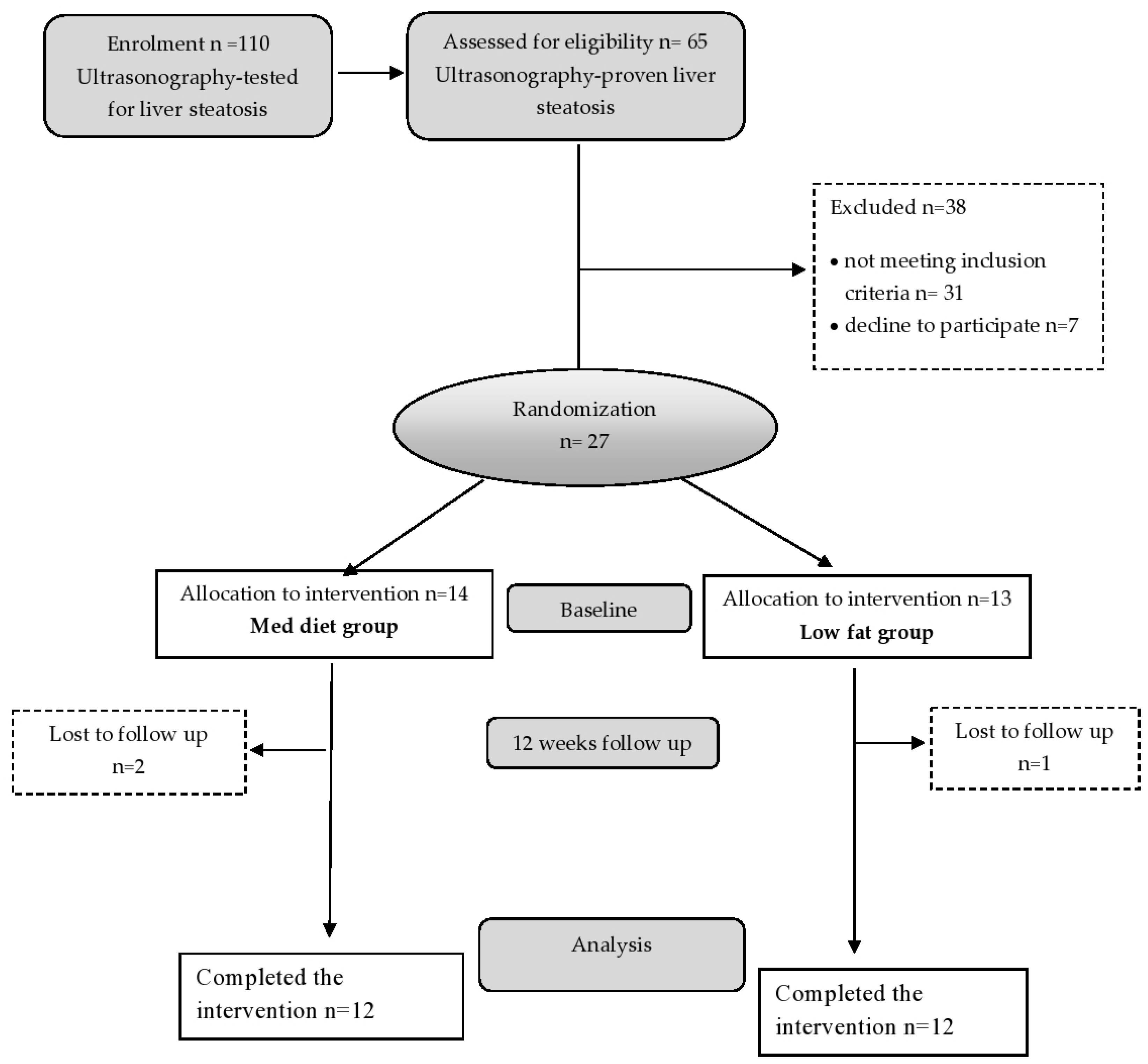
2.1. Study Participants
2.2. Study Design
2.3. Biochemical Analysis
2.4. Anthropometric Parameters and Calculated Indexes
2.5. Fatty Acid Analysis
2.6. Sample Size Calculation
2.7. Statistical Analysis
3. Results
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Portillo-Sanchez, P.; Cusi, K. Treatment of nonalcoholic fatty liver disease (NAFLD) in patients with type 2 diabetes mellitus. Clin. Diabetes Endocrinol. 2016, 2, 1–9. [Google Scholar] [CrossRef] [Green Version]
- Chalasani, N.; Younossi, Z.; Lavine, J.E.; Charlton, M.; Cusi, K.; Rinella, M.; Harrison, S.A.; Brunt, E.M.; Sanyal, A.J. The diagnosis and management of nonalcoholic fatty liver disease: Practice guidance from the American association for the study of liver diseases. Hepatology 2018, 67, 328–357. [Google Scholar] [CrossRef] [PubMed]
- Pan, J.J.; Fallon, M.B. Gender and racial differences in nonalcoholic fatty liver disease. World J. Hepatol. 2014, 6, 274–283. [Google Scholar] [CrossRef] [PubMed]
- Kawano, Y.; Cohen, D.E. Mechanisms of hepatic triglyceride accumulation in non-alcoholic fatty liver disease. J. Gastroenterol. 2013, 48, 434–441. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sporea, I.; Popescu, A.; Dumitrașcu, D.; Brisc, C.; Nedelcu, L.; Trifan, A.; Gheorghe, L.; Fierbințeanu Braticevici, C. Nonalcoholic fatty liver disease: Status quo. J. Gastrointestin. Liver. Dis. 2018, 27, 439–448. [Google Scholar] [CrossRef]
- Trovato, F.M.; Catalano, D.; Martines, G.F.; Pace, P.; Trovato, G.M. Mediterranean diet and non-alcoholic fatty liver disease: The need of extended and comprehensive interventions. Clin. Nutr. 2015, 34, 86–88. [Google Scholar] [CrossRef]
- Promrat, K.; Kleiner, D.E.; Niemeier, H.M.; Jackvony, E.; Kearns, M.; Wands, J.R.; Fava, J.L.; Wing, R.R. Randomized controlled trial testing the effects of weight loss on nonalcoholic steatohepatitis. Hepatology 2010, 51, 121–129. [Google Scholar] [CrossRef]
- Sorrentino, G.; Crispino, P.; Coppola, D.; De Stefano, G. Efficacy of lifestyle changes in subjects with non-alcoholic liver steatosis and metabolic syndrome may be improved with an antioxidant nutraceutical: A controlled clinical study. Drugs RD 2015, 15, 21–25. [Google Scholar] [CrossRef] [Green Version]
- Marchesini, G.; Petta, S.; Dalle Grave, R. Diet, weight loss, and liver health in nonalcoholic fatty liver disease: Pathophysiology, evidence, and practice. Hepatology 2016, 63, 2032–2043. [Google Scholar] [CrossRef]
- Plaz Torres, M.; Aghemo, A.; Lleo, A.; Bodini, G.; Furnari, M.; Marabotto, E.; Miele, L.; Giannini, E. Mediterranean diet and NAFLD: What we know and questions that still need to be answered. Nutrients 2019, 11, 2971. [Google Scholar] [CrossRef] [Green Version]
- Abenavoli, L.; Milic, N.; Peta, V.; Alfieri, F.; De Lorenzo, A.; Bellentani, S. Alimentary regimen in non-alcoholic fatty liver disease: Mediterranean diet. World J. Gastroenterol. 2014, 20, 16831–16840. [Google Scholar] [CrossRef] [PubMed]
- Ferramosca, A.; Zara, V. Modulation of hepatic steatosis by dietary fatty acids. World J. Gastroenterol. 2014, 20, 1746–1755. [Google Scholar] [CrossRef]
- Tetri, L.H.; Basaranoglu, M.; Brunt, E.M.; Yerian, L.M.; Neuschwander-Tetri, B.A. Severe NAFLD with hepatic necroinflammatory changes in mice fed trans fats and a high fructose corn syrup equivalent. Am. J. Physiol. Gastrointest. Liver Physiol. 2008, 295, 987–995. [Google Scholar] [CrossRef]
- Di Minno, M.N.; Russolillo, A.; Lupoli, R.; Ambrosino, P.; Di Minno, A.; Tarantino, G. Omega-3 fatty acids for the treatment of non-alcoholic fatty liver disease. World J. Gastroenterol. 2012, 18, 5839–5847. [Google Scholar] [CrossRef]
- López-Bautista, F.; Barbero-Becerra, V.J.; Ríos, M.Y.; Ramírez-Cisneros, M.Á.; Sánchez-Pérez, C.A.; Ramos-Ostos, M.H.; Uribe, M.; Chávez-Tapia, N.C.; Juárez-Hernández, E. Dietary consumption and serum pattern of bioactive fatty acids in NAFLD patients. Annals Hepatol. 2020, 19, 482–488. [Google Scholar] [CrossRef] [PubMed]
- Elizondo, A.; Araya, J.; Rodrigo, R.; Signorini, C.; Sgherri, C.; Comporti, M.; Poniachik, J.; Videla, L.A. Effects of weight loss on liver and erythrocyte polyunsaturated fatty acid pattern and oxidative stress status in obese patients with non-alcoholic fatty liver disease. Biol. Res. 2008, 41, 59–68. [Google Scholar] [CrossRef]
- Guo, X.; Yang, B.; Tang, J.; Li, D. Fatty acid and non-alcoholic fatty liver disease: Meta-analyses of case-control and randomized controlled trials. Clin. Nutr. 2018, 37, 113–122. [Google Scholar] [CrossRef]
- Vernon, G.; Baranova, A.; Younossi, Z.M. Systematic review: The epidemiology and natural history of non-alcoholic fatty liver disease and nonalcoholic steatohepatitis in adults. Aliment. Pharmacol. Ther. 2011, 34, 274–285. [Google Scholar] [CrossRef] [PubMed]
- Trumbo, P.; Schlicker, S.; Yates, A.A.; Poos, M. Dietary reference intakes for energy, carbohydrate, fiber, fat, fatty acids, cholesterol, protein and amino acids. J. Am. Diet. Assoc. 2002, 102, 1621. [Google Scholar] [CrossRef]
- Amato, M.C.; Giordano, C.; Galia, M.; Criscimanna, A.; Vitabile, S.; Midiri, M.; Galluzzo, A. Visceral adiposity index: A reliable indicator of visceral fat function associated with cardiometabolic risk. Diabetes Care 2010, 4, 920–922. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Keskinler, V.M.; Mutlu, H.; Sirin, A.; Senates, E.B.; Colak, Y.; Tuncer, I.; Oguz, A. Visceral adiposity index as a practical tool in patients with biopsy-proven nonalcoholic fatty liver disease/nonalcoholic steatohepatitis. Metab. Syndr. Relat. Disord. 2020, 1–6. [Google Scholar] [CrossRef] [PubMed]
- Gastaldelli, A.; Kozakova, M.; Hojlund, K.; Flyvbjerg, A.; Favuzzi, A.; Mitrakou, A.; Balkau, B. The RISC investigators. Fatty liver is associated with insulin resistance, risk of coronary heart disease, and early atherosclerosis in a large European population. Hepatology 2009, 49, 1537–1544. [Google Scholar] [CrossRef] [PubMed]
- Lee, J.H.; Kim, D.; Kim, H.J.; Lee, C.H.; Yang, J.I.; Kim, W.; Kim, Y.J.; Yoon, J.-H.; Cho, S.-H.; Sung, M.-W.; et al. Hepatic steatosis index: A simple screening tool reflecting nonalcoholic fatty liver disease. Dig. Liver. Dis. 2010, 42, 503–508. [Google Scholar] [CrossRef] [PubMed]
- Bedogni, G.; Kahn, H.S.; Bellentani, S.; Tiribelli, C. A simple index of lipid over accumulation is a good marker of liver steatosis. BMC Gastroenterol. 2010, 10, 98. [Google Scholar] [CrossRef] [Green Version]
- Ristić-Medić, D.; Ristić, V.; Tepšić, V.; Ranić, M.; Ristić, G.; Vrbaški, S.; Estelecki, I. Effect of soybean Leci-Vita product on serum lipids and fatty acid composition in patients with elevated serum cholesterol and triglyceride levels. Nutr. Res. 2003, 23, 465–477. [Google Scholar] [CrossRef]
- Musso, G.; Cassader, M.; Rosina, F.; Gambino, R. Impact of current treatments on liver disease, glucose metabolism and cardiovascular risk in nonalcoholic fatty liver disease (NAFLD): Systematic review and meta-analysis of randomised trials. Diabetologia 2012, 55, 885–904. [Google Scholar] [CrossRef] [PubMed]
- Abenavoli, L.; Greco, M.; Milic, N.; Accattato, F.; Foti, D.; Gulletta, E.; Luzza, F. Effect of Mediterranean diet and antioxidant formulation in non-alcoholic fatty liver disease: A randomized study. Nutrients 2017, 9, 870. [Google Scholar] [CrossRef]
- Goldberg, I.J.; Ginsberg, H.N. Ins and outs modulating hepatic triglyceride and development of nonalcoholic fatty liver disease. Gastroenterology 2006, 130, 1343–1346. [Google Scholar] [CrossRef]
- Fabbrini, E.; Mohammed, B.S.; Magkos, F.; Korenblat, K.M.; Patterson, B.W.; Klein, S. Alterations in adipose tissue and hepatic lipid kinetics in obese men and women with nonalcoholic fatty liver disease. Gastroenterology 2008, 134, 424–431. [Google Scholar] [CrossRef] [Green Version]
- Min, H.K.; Kapoor, A.; Fuchs, M.; Mirshahi, F.; Zhou, H.; Maher, J.; Kellum, J.; Warnick, R.; Contos, M.J.; Sanyal, A.J. Increased hepatic synthesis and dysregulation of cholesterol metabolism is associated with the severity of nonalcoholic fatty liver disease. Cell Metab. 2012, 15, 665–674. [Google Scholar] [CrossRef] [Green Version]
- Trojak, A.; Waluś-Miarka, M.; Woźniakiewicz, E.; Małecki, M.T.; Idzior-Waluś, B. Nonalcoholic fatty liver disease is associated with low HDL cholesterol and coronary angioplasty in patients with type 2 diabetes. Med. Sci. Monit. 2013, 19, 1167–1172. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- DeFilippis, A.P.; Blaha, M.J.; Martin, S.S.; Reed, R.M.; Jones, S.R.; Nasir, K.; Blumenthal, R.S.; Budoff, M.J. Nonalcoholic fatty liver disease and serum lipoproteins: The multi-ethnic study of atherosclerosis. Atherosclerosis 2013, 227, 429–436. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sofi, F.; Casini, A. Mediterranean diet and non-alcoholic fatty liver disease: New therapeutic option around the corner? World J. Gastroenterol. 2014, 20, 7339–7346. [Google Scholar] [CrossRef] [PubMed]
- Finelli, C.; Tarantino, G. Is there any consensus as to what diet or lifestyle approach is the right one for NAFLD patients? J. Gastrointestin. Liver Dis. 2012, 21, 293–302. [Google Scholar] [PubMed]
- Velasco, N.; Contreras, A.; Grassi, B. The mediterranean diet, hepatic steatosis and nonalcoholic fatty liver disease. Curr. Opin. Clin. Nutr. Metab. Care. 2014, 17, 45–57. [Google Scholar] [CrossRef] [PubMed]
- Ryan, M.C.; Itsiopoulos, C.; Thodis, T.; Ward, G.; Trost, N.; Hofferberth, S.; O’Dea, K.; Desmond, P.V.; Johnson, N.A.; Wilson, A.M. The Mediterranean diet improves hepatic steatosis and insulin sensitivity in individuals with non-alcoholic fatty liver disease. J. Hepatol. 2013, 59, 138–143. [Google Scholar] [CrossRef] [PubMed]
- Abenavoli, L.; Milic, N.; Di Renzo, L.; Preveden, T.; Medić-Stojanoska, M.; De Lorenzo, A. Metabolic aspects of adult patients with nonalcoholic fatty liver disease. World J. Gastroenterol. 2016, 22, 7006–7016. [Google Scholar] [CrossRef]
- Gentile, C.L.; Pagliassotti, M.J. The role of fatty acids in the development and progression of nonalcoholic fatty liver disease. J. Nut. Biochem. 2008, 19, 567–576. [Google Scholar] [CrossRef] [Green Version]
- Wang, X.; Cao, Y.; Fu, Y.; Guo, G.; Zhang, H. Liver fatty acid composition in mice with or without nonalcoholic fatty liver disease. Lipids Health Dis. 2011, 10, 234. [Google Scholar] [CrossRef] [Green Version]
- Araya, J.; Rodrigo, R.; Videla, L.A.; Thielemann, L.; Orellana, M.; Pettinelli, P.; Poniachik, J. Increase in long-chain polyunsaturated fatty acid n-6/n-3 ratio in relation to hepatic steatosis in patients with non-alcoholic fatty liver disease. Clin. Sci. 2004, 106, 635–643. [Google Scholar] [CrossRef] [Green Version]
- Juarez-Hernandez, E.; Chavez-Tapial, N.C.; Uribe, M.; Barbero-Becerra, V.J. Role of bioactive fatty acids in nonalcoholic fatty liver disease. Nutr. J. 2016, 15, 72–81. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hwang, J.; Chang, Y.H.; Park, J.H.; Kim, S.Y.; Chung, H.; Shim, E.; Hwang, H.J. Dietary saturated and monounsaturated fats protect against acute acetaminophen hepatotoxicity by altering fatty acid composition of liver microsomal membrane in rats. Lipids Health Dis. 2011, 10, 184. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bhattacharjee, B.; Pal, P.; Chattopadhyay, A.; Bandyopadhyay, D. Oleic acid protects against cadmium induced cardiac and hepatic tissue injury in male Wistar rats: A mechanistic study. Life Sci. 2020, 244, 117324. [Google Scholar] [CrossRef] [PubMed]
- De Castro, G.S.; Calder, P.C. Non-alcoholic fatty liver disease and its treatment with n-3 polyunsaturated fatty acids. Clin. Nutr. 2018, 37, 37–55. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Guebre-Egziabher, F.; Rabasa-Lhoret, R.; Bonnet, F.; Bastard, J.P.; Desage, M.; Skilton, M.R.; Vidal, H.; Laville, M. Nutritional intervention to reduce the n-6/n-3 fatty acid ratio increases adiponectin concentration and fatty acid oxidation in healthy subjects. Eur. J. Clin. Nutr. 2008, 62, 1287–1293. [Google Scholar] [CrossRef] [PubMed]
- Seethaler, B.; Basrai, M.; Vetter, W.; Lehnert, K.; Engel, C.; Siniatchkin, M.; Halle, M.; Kiechle, M.; Bischoff, S.C. Fatty acid profiles in erythrocyte membranes following the Mediterranean diet-data from a multicenter lifestyle intervention study in women with hereditary breast cancer (LIBRE). Clin. Nutr. 2020, 39, 2389–2398. [Google Scholar] [CrossRef]
- Green, C.J.; Pramfalk, C.; Charlton, C.A.; Gunn, P.J.; Cornfield, T.; Pavlides, M.; Karpe, F.; Hodson, L. Hepatic de novo lipogenesis is suppressed and fat oxidation is increased by omega-3 fatty acids at the expense of glucose metabolism. BMJ Open Diabetes Res. Care 2020, 8, e000871. [Google Scholar] [CrossRef] [Green Version]
- Marin-Alejandre, B.A.; Abete, I.; Cantero, I.; Monreal, J.I.; Elorz, M.; Herrero, J.I.; Huarte-Muniesa, M.P. The metabolic and hepatic impact of two personalized dietary strategies in subjects with obesity and nonalcoholic fatty liver disease: The fatty liver in obesity (FLiO) randomized controlled trial. Nutrients 2019, 11, 2543. [Google Scholar] [CrossRef] [Green Version]


{kind=link}
| Med Diet Baseline (12) | Med Diet End (12) | p-Value | Low-Fat Diet Baseline (12) | Low-Fat Diet End (12) | p-Value | Low-Fat Diet End vs. Med Diet End p-Value | |
|---|---|---|---|---|---|---|---|
| Age (years) | 34.42 ± 4.66 | 32.92 ± 3.78 | |||||
| Body weight (kg) | 101.11 ± 9.09 | 91.88 ± 9.48 | 0.000 | 102.12 ± 8.19 | 92.41 ± 8.14 | 0.000 | 0.342 |
| BMI (kg/m2) | 30.43 ± 1.81 | 27.65 ± 1.80 | 0.000 | 30.17 ± 2.28 | 27.68 ± 2.44 | 0.000 | 0.342 |
| Waist circumference (cm) | 105.67 ± 5.94 | 95.83 ± 5.73 | 0.000 | 107.58 ± 6.96 | 98.83 ± 8.04 | 0.000 | 0.233 |
| Body fat % | 26.17 ± 1.71 | 21.27 ± 3.05 | 0.000 | 26.93 ± 3.50 | 21.86 ± 3.95 | 0.000 | 0.989 |
| VAI | 2.26 ± 0.81 | 1.05 ± 0.36 | 0.000 | 2.64 ± 0.88 | 1.52 ± 0.47 | 0.000 | 0.083 |
| FLI | 81.92 ± 9.95 | 43.17 ± 7.99 | 0.000 | 83.52 ± 10.76 | 55.08 ± 18.22 | 0.000 | 0.022 |
| HSI | 47.6 ± 4.92 | 39.34 ± 3.24 | 0.000 | 45.85 ± 4.63 | 37.67 ± 4.07 | 0.000 | 0.435 |
| ultrasonography diagnosed NAFLD | 12 | 6 | 12 | 8 |
| Med Diet Baseline | Med Diet End | p-Value | Low-Fat Diet Baseline | Low-Fat Diet End | p-Value | Low-Fat Diet End vs. Med Diet End p-Value | |
|---|---|---|---|---|---|---|---|
| Triglycerides (mmol/L) | 1.92 (1.35–2.55) | 1.06 (0.80–1.20) | 0.000 * | 2.40 (1.55–2.69) | 1.29 (1.20–1.57) | 0.000 * | 0.048 |
| Total cholesterol (mmol/L) | 6.00 ± 0.78 | 4.83 ± 0.95 | 0.000 | 6.08 ± 0.69 | 4.81 ± 0.82 | 0.000 | 0.760 |
| LDL-cholesterol (mmol/L) | 3.67 ± 0.72 | 2.88 ± 0.82 | 0.000 | 3.96 ± 0.89 | 3.14 ± 0.85 | 0.009 | 0.857 |
| HDL-cholesterol (mmol/L) | 1.29 ± 0.13 | 1.41 ± 0.15 | 0.000 | 1.22 ± 0.12 | 1.28 ± 0.11 | 0.041 | 0.041 |
| TG/HDL-cholesterol ratio, | 1.63 ± 0.60 | 0.78 ± 0.26 | 0.000 | 1.87 ± 0.61 | 1.12 ± 0.36 | 0.000 | 0.025 |
| ALT(IU/L) | 65.33 ± 23.90 | 27.33 ± 6.46 | 0.000 | 63.17 ± 15.76 | 31.92 ± 11.89 | 0.000 | 0.128 |
| AST(IU/L) | 32.50 (23.00–32.75) | 20.00 (16.00–21.75) | 0.000 * | 35.65 (25.00–41.50) | 25.50 (18.75–30.75) | 0.006 * | 0.017 |
| GGT(IU/L) | 47.42 ± 36.25 | 24.33 ± 11.57 | 0.000 | 42.53 ± 10.48 | 27.08 ± 9.90 | 0.000 | 0.224 |
| Fasting glucose (mmol/L) | 5.11 ± 0.51 | 4.49 ± 0.68 | 0.000 | 5.20 ± 0.45 | 4.84 ± 0.48 | 0.032 | 0.145 |
| Fasting insulin (pmol/L) | 17.70 ± 3.24 | 13.67 ± 2.94 | 0.000 | 17.33 ± 3.76 | 14.38 ± 3.17 | 0.006 | 0.475 |
| HOMA-IR | 3.96 (3.40−4.76) | 2.63 (2.28–3.04) | 0.000 * | 4.07 (3.45–4.43) | 2.86 (2.53–3.37) | 0.000 * | 0.142 |
| hs-CRP (mg/L) | 1.02 (0.75–2.23) | 0.81 (0.34–1.40) | 0.000 * | 2.10 (0.98–3.20) | 0.77 (0.54–1.27) | 0.008 * | 0.239 |
| LAP | 78.44 ± 27.40 | 34.66 ± 16.78 | 0.000 | 94.58 ± 33.92 | 46.63 ± 12.51 | 0.000 | 0.032 |
| Fatty Acid (%) | Med Diet Baseline | Med Diet End | p-Value | Low-Fat Diet Baseline | Low-Fat Diet End | p-Value | Low-Fat Diet End vs. Med Diet End p-Value |
|---|---|---|---|---|---|---|---|
| 16:0 | 30.18 ± 3.33 | 27.58 ± 1.89 | 0.017 | 30.32 ± 2.93 | 29.94 ± 2.59 | 0.404 | 0.038 |
| 18:0 | 16.09 ± 2.01 | 15.47 ± 1.32 | 0.561 | 16.40 ± 1.21 | 15.92 ± 2.26 | 0.408 | 0.236 |
| SFA | 46.26 ± 4.04 | 43.05 ± 1.73 | 0.036 | 46.72 ± 2.24 | 45.86 ± 2.73 | 0.237 | 0.020 |
| 16:1 n-7 | 0.36 ± 0.11 | 0.41 ± 0.15 | 0.210 | 0.42 ± 0.17 | 0.36 ± 0.07 | 0.329 | 0.208 |
| 18:1 n-9 | 8.37 ± 1.60 | 10.58 ± 2.56 | 0.049 | 9.80 ± 1.33 | 8.57 ± 0.78 | 0.000 | 0.048 |
| 18:1 n-7 | 1.56 ± 0.32 | 1.57 ± 0.65 | 0.942 | 1.17 ± 0.57 | 1.43 ± 0.44 | 0.403 | 0.597 |
| MUFA | 10.28 ± 1.66 | 12.57 ± 2.18 | 0.033 | 11.39 ± 1.42 | 10.36 ± 0.95 | 0.037 | 0.011 |
| 18:2 | 23.91 ± 3.69 | 21.49 ± 3.97 | 0.040 | 22.44 ± 3.32 | 22.69 ± 2.89 | 0.055 | 0.125 |
| 20:3 | 3.08 ± 0.76 | 2.63 ± 1.00 | 0.341 | 3.45 ± 0.68 | 2.87 ± 0.94 | 0.605 | 0.809 |
| 20:4 | 12.15 ± 1.35 | 12.10 ± 1.81 | 0.936 | 11.49 ± 1.90 | 10.85 ± 1.57 | 0.389 | 0.237 |
| 22:4 | 0.63 (0.51−0.94) | 0.62 (0.41–1.11) | 0.865 * | 0.60 (0.36–0.81) | 0.44 (0.25–0.80) | 0.605 * | 0.455 |
| n-6 PUFA | 40.02 ± 4.36 | 37.06 ± 4.26 | 0.111 | 37.96 ± 2.86 | 36.93 ± 3.53 | 0.119 | 0.587 |
| 18:3 | 0.22 (0.07–0.33) | 0.12 (0.09–0.32) | 0.879 * | 0.17 (0.13–0.25) | 0.26 (0.13–0.40) | 0.176 * | 0.696 |
| 20:5 | 0.22 (0.20–0.26) | 0.39 (0.25–0.53) | 0.030 * | 0.38 (0.28–0.71) | 0.88 (0.44–1.56) | 0.047 * | 0.425 |
| 22:5 | 0.61 ± 0.23 | 0.69 ± 0.27 | 0.288 | 0.66 ± 0.12 | 0.76 ± 0.16 | 0.101 | 0.757 |
| 22:6 | 2.67 ± 0.95 | 5.17 ± 1.19 | 0.002 | 2.56 ± 0.77 | 3.96 ± 1.02 | 0.004 | 0.050 |
| n-3 PUFA | 3.74 ± 1.27 | 6.53 ± 1.40 | 0.002 | 3.87 ± 1.04 | 5.92 ± 1.71 | 0.005 | 0.397 |
| PUFA | 43.76 ± 4.22 | 43.59 ± 3.97 | 0.987 | 41.83 ± 2.42 | 42.85 ± 3.67 | 0.189 | 0.977 |
| n-6/n-3 | 11.92 ± 4.35 | 5.94 ± 1.49 | 0.003 | 10.53 ± 3.44 | 6.74 ± 2.14 | 0.004 | 0.245 |
| MUFA/SFA | 0.22 ± 0.41 | 0.29 ± 1.26 | 0.000 | 0.24 ± 0.03 | 0.23 ± 0.03 | 0.138 | 0.004 |
| MUFA/n-6 | 0.26 ± 0.38 | 0.34 ± 0.51 | 0.009 | 0.30 ± 0.05 | 0.28 ± 0.01 | 0.172 | 0.079 |
| MUFA/n-3 | 2.75 ± 1.30 | 1.92 ± 1.56 | 0.023 | 3.13 ± 0.90 | 1.90 ± 0.63 | 0.000 | 0.576 |
| MUFA/PUFA | 0.22 (0.20–0.26) | 0.25 (0.25–0.33) | 0.099 * | 0.26 (0.24–0.31) | 0.23 (0.21–0.26) | 0.015 * | 0.089 |
| Fatty Acid (%) | Med Diet Baseline | Med Diet End | p-Values | LF Diet Baseline | LF Diet End | p-Values | Low-Fat Diet End vs. Med Diet End p-Value |
|---|---|---|---|---|---|---|---|
| 16:0 | 23.24 ± 2.33 | 22.74 ± 2.23 | 0.436 | 25.29 ± 1.74 | 24.62 ± 1.06 | 0.344 | 0.296 |
| 18:0 | 20.50 ± 1.48 | 20.08 ± 1.29 | 0.627 | 21.91 ± 1.35 | 21.31 ± 2.78 | 0.521 | 0.353 |
| SFA | 43.74 ± 3.21 | 42.82 ± 2.11 | 0.447 | 47.20 ± 2.40 | 45.93 ± 3.29 | 0.243 | 0.225 |
| 16:1 n-7 | 0.26 ± 0.13 | 0.28 ± 0.11 | 0.575 | 0.30 ± 0.15 | 0.31 ± 0.10 | 0.845 | 0.694 |
| 18:1 n-9 | 14.03 ± 1.39 | 15.53 ± 1.20 | 0.002 | 14.45 ± 1.85 | 15.10 ± 2.08 | 0.256 | 0.222 |
| 18:1 n-7 | 1.14 ± 0.24 | 1.36 ± 0.28 | 0.138 | 1.49 ± 0.52 | 1.49 ± 0.25 | 0.911 | 0.724 |
| MUFA | 15.44 ± 1.48 | 17.17 ± 1.37 | 0.002 | 16.25 ± 1.90 | 16.89 ± 2.24 | 0.208 | 0.144 |
| 18:2 | 14.02 ± 1.38 | 12.92 ± 1.49 | 0.158 | 12.67 ± 2.08 | 11.91 ± 2.42 | 0.209 | 0.795 |
| 20:3 | 1.71 ± 0.38 | 1.55 ± 0.31 | 0.328 | 1.52 ± 0.32 | 1.36 ± 0.30 | 0.232 | 0.341 |
| 20:4 | 16.00 ± 2.02 | 16.20 ± 2.45 | 0.858 | 14.19 ± 1.17 | 14.40 ± 1.25 | 0.677 | 0.179 |
| 22:4 | 4.02 (3.32–4.64) | 3.62 (3.29–4.37) | 0.956 * | 3.11 (2.42–4.94) | 3.27 (2.50–4.95) | 0.564 * | 0.671 |
| n-6 PUFA | 35.78 ± 1.87 | 34.73 ± 3.15 | 0.477 | 31.90 ± 2.37 | 31.39 ± 2.66 | 0.644 | 0.113 |
| 18:3 | 0.07 (0.05–0.28) | 0.11 (0.05–0.33) | 0.438 * | 0.07 (0.04–0.35) | 0.09 (0.06–0.27) | 0.555 * | 0.935 |
| 20:5 | 0.29 (0.27–0.39) | 0.45 (0.29–0.83) | 0.112 * | 0.29 (0.15–0.45) | 0.32 (0.23–0.53) | 0.992 * | 0.183 |
| 22:5 | 1.43 ± 0.43 | 1.68 ± 0.50 | 0.029 | 1.07 ± 0.41 | 1.29 ± 0.32 | 0.154 | 0.426 |
| 22:6 | 3.17 ± 0.75 | 4.12 ± 1.14 | 0.028 | 2.81 ± 0.95 | 3.69 ± 1.34 | 0.015 | 0.855 |
| n-3 PUFA | 5.04 ± 1.24 | 6.50 ± 1.72 | 0.011 | 4.40 ± 1.55 | 5.53 ± 1.82 | 0.021 | 0.554 |
| PUFA | 40.82 ± 2.54 | 41.24 ± 3.92 | 0.800 | 36.30 ± 3.22 | 36.92 ± 3.16 | 0.489 | 0.237 |
| n-6/n-3 | 7.41 (6.72–8.64) | 5.98 (4.41–6.50) | 0.004 * | 7.31 (6.31–9.58) | 5.04 (4.32–8.82) | 0.041 * | 0.679 |
| MUFA/SFA | 0.35 ± 0.46 | 0.40 ± 0.03 | 0.005 | 0.34 ± 0.04 | 0.37 ± 0.06 | 0.132 | 0.215 |
| MUFA/n-6 | 0.43 ± 0.79 | 0.50 ± 0.07 | 0.029 | 0.51 ± 0.09 | 0.54 ± 0.08 | 0.272 | 0.824 |
| MUFA/n-3 | 3.16 (2.83–3.62) | 2.67 (2.24–3.44) | 0.165 * | 3.62 (2.76–4.95) | 2.92 (2.26–5.38) | 0.079 * | 0.914 |
| MUFA/PUFA | 0.38 ± 0.58 | 0.42 ± 0.06 | 0.095 | 0.45 ± 0.09 | 0.46 ± 0.08 | 0.617 | 0.709 |
| ΔFLI | β | p | Adjusted R2 | |
|---|---|---|---|---|
| Model 1 | Low-fat diet vs. Med diet | 0.377 | 0.043 | 0.103 |
| Model 2 | Low-fat diet vs. Med diet | 0.452 | 0.023 | 0.243 |
| Age | −0.115 | 0.235 | ||
| Model 3 | Low-fat diet vs. Med diet | 0.466 | 0.032 | 0.273 |
| ΔAST | 0.010 | 0.964 | ||
| ΔHDL | −0.373 | 0.131 | ||
| ΔTG | −0.256 | 0.251 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Ristic-Medic, D.; Kovacic, M.; Takic, M.; Arsic, A.; Petrovic, S.; Paunovic, M.; Jovicic, M.; Vucic, V. Calorie-Restricted Mediterranean and Low-Fat Diets Affect Fatty Acid Status in Individuals with Nonalcoholic Fatty Liver Disease. Nutrients 2021, 13, 15. https://doi.org/10.3390/nu13010015
Ristic-Medic D, Kovacic M, Takic M, Arsic A, Petrovic S, Paunovic M, Jovicic M, Vucic V. Calorie-Restricted Mediterranean and Low-Fat Diets Affect Fatty Acid Status in Individuals with Nonalcoholic Fatty Liver Disease. Nutrients. 2021; 13(1):15. https://doi.org/10.3390/nu13010015
Chicago/Turabian StyleRistic-Medic, Danijela, Marijana Kovacic, Marija Takic, Aleksandra Arsic, Snjezana Petrovic, Marija Paunovic, Maja Jovicic, and Vesna Vucic. 2021. "Calorie-Restricted Mediterranean and Low-Fat Diets Affect Fatty Acid Status in Individuals with Nonalcoholic Fatty Liver Disease" Nutrients 13, no. 1: 15. https://doi.org/10.3390/nu13010015